
Abstract
Purpose
This study aimed to compare the effect of intravitreal aflibercept (IVA) and ranibizumab (IVR) on the maximal diameter of the largest intraretinal cyst (mdIRC), indicating chronicity in patients with diabetic cystoid macular edema (CME).
Methods
This retrospective, comparative study included a subgroup of patients from the MARMASIA Study with treatment-naïve diabetic CME who had IVA (IVA group) or IVR (IVR group) on a pro re nata regimen after a loading dose of 3-monthly injections and followed-up for 24 months. Best-corrected visual acuity (logMAR), central macular thickness (CMT, µm), and mdIRC (µm) and their changes during the study period in the IVA and IVR groups were compared.
Results
A total of 175 eyes (65 [37.1%] in IVA and 110 [62.9%] in IVR group) of 113 patients were included in the study analysis. Both groups had statistically significant improvements in BCVA and CMT during the follow-up (p < 0.05 for all), which were comparable between the groups at each time point. However, the mean reduction in mdIRCs was consistently and significantly higher in the IVA group compared to the IVR group at each follow-up examination (F[1, 3.52] = 6.93, p = 0.009).
Conclusion
IVA seems to have a greater impact in reducing cyst sizes than IVR in diabetic CME.
Keywords
Introduction
The most frequent cause of vision impairment in people with diabetic retinopathy (DR) is diabetic macular edema (DME), which affects 30% of people with the condition who have had it for more than 20 years. 1 DME encompasses various types, such as focal/diffuse edema, cystoid macular edema (CME), and serous macular detachment. 1 CME refers to the existence of intraretinal cystoid accumulation of fluid within the macular area. 1
CME typically presents as radial cystoid spaces filled with extracellular fluid, which arises due to impairment of the blood-retina barriers.2,3 Cysts are frequently seen in the central macula, where they take up the area that ordinarily belongs to migratory cells.2,3 These cysts can be observed in multiple retinal layers, commonly at the inner nuclear layer and outer plexiform layer.2,4 Histological investigations have revealed neuronal degeneration accompanied by swelling and necrosis of Müller cell cytoplasm, retinal vascular abnormalities, and CME. 2 The presence of cysts has been identified as an indicator of disease activity, chronicity of DME, and/or structural damage. 5 However, no specific treatment strategies based on the nature, size, or location of the cysts have been reported. Nevertheless, it has been previously observed that empty and large cysts are often associated with advanced disease stages, indicating chronicity. 6
Vascular endothelial growth factor (VEGF) primarily contributes to vascular enlargement and edema observed in various retinal vascular disorders, including diabetic retinopathy and DME. 6 Extensive research has demonstrated the efficacy of intravitreal injection of anti-VEGF agents in inhibiting VEGF and effectively treating DME. 7 Bevacizumab, ranibizumab, and aflibercept are three frequently employed intravitreal anti-VEGF agents for DME treatment. Notably, ranibizumab and aflibercept have obtained approval from the Food and Drug Administration (FDA) for this specific indication and have gained widespread usage.8,9 Aflibercept is a recombinant fusion protein that attaches to all isoforms of VEGF-A, VEGF-B, and placental growth factor (PlGF), whereas ranibizumab is a recombinant humanized monoclonal antibody fragment that specifically attaches to all human VEGF-A isoforms.
To the best of our knowledge, the effect of anti-VEGF treatment on cyst size in diabetic CME has not been previously investigated. Therefore, this study aims to compare the effects of intravitreal aflibercept (IVA) and ranibizumab (IVR) treatments on the largest cyst diameter in previously untreated eyes affected by diabetic CME.
Methods
This multicenter, comparative, retrospective-cohort study is a subgroup analysis of the MARMASIA Study conducted to evaluate real-world outcomes of intravitreal anti-VEGF treatment for DME in Turkey. The design and scope of the MARMASIA Study have been described previously. 10 Briefly, 21 retina specialists from 8 tertiary clinics located on the Asian Side of the Marmara Region of Turkey, i.e., the MARMASIA Study Group, thoroughly reviewed the medical records of 854 DME patients (1372 eyes) treated in a pro-re-nata protocol and followed at least 3 months up to 3 years. The study protocol was approved by the Institutional Review Board of Kocaeli University School of Medicine (No: GOKAEK-2022/07.19), ensuring compliance with ethical guidelines, including the 1964 Declaration of Helsinki and subsequent amendments. Written informed consent was obtained from all patients upon their initial presentation to the respective clinics, indicating their agreement to use their medical information for study analysis. The MARMASIA Study has been registered on ClinicalTrials.gov with the identifier NCT05472376.
Study population
Patients from the MARMASIA Study with treatment naïve diabetic CME, defined based on the report by the European School for Advanced Studies (ESASO) optical coherence tomography (OCT)-based grading of DME 11 were included in the analysis of this study.
