
Abstract
Conjunctival lymphangiomas are rare hamartomas of lymphatic origin that are usually located in the bulbar conjunctiva. They commonly present either as focal or diffuse bulbar chemosis or as dilatation of lymphatic vessels that resembles an isolated cyst or a group of cysts. There can be bleeding inside the lymphangioma resulting in “chocolate cysts”. 1 We report the unusual case of a conjunctival lymphangioma on a 36 year-old male that presented as a large horn-like protruding structure. The lesion was surgically removed with simple excision associated with cryotherapy to the lesion's borders, as malignancy could not be ruled out preoperatively. Histopathological examination revealed a lymphangioma composed of an ill-defined proliferation of dilated lymphatic channels in the lamina propria, underlying conjunctival epithelium with squamous metaplasia, acanthosis and hyperkeratosis. One year postoperatively, the patient remains asymptomatic and without recurrence of the lesion.
Keywords
Introduction
Conjunctival lymphangiomas are very infrequent lesions that usually present in the first decade of life, although there are reports of presentation up to 79 years old. 2 This diagnosis requires a high index of suspicion, mainly in patients with chemosis or conjunctival focal or multifocal lesions refractory to corticosteroid topical therapy and without other known causes. We report a very unique presentation of this condition in a patient with a rapidly growing conjunctival lesion with an associated keratin horn. Histopathological findings were essential in establishing the diagnosis and excluding malignancy. Complete written informed consent was obtained from the patient for the publication of this study and accompanying images.
Case description
A 36 year-old man presented to the Ophthalmology emergency department complaining of a foreign body sensation and localized conjunctival hyperemia associated with a recently growing conjunctival lesion. The patient had no personal history of any systemic or ophthalmological diseases and this was the first time he was evaluated by an Ophthalmologist.
Biomicroscopic examination of the patient's eye revealed a conjunctival lesion presenting as a large horn-like protruding structure with surrounding dilatation of conjunctival vessels in the inferior temporal quadrant of his left eye (Figure 1). He presented with no other abnormal features in the anterior segment and ocular fundus observation was normal. The patient denied any previous trauma or foreign body accidents concerning that eye. Thorough examination of the fellow eye was unremarkable.
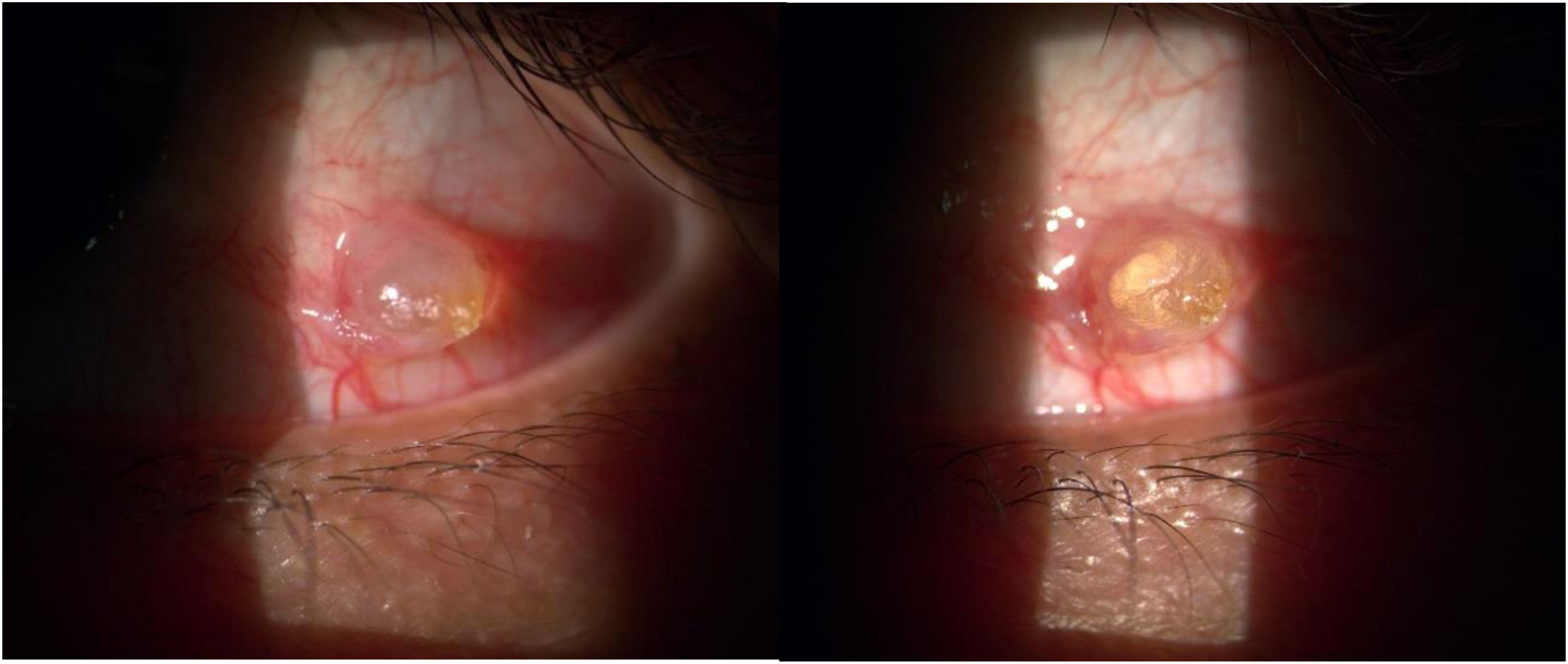
Slit lamp photography of the conjunctival lesion at presentation.
