
Abstract
Refractive surgery is one of the most commonly performed elective procedures in ophthalmology; it is mostly performed in patients who are older than 18 years of age. This routine procedure has been time-tested and is proven to be both safe and effective in adults. However, little is known about the safety and efficacy of refractive surgery in pediatric patients. Granted, refractive surgery should not be used in kids merely for the purpose of avoiding spectacles wear, but it can be of valuable help is preserving vision in patients with amblyopia and accommodative esotropia who otherwise couldn't comply with traditional management options. Refractive surgery in pediatric patients is a complex and challenging field due to the unique characteristics of their developing eyes. This review article aims to provide an overview of the current literature on refractive surgery in pediatric patients, focusing on the different surgical options, the advantages and disadvantages of each procedure.
Keywords
Introduction
The use of refractive surgery in pediatric patients has been limited since it was first introduced in the 1990's. 1 When it was first used in pediatric population, the goal of this therapeutic refractive surgery was to preserve vision and prevent the progression of amblyopia, in contrast to elective refractive surgery in adults where it aims to improve quality of life by eliminating the need for glasses wear. 2 The first study on refractive surgery in children was published in 1995, and it was initially used for children with high anisometropia or bilateral high emmetropia who otherwise couldn't comply with traditional management such as patching, penalization, spectacles, or contact lenses. 3 Generally speaking, two categories of pediatric refractive surgery can be recognized; the first is excimer laser, which includes surface treatments with Photorefractive Keratectomy (PRK), Laser-assisted Subepithelial Keratomileusis (LASEK) as well as Flap-based treatments Laser-assisted In situ Keratomileusis (LASIK). The second category is Intraocular Refractive Surgery with intraocular lens (IOL) implantation or refractive lens exchange.2,4 Performing refractive surgery in children has its own challenges and obstacles, making it much more complex than refractive surgery in adults. The cooperation of the pediatric group is generally limited; thus, the children need to be generally sedated when performing the surgery. 5 Additionally, postoperative care is difficult as they require constant monitoring and possibly eye patching in the early post operative period during the healing of epithelium or flap, in addition to the difficulty of performing a slit lamp exam in young children. 6
Due to the ongoing debate in this field, and the need for this intervention in special cases of amblyopia, there is a crucial need to invest more in this research to bridge the gap in the literature and monitor the constant progress that is being made in this topic. 7 We sought to offer a comprehensive summarization and an update on the available refractive surgery options in pediatric population, a comparison between the surgical techniques, and possible outcomes.
Methodology
A search was conducted using 3 different databases: PubMed, Google Scholar, and Scopus. We searched using keywords: “Refractive Surgical Procedures” OR “Refractive Surgeries” OR “Corneal surgery” OR “Lens Implantation” OR “Lens extraction” OR “Photorefractive Keratectomy” OR “PRK” OR “Laser-assisted Subepithelial Keratomileusis” OR “LASEK” OR “Laser-assisted In situ Keratomileusis” OR “LASIK” OR “Excimer laser” AND “pediatric” OR “Children”, Afterward, a refined selection of the articles was performed following these criteria: Randomized Clinical Trials (RCTs) and Non-randomized Studies of Intervention (NRSI), studies done on population in the age interval 18 years and below, original articles whose aim was to evaluate refractive surgeries, article in English
