
Abstract
Aims
To compare the long-term safety and efficacy of subconjunctival injection mitomycin C(MMC) with conventional sponge applied MMC during trabeculectomy.
Methods and Material
Retrospective analysis of 98 eyes of 90 patients who underwent trabeculectomy with Mitomycin C were divided into two groups, group 1- sponge (n = 52) and group 2- Injection(n = 46). Follow-up data were collected on day one, day 15, one month, three months, six months, one year, two years and three years. Data from baseline and follow-up visits were analyzed and compared to study the significant difference in intraocular pressure (IOP), number of antiglaucoma medications (AGM) and best corrected visual acuity (BCVA) . P-value of <0.05 was considered statistically significant.
Results
Mean preop IOP was 34.61 ± 13.3 mmHg in group one and 33.07 ± 9.6 mmHg in group two, which reduced to 11.43 ± 3.2 and 11.59 ± 3.2 mmHg at three years (p < 0.001 in both groups) with no significant difference between the groups. Mean number of preoperative AGM was 2.28 ± 0.8 and 2.42 ± 0.7 in group one and two respectively which reduced to 1.19 ± 1.1(p = 0.405) and 0.88 ± 0.9(p = 0.001) at three years. Complete and overall success rates (complete + qualified) were 59.3% and 78.9% in group one and 60.9% and 80.4% in group two at three years. No statistically significant difference was found in complication rates, post-operative interventions, and final visual outcome in both groups.
Conclusions
Subconjunctival Injection MMC was a safe and effective alternative to sponge application with comparable long term surgical outcomes.
Introduction
Trabeculectomy remains the most effective incisional surgical method for lowering IOP, inspite of the growing popularity of multiple minimally invasive glaucoma surgeries.1,2 MMC was first introduced for intraoperative use in trabeculectomy by Chen et al in 1983. 3 MMC is an antineoplastic antifibrotic agent isolated from the fermentation filtrate of Streptomyces caespitosus, which is a deoxyribonucleic acid cross-linker, thus inhibiting fibroblast formation. 4 Due to its antifibrotic effect, it reduces subconjunctival scarring and improves the likelihood of functional bleb formation. 5 MMC is indicated in young patients, patients who have undergone previous surgery, or patients of African- American descent. 6
The sponge technique is considered the conventional method where they are placed onto the scleral surgical site before creating the ostium, before or after the formation of a partial thickness scleral flap. The using of large and irregular sponges, improper positioning, and high concentrations of MMC can cause hypotony, bleb leakage, blebitis, limited reoperation area due to thin avascular conjunctiva, and surrounding scarring from exposure to MMC.7–9 A novel technique of MMC application has been described where it is injected into Tenon's layer prior to scleral flap formation. Recently there has been a trend toward subconjunctival injection of MMC during trabeculectomy. In our study, we aim to compare the long term safety and efficacy of subconjunctival MMC with conventional sponge soaked MMC during trabeculectomy.
Methods
This study was a retrospective comparative case series, designed from a consecutive series of trabeculectomies with mitomycin C performed in a tertiary eye care center in south India. It adhered to the tenets of the Declaration of Helsinki and complied with HIPAA requirements and local patient privacy protection policies. The study protocol was approved after a full review by the Institutional Research Ethics Committee. A written informed consent was obtained before utilizing the data for the study. Patients who underwent trabeculectomy with either subconjunctival MMC injection or MMC-soaked sponges between 2016 and 2018 and completed at least three years of follow-up postoperatively were included in the study. Monocular individuals, patients who had undergone previous ocular surgeries except for cataract surgery, suspected scleral thinning, active inflammation, patients with systemic comorbidities like connective tissue disorders, immunodeficiency, pregnant or nursing women, and those unwilling to provide informed consent were excluded. Data were collected from pre and post-operative clinical charts. Demographic data, preoperative intraocular pressure (IOP) with Goldmann applanation tonometry, best corrected visual acuity (BCVA), and number of anti-glaucoma medications were recorded. Postoperative data, including IOP, BCVA, number of antiglaucoma medications, postoperative complications, and interventions, if any, were collected on day one, two weeks, one month, three months, six months, one year, two years, and three years. Standardized definitions of post postoperative complications were used during the data collection process. Specifically, post-op data on complications including bleb leak, hypotony, shallow anterior chamber, and choroidal detachment were collected. Postoperative interventions like releasable suture removal, bleb needling, laser suture lysis, repeat trabeculectomy, etc were also noted. Complete success was defined as IOP ≤ 21 mmHg and ≥6 mmHg or more than 20% IOP reduction compared to pre-operative values, without the addition of anti-glaucoma medications. Qualified success was defined as IOP ≤ 21 mmHg and ≥6 mmHg or more than 20% IOP reduction with anti-glaucoma medications. Failure was defined as IOP >21 mmHg and <6 mmHg or less than 20% IOP reduction from baseline IOP in two consecutive visits after the follow-up of two weeks or the need for repeat surgery.
The primary outcome measure was intraocular pressure reduction in both groups. Reduction in antiglaucoma medications between the groups, surgical success, and any complications and interventions were the secondary outcomes.
Surgical procedure
All trabeculectomies were performed at a single institution by two experienced glaucoma surgeons (DM, MAK). Adequate anesthesia was obtained via a peribulbar injection (3 ml of lignocaine +50 IU/ml Hyaluronidase and 1:2,00,000 adrenaline). Our preparation of MMC included mixing 2 mg of MMC powder (Mitomycin 2, Zydus Celexa, SPAL Private Ltd, Telangana, India) with 10 ml sterile water diluent to achieve a concentration of 0.2 mg/ml. 0.1 ml of this solution was drawn to be injected subconjunctivally. A 30-gauge needle was introduced 7 to 8 mm from the limbus and the MMC preparation was injected subconjunctivally (Figure 1). To avoid egress to the limbus, the drug is gently pushed posteriorly with the aid of a spatula. After a waiting period of two minutes, a fornix-based conjunctival peritomy was done in the superior quadrant. For hemostasis, wet-field bipolar cautery was used. Using a 15-number blade, a 4 × 4 mm, triangular, partial thickness scleral flap was dissected. Using a 1 mm side port blade in the temporal cornea, a paracentesis was made. Kelly's punch was used to create a sclerotomy and DeWecker scissors were used to create a peripheral iridectomy. The scleral flap was then sutured with two fixed and one releasable 10-0 monofilament nylon sutures. Conjunctival closure was done with a running 8-0 polyglactin sutures. In the eyes that received MMC sponges, the sponges soaked in a similar concentration (0.2 mg/ml MMC) solution were inserted subconjunctivally. The sponges were placed for two minutes following which copious irrigation with normal saline was done after removal of the sponges. The trabeculectomy procedure was then performed as described previously. The postoperative regimen consisted of 2 hourly Dexamethasone (0.1%) with Chloramphenicol (0.5%) eye drops and topical cycloplegic for four weeks from the first post-operative day.