The patient was initially medicated with topical dexamethasone four times a day and lubricant with very little relief of the symptoms or change in the aspect of the eye. Therefore, a decision was made to surgically excise the lesion performing cryotherapy to its borders, as malignancy had not been excluded.
Histopathological analysis revealed an ill-defined proliferation of dilated lymphatic channels within the conjunctival lamina propria, lined by flattened endothelium (Figure 2). Underlying this lesion, the conjunctival epithelium showed squamous metaplasia, acanthosis and hyperkeratosis. The final diagnosis of conjunctival lymphangioma was made. Postoperatively, the patient was prescribed topical drops of ofloxacin 3 mg/ml to be used 5 times a day and dexamethasone 1 mg/ml to be used 4 times a day with a progressive tapering schedule.
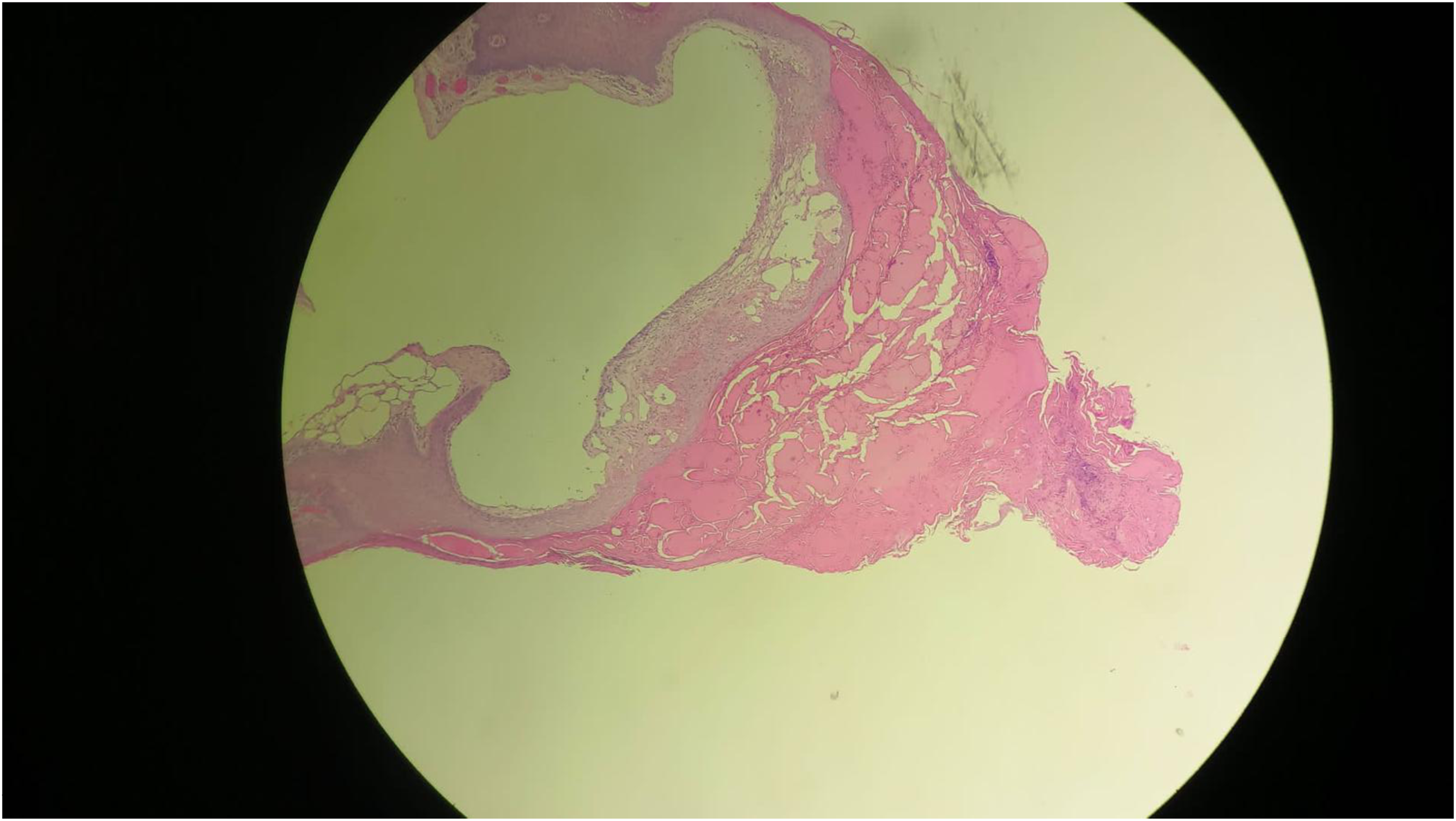
Histopathological findings of the surgically excised lesion (haematoxylin and eosin stain).
One week after the surgical procedure the patient resumed his professional activities. Follow up appointments were scheduled 1 month, 6 months and 1 year after the surgery. On our last observation, one year postoperatively, the patient remains asymptomatic and with no signs of recurrence of the lesion.
Conclusions
Conjunctival lymphangiomas are benign and infrequent lesions that correspond to vascular hamartomas of lymphatic origin. They represent only 1–3% of all orbital masses. 3 They usually present in young patients, with an average age at presentation of 25 years, with an average 3 year duration of symptoms at presentation. 4
Their most common location is the bulbar conjunctiva and they typically present as focal or diffuse bulbar chemosis or as a focal dilatation of lymphatic vessels that resembles an isolated cyst or group of cysts. In some cases, there may be intralesional haemorrhage, which may lead to a sudden increase in lesion size. 5 It may be an exclusively conjunctival lesion or it may represent the surface component of a deep orbital lymphangioma. 6