Laser-assisted refractive surgery
Excimer laser correction of refractive errors was shown to be both practical and safe in adults. 8 Pediatric therapeutic laser refractive surgery has different goals than adult elective laser refractive surgery. Correcting a child's refractive defect may not be necessary because spectacle independence is not a primary issue for children. What matters most is that the refractive error is sufficiently rectified to allow adequate visual growth and avoid amblyopia in one or both eyes. 9 lASIK entails the creation of a corneal stromal flap using a mechanical blade or blade-equivalent laser methodology. After reshaping of the corneal stroma to correct ametropia, the flap is repositioned and is held in place by initially tenuous, natural biomechanical bonds. 10 However, the surface-ablation procedures PRK and LASEK eliminate the potential flap complications because they do not require the creation of a stromal flap, so PRK and LASEK have been widely preferred over LASIK to avoid complications such as dislocation and striae, as well as the difficulty of checking the LASIK flap in children after surgery.9,10
Indications
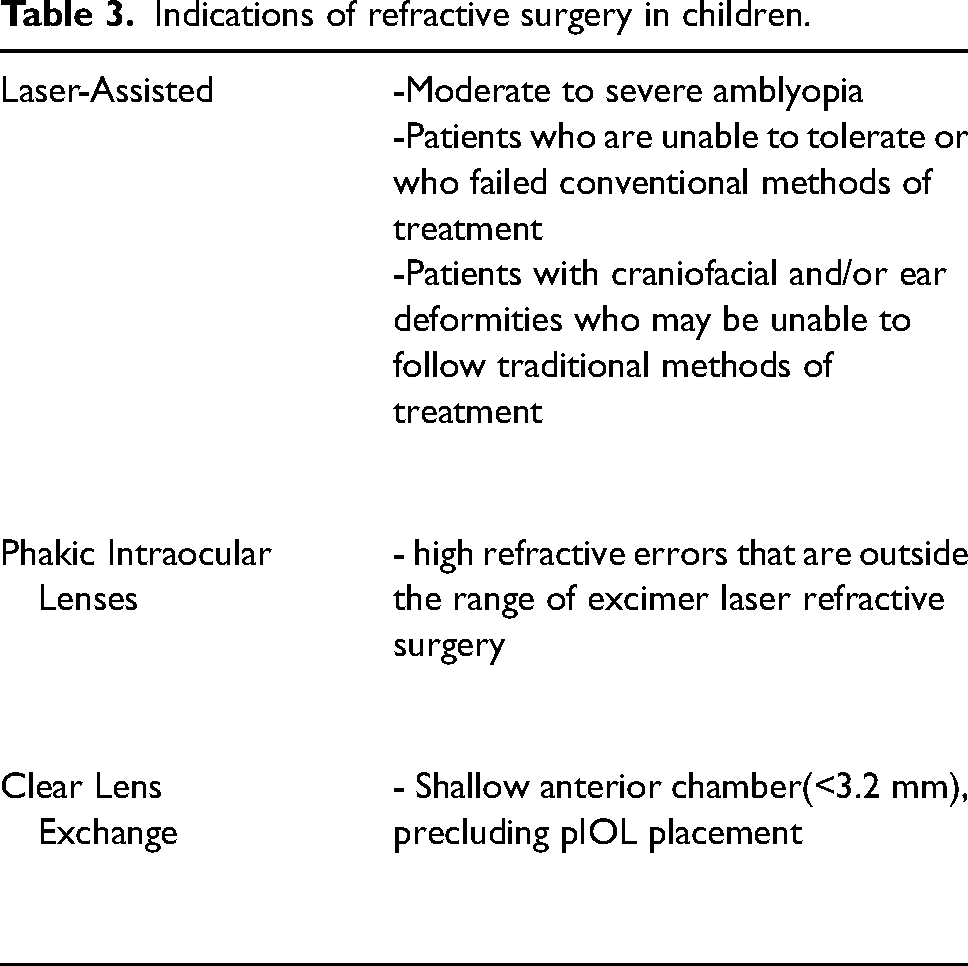
In addition to the usual indications of using excimer laser in adults, which include the absence of glaucoma, uveitis, recurrent conjunctivitis, tear film insufficiency, and endothelial dysfunction/ corneal dystrophy. There are specific indications of excimer laser for children, including amblyopia in the candidate eye equal to 2-optotype lines or worse; patients who are unable to tolerate or who failed conventional methods of treatment, in addition to patients with craniofacial and/or ear deformities who may be unable to follow traditional methods of treatment. Children with neurobehavioral disorders may be hesitant to wear anything on their heads or faces, making it difficult for them to comply with spectacles.9–13
Outcome
Regarding refractive error outcomes, in 2000, Agarwal et al. analyzed 16 eyes that underwent LASIK for high myopia. 14 The study showed significant improvement in the mean spherical equivalent [SE] from −14.88 ± 3.69 D to −1.44 ± 1.14 D. In addition, 7 out of the 16 eyes (43.7%) reached 1.00 D or less of the spherical goal refraction. 14 In 2004, O'Keefe et al. conducted a case-series study to evaluate the efficacy and safety of LASIK in 7 eyes with high myopic ranging from −5.00 to −16 D. At 2 years, 5/7 (83.3%) children showed a significant reduction in [SE] ranging from plano to 6.75 D. 15
When it comes to non-flap-based surface-ablation procedures PRK and LASEK, a case-control study done by Autrata et al. (2004) that analyzed 27 eyes of myopic amblyopic children (13 eyes treated by PRK and 14 treated by LASEK), the authors revealed that [SE] improved from −8.25 ± 2.37 D preoperative to −1.48 ± 1.13 D after 2 years postoperatively, and (53%) of the 27 eyes were within ±1.00 D for the target refraction. 16 In 2005, Tychsen et al. conducted a study on thirty-six eyes with amblyopia that had been treated by laser treatment (18 eyes by LASEK, 18 eyes by PRK) for large magnitude ametropia mean [SE] preoperatively was −11.48 D in 35/36 of the eyes, and only one patient with SE +5.87 D. In this study, the author reported that (89%) of the children achieved spherical goal refraction by ± 1.00 D, while the remaining (11%) reached 2.00 D of the spherical goal refraction. 10
