
Abstract
Introduction
We report a case of early-onset lipemia retinalis secondary to the FLAG-Ida protocol in the treatment of acute myeloid leukemia (AML) in an 11-year-old girl.
Case Report
An 11-year-old patient, diagnosed with AML at four months old, experienced a relapse and was treated with the FLAG-Ida protocol (fludarabine, idarubicin, granulocyte-colony stimulating factor, and high-dose cytarabine). Prior to allogeneic stem cell transplantation, she underwent a pre-transplantation eye examination. The patient exhibited normal visual acuity in both eyes. Fundus examination revealed cream-white retinal vessels and a salmon-pink retina, indicative of grade 3 lipemia retinalis. Laboratory tests, normal before treatment initiation, showed significantly elevated serum cholesterol (727.6 mg/dL) and triglyceride (6015.6 mg/dL) levels post-treatment. After receiving fenofibrate, these levels decreased markedly, and the retinal vessels normalized on follow-up fundus examination.
Conclusion
Lipemia retinalis, characterized by creamy-white retinal vessels resulting from hypertriglyceridemia, can develop as a secondary condition to chemotherapy. Early detection and treatment of hyperlipidemia are crucial to prevent severe ocular and systemic complications. This case highlights the importance of monitoring lipid levels and conducting thorough ophthalmologic examinations in patients undergoing chemotherapy.
Keywords
Introduction
Lipemia retinalis is a rare ocular finding associated with elevated serum cholesterol or triglyceride levels. It is considered an important indicator of hyperlipidemia, which contributes to early vascular atherosclerosis. The FLAG-Ida protocol, which includes fludarabine, cytarabine, granulocyte colony-stimulating factor (G-CSF), and idarubicin, is known to be an effective chemotherapy option for relapsed or high-risk childhood leukemias. This case represents the first documented example in the literature of lipemia retinalis resulting from the use of the FLAG-Ida protocol in the treatment of acute myeloid leukemia. The findings not only highlight an important systemic complication but also suggest that lipemia retinalis may be an early diagnostic clue in identifying underlying metabolic disturbances.
Case description
An 11-year-old girl was diagnosed with acute myeloid leukemia at the age of 4 months. Relapse was detected while being followed up on in remission. Before our ophthalmologic examination, the patient had been commenced on a FLAG-Ida protocol (fludarabine, idarubicin, granulocyte-colony stimulating factor, and high-dose cytarabine). An allogeneic stem cell transplantation decision was made for the patient, who was in remission after two cycles of treatment. She was referred to our clinic for a pre-transplantation eye examination. The patient demonstrated normal visual acuity in both eyes. On examination, her pupils were isochoric, the corneas were transparent, and intraocular pressures were within normal limits. Fundus examination revealed a color change in all retinal vessels and a salmon-pink retina was observed in both the left and right posterior poles (Figure 1). Spectral domain-optic coherence tomography (SD-OCT) (Spectralis; Heidelberg Engineering, Heidelberg, Germany) revealed high reflective points in the inner retinal layers (Figure 2a). Following this assessment, we determined that the patient had lipemia retinalis. Retinal fundus fluorescein angiography showed normal vascular flow bilaterally.