The study inclusion criteria were determined as follows: (1) Patients with treatment-naive diabetic CME with a central macular thickness (CMT) equal to or greater than 300 µm; (3) Patients diagnosed with non-proliferative or proliferative DR; (2) Patients who received intravitreal ranibizumab (IVR) or aflibercept (IVA) treatment starting with 3 monthly loading injections and with or without laser therapy or intravitreal steroids (dexamethasone or triamcinolone); (4) Patients who had a minimum follow-up of 24 months with at least four or more annual examination visits.
Patients treated with intravitreal bevacizumab (IVB); patients diagnosed with a retinal disease other than DME, such as age-related macular degeneration or retinal vein occlusion; patients with any other ocular disease, including uveitis, optic nerve disease, or ocular trauma, which may confound the study outcomes; patients with a history of phacoemulsification within one month before the study inclusion; patients with a history of any intraocular surgery including previous pars plana vitrectomy (PPV) for any reason and excluding phacoemulsification; patients who had panretinal, grid, focal, or micropulse laser treatments within the last four months of study inclusion; patients who received more than 3 intravitreal steroid injections during the 24 months follow-up period; and patients who received intravitreal steroid injection before 6 consecutive anti-VEGF treatments were excluded from the analysis of this study.
Baseline and follow-up data
Demographic data, including age, sex, duration and treatment of diabetes mellitus, the time interval of the first 3 monthly loading doses, presence of hypertension, acute myocardial infarction, and cerebrovascular accident, were retrieved and noted. The details of all evaluated demographics were previously given in the first report of the MARMASIA Study Group. 10
Patients underwent complete ophthalmological examination, including best-corrected visual acuity (BCVA), slit-lamp biomicroscopy, dilated fundus examination, and intraocular pressure measurement (IOP) by Goldmann applanation tonometry, OCT (Spectralis [Heidelberg Eng., Heidelberg, Germany], RS-3000 [Nidek, Gamagori, Japan], or RTVue-100 [Optovue Inc., CA, USA] depending on the availability in study centers), and fundus fluorescein angiography (FA) imaging, at baseline, one month after the loading period, and months 6, 12, and 24. In addition, the number of visits and injections over the two years, and if present, any complication due to treatment was noted. All functional and anatomical measurements were conducted according to the standardized protocol outlined by the first report of the MARMASIA Study Group. 10