In 2006, s case–control study was done by Paysse et al. to assess PRK effect on myopic and hyperopic anisometropia for 11 children (8/11 have myopic eyes). 12 They reported that refraction changed from −13.70 ± 3.77 D in the myopic group and +4.75 ± 0.50 D for the hyperopic group to −3.55 ± 2.2.5 D and +1.4 ± 1.07 D in the myopic and hyperopic group, respectively. Only (25%) of the myopic group achieved 1.00 D of the target refraction, and (63%) achieved 2.00 D. On the other hand, in the hyperopic group, 2 eyes were within 1.00 D of the target, and 1 had peripheral anterior corneal stromal haze; hence the patient achieved 2.00 D of the target. 12 A similar pattern of results was obtained by Tychsen and Hoekel, 2006, 14 which assessed 18 eyes of high bilateral myopic children with neurobehavioral disorders who underwent LASEK, where they found that (89%) of eyes achieved ± 1.00 D of spherical goal refraction. 17
Later in 2007, according to Yin et al., when authors investigated the outcome of 42 eyes with high hyperopic anisometropic amblyopia and 32 patients with high myopic anisometropic amblyopia following LASIK surgery, the mean preoperative [SE] refraction of the operated eyes was +6.41 ± 1.28 D in the hyperopic group and - 10.49 ± 4.31 D in the myopic group. Postoperatively, the reduction of the mean [SE] was statistically significant as it became +0.6 ± 0.8 D in the hyperopic group and −1.63 ± 2 D in the myopic group. 18 This comes in line with Astle et al. (2008) study, which assessed the long-term outcome of 56 eyes after PRK/LASEK, a remarkable improvement of [SE] was noticed from −10.40 D preoperatively to −1.73 D postoperatively. 11 However, in a study done by Utine et al. (2008), which involved 32 eyes with hyperopic anisometropic amblyopia that underwent LASIK surgery, the mean [SE] reduced after surgery from +5.17 ± 1.65 D to +1.39 ± 1.21 D after refractive surgery. 19
Lin et al. (2009) conducted a study involving 24 eyes with high unilateral anisometropic amblyopia that underwent LASIK surgery (19 myopia and 5 hyperopia). They reported improvement in [SE] from −8.01 ± 2.70 D to −1.32 ± 2.47 D in the myopic group and from +7.40 ± 1.73 D to +3.15 ± 0.86 D in the hyperopic group. Moreover, 12 of the 19 patients in the myopic group were within 1.00 D of the target [SE]. 20 Similarly, in 2010, a study evaluated the outcome of LASIK in 18 children with myopic anisometropia done by Ghanem et al., (2010), where they found that (55.6%) of the children achieved 1.00 D of the spherical goal at 2 years post-surgery, and there was a great reduction in the mean [SE] as well from −9.25 ± 3.43 D to −1.50 ± 1.23 D. 21
Recent case series studies were conducted from 2017–2021. In 2017, Zhang and Yu evaluated the effects of FS-LASIK and small-incision lenticule extraction (SMILE) in 33 unilateral highly myopic amblyopic eyes (only 3 underwent SMILE). The study shows a significant reduction in the mean [SE] from −10.00 ± 2.39 D to −0.60 ± 1.43 at 8 months after the refractive procedure. 22 Ram et al., 2019 measured long-term corneal outcomes following PRK in 12 eyes (10 myopic, 2 hyperopic). The preoperative [SE] ranged from −13.00 to −6.25 D in the myopic eyes and +5.25 to +6.00 D in the hyperopic eyes. Postoperatively, there was a great improvement in [SE], ranging from −8.38 to +1.25 D in the myopic eyes and +2.50 in the hyperopic eyes. 23
