
Abstract
Introduction
A concave iris configuration is a characteristic feature of pigment dispersion syndrome (PDS). Therapeutic strategies to modify this configuration may be considered as first-line options for the treatment of ocular hypertension in PDS patients.
Case description
A 37-year-old male patient with myopic anisometropia presented bilateral PDS with concave iris, Krukenberg's spindle and iris transillumination defect in both eyes. The intraocular pressure (IOP) was 27 mmHg in both eyes. Optic nerve and visual field parameters were normal. The right eye was treated with a neodymium:YAG LPI. In the left eye, an implantable collamer lens (ICL) V4c model implantation for myopia correction was performed. Six-months postoperatively, both eyes evidenced an anteriorization of the iris, the morphology of the concave iris improved with the ICL V4c in place, becaming flattener in left eye. The IOP was 18 mmHg without treatment.
Conclusion
This case report reinforces the idea that in myopic patients with a concave iris, the refractive correction approach through ICL V4c implantation might also improve the iris configuration, similarly to laser peripheral iridotomy (LPI). Therefore, in this specific patient profile, this surgical procedure might be considered as a prophylactic treatment alternative to prevent the complications associated with this iris configuration, although its invasive nature should be taken into consideration.
Introduction
A concave iris configuration is a risk factor in developing a pigment dispersion syndrome (PDS),1–5 which, over time, can lead to an increase in intraocular pressure (IOP) and pigmentary glaucoma (PG). One possible option to modify iris concavity is to perform a laser peripheral iridotomy (LPI). This procedure consists of using a laser light beam to create a small opening in the iris to allow the flow of the aqueous fluid through it from the posterior to the anterior chamber and vice versa. This mechanism balances the internal pressure between the anterior and posterior chambers, shifting the iris shape from concave to flattened. 6 Consequently, it reduces the iris-lens friction related to concave iris shape and, hence, pigment shedding.
A recent study found that the implantable collamer lens (ICL) V4c model (Staar Surgical AG, Nidau, Switzerland), which incorporates a 360 μm central hole, significantly modify the morphology of concave iris, suggesting that it might reduce the risk of intraocular pigment dissemination provoked by iris concavity. 7
This case report presents a patient with anisometropia who attended our centre for a refractive surgery consultation. After clinical exploration, bilateral PDS with concave iris and ocular hypertension (OHT) was observed in both eyes. The manifest refraction was close to emmetropia in the right eye, and an LPI was performed. In the left eye, with moderate myopia, an ICL V4c model was implanted with refractive purpose, and later on, we monitored the iris morphology and IOP control.
Case description
A 37-year-old man presented for a refractive surgery consultation at the Fernández-Vega Ophthalmological Institute (Oviedo, Spain). The initial assessment revealed an uncorrected distance visual acuity (UDVA) of 20/25 in the right eye and 20/400 in the left eye. His manifest refraction was −0.50 dioptres (D) sphere in the right eye, and −4.75 D sphere and −1.00 D cylinder at the 70° axis in the left eye, reaching a corrected distance visual acuity (CDVA) of 20/20 in both eyes. The analysis of the corneal topo-tomographic (Sirius, CSO Ophthalmic, Spain) showed a healthy cornea without signs compatible with corneal ectasia and a central thickness of 586 µm in both eyes. The IOP measured by Goldmann applanation tonometry was 27 mmHg in both eyes. The biomicroscopy examination revealed Krukenberg's spindle and iris transillumination defect (Figure 1(a)). We proceeded to carry out a gonioscopy (four-mirror lens), observing pigment deposition on trabecular meshwork and iris concavity. The Anterior-Segment Optical Coherence Tomography (AS-OCT, CASIA2, Tomey, Japan) evaluation reported an anterior chamber depth (ACD) of 3.3 mm, with a concave iris in both eyes (Figure 1(b)). The exploration of the optic nerve through the slit-lamp biomicroscopy with a handheld lens and the retinal nerve fibre layers examination (Optovue OCT, Optovue Inc., Fremont, CA, USA) did not evidence optic nerve damage. Finally, we performed a standard automated perimetry (Humphrey visual field analyzer, Carl Zeiss, Germany), and all visual field parameters were within normal limits.
