
Abstract
Objective
To investigate the prevalence of anxiety and depression, and explore their related factors in all types of diabetic retinopathy (DR) patients more precisely and accurately by multiple scales.
Methods
Beck anxiety inventory (BAI), self-rating anxiety scale (SAS), beck depression inventory (BDI), and self-rating depression scale (SDS) scores were assessed in 247 DR patients and 250 non-retinopathic diabetes mellitus (NRDM) patients.
Results
In DR patients, there were 32 patients with proliferative DR and 115 patients with impaired visual acuity. The prevalences (95% confidence interval) of anxiety were 38.5% (32.4%–44.6%) and 32.0% (26.2%–37.8%) by BAI and SAS, while those for depression were 31.6% (25.8%–37.4%) and 25.1% (19.7%–30.5%) by BDI and SDS in DR patients. BAI score (P = 0.003), BAI-defined anxiety rate (P = 0.010), SAS score (P = 0.001), SAS-defined anxiety rate (P = 0.006), BDI score (P = 0.005), BDI-defined depression rate (P = 0.028), and SDS score (P = 0.001) were increased in DR patients versus NRDM patients. In DR patients, proliferative DR independently related to BAI-defined anxiety (P < 0.001) and SAS-defined anxiety (P < 0.001). Female (P = 0.016) and proliferative DR (P < 0.001) independently associated with BDI-defined depression; female (P = 0.007), DM duration (P = 0.025), triglyceride (TG) (P = 0.026), and proliferative DR (P = 0.014) independently associated with SDS-defined depression. The combination of these independent factors showed acceptable abilities in predicting BAI-defined anxiety, SAS-defined anxiety, BDI-defined depression, or SDS-defined depression in DR patients, with area under curves of 0.626, 0.656, 0.696, and 0.741, respectively (all P < 0.001).
Conclusion
Anxiety and depression are prevalent; meanwhile, proliferative DR, female, DM duration, and TG independently relate to anxiety or depression in DR patients.
Introduction
Diabetic retinopathy (DR) is a common retinal vascular complication of diabetes mellitus, which affects approximately 30% of the diabetic population.1–3 DR is caused by chronic hyperglycemia-induced destruction of the blood vessels, fluid accumulation, and hemorrhage in the retina, which leads to severe visual impairment (cloudy or blurred vision) and even blindness in DR patients. 4 In addition to the impairment of vision, DR patients also frequently experience reduced physical function, social isolation, and increased financial strain, and thereby, they may be prone to suffer from a series of mental burdens.5–7 Worse still, these mental burdens negatively affect the quality of life of DR patients, reduce treatment compliance, and even hamper disease control.6,8 Therefore, focusing on the mental health status and exploring the related factors is meaningful to prevent psychological disorders in DR patients.
Currently, more and more studies have attached importance to the mental status of DR patients.9–11 It is reported that anxiety and depression rates are 13.5%–41.1% and 25.0%–40.5% respectively in DR patients.9,10,12,13 Notably, anxiety and depression are considered to be influenced by different DR characteristics.10,14,15 For example, one previous study showed that DR severity had a positive linear relationship with the diagnosis of depression in DR patients. 14 Another study found that DR patients who were blind or had severe impairment in visual acuity were more likely to have higher levels of depression than those with mild-to-moderate impairment in visual acuity. 10 It was also reported that diabetic macular edema and proliferative DR were related to higher levels of anxiety in DR patients. 15 In addition, there are also some studies assessing other anxiety- and depression-related factors in DR patients.9–11 One study revealed that stress and chronic diseases (including hypertension, cerebrovascular disease, hyperthyroidism, heart disease, tumor, and neurasthenia) were anxiety- and depression-related factors in DR patients. 9 Another study illustrated that reduced self-care skills and diastolic blood pressure were independently linked to elevated anxiety score; rural residence, history of hypertension, and decreased exercise of self-care agency total score were independently related to increased depression score in DR patients. 10 However, these above studies have certain limitations, such as the relatively small sample size or the application of a single scale to assess anxiety and depression in DR patients. By using multiple scales, the identification of the prevalence and risk factors of anxiety and depression may be more precise and accurate.