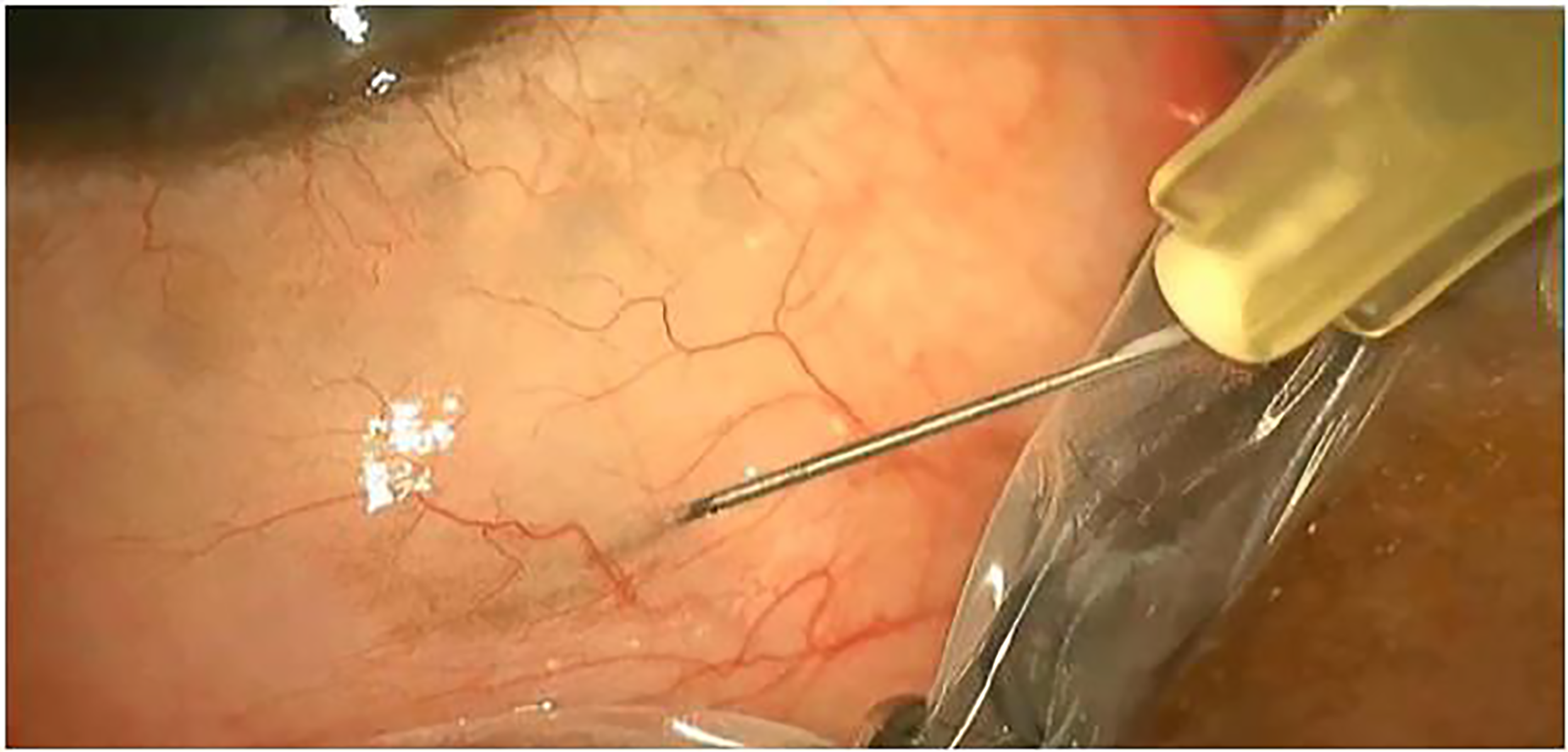
Subconjunctival injection of mitomycin C.
Statistical analysis
All statistical analysis were performed using STATA, version 14.2 (StataCorp, USA). The normality of the data was assessed using the Shapiro-Wilk test and Box-Whisker's plot. Descriptive statistics of the data were reported using frequencies (n) and percentages (%) for categorical variables and mean (standard deviation, SD) for continuous variables. A chi-square test was performed to assess the association between groups of categorical variables. Visual acuity values were converted into logarithm of minimal angle of resolution (log MAR) from Snellen's equivalent value for statistical analysis and were reported in median (interquartile range, IQR). To adjust for possible biases derived from the inclusion of both eyes of the same patient and for differences in the follow-up visits of pre-operative intraocular pressure (IOP) and IOP measured at 1 day, 2 weeks, 1 month, 3 months, 6 months, 1 year, 2 years and 3 years post-operatively were compared using a mixed effect regression model in which each subject's identification number was regarded as random effect and the time (follow-up periods) was considered as a fixed effect. Post-operative changes in the number of anti-glaucoma medications (AGM) and best-corrected visual acuity (BCVA) were also analyzed using the mixed effect model. Comparison of IOP between the sponge and injection group was assessed using an independent t-test. The between-group comparison of AGM and BCVA was evaluated using the Wilcoxon rank sum test. Successful IOP control was defined and the cumulative probabilities were assessed using Kaplan-Meier (KM) survival analysis. The success curve between the sponge and injection groups was compared using the log-rank test. A P-value less than 0.05 was considered statistically significant
Results
In total, 98 eyes of 90 patients were included in the study (Table 1). 52 eyes underwent trabeculectomy with MMC-soaked sponges (Group 1) and 46 eyes with Injection mitomycin C (Group 2).For patients(N = 8) whose both eyes were included, the same surgical technique was used for both eyes.
Demographic details of the study participants.