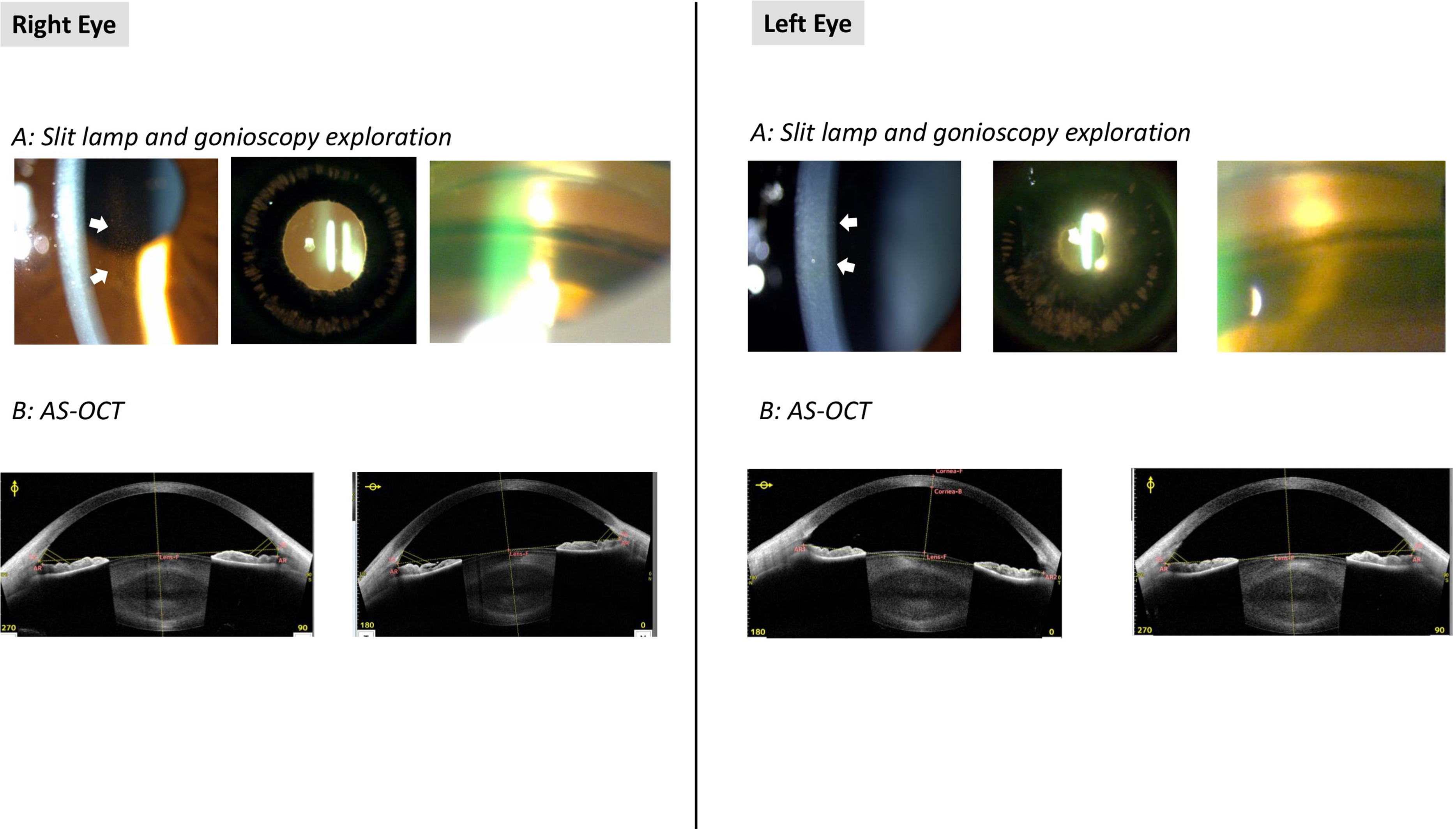
Preoperative clinical examination showing the classical triad clinical features of a PDS: pigment deposition on the posterior surface of the central cornea (Krukenberg's Spindle), mid-peripheral iris transillumination defects, and dense trabecular meshwork pigmentation (a); iris concave shape confirmed by AS-OCT evaluation (b). The IOP was elevated but without visual field loss or optic.