The beck anxiety/depression inventory (BAI/BDI) and self-rating anxiety/depression scale (SAS/SDS) are brief and easy-to-score scales with good internal consistency and test–retest reliability.16–20 Meanwhile, these scales have their respective features.19–22 Specifically, the BAI scale has small measurement errors and is suitable for screening for anxiety related to panic attacks.19,21 The SAS scale fulfills the screen for anxiety regarding panic attacks and generalized anxiety disorder. 19 The BDI scale is fit for depression screening and measurement of depression severity. 20 The SDS scale is suitable for measuring depression severity, and its items can be understood more easily than those of the BDI scale.20,22
Therefore, our study used multiple scales (BAI, SAS, BDI, and SDS scales), intending to investigate the prevalence of anxiety and depression, as well as explore the influence of related factors (including DR characteristics) on anxiety and depression in DR patients in a more precise and accurate way.
Methods
Study design
This cross-sectional study enrolled 247 DR patients and 250 non-retinopathic diabetes mellitus (NRDM) patients who visited or revisited our hospital (The First Affiliated Hospital of Harbin Medical University, Harbin, China) from October 2020 to August 2021. There was approval for the study from the Ethics Committee. Written informed consent was obtained from all DR patients and NRDM patients.
Inclusion and exclusion criteria
The inclusion criteria for DR patients were: a) diagnosed as DR by ophthalmological examination, including visual acuity, slit lamp examination, and funduscopy for the presence of retinopathy 23 ; b) aged ≥18 years; c) had good compliance, understanding, and expression ability; d) willing to cooperate in completing all questionnaires. The exclusion criteria for DR patients were: a) had a history of eye diseases such as eye tumors or eye injuries; b) had active eye infection; c) combined with severe cancers, malignant hematologic diseases, or other serious systemic diseases; d) had a treatment history of anxiety or depression; e) pregnant or breastfeeding females. The inclusion criteria for NRDM patients were: a) diagnosed as NRDM by ophthalmological examination, including visual acuity, slit lamp examination, and funduscopy for the absence of retinopathy23,24; b) aged ≥18 years; c) had good compliance, understanding, and expression ability; d) willing to cooperate in completing all questionnaires. The exclusion criteria for NRDM patients were the same as the DR patients.
Data collection
After the enrollment of NRDM and DR patients, the characteristics were collected in time. The collected characteristics included the patient's age, sex, body mass index (BMI), education, employment, marriage, smoking, drinking, hypertension, hyperlipidemia, DM duration, stage of DR, DR type, best-corrected visual acuity (BCVA), diastolic blood pressure (DBP), systolic blood pressure (SBP), heart rate (HR), glycated hemoglobin A1c (HbA1c), alanine aminotransferase (ALT), aspartate aminotransferase (AST), serum creatinine (Scr), triglyceride (TG), and total cholesterol (TC). Stage of DR was assessed according to Evidence-based guidelines for the diagnosis and treatment of diabetic retinopathy in China (2022), and stage IV-VI was defined as proliferative DR. 25 Impairment of visual acuity was defined by reference to previous literature as BCVA <0.3 (20/63).26,27
Anxiety and depression assessment
The BAI score, SAS score, BDI score, and SDS score were evaluated of the DR patients and NRDM patients after enrollment.