Kulikova et al., 2020 analyzed the clinical outcome of femtosecond LASIK (FSLASIK) in 24 kid with hyperopic anisometropic amblyopia. The study showed that mean [SE] before surgery was +3.90 ± 1.60 D, and after surgery was within ±0.50 D in (31%) of the patients, ± 1.00 D and ±2.00 D in (38%) and (92%), respectively. 24 lastly, in Samir et al. (2021) study reported remarkable improvement in [SE] from −7.07 ± 1.45 D to −0.88 ± 0.68 D at 4 years after femtosecond laser SMILE procedure in 124 myopic eyes. 25
Regarding astigmatism, in Tychsen et al. (2005) and Tychsen and Hoekel., (2006) studies, all children (100%) with astigmatism achieved 1.00–2.00 D of the cylindric correction goal.10,14 likewise, in Autrata et al. (2004) and Ghanem et al. (2010) studies the mean keratometric astigmatism ranged from −0.25 to −1.25 D after surgery (before surgery; ranging from −0.25 to −3.25 D).16,21
An improvement in visual acuity postoperatively was noticed in Tychsen et al. (2005) study, as 38% improved by 1 optotype line or less in the visual acuity chart, and 26% improved by ≥ 3 optotype lines. 10 In Astle et al., Out of 28 eyes who had a measurable preoperative BCVA, 7 of them gained ≥4 optotype lines, 5 eyes gained 1–2 optotype lines, and there was no improvement in BCVA in 16 eyes. 11 likewise, in Paysse et al. (2006) study, only 9 out of 11 children performed the visual acuity test, which showed that (78%) of them gained ≥ 2 optotype lines in uncorrected visual acuity (UCVA), while (33%) of them improved ≥2 logMAR lines in BCVA. 12
On the other hand, there was a noticeable improvement in visual acuity in Autrata et al. (2004) study, as 17/ 27 (63%) eyes gained 4 to 8 optotype lines, 7/27 (26%) eyes gained 1 to 3 optotype lines, and 3/27 (11%) showed no improvement. 16 Similarly, Ghanem et al. (2010) study, 50% of the 9 eyes gained ≥ 5 optotype lines, and the remaining gained from 1–4 optotype lines. 21 While in Utine et al., (2008) study, BCVA improved in 22 out of 32 eyes, as 6 eyes gained ≥4 optotype lines, 4 eyes gained 2 to 3 optotype lines, 12 eyes gained 1 optotype line, 9 eyes remained unchanged, and 1 eye lost 1 optotype line. While UCVA 6 eyes remained the same, 8 eyes gained ≥4 optotype lines, and the rest gained 1–3 optotype lines. 19 likewise, in Samir et al., (2021) study, the authors reported loss of 1 optotype line in best corrected distance visual acuity (BCDVA) in (2%) of the 124 cases. However, (23) % of the cases gained 1–2 optotype lines, and the rest remained unchanged. 25
As per Lin et al. (2009) study, the UCVA and BCVA improved by ≥2 logMAR lines from the preoperative status in 17 eyes out of 24. 20 In Zhang and Yu's (2017) study, the logMAR of BCVA improved by more than 2 lines in (45%) 15 eyes of the cases at 3 days, (50%) in (16 eyes) at 1 month, (74%) in (17 eyes) at 3 months and (86%) in (19 eyes) at 8 months, post-surgery. No patients lost any lines of visual acuity after surgery. 22 Regarding Ram et al. (2019) study, the mean BCVA changed from 20/200 before surgery to 20/80 after surgery. 23
Advantages and disadvantages of laser-assisted refractive surgery
Excimer laser procedure faces a number of challenges, including the fact that excimer laser machines are usually located at outpatient surgical facilities or offices, which raises a logistical issue as performing these surgeries at this age group requires monitored anesthesia. 2 Additionally, the advantage of PRK and LASEK is avoiding flap-related problems that happen more commonly with LASIK, as mentioned before.14,19,20,25 Regarding SMILE procedure, there was a reported case of lenticular decentration, which was managed conservatively by spectacles. 25