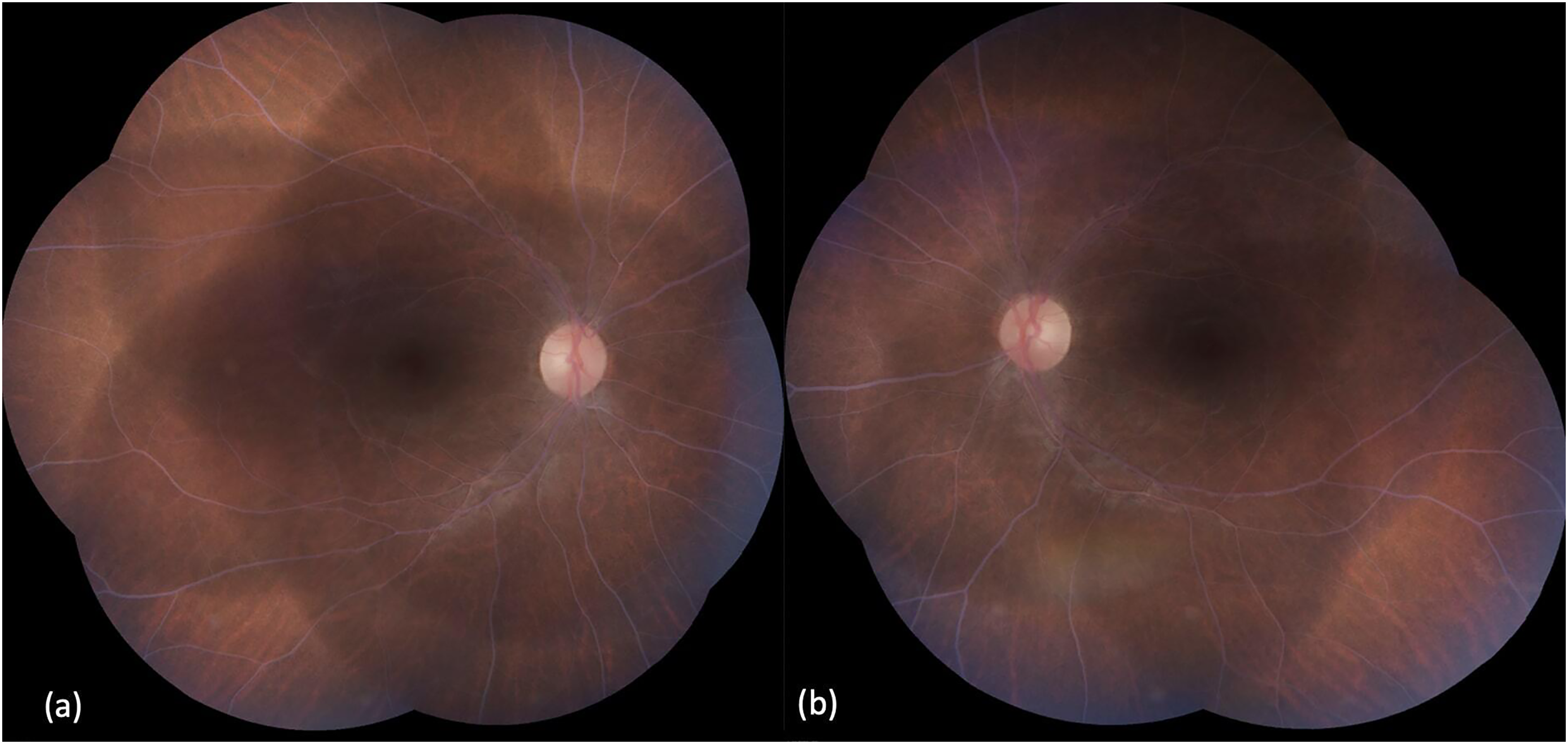
Fundus photograph of the right (a) and left (b) eye, depicting grade 3 lipemia retinalis. All vessels appear creamy white in color, making it difficult to distinguish between arteries and veins.