CMT was automatically determined by the available OCT device in each clinic within a central 1 mm of the presumed fovea location ensured by the clinician. The center region of the retina without inner retinal layers was described as the presumed fovea. 12 At each study visit, the maximal diameter of the largest intraretinal cyst (mdIRC) within 1000 µm distance from the foveal center was measured manually by two independent observers, and the average of the two measurements was taken (Figure 1). Whenever a difference of 10 microns or more was identified between the observers, the measurement was repeated, presumably to verify the accuracy of the results. Measurements were performed on the same cyst each time, and patients with newly formed, larger cysts that could cause confusion were excluded from the study. CMT and mdIRC values from OCT devices other than Spectralis were recalculated using the formulas provided by Pierro L et al. according to Spectralis OCT to correct the differences. 13 Baseline and follow-up data were compared between the eyes treated with IVR (IVR group) and IVA (IVA group).
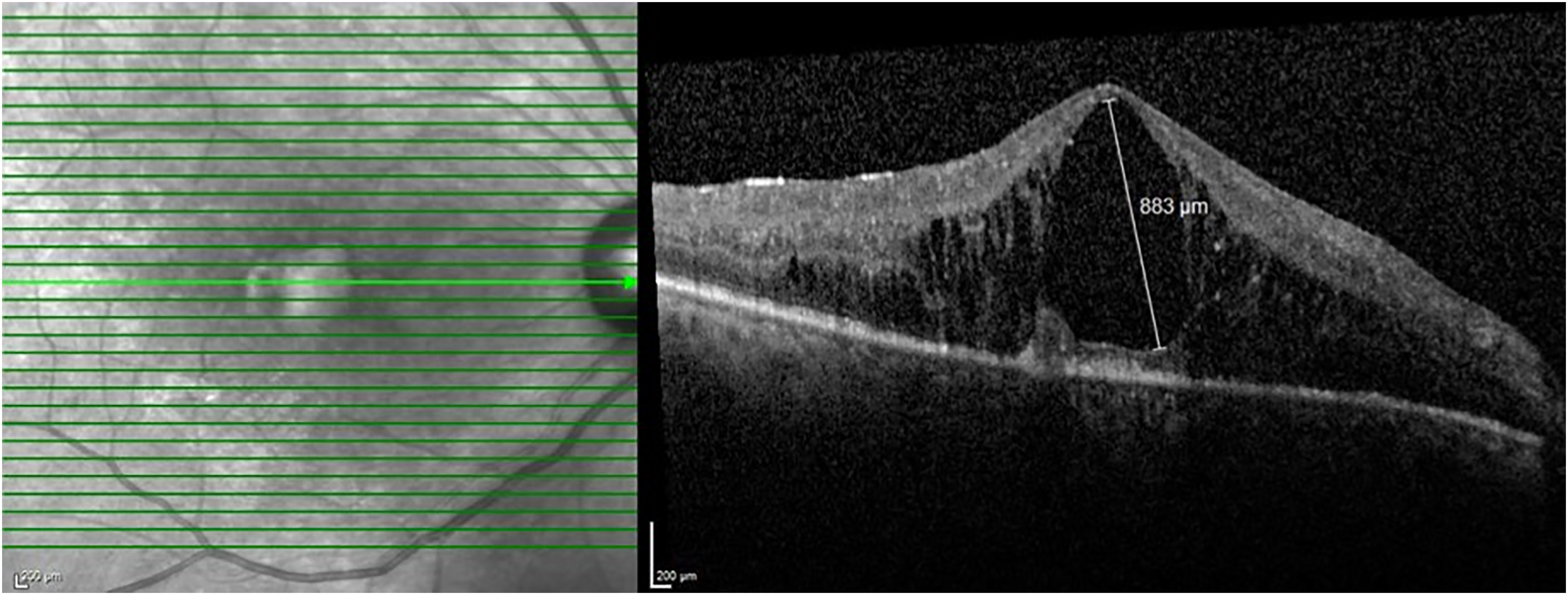
Spectral-domain optical coherence tomography infrared (left) and B-scan (right) images of a 62 years-old male patient included in the study with treatment naïve diabetic cystoid macular edema. Note that the measurement of the cyst diameter (883 µm) was from the largest cyst within 1000 µm of the presumed foveal center and the maximal diameter plane of the cyst, regardless of vertical or horizontal planes. The green arrow in the infrared image indicates the plane of the B-scan image.
Statistical analysis
SPSS software for Windows version 26.0 (IBM Crop., Armonk, NY, USA) was used for statistical analyses. The data distribution was evaluated using histogram graphs and the Shapiro-Wilk test. BCVAs were converted from Snellen to logMAR for statistical analyses, and the logMAR equivalent value for “counting fingers” and “hand motion” were assumed to be 2.10 and 3.10, respectively. Quantitative data were