The anxiety of the patients was assessed using the BAI and SAS scales. The BAI scale was a Likert-type self-rating scale used to assess patients’ anxiety. The scale covered 21 symptoms with a maximum score of 63 and a minimum score of 0. 28 Patients with a BAI score ≥10 was defined as having anxiety. 29 The SAS scale consisted of 20 test items, with each item categorized into 4 levels. The total score of the scale was 100, 30 and patients were defined as having anxiety if they scored ≥50. 31
The depression of the patients was measured by BDI and SDS scales. The BDI scale included 21 items, and each item was categorized into 3 levels to measure the depression of the patient. The total score ranged from 0–63, and patients with a total score ≥10 were defined as depression. 32 The SDS scale was used to assess the patient's depression. The scale comprised 20 items with a total score ranging from 0–100. A higher score for the patient indicated a higher level of depression. Patients were defined as depression if their total score was ≥50.30,31
Statistical analyses
Statistical software (SPSS V24, IBM Crop., USA) was utilized for the statistical analysis of the data for this study. Student's t, Mann-Whitney U, and χ2 tests were used for comparison between DR and NRDM patients. Univariate and stepwise forward multivariate analysis by logistic regression was performed to find the factors that had an association with the anxiety and depression of the DR patients. All factors shown in the univariate analysis were included in the multivariate analysis. Then, the independent risk factors were combined to analyze their ability to identify anxiety and depression in DR patients via the receiver operating characteristic (ROC) curves. P-values less than 0.05 were considered statistically different.
Results
Clinical features of DR and NRDM patients