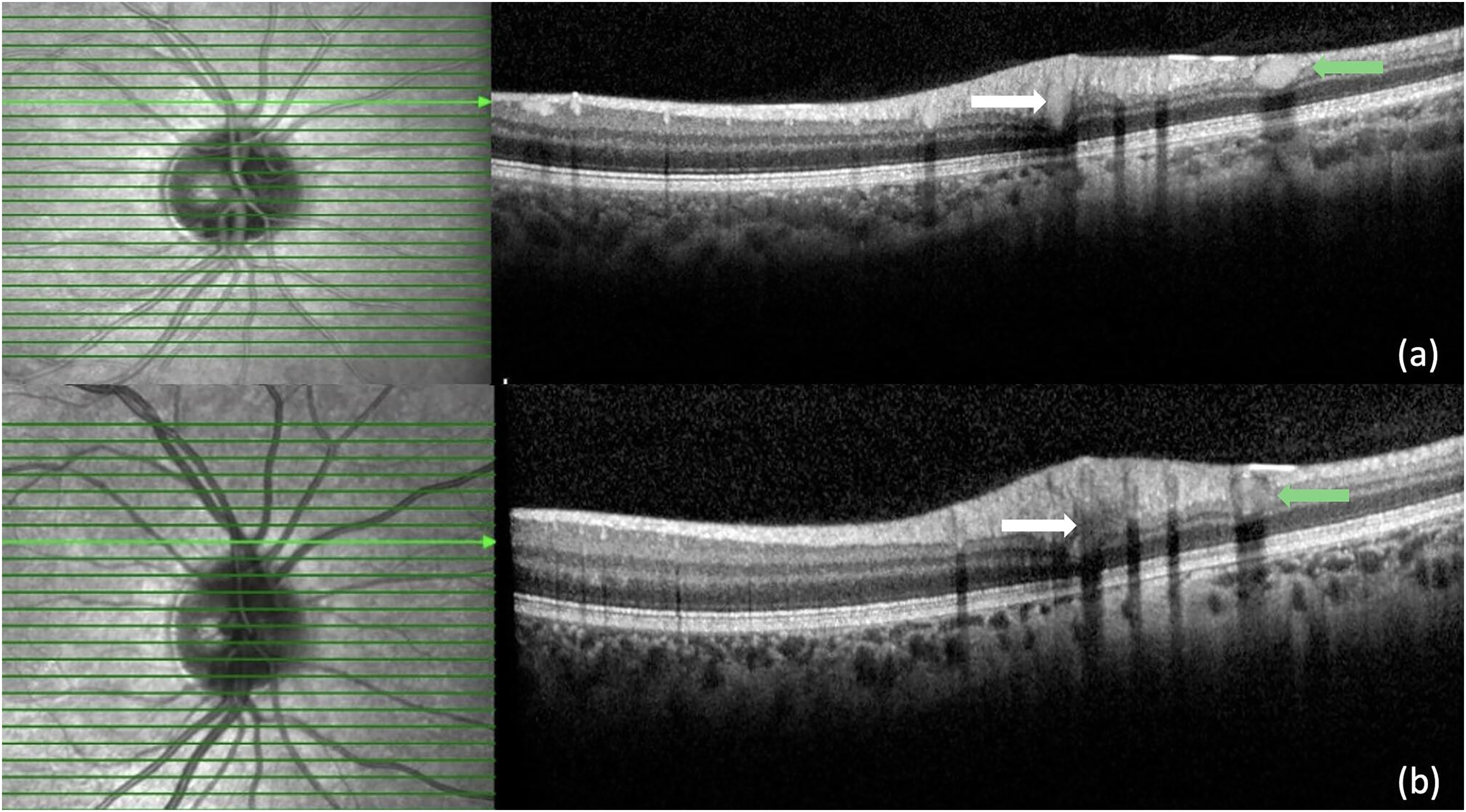
Spectral-domain optical coherence tomography images reveal hyperreflective spots accumulated especially in the retinal vessels (a). Spectral-domain optical coherence tomography image taken after the 10th day of treatment shows a remarkable decrease in hyperreflective spots on the retina (b). Hyperreflective spots indicated by white and green arrows indicate intravascular lipid accumulation.
Before starting treatment, the patient's routine blood test revealed a cholesterol level of 131.2 mg/dL and a triglyceride level of 89.8 mg/dL, both within normal limits. However, laboratory evaluation after treatment showed that the total serum cholesterol level had increased to 727.6 mg/dL (normal range: 120–220 mg/dL) and the triglyceride level to 6015.6 mg/dL (normal range: 50–149 mg/dL). Following these results, the patient began using fenofibrate (Lipanthyl® 267 mg capsules), and her blood lipid levels were tested again 10 days later. The laboratory examination revealed decreases in cholesterol (265 mg/dL) and triglyceride (743 mg/dL) levels. During follow-up, retinal vessels were visible in the color fundus image (Figure 3). SD-OCT showed a remarkable reduction in hyperreflective spots in the retina (Figure 2b).