given as mean ± standard deviation and qualitative data were presented as frequency (n) and percentage (%). The independent-samples t-test was used to compare the baseline findings between groups. The chi-square test was used for comparing categorical data between groups. A two-way mixed analysis of variance (ANOVA) test was performed to evaluate the interaction between the treatment group and time on the functional and anatomic parameters evaluated. The assumption of sphericity was assessed with Mauchly's test. If the assumption of sphericity was not met, then epsilon (ε) was calculated according to Huynh-Feldt correction. Bonferroni correction was employed for the pairwise comparisons, and adjusted p-values were given where appropriate. Statistical significance was evaluated at the level of p < 0.05.
Results
A total of 175 eyes (12.7% of 1372 eyes in the original cohort) of 113 patients fulfilling the inclusion criteria (13.2% of 845 patients in the original cohort) were included in the study. The IVR group comprised 110 (70), and the IVA group comprised 65 (43) eyes (patients). The baseline characteristics of the patients are presented in Table 1.
Baseline characteristics of the patients in the study groups.
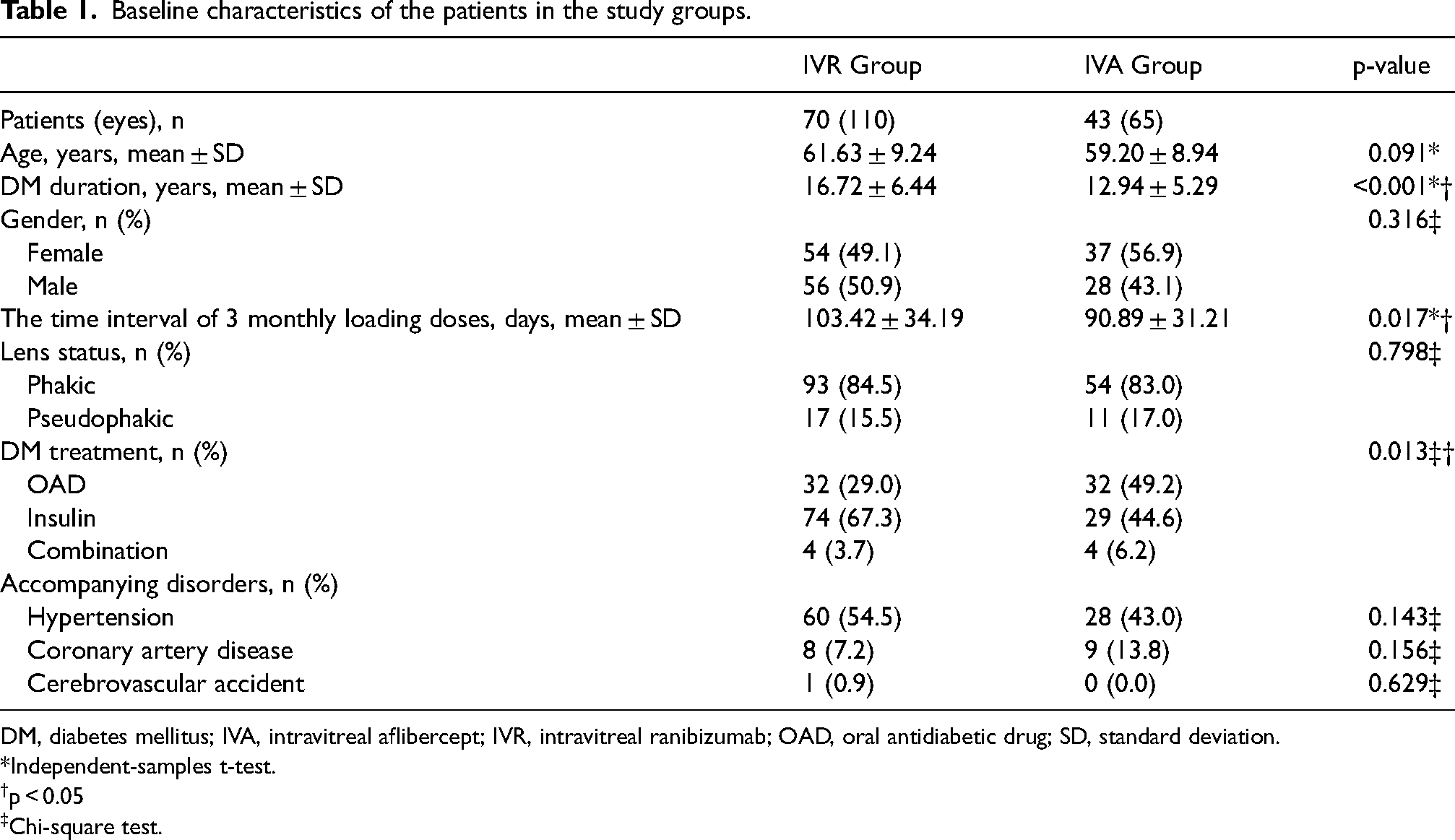
DM, diabetes mellitus; IVA, intravitreal aflibercept; IVR, intravitreal ranibizumab; OAD, oral antidiabetic drug; SD, standard deviation.
Independent-samples t-test.
p < 0.05
Chi-square test.
Visit, intravitreal anti-VEGF injection, and intravitreal steroid injection counts among the groups during the study period were presented in Table 2. IVR group had significantly higher visit counts at all study time points (p < 0.001 for all). In the 12th month, the intravitreal injection counts were higher in the IVA group (5.17 ± 1.22) compared to the IVR group (4.63 ± 1.52) (p = 0.011). However, no significant difference was observed between the groups at the other study time points (p > 0.05). Twenty-four months of intravitreal steroid injection counts were similar among the groups (p = 0.835).
Visit, intravitreal injection, and intravitreal steroid injection counts among the groups during the study period.
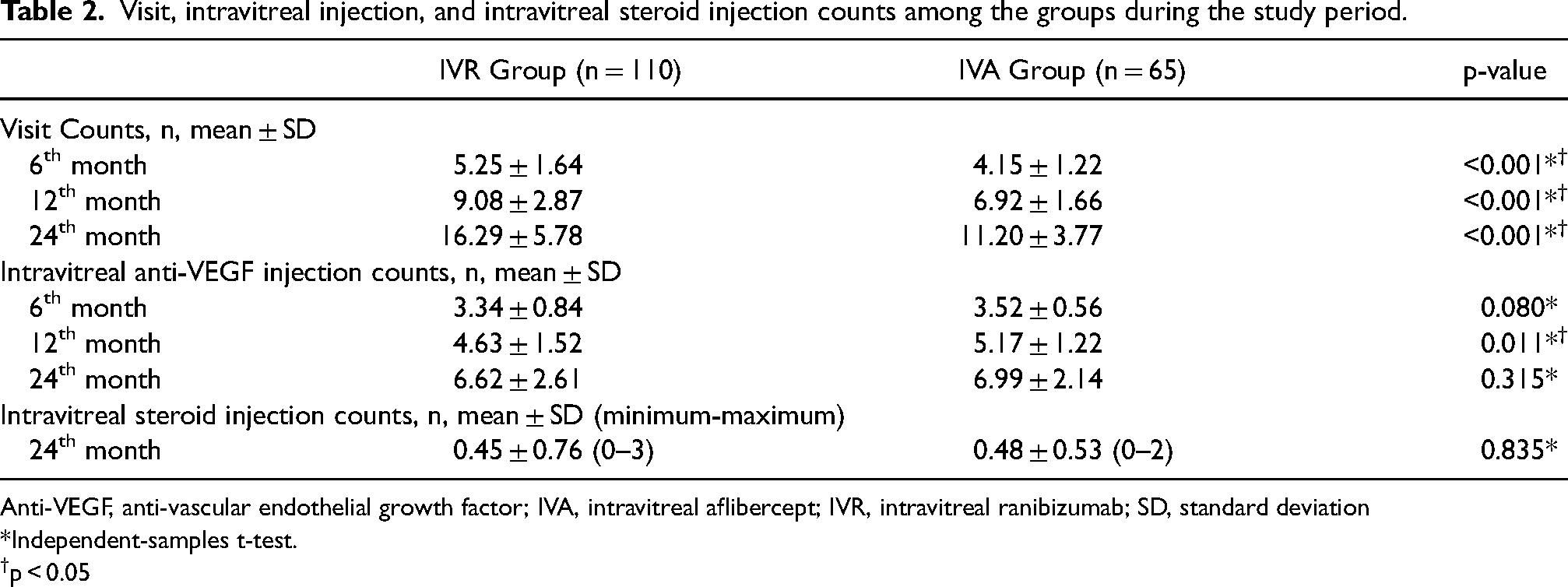
Anti-VEGF, anti-vascular endothelial growth factor; IVA, intravitreal aflibercept; IVR, intravitreal ranibizumab; SD, standard deviation
Independent-samples t-test.