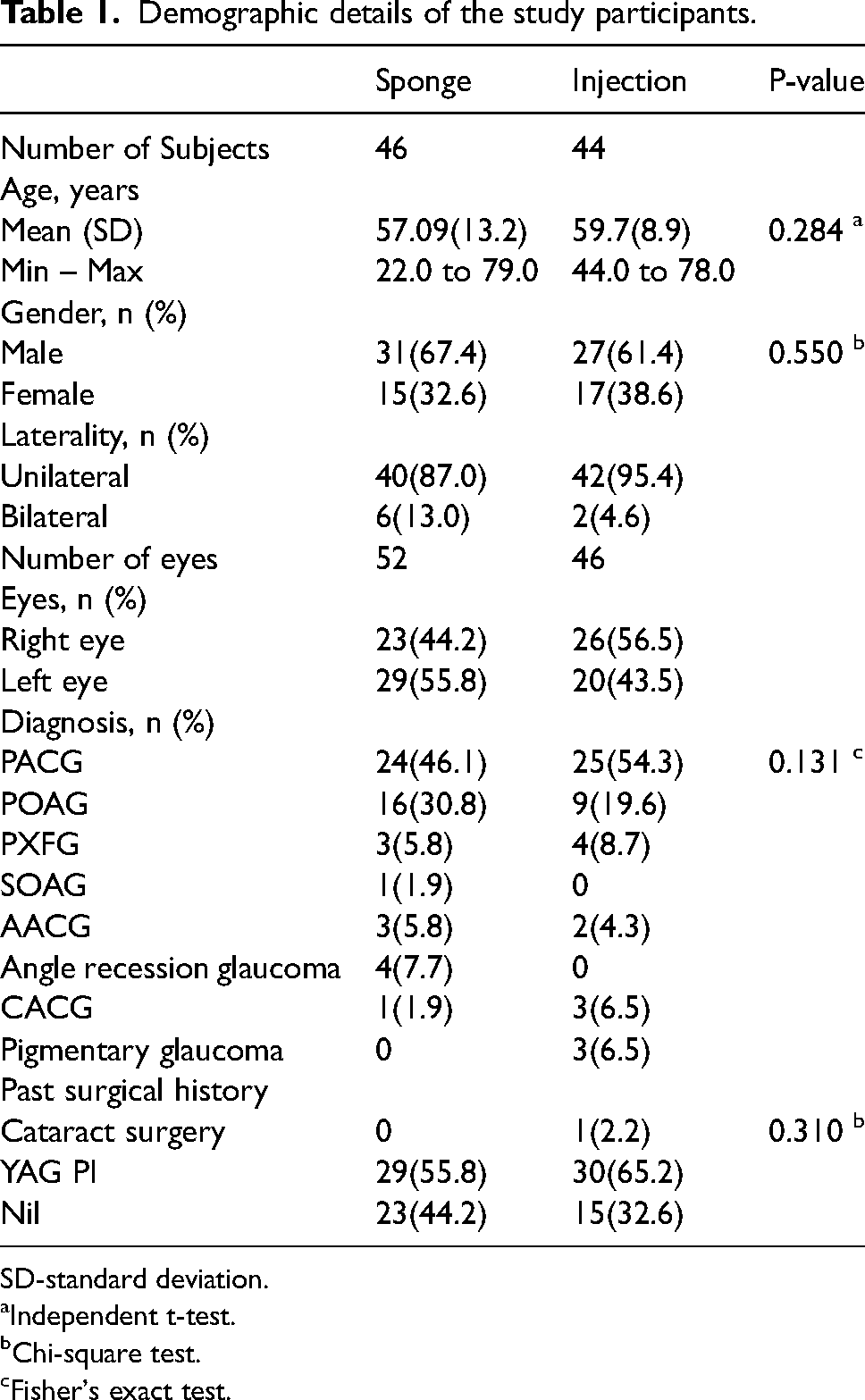
SD-standard deviation.
Independent t-test.
Chi-square test.
Fisher's exact test.
Mean preop IOP was 34.61 ± 13.3 mmHg in group one and 33.07 ± 9.6 mmHg in group two, which reduced to 11.87 ± 3.8 and 12.67 ± 3.8 mmHg (6 months), 12.15 ± 4.2 and 12.41 ± 3.1 mmHg (one year), 12.69 ± 4.7 and 12.20 ± 3.3 mmHg(two years) and11.43 ± 3.2 and 11.59 ± 3.2 mmHg at final visit in group one and two respectively (p < 0.001 in both groups). (Table 2) No significant