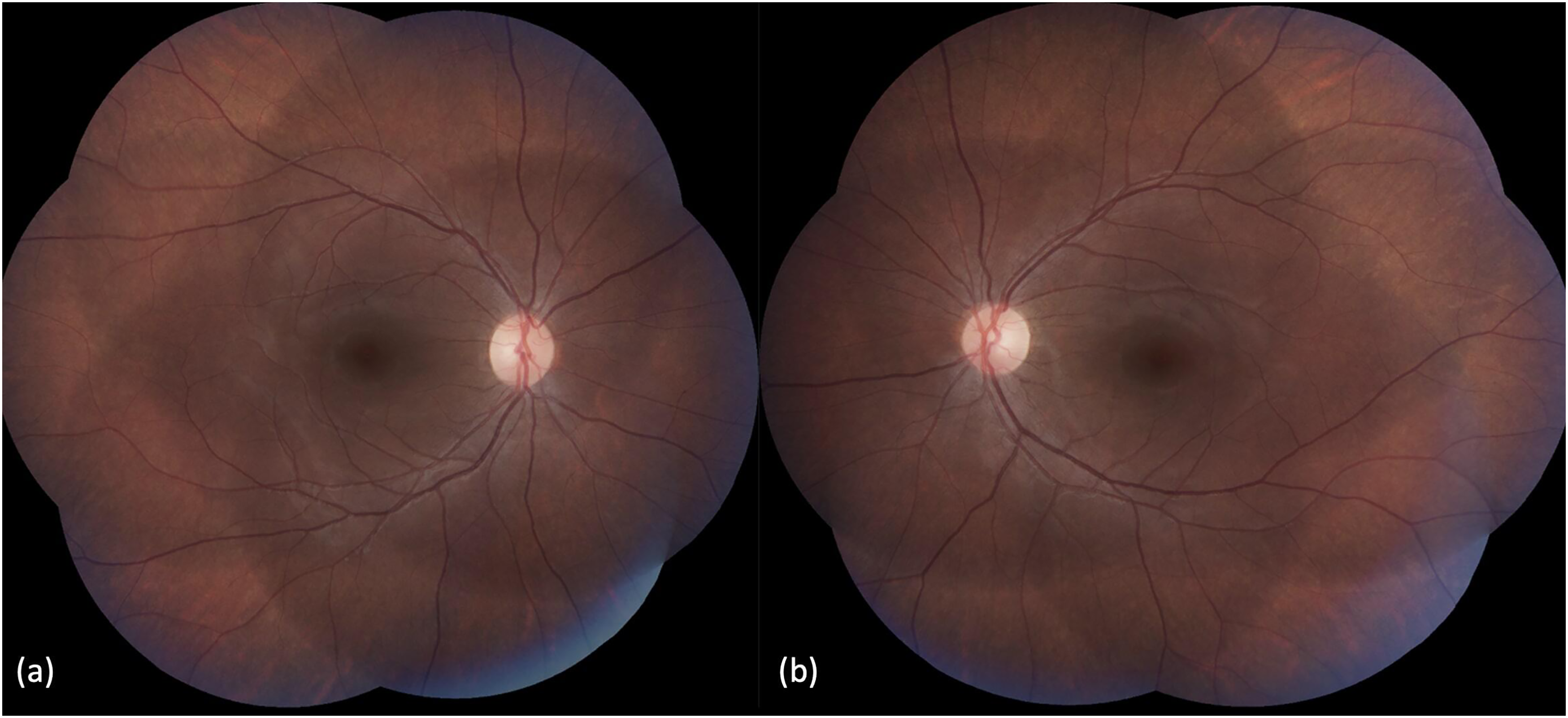
Fundus photograph of the right (a) and left (b) eye, captured on the 10th day follow-up, showing a return to normal in retinal vessels after lipid-lowering therapy.
The patient did not have abdominal pain or skin involvement. Amylase and lipase levels remained within normal limits throughout follow-up. After a detailed pediatric examination and tests, other causes of hyperlipidemia were excluded. The lipid profiles of both the mother and father were within normal ranges; therefore, drug-induced hypertriglyceridemia was primarily considered. The patient underwent allogeneic stem cell transplantation shortly after discontinuing fenofibrate (Lipanthyl® 267 mg capsule) treatment. During long-term follow-up, there were no signs of hyperlipidemia or related ocular findings.