Based on all these parameters, the patient was diagnosed, beyond the myopic anisometropia, of bilateral PDS with concave iris and OHT without optic nerve damage or visual field loss.
Topical prostaglandin analogue eyedrops (Tafluprost, Santen Inc, Japan) once a day was prescribed, and IOP reduction to 15 mmHg was observed over the next three weeks in both eyes. Subsequently, the right eye was treated with a neodymium: YAG LPI. In the left eye, we performed an ICL V4c model implantation for myopia correction, and, secondary, we expected that ICL V4c induced an iris reshaping from concave to flattened. The surgical procedure was performed according to the standard procedure previously described. 8
Six months postoperatively, the UDVA was 20/25 in both eyes, the manifest refraction was −0.50 D sphere in the right eye, and −0.50 D cylinder at the 180° axis in the left eye, reaching a CDVA of 20/20 in both eyes. The IOP was 18 mmHg without topical medication. The AS-OCT evidenced an anteriorization of the iris and an approximation of the iris to scleral spurs (Figure 2). These changes provoked a significant reduction in the angle opening distance (AOD) and trabecular iris space (TISA) parameters (Table 1) All parameters remained without changes at the 1-year postoperative visit.
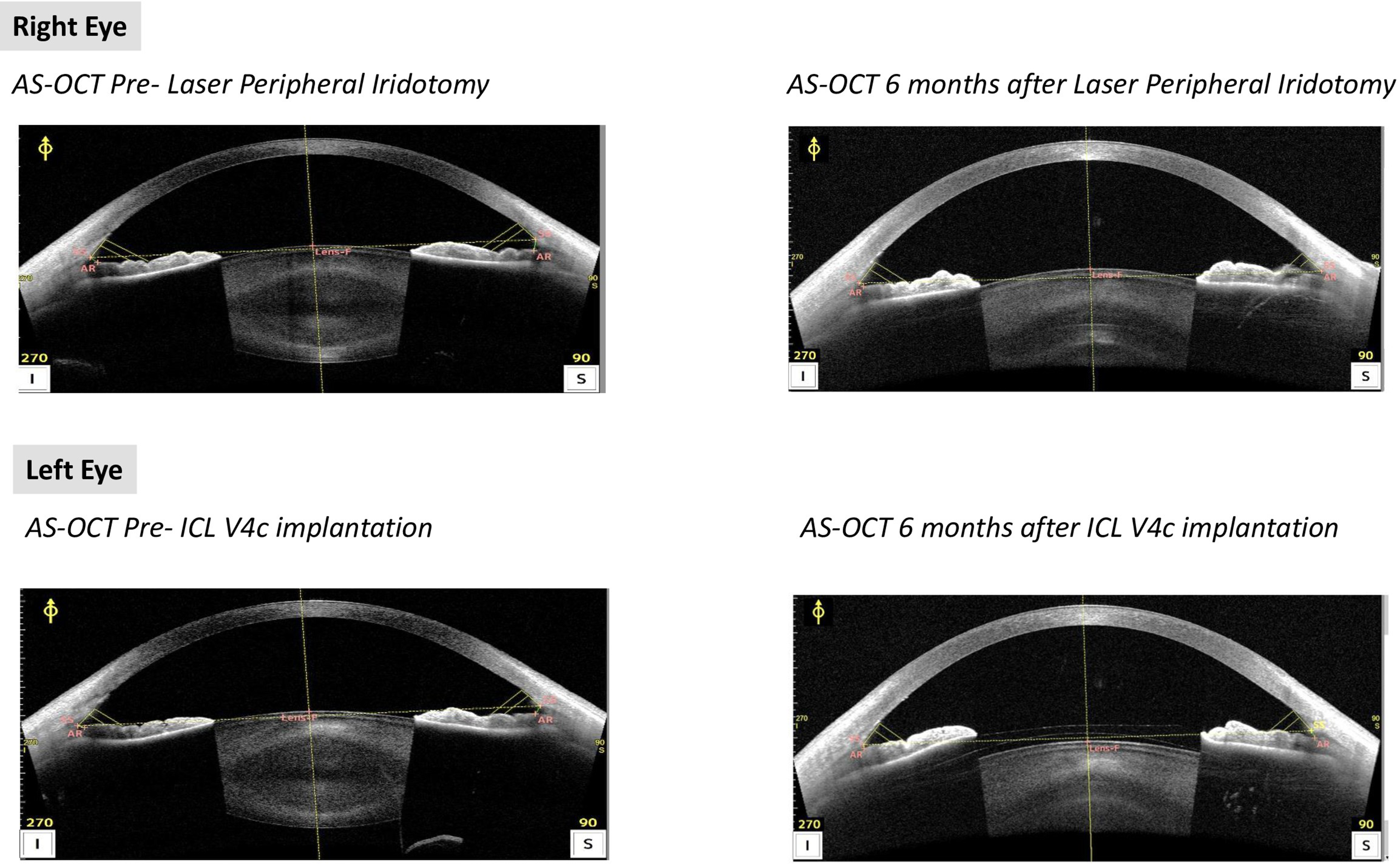