difference was found between the two groups by the end of three years (Figure 2).
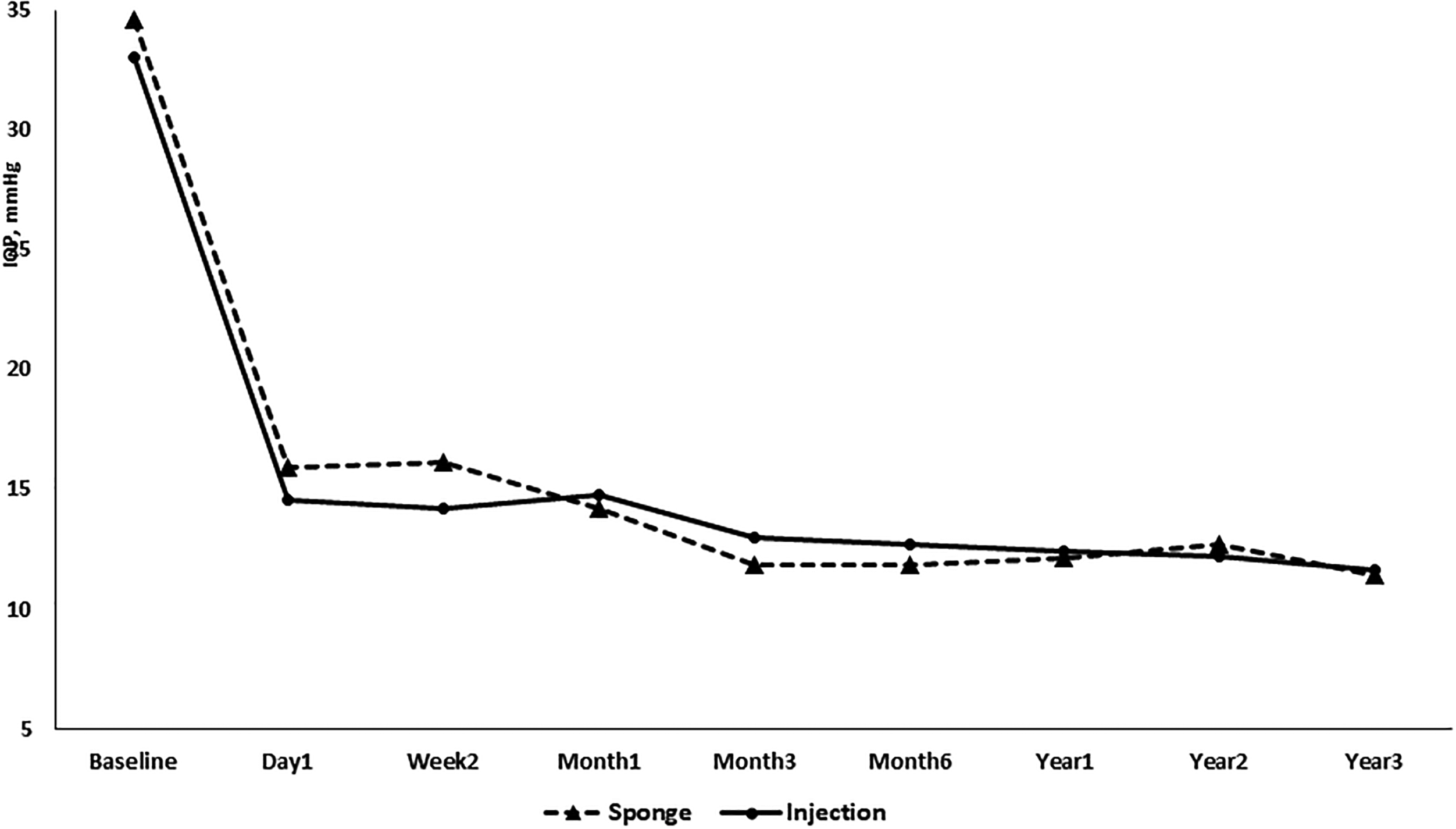
Line graph illustrating the trajectory line of IOP between sponge and injection groups over the follow-up visits.
Comparison of IOP's and medications between the sponge and injection group.
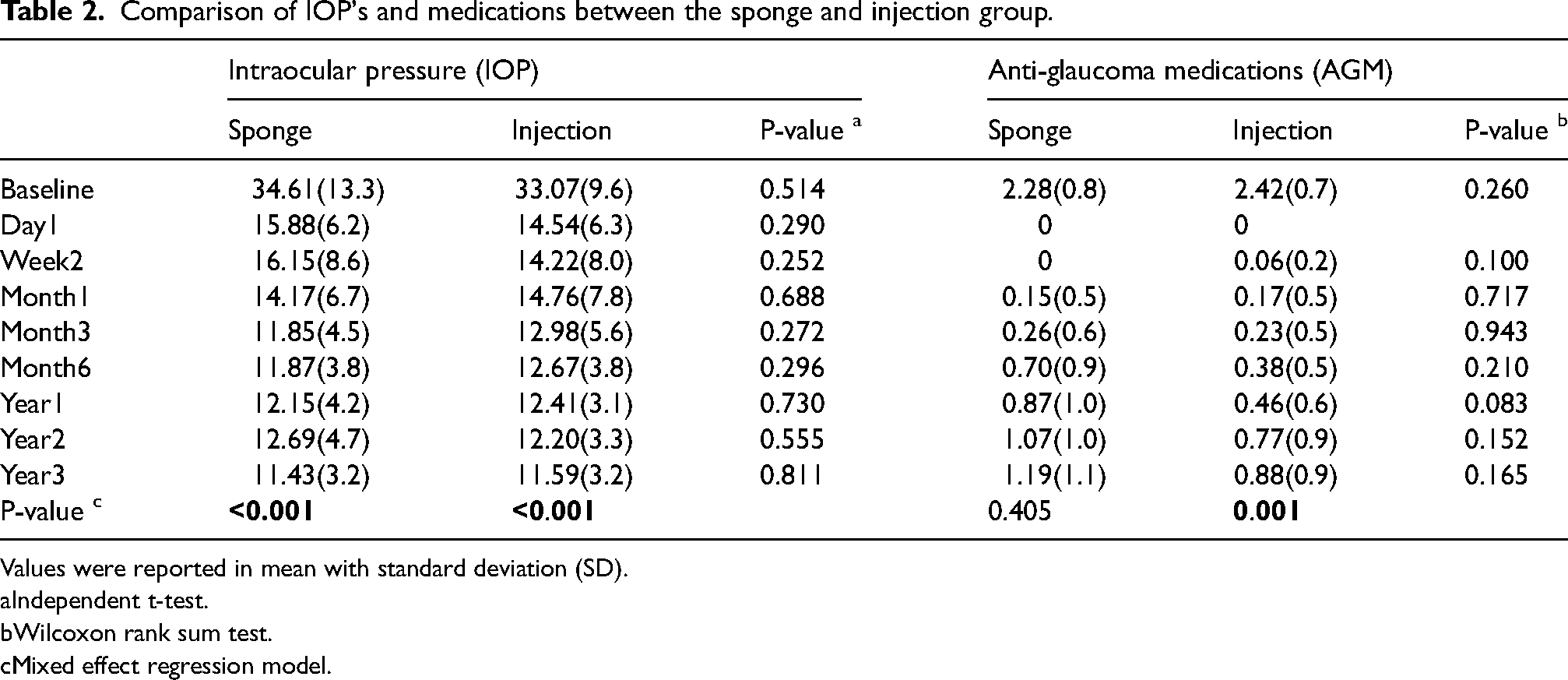
Values were reported in mean with standard deviation (SD).
Independent t-test.
Wilcoxon rank sum test.
Mixed effect regression model.