p < 0.05
Visual outcomes
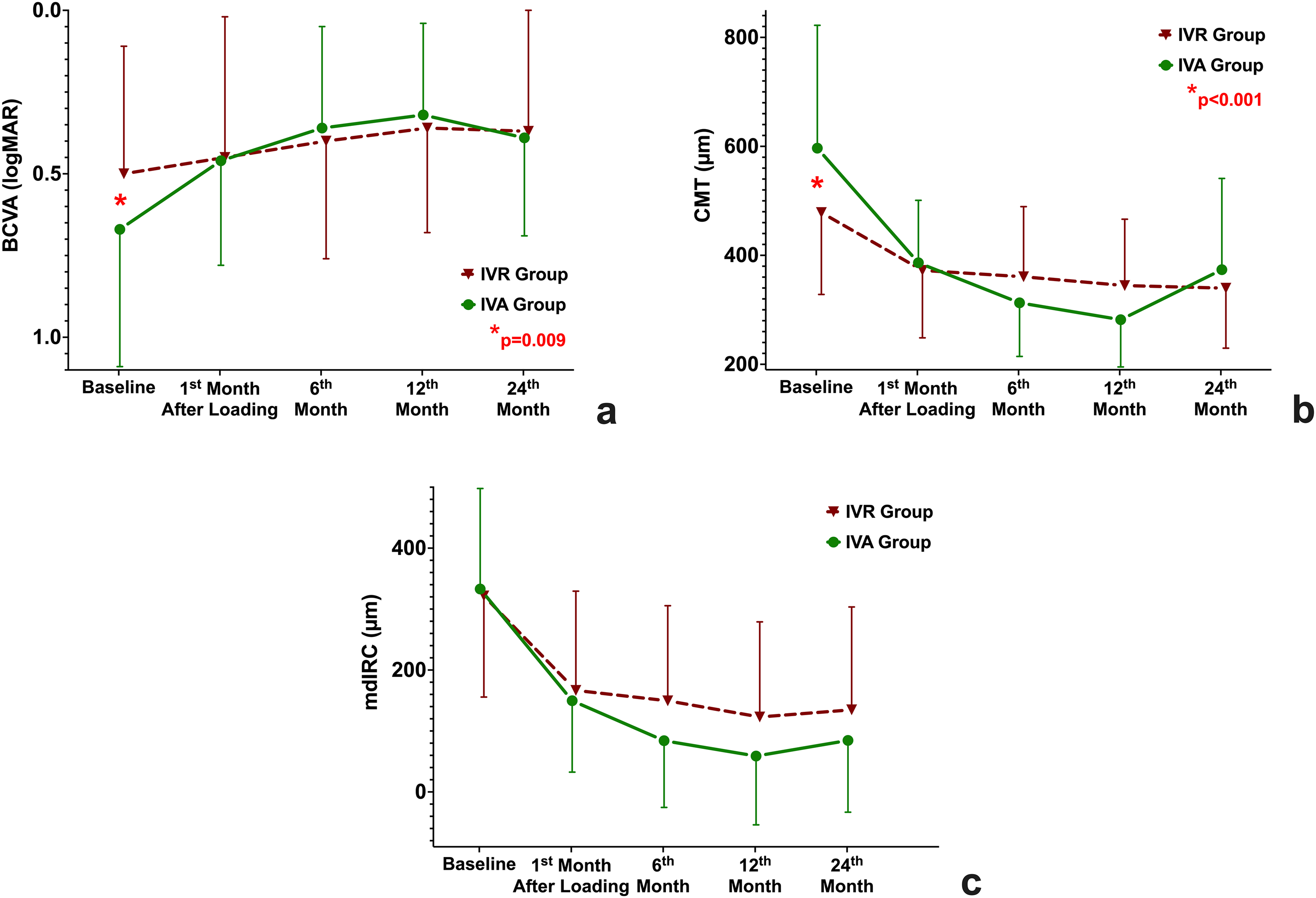
The mean baseline BCVA was 0.50 ± 0.39, logMAR (≈20/63 snellen equivalent) in the IVR group and 0.67 ± 0.42, logMAR (≈20/93 snellen equivalent) in the IVA group (p = 0.009) (Figure 2a). The mean BCVA demonstrated a statistically significant improvement one month after the loading period and 6th, 12th, and 24th months compared to baseline in the IVA group (p < 0.05 for all time points) (Figure 2a). In the IVR group, the mean BCVA was statistically increased for all the time points, except only one month after the loading period (p = 0.116 for month 3, p < 0.05 for all other time points) (Figure 2c). During the follow-up period, there was no statistically significant difference in the mean change in visual acuity between groups (F[1, 2.82] = 0.26, p = 0.61, ε=0.688, partial η2 = 0.001) (Table 3).