During follow-up intervals, many authors reported corneal haze and myopic regression. According to the literature, postoperative haze is less common with LASIK than PRK/ LASEK (Table 1). In Tychsen et al., 2005, the grading of the corneal haze ranged from 0–4, as (78%) of the children measured grade 0–1, (14%) grade 2, and (8%) grade 3–4. 10 The incidence of corneal haze in PRK was lower than in LASEK, according to Autrata et al. (2004) study. However, only 4 cases were reported out of the 27 in this study, with + 2 haze that cleared to +1 haze by 12 months. 16 Moreover, in Agarwal et al. (2000) study, 3 eyes with [SE] more than −17.0 D suffered from grade 2 corneal haze. 14
Summary of excimer laser studies.
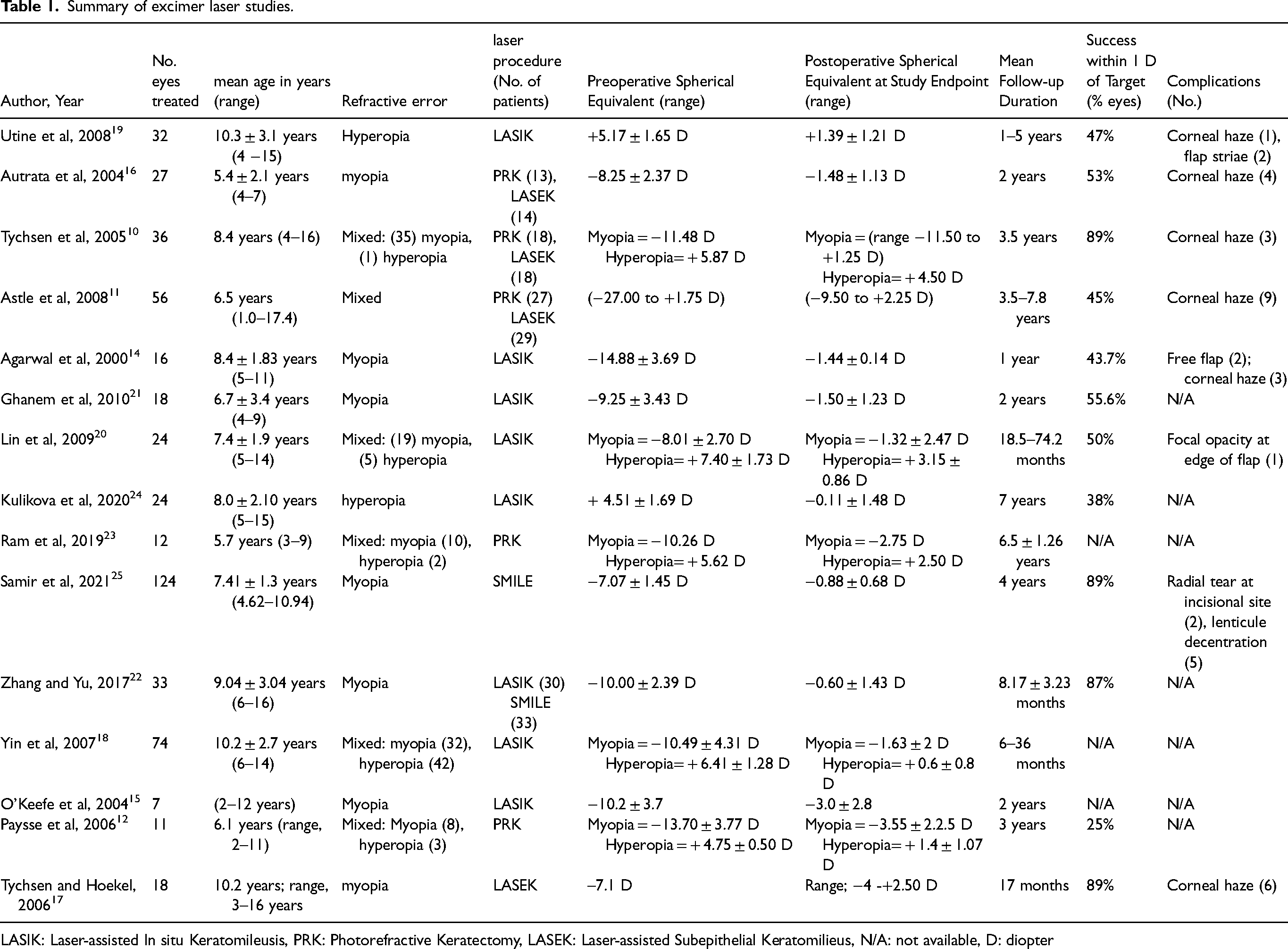
LASIK: Laser-assisted In situ Keratomileusis, PRK: Photorefractive Keratectomy, LASEK: Laser-assisted Subepithelial Keratomilieus, N/A: not available, D: diopter
In regard to refractive regression, the progression of myopia is usually expected with time as axial length continues to increase with aging. More than half of the children experienced myopic regression in Tychsen et al. (2005) study. 10 Similarly, in a study done by Astle et al. (2008), (43%) of the children exhibited some evidence of myopic regression (54% in the PRK group and 46% in the LASEK group); thus, a secondary procedure by LASEK was required. 11 Contrary to the findings of Tychsen and Hoekel (2006), where only (33%) experienced myopic regression and did not require any secondary intervention. 17
In Paysse et al. (2006) study, the myopic group had moderate refractive regression over the first 12 months of follow up, which stabilized in the next 12 months, while the hyperopic group showed mild regression to hyperopia over 36 months. 12
According to Lin et al. (2009) study, 11 developed myopic regression out of 19 eyes of the myopic group, 7 eyes developed hyperopic regression, and only one was with no regression. Meanwhile, all 5 eyes of the hyperopic group developed SE regression. 20 In Ghanem et al. (2010) study, almost (77.8%) of the eyes reached target [SE] at 6 months postoperative, the significant changes in [SE] at 2 years (as mentioned above the percentage of those who achieved [SE] goal was 55.6% at 2 years) suggest myopic regression, a similar concept was found in Yin et al., (2007) study where there was myopic regression from 0.45 D at 6 months to 1.63 D at 36 months, after surgery.18,21
The hypothesis behind refractive regression was suggested and discussed in several studies, as the authors believed that it is attributed to increased axial length due to normal growth of pediatric eyes, corneal thickness, corneal-healing response, and slight decentration due to general anesthesia.11,12,16,17,23 Additionally, in Tychsen et al., 2005 study, 4/35 of the children underwent a trial of topical corticosteroid drops and oral Vitamin C to reduce the likelihood of producing haze; noteworthy, it was significantly milder than the other patients, and 3 of the 4 experienced no myopic regression. 10 This was supported by Paysse et al.2012 as the authors recommend topical fluorometholone for 6 months as well as daily vitamin C following laser procedure to prevent haze. 26
Phakic intraocular lenses (pIOL)
Phakic intraocular lenses (pIOLs) were first used in the 1990's for the treatment of high myopia, where the first pediatric case using pIOL was reported in 1999. 27 The IOL is implanted in the presence of the natural crystalline lens. It is inserted between the cornea and the patient's lens. There are three models; [1] angle-supported anterior chamber pIOLs; [2] iris-fixated pIOLs, which is anchored to the mid-peripheral iris stroma; and [3] posterior chamber pIOLs where the lens is positioned in the posterior chamber just in front of the natural crystalline lens.28,29
Indications