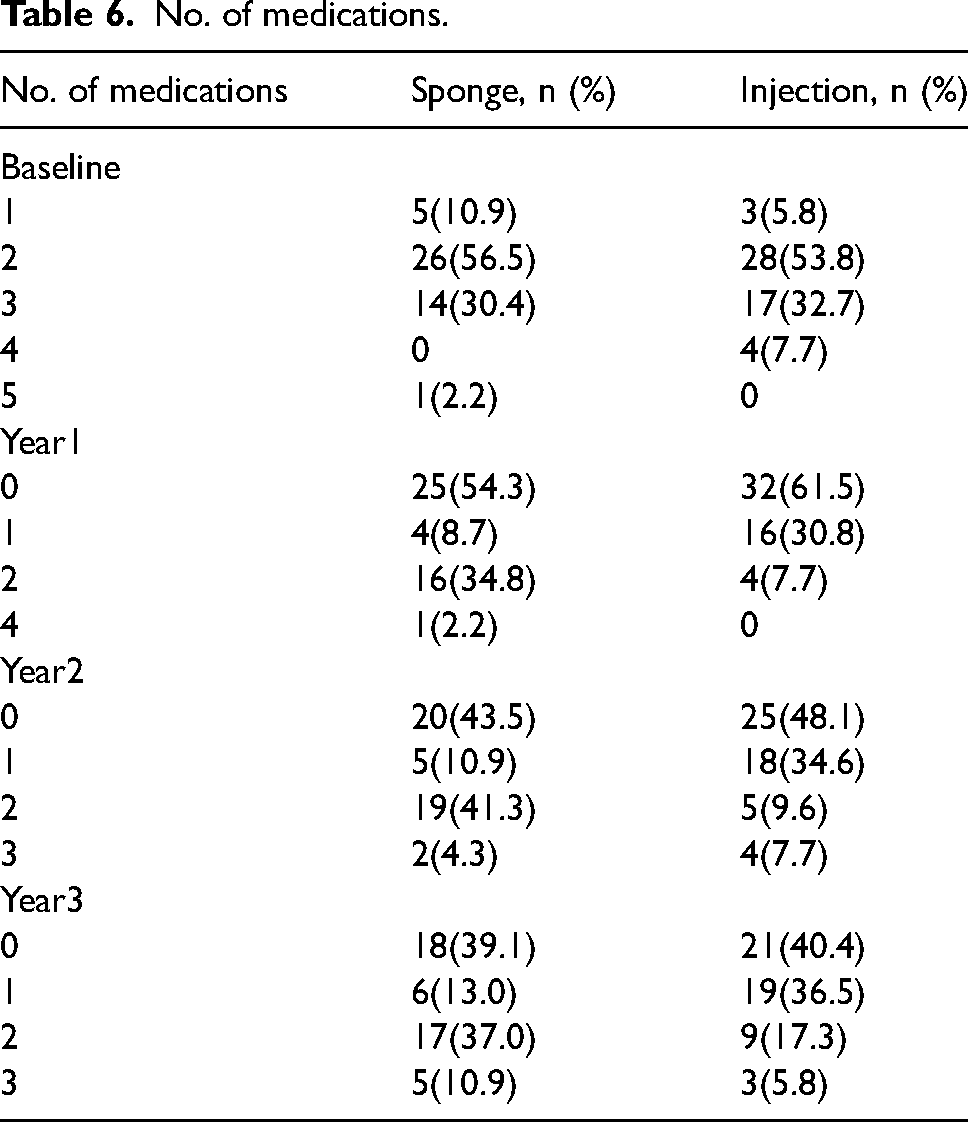
The mean number of preoperative AGM was 2.28 ± 0.8 and 2.42 ± 0.7 in groups one and two respectively which reduced to 1.19 ± 1.1(p = 0.405) and 0.88 ± 0.9(p = 0.001) at three years (Table 2). The number of patients remaining medication-free was 39.1% in the sponge group and 40.4% in the injection group at the end of three years (Table 6)
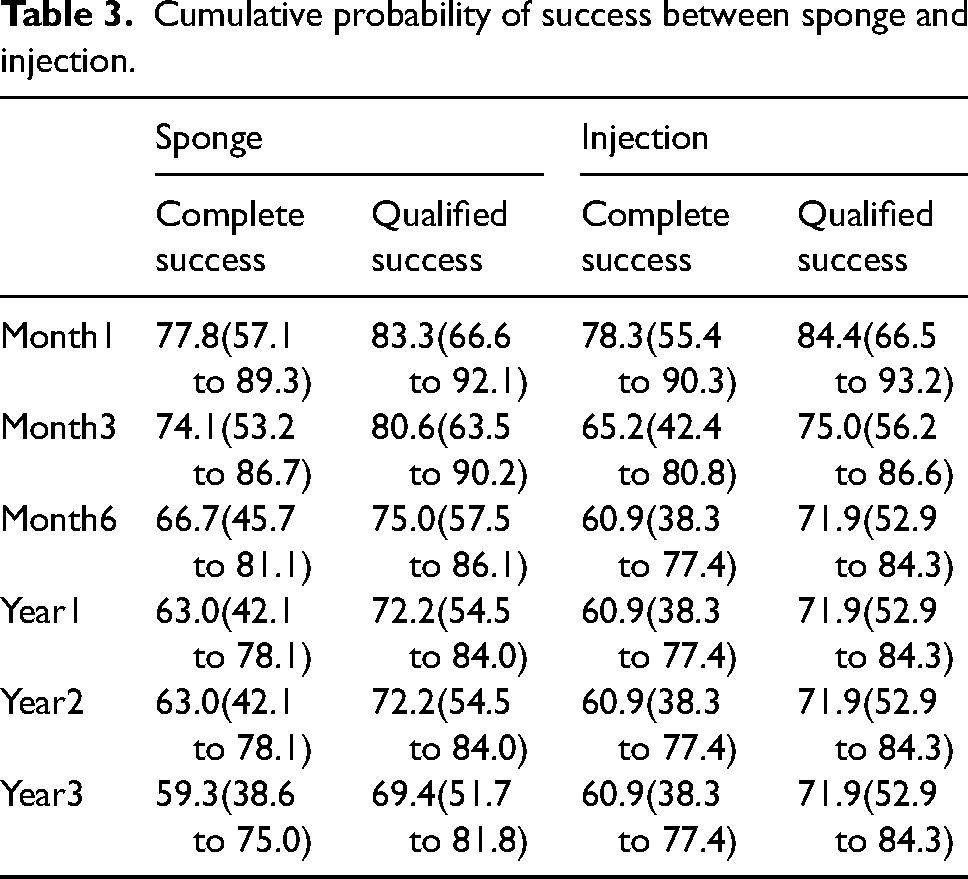
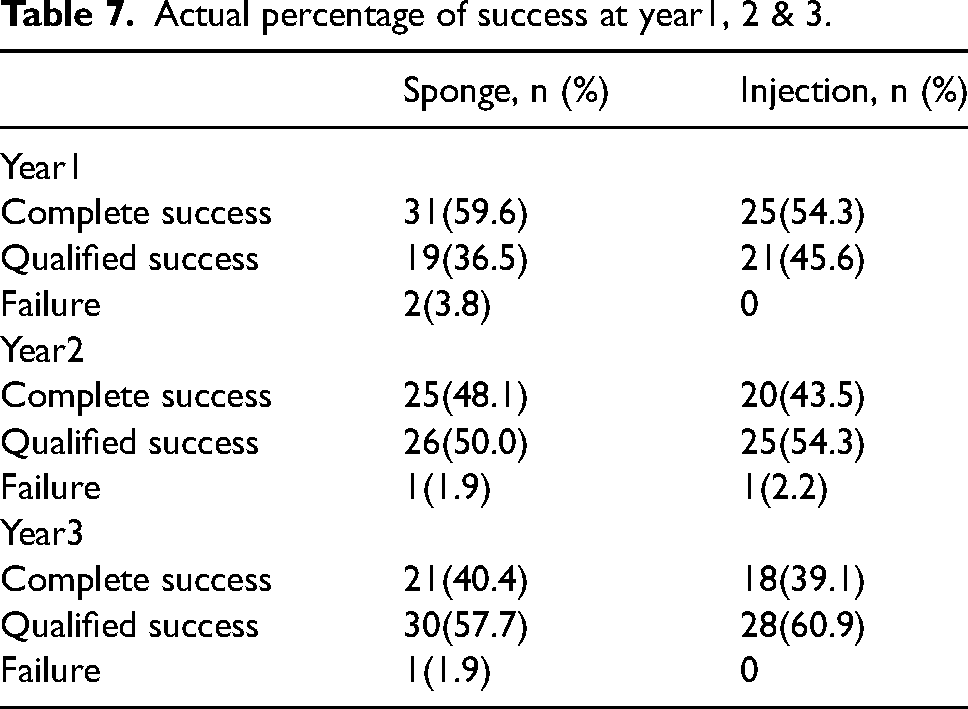
The complete success rate was 59.3% in the sponge group and 60.9% in the injection group at the end of three years. The qualified success rate