The mean age of DR patients was 55.7 ± 10.5 years, and there were 131 (53.0%) females. NRDM patients had a mean age of 54.2 ± 13.1 years, and 121 (48.4%) patients were females. Notably, the percentage of unmarried DR patients was lower than that of unmarried NRDM patients (P = 0.029). Meanwhile, DM duration was elevated in DR patients versus NRDM patients (P < 0.001). Regarding biochemical indices, HbA1c in DR patients was higher than that in NRDM patients (P = 0.008). In addition, ALT (P = 0.004) and AST (P < 0.001) were decreased in DR patients versus NRDM patients, respectively. Other clinical characteristics did not vary between DR and NRDM patients (all P > 0.05). Among DR patients, there were 32 (13.0%) patients with proliferative DR and 115 (38.7%) patients with an impairment of visual acuity. The median (interquartile range) BCVA values of DR patients were 0.4 (0.2–0.5). More information on DR and NRDM patients is listed in Table 1.
Characteristics of NRDM and DR.
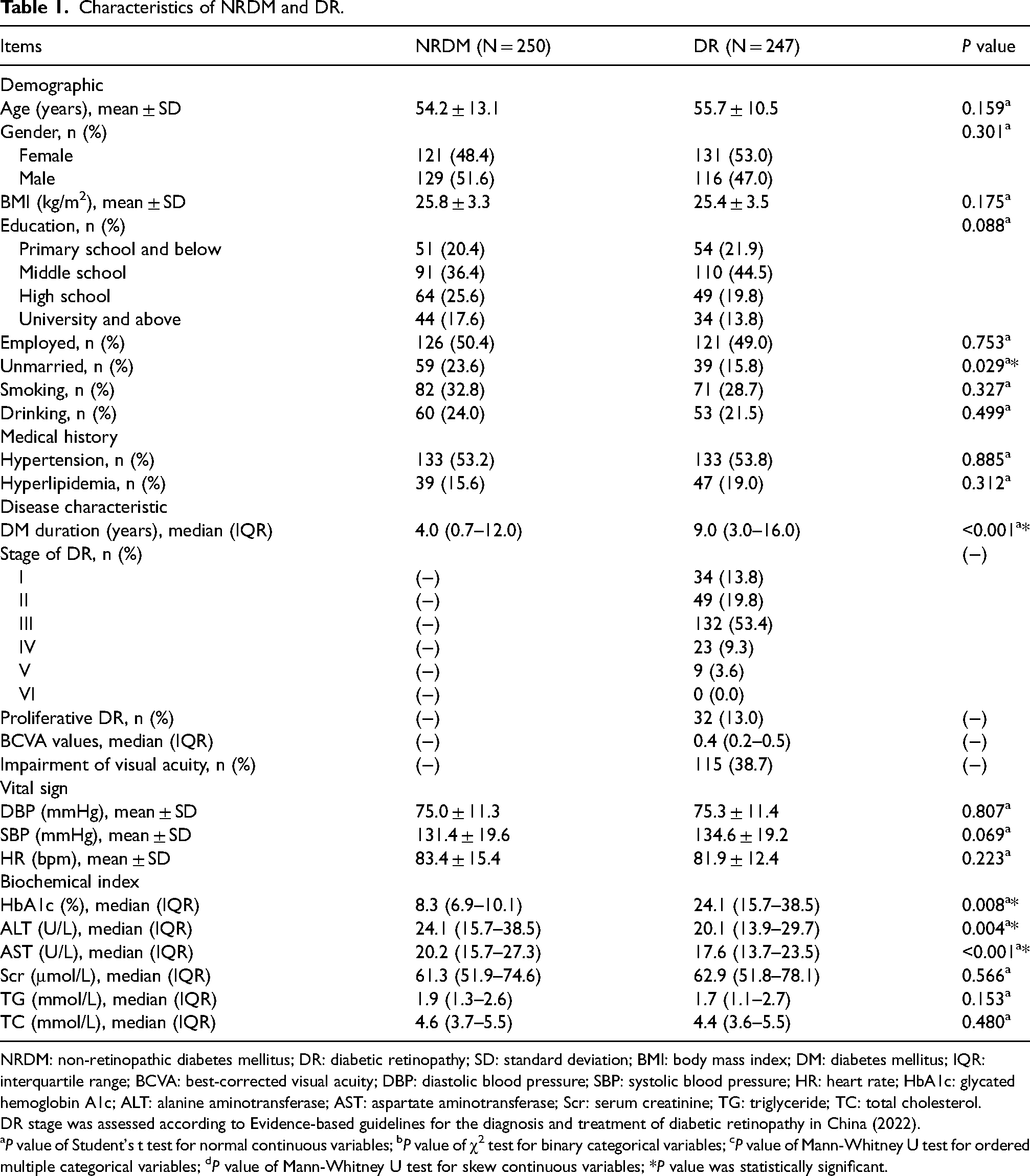
NRDM: non-retinopathic diabetes mellitus; DR: diabetic retinopathy; SD: standard deviation; BMI: body mass index; DM: diabetes mellitus; IQR: interquartile range; BCVA: best-corrected visual acuity; DBP: diastolic blood pressure; SBP: systolic blood pressure; HR: heart rate; HbA1c: glycated hemoglobin A1c; ALT: alanine aminotransferase; AST: aspartate aminotransferase; Scr: serum creatinine; TG: triglyceride; TC: total cholesterol.
DR stage was assessed according to Evidence-based guidelines for the diagnosis and treatment of diabetic retinopathy in China (2022).
aP value of Student's t test for normal continuous variables; bP value of χ2 test for binary categorical variables; cP value of Mann-Whitney U test for ordered multiple categorical variables; dP value of Mann-Whitney U test for skew continuous variables; *P value was statistically significant.
Comparisons of anxiety and depression between DR and NRDM patients
The prevalences (95% confidence interval (CI)) of anxiety were 38.5% (32.4%–44.6%) and 32.0% (26.2%–37.8%) from using the BAI and SAS, while those for depression were 31.6% (25.8%–37.4%) and 25.1% (19.7%–30.5%) from using the BDI and SDS in DR patients. In NRDM patients, the prevalences (95%CI) of anxiety were 27.6% (22.1%–33.1%) and 21.2% (16.1%–26.3%) from using the BAI and SAS, while those for depression were 22.8% (17.6%–28.0%) and 18.4% (13.6%–23.2%) from using the BDI and SDS.