Phakic IOLs are used in cases of anisometropic amblyopia, bilaterally high refractive errors with a neurodevelopmental disability, and high refractive errors that are outside the range of excimer laser refractive surgery. Phakic IOL surgeries come with their own prerequisites; it is recommended that anterior chamber depth be ≥3.2 mm and absence of ocular diseases, such as glaucoma, uveitis, endothelial dysfunction, untreated retinal tear, and cataract.2,5,30,31
Outcomes
In 2011, Alió JL et al. conducted consecutive case series of 10 eyes, where 9 of them underwent iris-fixated pIOL and 1 with a posterior chamber pIOL (1/10 was hyperopic). The visual improvement was rewarding as the mean preoperative sphere reduced from −9.63 ± 6.94 D to −1.06 ± 1.70 D postoperatively. In addition, an impressive improvement in CDVA was noticed as it ranged from 20/100 to 20/2000 before surgery to 20/20 to 20/50 after surgery, except for one patient who underwent posterior chamber pIOL gained one line only. 32 This is also supported by the results published by Ryan A et al. (2012), which reported improvement in mean [SE] from −14.6 to −2.4 D in all 7 eyes who underwent iris-fixated pIOL and mean logMAR vision improvement from 6 ⁄ 40 ± 4 lines to 6 ⁄ 28 ± 3.4 lines. 33 In regard to posterior chamber pIOL, Tychsen et al. (2017) revealed that (88%) of the 40 myopic eyes were within 1.00 D of the refraction goal, and postoperative UCDVA improved 25-fold from mean 20/1050 [logMAR 1.72] to mean 20/42 [logMAR 0.48]. 34
Multiple case series evaluated the effect of anterior chamber pIOL (AC-pIOL). Pirouzian et al. (2009) assessed 6 eyes with anisometropic myopia who underwent AC-pIOL, the study findings showed great improvement in visual acuity, as each recruited child in the study had visual acuity of 20/200 or worse prior to surgery, and 6 months post-surgery there was noticeable improvement (> 6 lines of Allen/Snellen) in (66.6%) of the patients while the rest of the patient improved > 4 lines of visual acuity. 27 later on, in 2010, Pirouzian and Ip evaluated the efficacy of AC-pIOL in 7 eyes with myopia (mean SE −14.28 ± 2.2 D, preoperatively). The authors revealed reduction in the mean [SE] at 3 years postoperative to −1.10 ± 0.75 D, and all patients showed a significant improvement in CDVA (>6 lines Allen/Snellen gained) after surgery. 35 Meanwhile, Tychsen L. et al. (2008) evaluated 20 myopic and hyperopic eyes that underwent AC-pIOL, where the authors reported improvement in both [SE] and BCVA. BCVA was 20/98 before surgery and 20/32 after surgery. 4 No loss of optotype lines was reported in these studies.27,35–37 Table 2 highlights the important findings of the previous published studies.
Summary of pIOL studies.
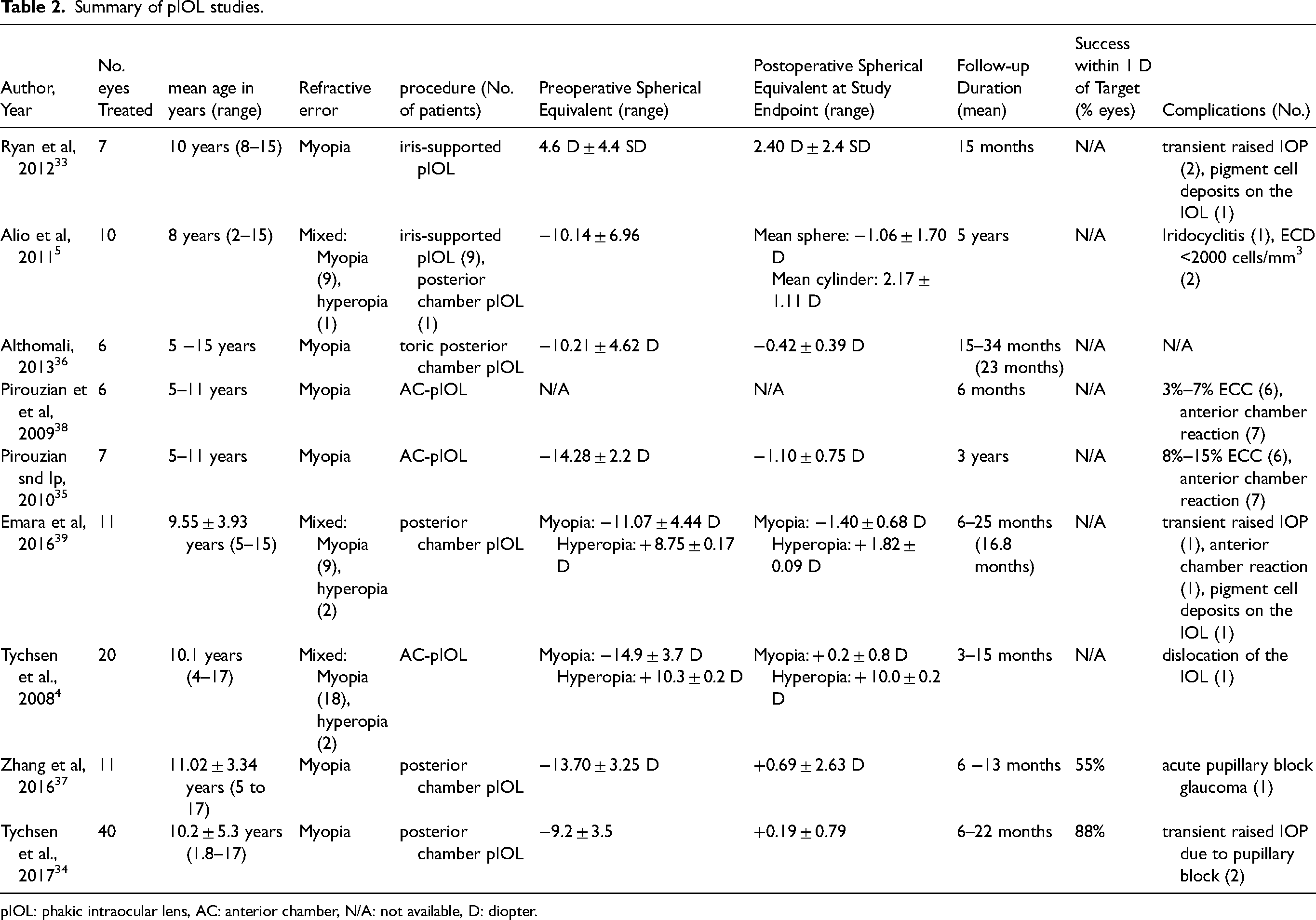
pIOL: phakic intraocular lens, AC: anterior chamber, N/A: not available, D: diopter.
Several authors have studied the implantation of toric and spherical pIOLs in children. In 2013, Althomali placed toric posterior chamber pIOL in six amblyopic children, where 5/6 gained three lines of BCVA (one eye gained 8 lines), and 1/6 gained 2 lines. Moreover, the mean [SE] cycloplegic refraction improved from −10.21 ± 4.62 D to −0.42 ± 0.39 D postoperatively. 36 While in 2016, Emara et al. placed toric and spherical pIOLs in 11 eyes (9 myopic, 2 hyperopic, and 3 received toric ICL), where the authors reported improvement in CDVA in both myopic and hyperopic groups as all 9 myopic eyes gained 2 or more optotype lines (one eye gained 9 lines), and 1 hyperopic eye gained 4 lines whereas the remaining hyperopic eyes gained 9 lines after surgery. 39
Advantages and disadvantages