was 69.4% in the sponge group and 71.9% in the injection group by the end of three years (Tables 3–6). The overall success was found to be 78.9% and 80.4% at three years in the sponge and injection group respectively which was not statistically significant (p = 0.870) (Figure 3). Success rates at the end of each year are depicted in Table 7.
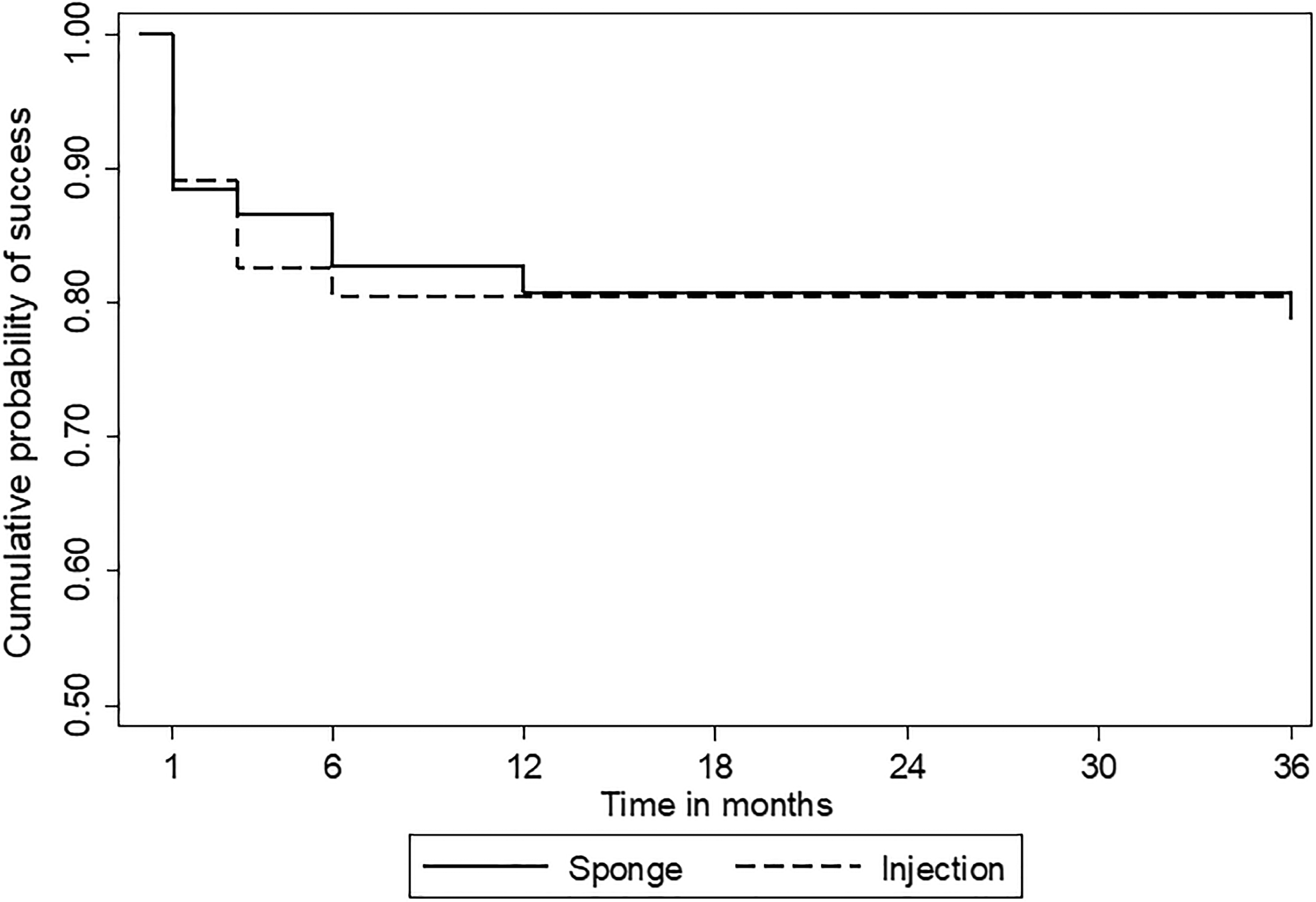
Kaplan-Meier survival curve showing the cumulative probability of success between sponge and injection group.
Cumulative probability of success between sponge and injection.
Post-operative complications and interventions.