Functional and anatomical outcomes in the treatment groups during the study period.
Functional and anatomical outcomes of the groups during the study period.
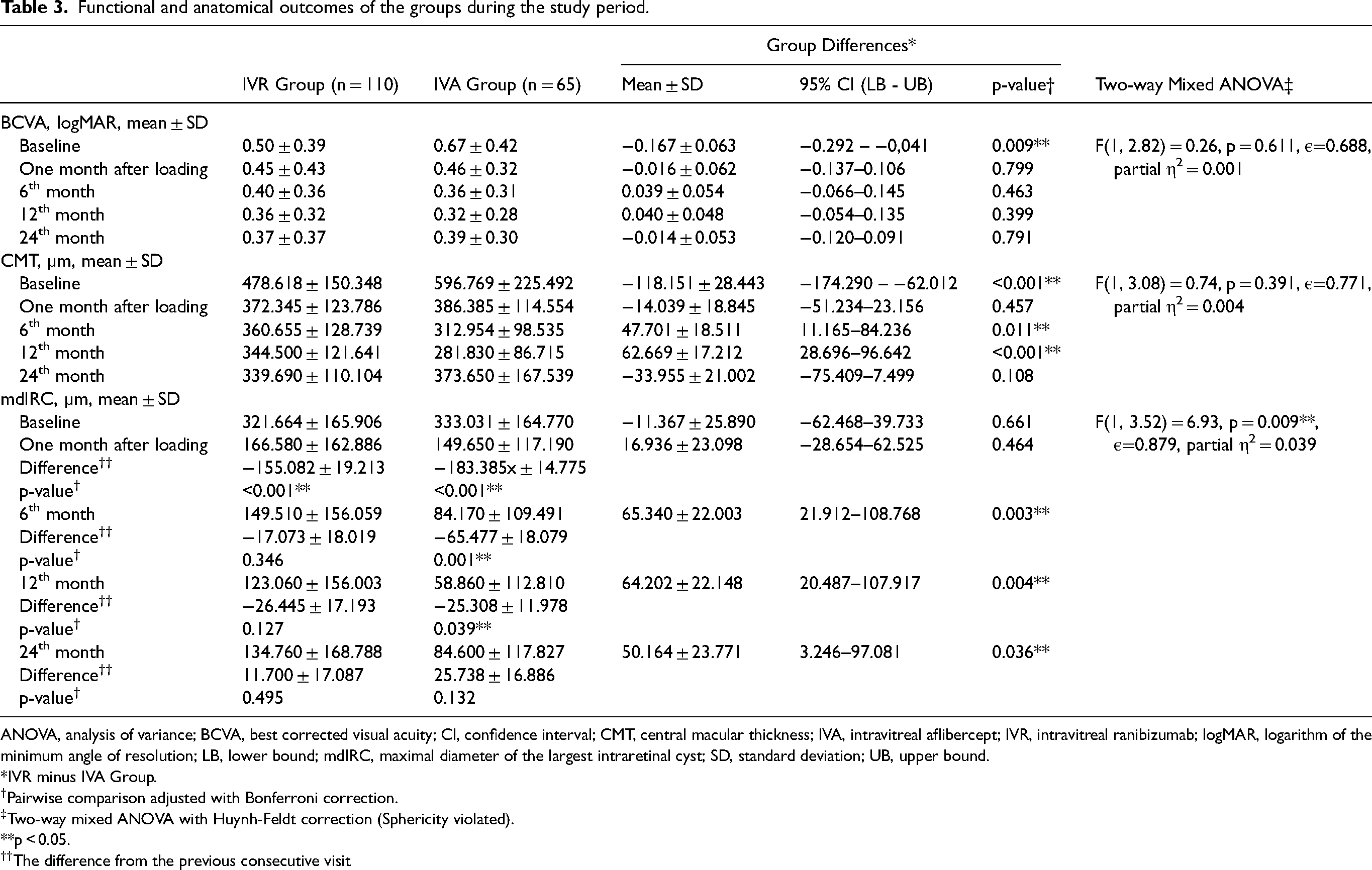
ANOVA, analysis of variance; BCVA, best corrected visual acuity; CI, confidence interval; CMT, central macular thickness; IVA, intravitreal aflibercept; IVR, intravitreal ranibizumab; logMAR, logarithm of the minimum angle of resolution; LB, lower bound; mdIRC, maximal diameter of the largest intraretinal cyst; SD, standard deviation; UB, upper bound.