In the case of phakic IOL, the implanted lens is exchangeable, permitting potential reversibility, unlike laser surgeries and refractive lens exchange. It also allows the lens to maintain its function of accommodation, which is valuable and needed in this age group, and potentially reduces the chance of vitreoretinal complications. Additionally, unlike laser procedures, it holds fewer concerns regarding corneal haze, corneal thinning, or future corneal ectasia. 40
As for the disadvantages, Alió JL et al. (2011) reported no major postoperative complications except for acute iridocyclitis, which was detected immediately after implantation and resolved with steroid treatment, in addition to the mean reduction in the endothelial cell density (ECD), which accounted for (10.24 ± 2.53%) at 60 months after surgery, however 2/10 eyes had ECD <2000 cells/mm3 due to spring catarrh allergic conjunctivitis in one patient and ocular trauma in the other patient. 32 These findings are supported by Pirouzian et al. (2009), where all patients showed (3–7%) ECD loss within 6 months from surgery. 27 Additionally, in Ryan et al. (2012) study, 3 out of 11 eyes had (6.6%) ECD loss (all of them had previous congenital cataract), while in the rest of the eyes, the ECC was unmeasurable due to some limitations. 33 Another study conducted by Pirouzian and Ip in 2010 is in line with the previously mentioned literature, as ECD loss ranges between (6.5–15.2%) following the insertion of pIOL. The normal annual rate of ECD loss is estimated at approximately (2.9%) up to the age of 14 years and (0.3%) thereafter. 35
However, those who underwent AC-pIOL exhibited some anterior chamber reactions.35,38 Tychsen et al. (2008) also reported IOL dislocation in one patient out of twenty eyes after surgery which required reoperation. 4 Also, it was reported in some literature that pIOL can adversely lead to pigment dispersion, transient raised in intraocular pressure, and acute pupillary block.33,34,37,39
Clear lens exchange (CLE)
Clear or refractive lens exchange/extraction is another surgical refractive option for children. Such intervention involves lensectomy with or without IOL implantation. 3
Indications
This intervention can be performed in pediatric cases with extreme refractive error exceeding 15 diopters if the anterior chamber is shallow (<3.2 mm), precluding pIOL placement.3,41
Outcomes
A study conducted by Tychsen et al. (2006), involved 26 myopic eyes with [SE] ranged from −14.25 to −26.00 D (12 underwent CLE, and 14 underwent CLE with IOL). The study reported that (73%) gained significant improvement in [SE] post-surgery as it was corrected within ± 1 D of the goal refraction. 3 This result ties well with another study by Ali et al, (2007) which reported the outcome of 7 myopic eyes (mean SE −16.7 D) following lensectomy (2 eyes had IOL implantation). The authors revealed that 6 eyes were within ± 3.0 D of the target refraction. A significant improvement in UCVA was rereported as all 7 eyes improved from a mean 20/2550 to a mean 20/130. 42
On the other hand, Ram et al. (2014) compared the efficacy of monofocal versus multifocal IOL in 42 eyes (14 eyes received multifocal IOL, and 28 eyes received monofocal IOL). The study showed that (64.28%) of 14 eyes in the multifocal IOL group gained BCVA of 20/40 or better, and the remaining (35.71%) was in the range of 20/50–20/200. Compared to the monofocal IOL group where 50% of 28 eyes gained a BCVA of 20/40 or better, and the remaining (39.2%) had a BCVA ranging from 20/50–20/80, the difference between the two groups was not statistically significant. 43
Advantages and disadvantages