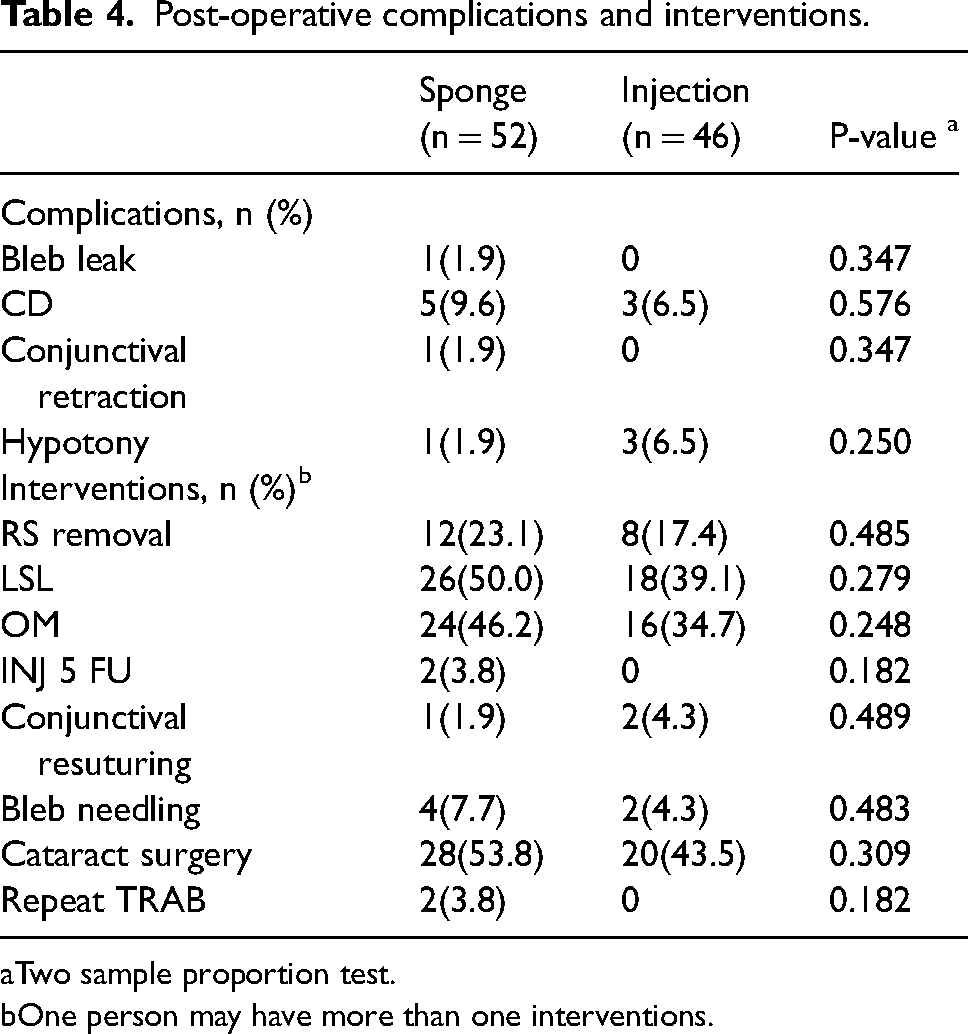
Two sample proportion test.
One person may have more than one interventions.
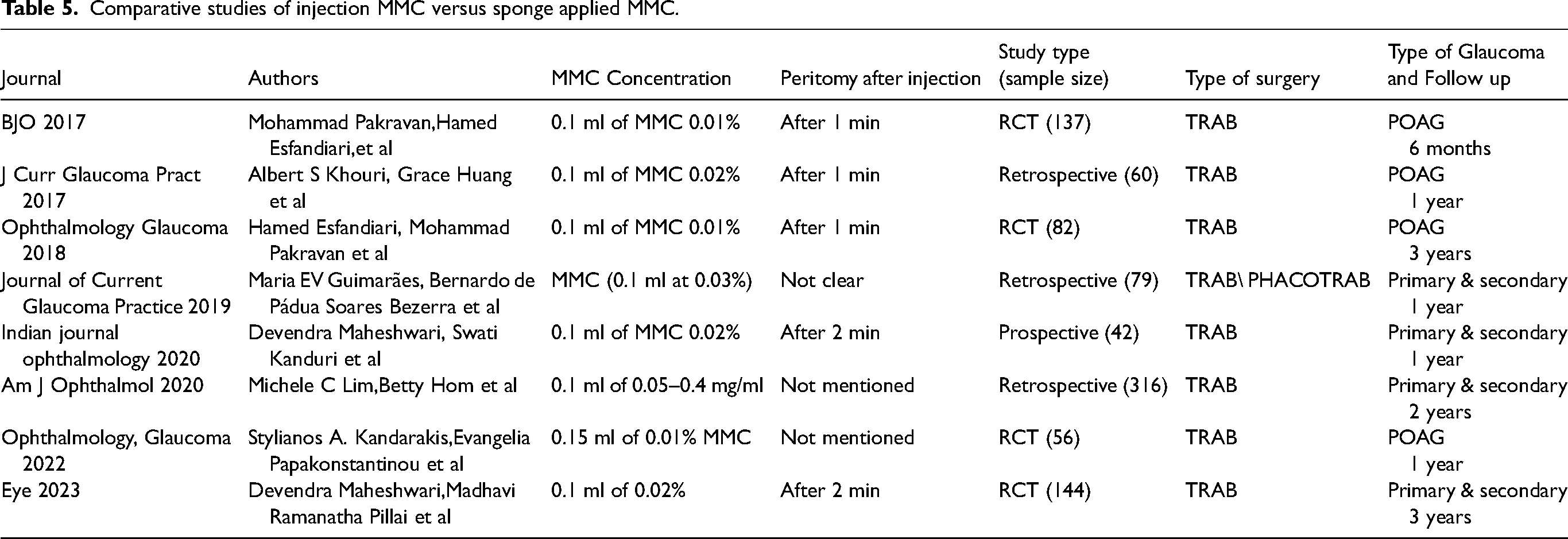
Comparative studies of injection MMC versus sponge applied MMC.
No. of medications.
Actual percentage of success at year1, 2 & 3.
