
Abstract

Dear Editor,
We read with great interest the study by Panozzo et al. published recently in the European Journal of Ophthalmology. 1 It showed that the European School of Advanced Studies in Ophthalmology (ESASO) optical coherence tomography (OCT)-based classification of diabetic maculopathy (DM), is an easy and reproducible method to stage DM during clinical practice.1,2 The study concluded that the disseminated use of this common and validated system may offer several clinical and scientific advantages. We herein present a concise representation of the ESASO classification in the form of a scoring sheet that can be used as a ready reference for easy application of the system in busy clinics.
The ESASO classification system consists of two tables. In the first, the ESASO has introduced grading of seven different pathological changes in the retina that are identifiable on spectral-domain macular OCT scans, denoted by alphabets. In the second, a staging system for DM is provided according to different combinations of the first four variables (T, C, E and D). 2 We have further summarized these two tables and provided a concise representation of the same in our proposed scoring sheet (Table 1). One such sheet is made for each eye of the patient for which OCT has been performed reliably. A numeral is written in the corresponding column of ‘score’, and a checkmark is placed on the corresponding column of ‘stage’ of DM.
Concise representation and scoring sheet for the European School of Advanced Studies in Ophthalmology optical coherence tomography-based classification system of diabetic maculopathy.
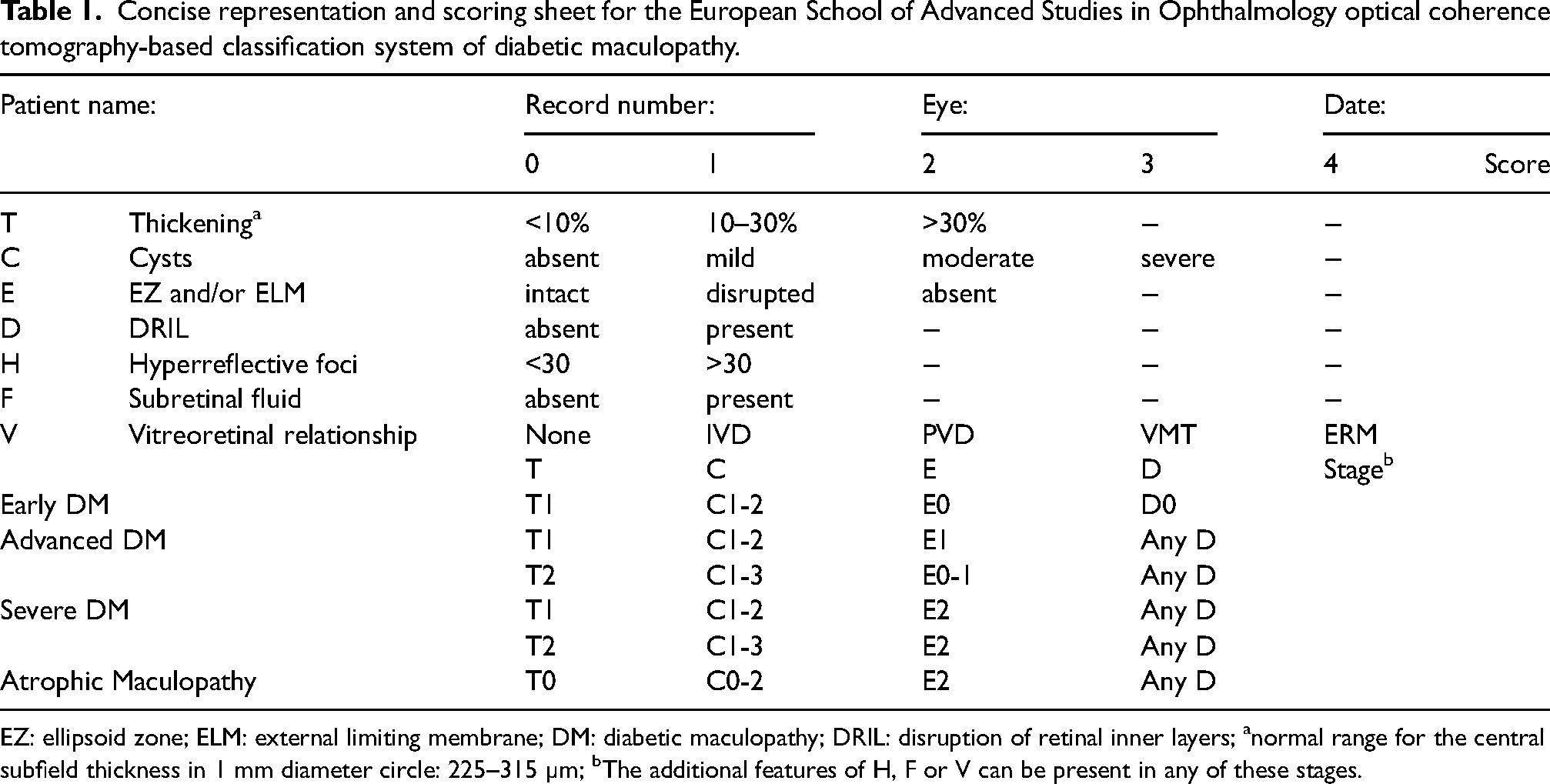
EZ: ellipsoid zone; ELM: external limiting membrane; DM: diabetic maculopathy; DRIL: disruption of retinal inner layers; anormal range for the central subfield thickness in 1 mm diameter circle: 225–315 µm; bThe additional features of H, F or V can be present in any of these stages.