The Anterior-Segment Optical Coherence Tomography (AS-OCT, CASIA2, Tomey, Nagoya, Japan) evaluation before and after Laser Peripheral Iridotomy in the right eye (upper) and before and after ICL V4c implantation (lower).
Anterior chamber angle parameters before and after treatments of each eye, assessed with Anterior Segment Optical Coherence Tomography.
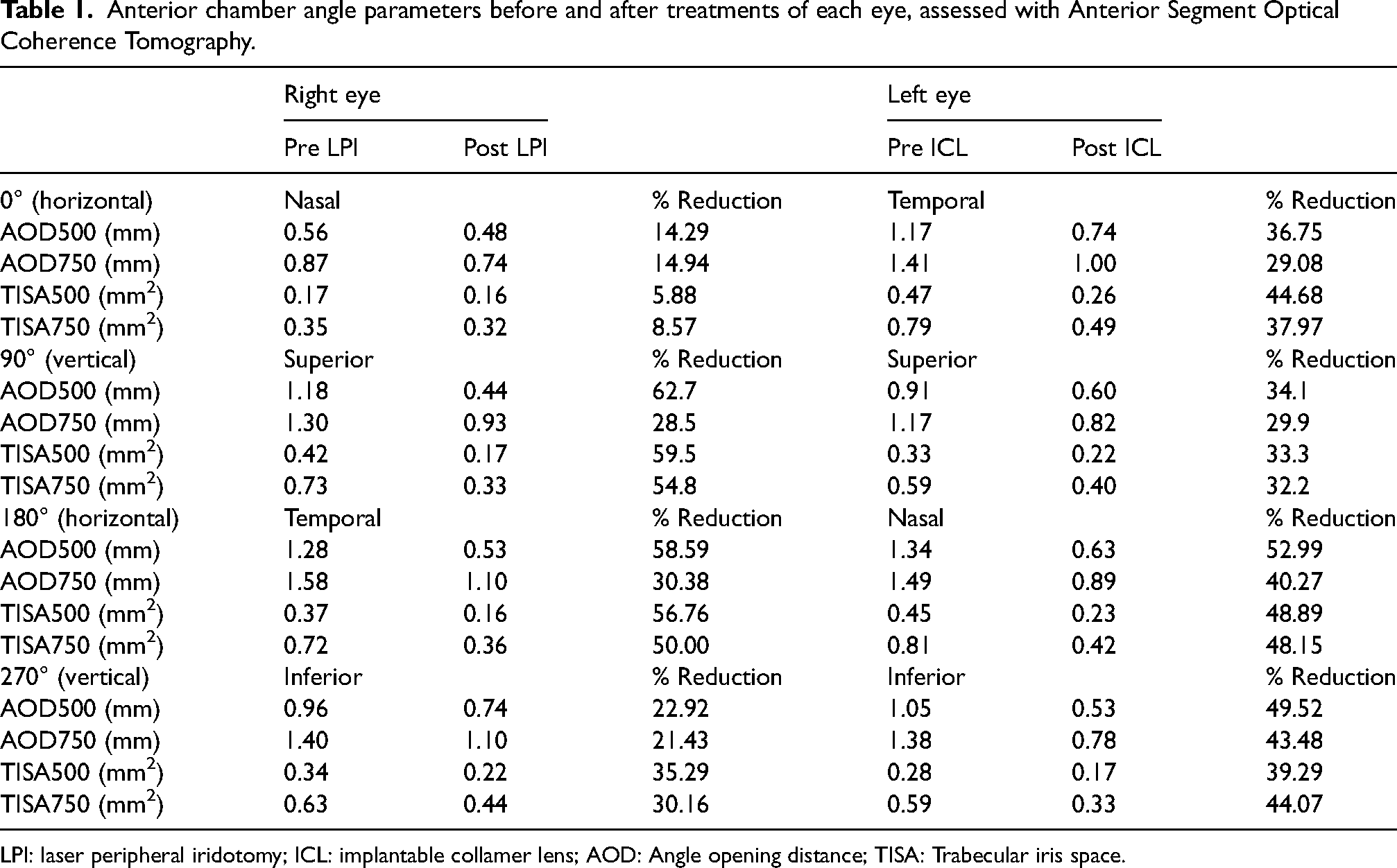
LPI: laser peripheral iridotomy; ICL: implantable collamer lens; AOD: Angle opening distance; TISA: Trabecular iris space.
Discussion
The clinical examination of the patient presented in this case report evidenced the classical triad of clinical features present in PDS: dense trabecular meshwork pigmentation, mid-peripheral iris transillumination defects, and pigment deposition on the posterior surface of the central cornea (Krukenberg's spindle). The IOP was elevated in both eyes but without visual field loss or confirmed optic neuropathy. Furthermore, an iris concave configuration was confirmed by gonioscopy and AS-OCT evaluation.
The iris concave configuration triggers pigment shedding due to the mechanical rubbing between the peripheral iris and lens zonules during pupillary activity. This morphologic sign is common in patients with PDS and PG.1–5 Hence, therapeutic strategies to modify the concave iris shape aiming to stop the mechanism that induces pigment dispersion might be a useful therapy for PDS treatment.1–9
Iris concave morphology is considered to be caused by a reverse pupillary block. 10 In these eyes, the pressure in the anterior chamber is higher than in the posterior chamber, provoking a posterior bowing of the iris and, consequently, a concave configuration. An LPI irrupts this anterior-posterior pressure balance. The hole opened on the iris tissue allows the aqueous humour drainage from the posterior to anterior chamber but also, on the contrary way, that is, from the anterior to the posterior chamber. This feature would equalise the pressures of the anterior and posterior pressure chambers and prevent the iris from deforming towards the inside; consequently, the iris configuration would become flattened. 6
Recently, Zhang et al. 7 analyzed the changes in the morphological iris induced by an ICL V4c in high myopic patients with a concave iris morphology without reported signs of PDS. The morphology of the concave iris significantly improved with the ICL V4c in place and became flattener. The Iris curvature, Iris-Lens Contact Distance and iridocorneal angle were significantly decreased after ICL V4c implantation. It is important to note that the ICL V4c incorporates a central hole, and it is not needed to perform an LPI as with the predecessor models. Therefore, the changes in the iris morphology were produced by the lens.