Conclusion
Lipemia retinalis is characterized by cream-white retinal blood vessels in patients with hypertriglyceridemia. 1 When triglyceride levels exceed 1000 mg/dl, it is called chylomicronemia syndrome. Components of this syndrome include xanthomas of the skin (40%), lipemia retinalis (23%), and recurrent abdominal pain/pancreatitis (63%). 1 Depending on the examination findings, early, moderate, and marked classifications can be made. In the early (grade 1) stage, white cream-colored vessels begin to be observed in the peripheral retina. In the moderate (grade 2) stage, white cream veins are also found around the optic disc. In the marked (grade 3) stage, the salmon pink color of the retina and cream color of all arteries and veins are characteristic. 1 In our patient, the fundus image was compatible with grade 3, marked lipemia retinalis. SD- OCT shows hyperreflective material inside the vessel lumen in the ganglion cell, inner plexiform, and outer plexiform layers, in addition to vascular involvement of lipemia retinalis. Extravasated lipid materials may represent hyperreflective dots in the retinal layers. 2
Other ocular findings reported in hyperlipoproteinemias include xanthelasma, lipid keratopathy, retinal artery vein occlusion, ischemic optic neuropathy, cataracts, and dry eye. 3 The reason why lipemia retinalis was not observed in each case with high triglyceride levels was attributed to the change in hematocrit value or the interpersonal variation of retinal and choroidal vessel translucency.
Any defect in the lipid metabolism pathway in congenital hyperlipidemia causes changes in blood lipid values. Hypertriglyceridemia, which may be inherited, is an autosomal recessive condition with an incidence of less than 1 in 1,000,000. On the other hand, lipemia retinalis may develop secondary to diabetes, hypothyroidism, kidney and liver diseases, multiple myeloma, drug use (such as glucocorticoids or oral contraceptives), and alcohol use. 4
Genetically, APOC2 deficiency, LPL deficiency, and mutations in endogenous circulating LPL inhibitors are responsible. These mutations prevent proper chylomicron clearance from the blood, leading to high levels
Hypertriglyceridemia and low LDL and HDL values may be seen in hematological malignancies. Severe hypertriglyceridemia (>1000 mg/dL) is a well-known side effect of induction chemotherapy in acute leukemia. This is usually secondary to the combination of L-asparaginase and glucocorticoids, both of which are essential drugs at this stage of treatment. There are two cases reported in the literature of altered lipid profile irregularities after steroid treatment.5,6 No cases of lipemia retinalis have been reported due to the FLAG-Ida protocol (fludarabine, idarubicin, granulocyte-colony stimulating factor, and high-dose cytarabine) used in the treating of AML. However, it is important to recognize that the absence of previously reported cases does not rule out the possibility of a drug-induced cause, particularly in the context of a complex treatment protokol. In our case, lipid levels, which were normal before chemotherapy treatment, increased significantly after treatment. The temporal relationship between the initiation of chemotherapy and the development of lipemia retinalis strongly suggests a drug-induced etiology
Hypertriglyceridemia can be managed with lipid-lowering therapies, exercise, and lifestyle changes. First-line medications include fibric acid derivatives (fibrates). In cases with high blood lipid levels, comprehensive examinations of the cardiovascular, integumentary, and ophthalmologic systems are vital. These patients are at increased risk of coronary artery disease, stroke, myocardial infarction, pancreatitis, and retinal artery and vein occlusion.1,10 Therefore, it is crucial to consider the potential role of medications in the development of lipemia retinalis, especially in patients undergoing treatments known to impact lipid metabolism. Lipemia retinalis is important not only for ophthalmology but also for identifying underlying genetic and metabolic disorders. This case highlights the need for careful monitoring of hyperlipidemia in patients undergoing similar chemotherapy protocols. A multidisciplinary approach is critical for rapid detection and intervention, helping to prevent serious ocular and systemic complications. In addition, patients should adopt lifestyle changes and undergo genetic assessment to inform long-term management strategies.
Footnotes
Additional contributions
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patients have given their consent for their images and other clinical information to be reported in the journal.
Data availability
Data sharing is not applicable to this article as no datasets were generated or analyzed during the current study.
The study was conducted at the Pediatric Ophthalmology Unit, Medipol Mega University Faculty of Medicine, Istanbul, Turkey.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.