In the sponge group, 9.6% (5 patients) developed Choroidal detachment and one patient developed hypotony which resolved with conservative management whereas 6.5%(3 patients) developed choroidal detachment and three patients developed hypotony in the injection group. However, this was not found to be statistically significant. In both groups, choroidal detachment and hypotony occurred in the early postoperative course(up to 3 months). One patient each in the sponge and the injection group developed delayed onset hypotony and choroidal detachment one year after surgery.50% of the patients in the sponge group required argon laser suture lysis whereas 39.1% required ALS in the injection group. Four (7.7%) patients in the sponge group required bleb needling compared to 2 (4.3%) patients in the injection group. 2 patients in the sponge group underwent repeat trabeculectomy by the end of two years and 2 patients received 5-FU. Cataract surgery was done in 53.8% of the eyes in the sponge group and 43.5% of the eyes in the injection group, mostly between two to three years of follow-up period (Table 4).
The LogMAR BCVA at baseline was 0.40(0.6) [Mean(SD)] and at three years was 0.39(0.6) in the sponge group and in the injection group was 0.36(0.5 and 0.29(0.5) at baseline and three years respectively. There was no statistically significant difference between baseline and final visual acuity in the sponge group (p = 0.832) and injection group (p = 0.522).
Discussion
Trabeculectomy, being the most common and effective surgical procedure for lowering IOP in glaucoma, has undergone several technical modifications over the years, like the use of antimetabolites, releasable sutures, and new surgical instruments. 10 Since first described in the late 1960s by Cairns, 11 trabeculectomy has been modified with the goals of enhanced success rates and decreased complication rates. 12 Position of the conjunctival opening (limbal vs fornix), size and shape of the scleral flap design, use of releasable and adjustable sutures, and use of antimetabolites like MMC or 5-FU are the most notable modifications.
To increase the success rate of the surgical procedure, augmentation with antimetabolites like Mitomycin C or 5-Fluorouracil is usually done. Sponge-soaked MMC is the most common mode of administration of MMC. The most commonly used concentration of MMC is 0.2 mg/ml – 0.4 mg/ml applied for 1 to 5 min, depending on the patient's profile, age, ethnic background, age, and type of glaucoma13–17 (Table 5). The demerits of using sponge-soaked MMC are the possibility of sponge retention, fragmentation, excessive conjunctival manipulation, longer surgical time, and difficulty in predicting the dose of MMC delivered.
A novel technique of MMC application was described by Lee et al 18 involving subconjunctival or intratenon injection of MMC during trabeculectomy surgery and reported favorable outcomes. There are several advantages of subconjunctival MMC over the traditional method of sponge application. These include the reduced risk of MMC burns, less conjunctival damage during manipulation, and eliminating the risk of inadvertently retained sponge material. 19 Additionally, compared to MMC-soaked sponges, which have been proven to have considerable intra- and inter-observer variability in quantification, it enables the delivery of a more exact amount of MMC.20,21 Subconjunctival injection of MMC also offers a better coverage area and can result in better bleb morphology and filtering function.22,23
In our study, we used 0.1 ml of 0.2 mg/ml concentration of MMC. Comparatively, 0.1 ml of 0.1 mg/ml MMC was utilized by Pakravan et al, 24 Esfandiari et al, 25 and 0.15 ml by Kandarakis et al, 12 however, Kandarakis et al employed a greater injection volume. In our study, there was a statistically significant reduction of IOP from the baseline in both groups. In the sponge group and the injection group, the median IOP was reduced by 64.3% and 66.7%, respectively, from the baseline. Studies by Khouri et al., 26 Chiew et al., 27 and Kandarakis et al. 12 were shown to be compatible with this. In the Esfandiari et al study and in another randomized controlled trial by us, where the patients were followed up for three years, the reduction in IOP was comparable between the groups.25,28 In a study by Lim et al, 29 the change in IOP from baseline was significantly lower in the MMC sponge group at postoperative month 24. This could probably be because of the lower preoperative IOP in the injection group which made it difficult to exert a change.
In the injection group, the decrease from baseline in the use of anti-glaucoma drugs was statistically significant (p = 0.001), but not in the sponge group (p = 0.405). However, there was no statistically significant difference between the groups at the end of three years. This was similar to the study by Esfandiari et al which did not find a significant difference in antiglaucoma medications between the groups at the end of three years. 25
In our study, at the end of three years, the complete success rate was 59.3% in the sponge group and 60.9% in the injection group. At the end of our follow-up, Kaplan Meier survival analysis, which was used to assess the cumulative probability of success between the two groups, showed that the sponge group had an overall success rate of 78.9% and the injection group had an overall success rate of 80.4% (Figure 2). The study by Esfandiari et al had a cumulative probability of success of 72.2% in the injection group and 65.1% in the sponge group. In a retrospective analysis, Lim et al 29 found that the sponge group had a success rate of 68.9% while the injection group had a success rate of 66.8%. In a study by Kandarakis et al 12 complete surgical success was 81.5% and 82.8% in the injection and sponge group respectively. In a study by Pakravan et al, 24 82.5% of the patients in both groups achieved complete success. It is to be noted that the definition of complete success and the follow-up periods varied in the above-mentioned studies. In another randomized controlled trial by our group with a follow-up period of three years, we found an overall success of 75.3% and 70.7% in the injection and sponge groups respectively 28
In our study, we encountered complications like bleb leak, hypotony, and choroidal detachment and post-operative interventions like releasable suture removal, laser suture lysis, bleb needling, injection 5-FU, and repeat trabeculectomy in both groups. However, the percentage of patients encountering complications and requiring post-operative interventions in their follow-up visits were more in the sponge group. Studies by Khouri et al, 26 Pakravan et al, 24 Esfandiari et al, 25 Maheshwari et al 28 suggested that complication rates did not differ with injection or sponge application of MMC. In our study, two patients out of 52 patients (3.8%) in the sponge group received Injection 5 FU postoperatively. This was comparable to the study by Khouri et al, 26 who found that the group who received subconjunctival MMC injections had less need for postoperative 5-FU injections (16.6%).
The limitations of our study were that this was a retrospective study where the patients were operated on and followed up by different surgeons postoperatively. Inclusion of patients who came for three-year follow-up only would have caused a bias in the reported postoperative complications. We also acknowledge that the bleb morphology should have been another important outcome that needed more focus.
Conclusion
Subconjunctival Injection MMC is a safe and effective alternative to the conventional sponge application with comparable long term surgical outcomes, treatment success and lesser postoperative interventions.
Footnotes
Acknowledgements
Nil.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.