Patients may develop foreign body sensation, local irritation, tear film disruption and aesthetical concerns, especially in the most prominent lesions. Upper airway infections may exacerbate these symptoms. 7 Lymphangiomas mainly present in the first decade of life although they can also occur throughout life and this diagnosis requires a high index of suspicion. They should be considered in patients with chemosis or conjunctival focal or multifocal lesions refractory to corticosteroid topical therapy and without other known causes.
Surgical excision is the most common approach to this situation, and it can be associated with cryotherapy or amniotic membrane graft depending on the case. However, conservative treatment has also been tried with success in a small number of cases with some reports of spontaneous resolution. 8 There have also been some case reports of successful alternative treatments such as carbon dioxide laser, beta irradiation and liquid nitrogen cryotherapy.4,9,10 Recurrence of the lesion is always a possibility and patient should be monitored.
We reported a case of an atypical presentation of lymphangioma as a conjunctival horn, which represents reactive changes of the tumor's overlying epithelium. To the best of our knowledge, there is only one other published case of a conjunctival lymphangiectasia presenting in this manner. 11 Regarding conjunctival horns, the differential diagnosis includes inflammatory conditions, trauma, chronic irritation, infection or tumors. We found in the literature reports of squamous cell carcinoma of the conjunctiva in an 82 year old patient with a history of chronic sun exposure and in a 46 year-old healthy woman.12,13 There is also a report of a conjunctival malignant melanoma resembling a horn. 14 Benign lesions such as seborrheic keratosis have also been found to be associated with pseudohorn cysts containing keratin and there is one reported case of complete conjunctival and corneal keratinization in a severe case of ocular cicatricial pemphigoid.15,16 There are not many other reports in the literature, as conjunctival horns are rare entity and represent only a very small percentage of ocular surface anomalies.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.