In our experience, the use of the scoring sheet further simplifies the application of the ESASO classification system in our busy clinics. For example, we have affixed a printout of this summary table on the wall of our retina clinic. We also routinely append this sheet to patient records and OCT studies, which results in ready reference during primary examination and follow-up OCT examinations.
While it is true that all this information can be recorded in the ophthalmic examination report and thus retrieved without the need for this additional printed sheet, the context of diabetic retinopathy, with its high prevalence and incidence leading to numerous annual visits to ophthalmic clinics (both initial and follow-up), warrants consideration. Given the large number of ophthalmic reports generated, the use of this printed sheet could be beneficial for recording the ESASO score, minimizing typographical errors or distractions (due to the numerous letters and numbers that must be entered in an ophthalmic report), and providing immediate readability and visual impact during follow-up (FU) visits. We hope that the wide dissemination of this scoring sheet results in more clinics adopting the use of the ESASO classification system for uniformity in recording, reporting and prognosticating diabetic maculopathy.
A separate sheet with a single chart showing the progression of the disease stage over various follow-up visits, indicating any transitions between stages or stability over time may also be incorporated (Table 2). Summarizing this approach could save time by facilitating a quick ESASO classification comparison with previously printed sheets in the FU examination without the necessity of reviewing the entire previous ophthalmic reports. Additionally, in clinical practice, monitoring the progression of DM stages over time is particularly useful. Similar to the trend graphs printed for each visual field examination, such as the Visual Field Index (VFI) in glaucoma, this provides an immediate visual impact of the condition in a single chart. Future approaches could dwell further on the feasibility and utility of this proposal in daily clinical practice.
Proposed chart for denoting the progression of the disease stage over various follow-up visits.a
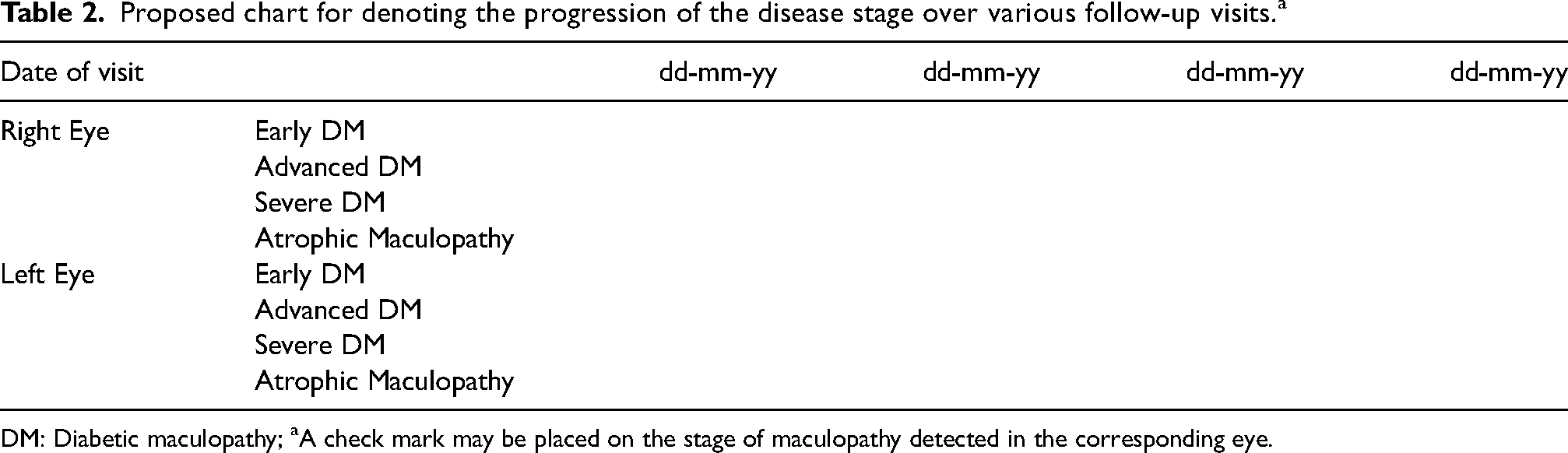
DM: Diabetic maculopathy; aA check mark may be placed on the stage of maculopathy detected in the corresponding eye.
Footnotes
Acknowledgements
We thank Prof Dr Rajvardhan Azad, former Chief and Head of Vitreoretinal Services, Dr RP Centre for Ophthalmic Sciences, All India Institute of Medical Sciences, New Delhi, India. We also thank the reviewers for their valuable suggestions.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.