BAI score (8.8 ± 5.2 versus 7.5 ± 4.2; P = 0.003) (Figure 1(a)) and BAI-defined anxiety rate (38.5% versus 27.6%; P = 0.010) (Figure 1(b)) were elevated in DR patients compared to NRDM patients. Likewise, SAS score (46.4 ± 8.5 versus 43.8 ± 8.0; P = 0.001) (Figure 1(c)) and SAS-defined anxiety rate (32.0% versus 21.2%; P = 0.006) (Figure 1(d)) were increased in DR patients compared to NRDM patients. In terms of depression, BDI score (8.3 ± 5.2 versus 7.1 ± 3.7; P = 0.005) (Figure 1(e)) and BDI-defined depression rate (31.6% versus 22.8%; P = 0.028) (Figure 1(f)) were increased in DR patients compared to NRDM patients. SDS score was also ascended in DR patients versus NRDM patients (44.3 ± 8.6 versus 41.9 ± 8.6; P = 0.001) (Figure 1(g)). However, SDS-defined depression rate was non-differential between DR patients and NRDM patients (25.1% versus 18.4%; P = 0.070) (Figure 1(h)).
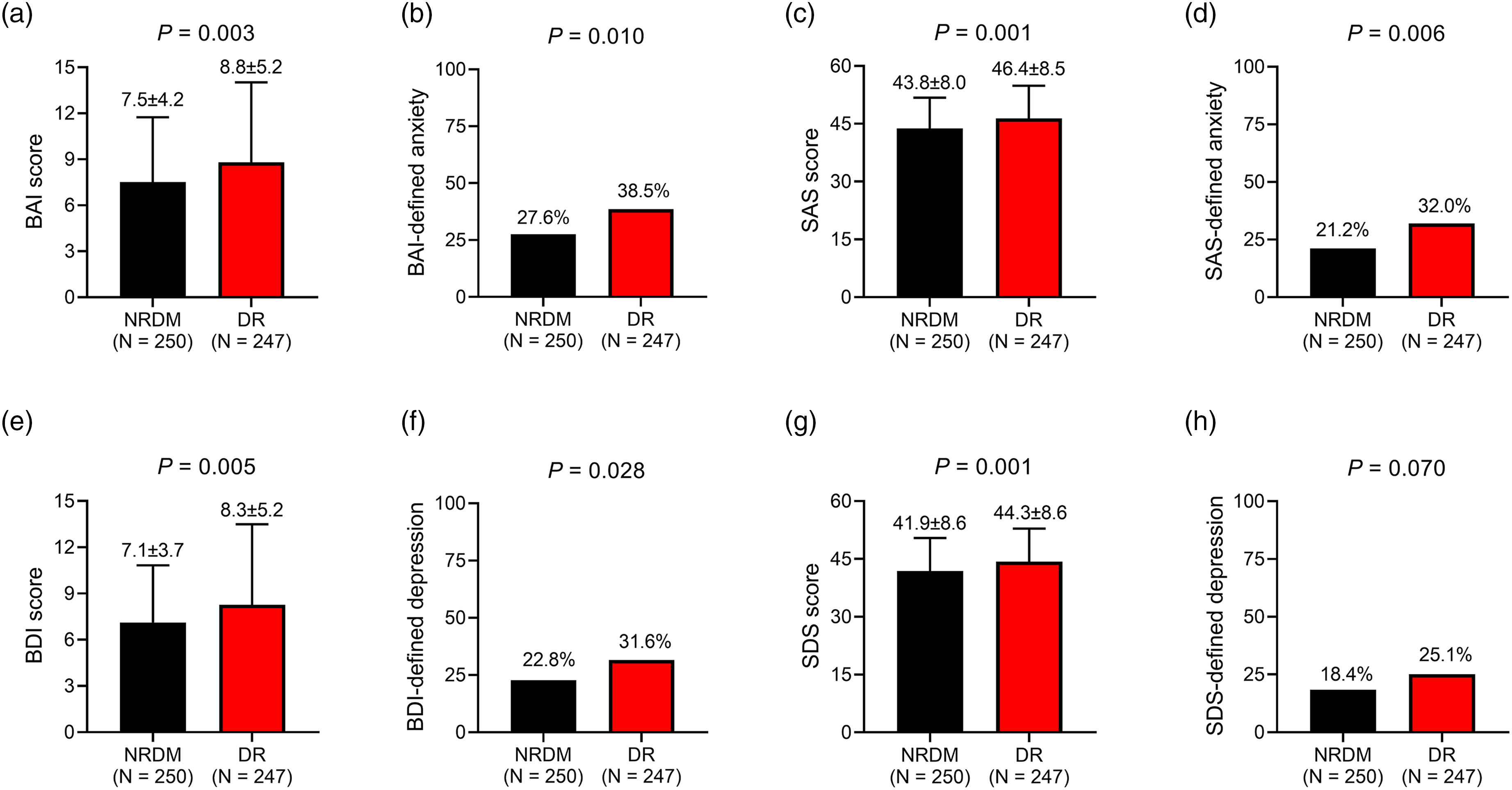