The authors pointed out that the physical ICL space-occupying, in contact with the posterior surface of the iris, induced an iris displacement and partly explained the iris configuration change. Of note that it seems that the ICL material characteristics (biocompatibility, soft, elastic and hydrophilic surface) make that the contact between the lens and iris did not represent a significant risk for a mechanical loss of pigment, and the ICL V4c model provides safe outcomes in terms of induced-IOP changes. 11 Furthermore, the central hole of the ICL V4c allows the flow of the aqueous fluid through the ICL,12–14 acting similarly to LPI, preventing the reverse pupillary block and consequently reversing the iris concave morphology. Hence, the authors concluded that an ICL V4c implantation might have a similar effect to LPI for reverting a concave iris morphology. Obviously, the approach of an ICL implantation should be only considered in cases with a refractive error. This surgical procedure must only be considered in cases interested in refractive surgery and meet the safety criteria for ICL implantation. That is, the first aim of this approach must be refractive, and subsequently, it must evaluate whether it is also effective in correcting the iris morphology.
In the present case report, we evaluated both approaches (LPI and ICL V4c implantation, one in each eye) simultaneously due to the patient's anisometropia and interest in correcting his left eye's myopia. Furthermore, unlike the study by Zhang et al., 7 the clinical exploration evidenced a PDS and raised IOP. We observed that both LPI and ICL V4c had similar effects. The AS-OCT evidenced an anteriorization of the iris in both eyes, provoking an iris reshaping to a flattened configuration that remained over one year of follow-up. These findings agree with those previously reported by Zhang et al. 7 Furthermore, the OHT was also successfully managed (decreasing from 27 mmHg to 18 mmHg), and the patient did not require hypotensive medical treatment.
The role of LPI in the natural history of PDS and PG remains controversial. 9 Similarly, whether the ICL V4c implantation might be an effective treatment for OHT in PDS is still unknown. However, there are anatomical changes in the anterior chamber after both procedures, particularly concerning iris configuration. In the present case, these changes were accompanied by significant IOP reduction in both eyes. This finding had been described after LPI in PDS/PG, 9 yet this is the first report regarding ICL, as far as authors are concerned.
Furthermore, this described change in iris configuration (flat or convex, rather than concave) obtained after LPI/ICL V4c might lead to a modification in the pathogenic mechanism of pigment dispersion, at least theoretically: a reduction in rubbing between the crystalline lens and posterior surface of the iris might release less amount of melanin granules, decreasing further damage on the trabecular meshwork, thus reducing aqueous humour outflow resistance.
This case report reinforces the idea that in myopic patients with a concave iris, the refractive correction approach through ICL V4c implantation might improve the iris similarly to LPI. Therefore, this surgical procedure might be considered as a prophylactic treatment alternative in myopic cases that meet the safety criteria for ICL implantation, with a concave iris (with or without PDS and OHT) to prevent the subsequent complications associated with this iris configuration. Further clinical studies, including more cases, should be conducted to evaluate this approach properly.
Footnotes
Acknowledgements
Not applicable.
Authors’ contributions
IRU: Conceptual design, supervision, manuscript elaboration, revision and approval.
LFV: Conceptual design, manuscript elaboration, revision and approval.
BAB: Data acquisition, manuscript revision and approval.
AFV: Data acquisition, manuscript revision and approval.
IMA: Data acquisition, manuscript revision and approval.
DMC: Conceptual design, supervision, manuscript revision and approval.
JFA: Conceptual design, supervision, manuscript revision and approval.
Availability of data and materials
The datasets used during the current study are available from the corresponding author on reasonable request.
Consent for publication
Not applicable.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics approval and consent to participate
This study was conducted in compliance with the tenets of the Declaration of Helsinki, and full ethical approval from the Fernández-Vega Ophthalmological Institute was obtained.
Correction (January 2025):
In paragraph 5 of the Discussion section, an error was noted in the sentence “Of note that it….. induced-IOP changes”. In this sentence, the term “hydrophobic surface” has been changed to “hydrophilic surface.” The article has been updated online to reflect this change.