IVR minus IVA Group.
Pairwise comparison adjusted with Bonferroni correction.
Two-way mixed ANOVA with Huynh-Feldt correction (Sphericity violated).
p < 0.05.
The difference from the previous consecutive visit
Anatomical outcomes
The mean baseline CMT were 478.618 ± 150.348 and 596.769 ± 225.492 µm in the IVR and IVA groups, respectively (p < 0.001). Compared to the baseline, the mean CMT showed statistically significant improvement following treatment at all follow-up visits in both groups (p < 0.001 for all) (Figure 2b). During the study period, there was no significant difference in the mean change in CMT between groups (F[1, 3.08] = 0.74, p = 0.391, ε=0.771, partial η2 = 0.004) (Table 3).
The mean baseline mdIRCs were 321.664 ± 165.906 µm and 333.031 ± 164.770 µm in the IVR and IVA groups, respectively (p = 0.661). The mean mdIRC was decreased one month after the loading period and at the 6th, 12th, and 24th months compared to baseline in both of the treatment groups (p < 0.001 for all time points) (Figure 2c). The two-way mixed ANOVA revealed a statistically significant interaction between the treatment group and time on mdIRC (F[1, 3.52] = 6.93, p = 0.009, ε=0,879, partial η2 = 0,039). mdIRC was statistically significantly greater in the IVR group at 6th (65.340 ± 22.003 µm, p = 0.003), 12th (64.202 ± 22.148 µm, p = 0.004), and 24th (50.164 ± 23.771 µm, p = 0.036) months than the IVA group (Table 3).
Discussion
Aflibercept and ranibizumab have been extensively studied regarding their ability to reduce CMT and improve visual acuity in DME.14–16 However, the impact of these treatments on cyst size in CME has not been thoroughly investigated. Our study compared the effects of IVA and IVR on cyst size in treatment-naive eyes with diabetic CME. During the 24-month follow-up period, the IVA and IVR groups exhibited a statistically significant decrease in CMT. In the IVR group, a significant visual improvement was observed after the 6th month, whereas in the IVA group, a significant visual improvement was noted one month after the loading period. Mean changes in visual acuity and CMT did not differ significantly between the two treatment groups at any time point. Using a two-way mixed ANOVA test, we observed a statistically significant difference in the reduction of the mdIRC between the IVA and IVR groups. Specifically, the IVA group exhibited a more substantial reduction in the mdIRC when compared to the IVR group.
Several comprehensive reviews and theoretical frameworks have already elucidated the pathogenesis of CME.3,17,18 The development of CME involves multiple factors, including increased leakage from retinal vessels and additional pathophysiological mechanisms. It refers to fluid accumulation within the macula, surpassing the compensatory capacity of fluid removal mechanisms during edema formation. The retinal pigment epithelial (RPE) cells actively transfer excess fluid from the retina to the choroid, while retinal Müller cells remove fluid from the retinal interstitial tissue. Dysfunction in the RPE pump, responsible for fluid clearance from the retina, is one of the underlying pathophysiological mechanisms. Histological characteristics of the inner and outer limiting membranes provide insights into the formation of cysts within specific retinal layers during CME. Moreover, the synaptic regions of the outer and inner plexiform layers pose formidable obstacles to fluid flow, causing fluid leakage from the middle and deep capillary plexus and subsequent accumulation in the inner nuclear layer, leading to cyst-like structures. Previous studies have suggested the detrimental impact of cyst formation on ganglion and bipolar cells.19–21 Notably, macular cystoid spaces have been identified as a predictive factor for visual deterioration, with larger cystoid spaces having a more disruptive effect than smaller ones.22–24 While some studies have investigated the relationship between the remaining intact tissue between cysts and visual prognosis, no definitive conclusions have been drawn regarding cyst sizes to date.23–25
In DME, intraretinal cysts serve as important landmarks in OCT imaging A preliminary investigation proposed that massive fused macrocysts in severe and persistent DME could indicate retinal cystoid degeneration and may be linked to malfunction or necrosis of Müller cells. 25 These large cystic spaces have been linked to increased central subfield thickness, a higher incidence of outer retinal damage, macular ischemia, and diffuse macular edema. 25 However, the question remains: What does the size of the cysts or the extent of resudual macular tissue imply in terms of choosing the optimal treatment approach?