Anxiety and depression in DR and NRDM patients. Comparisons of BAI score (a), BAI-defined anxiety rate (b), SAS score (c), SAS-defined anxiety rate (d), BDI score (e), BDI-defined depression rate (f), SDS score (g), SDS-defined depression rate (h) between DR and NRDM patients.
Independent factors linked with BAI- and SAS-defined anxiety in DR patients
Univariate analysis by logistic regression showed that unmarried (yes versus no) [odds ratio (OR) = 2.113, P = 0.034], DM duration (OR = 1.036, P = 0.029), Scr (OR = 1.011, P = 0.033), higher stage of DR (OR = 4.535, P < 0.001), proliferative DR (yes versus no) (OR = 11.674, P < 0.001), and impairment of visual acuity (yes versus no) (OR = 1.836, P = 0.024) were linked with BAI-defined anxiety in DR patients. After the adjustment of variables, multivariate analysis by logistic regression illustrated that proliferative DR (yes versus no) was independently linked with BAI-defined anxiety in DR patients (OR = 11.143, P < 0.001) (Table 2).
Univariate and multivariate analysis by logistic regression of BAI-defined anxiety in DR.
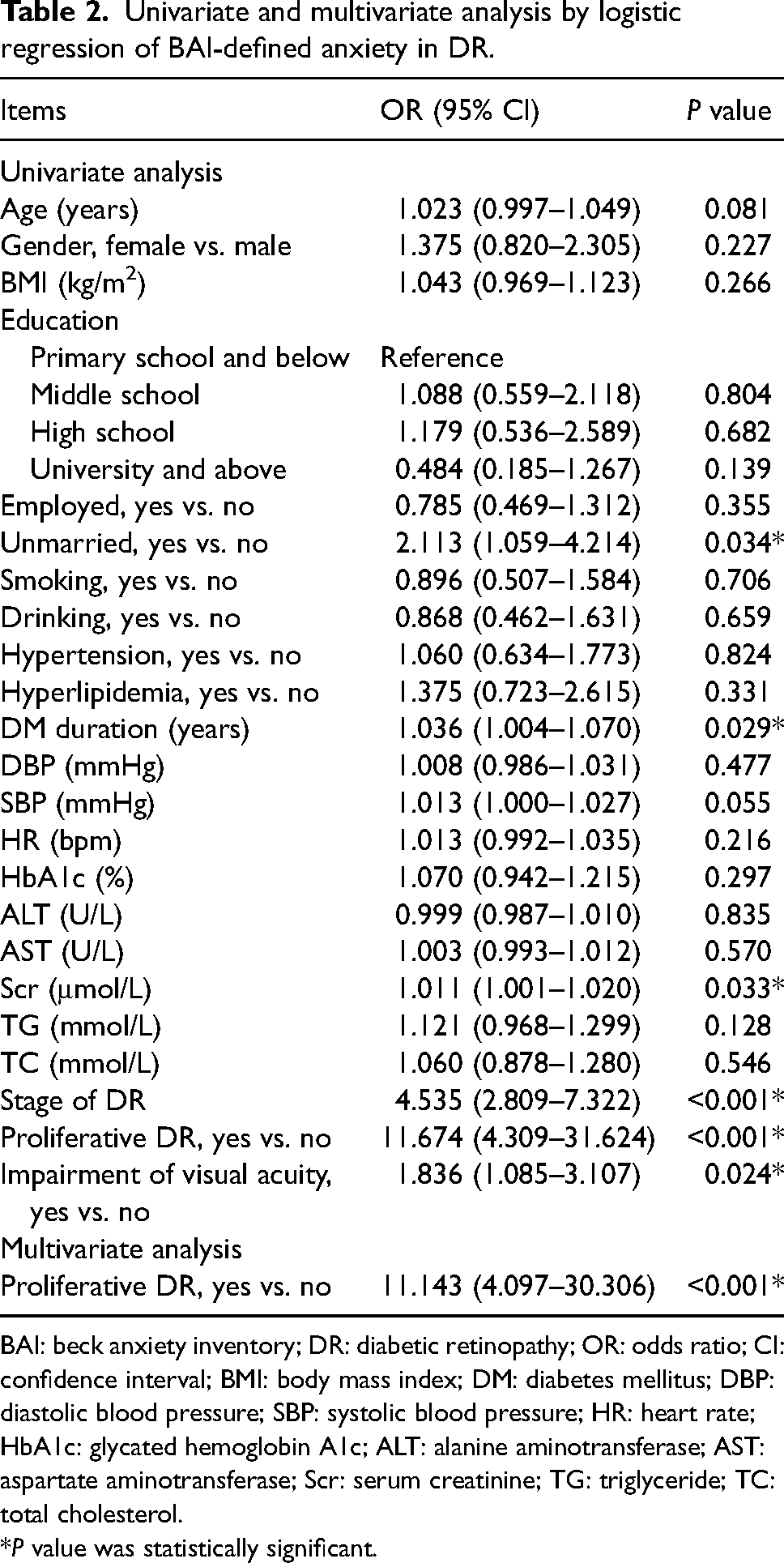
BAI: beck anxiety inventory; DR: diabetic retinopathy; OR: odds ratio; CI: confidence interval; BMI: body mass index; DM: diabetes mellitus; DBP: diastolic blood pressure; SBP: systolic blood pressure; HR: heart rate; HbA1c: glycated hemoglobin A1c; ALT: alanine aminotransferase; AST: aspartate aminotransferase; Scr: serum creatinine; TG: triglyceride; TC: total cholesterol.
*P value was statistically significant.
BMI (OR = 1.082, P = 0.047), unmarried (yes versus no) (OR = 2.066, P = 0.041), DM duration (OR = 1.045, P = 0.009), SBP (OR = 1.018, P = 0.016), Scr (OR = 1.012, P = 0.017), higher stage of DR (OR = 3.642, P < 0.001), proliferative DR (yes versus no) (OR = 16.927, P < 0.001), and impairment of visual acuity (yes versus no) (OR = 2.278, P = 0.003) were related to SAS-defined anxiety in DR patients. After adjustment, proliferative DR (yes versus no) was independently associated with SAS-defined anxiety in DR patients (OR = 16.312, P < 0.001) (Table 3).
Univariate and multivariate analysis by logistic regression of SAS-defined anxiety in DR.