CLE may be the only option for some cases, especially those with high hyperopia and shallow anterior chamber, but it comes with some potential risks and adverse effects. By removing the natural lens, accommodation becomes impossible, and this necessitates the wear of bifocal glasses, which is very difficult for many of those cases. Therefore, some authors have advocated the use of multifocal lenses in children. 43 Myopic regression during follow-up interval was reported to account for (100%) in Ali et al. (2007) study and (69%) in Tychsen et al. (2006).42,44
Posterior capsule opacification (PCO) was also reported in older children, Ali et al. (2007) reported 2 cases aged 10 or older required YAG-laser capsulotomy due to PCO, which occurred approximately 1.5 years after lensectomy. 42 In Tychsen et al. (2006) study, the authors reported 13 out of 26 eyes suffered from PCO postoperatively, necessitating a secondary procedure (YAG-laser or pars- plana capsulotomy). However, in the same study, the remaining 13 eyes underwent primary posterior capsulectomy and subtotal vitrectomy; thus, none of these eyes required re-entering the operating room. 3 Moreover, the authors stated that primary IOL implantation did not affect the rate of developing PCO, as opacification occurred in both cases that had lens extraction alone and refractive lens exchange.3,42
In like manner, Ram et al., 2014 study showed a total of 20 eyes (6/14 eyes of multifocal IOL and 14/28 eyes of monofocal IOL) performed primary posterior capsulotomy combined with anterior vitrectomy after lensectomy. 15 eyes (35%) developed PCO ((5/14) eyes of multifocal IOL, and (10/28) eyes of monofocal IOL), non of which had primary posterior capsulotomy with anterior vitrectomy. Only six eyes (6/15) classified as significant PCO and underwent laser or surgery. Nd: YAG- laser was done in 2 eyes in the multifocal IOL group and 3 eyes in the monofocal IOL group, while one eye of the monofocal IOL group required surgical capsulotomy. 43
In addition, one study encountered hyphema 1 day after surgery, which was diffused into the vitreous cavity and required secondary surgery 1 week after (anterior chamber washout and vitrectomy). 42 Other complications reported by Tychsen et al. (2006), including rhegmatogenous retinal detachment after ocular trauma and dislocated IOL posteriorly into the vitreous cavity necessitating IOL exchange. 3
Conclusion
Refractive surgery in pediatric requires special consideration due to the ongoing changes of refraction with time. Unlike adults, pediatric refractive surgery carries considerable challenges, such as the need for general anesthesia, lack of proper communication, and special requirements after surgery to reduce unwanted complications. The indications for refractive surgery here is different than adults and should be considered carefuly before considering this intervention (Table 3). One of the biggest concerns of refractive surgery in children is the progression of myopia with age, and so methods of myopia control such as the use of low-dose Atropine may be considered for these patients after surgery. This article reviews the role of refractive surgery in children, and the different options avalibile. Due to the nature of the disease, it is extremely difficult to conduct a large-scale prospective controlled trials to accurately evaluate the results of these procedures and study the potential side effects. Despite the lack of convincing evidence, refractive surgery may be the only option to preserve vision and reduce the chance of amblyopia is some cases where other treatment modalities have failed.
Indications of refractive surgery in children.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.