Previous research has demonstrated that DME cases with great perifoveal cysts, unresponsive to anti-VEGF therapy, have shown improvement in BCVA upon switching to a dexamethasone implant.19,26 These findings suggest that alternative treatments, such as dexamethasone implants, can lead to positive outcomes for DME patients with sizable cysts that do not respond favorably to anti-VEGF agents. Despite the extensive investigations conducted on the effects of anti-VEGF agents in DME, the impact of these treatments on cyst size has not been adequately explored yet.
Despite studies comparing aflibercept with ranibizumab in chronic and resistant DME, there is currently a lack of research comparing their effectiveness, specifically in CME. Post hoc analyses of Protocol T have indicated that the frequency of chronic persistent DME after two years tended to be lower in the aflibercept group compared to the ranibizumab group. 5 Tsai et al. reported that both aflibercept and ranibizumab improved vision and resolved edema, but aflibercept demonstrated better vision maintenance and fewer subretinal fluid recurrences at 12 months in real-world settings. 27 This has been attributed to aflibercept's potent inhibition of both PlGF and VEGF. Vandekerckhove compared the efficacy of aflibercept and ranibizumab in persistent and recurrent macular edema, reporting that aflibercept was more effective anatomically and functionally. 28 These differences have been attributed to three potential mechanisms. Firstly, aflibercept may exhibit superior VEGF binding affinity, with approximately 100 times stronger binding affinity to VEGF-A than ranibizumab. Secondly, there may be potential tachyphylaxis or tolerance to ranibizumab. However, the most plausible explanation lies in the variations in the pharmacodynamic characteristics of the medications. In addition to VEGF-A, PlGF-1 also plays a role in the pathogenesis of DME. PlGF-1 contributes to diabetic retinal edema by inducing rupture of the outer retinal barrier (RPE junctions) through VEGF receptor 1-mediated mechanisms. Aflibercept, unlike ranibizumab, blocks PlGF in addition to specifically and strongly binding to VEGF receptors 1 and 2, thus inhibiting their activation. Diabetic retinopathy patients exhibit elevated vitreous levels of PlGF-1. Both aflibercept and ranibizumab successfully inhibit vitreous VEGF-A, thus preventing the activation of VEGF receptor 2. Only aflibercept, however, prevents PlGF from binding to and activating either VEGF receptor 1 or 2.
Alsaedi et al. conducted a comparative study between aflibercept and ranibizumab in eyes with persistent macular edema and found that aflibercept resulted in a greater reduction in DME compared to ranibizumab. 29 Similarly, Zu et al. compared the effects of aflibercept and triamcinolone on CME and concluded that intravitreal aflibercept injection was significantly more effective in treating CME than triamcinolone acetonide injection. 30 The study also reported lower levels of inflammatory cytokines such as VEGF, MCP-1, and ANGPTL4 in the aqueous humor of the aflibercept group compared to the triamcinolone group. The authors ascribed this observation to the capability of aflibercept to bind to VEGF receptors and impede downstream signaling pathways, thereby hindering VEGF-mediated chemotaxis of inflammatory cells and decreasing the levels of VEGF, MCP-1, and ANGPTL4. Cysts in CME, a chronic and resistant form of edema, often require repeated anti-VEGF injections. In our study, we observed that cyst diameters showed a greater regression rate in the IVA group, despite similar numbers of injections. Additionally, the number of steroid injections was similar in both groups. The strong affinity of aflibercept for VEGF, its ability to bind to different regions of VEGF, and its inhibition of PIGF may contribute to these findings.
Our study has several limitations, including its retrospective design and a limited number of patients. Furthermore, we only measured the greatest diameter of the largest IRC at a fixed distance of 1000 µm from the center of the fovea. We did not determine the specific retinal layer where the cysts were located, and accordingly, a detailed layer-specific measurement was not performed. The measurements were conducted using OCT B-scan, and evaluations were not performed using en-face OCT images. The BCVA and CMT measurements at baseline exhibited statistically significant differences between the groups, consistent with the nature of real-life studies. The study did not evaluate the effect of treatment groups on different types of DME. Additionally, future studies need to do volumetric study of the cysts taking in consideration size and number of the cysts.
Conclusion
In this study, we made a novel observation that IVA treatment resulted in a greater improvement in the mdIRC, indicative of chronicity, compared to IVR. These findings align with the results from the chronic persistent edema subgroup analysis of Protocol T. The present study makes a notable scholarly contribution to the existing literature, warranting further exploration with expanded patient cohorts and rigorous, comprehensive investigations. Given the limitations of our study, there is a need for more comprehensive randomized controlled prospective studies to evaluate the effect of IVA and IVR on mdIRC in CME.
Footnotes
Acknowledgements
All authors certify that this work is original and has not been published elsewhere, nor is it currently under consideration for publication anywhere. Also, none of the authors have any conflicts of interest to disclose. No funding was received for conducting this study. The authors have no financial interests to report.
Code availability
Not applicable.
Data availability
The data supporting this study's findings are available from the corresponding author (EÖT) upon reasonable request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards (GOKAEK-2022/07.19)
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Informed consent was obtained from all individual participants included in the study.