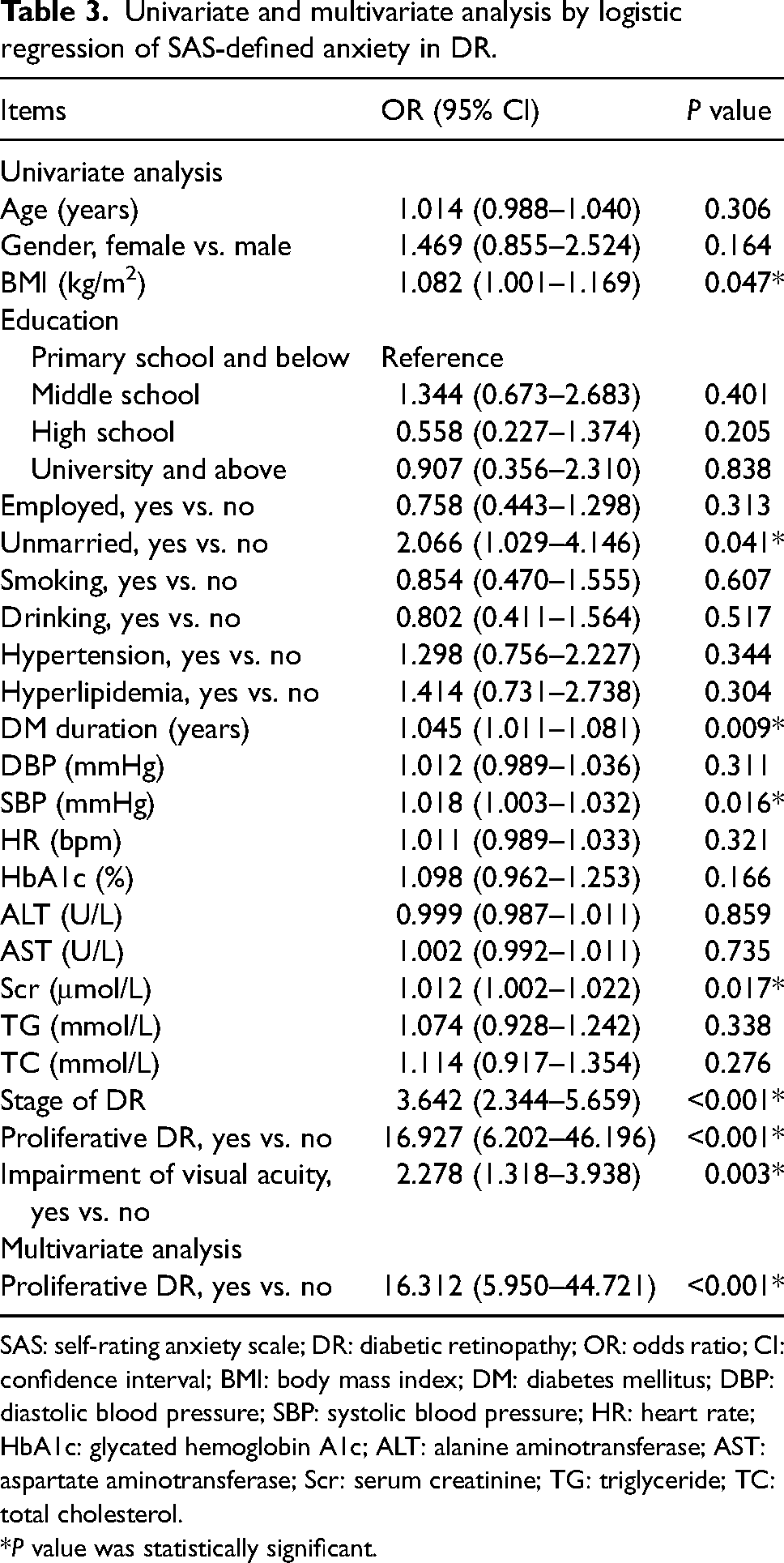
SAS: self-rating anxiety scale; DR: diabetic retinopathy; OR: odds ratio; CI: confidence interval; BMI: body mass index; DM: diabetes mellitus; DBP: diastolic blood pressure; SBP: systolic blood pressure; HR: heart rate; HbA1c: glycated hemoglobin A1c; ALT: alanine aminotransferase; AST: aspartate aminotransferase; Scr: serum creatinine; TG: triglyceride; TC: total cholesterol.
*P value was statistically significant.
Independent factors linked with BDI- and SDS-defined depression in DR patients
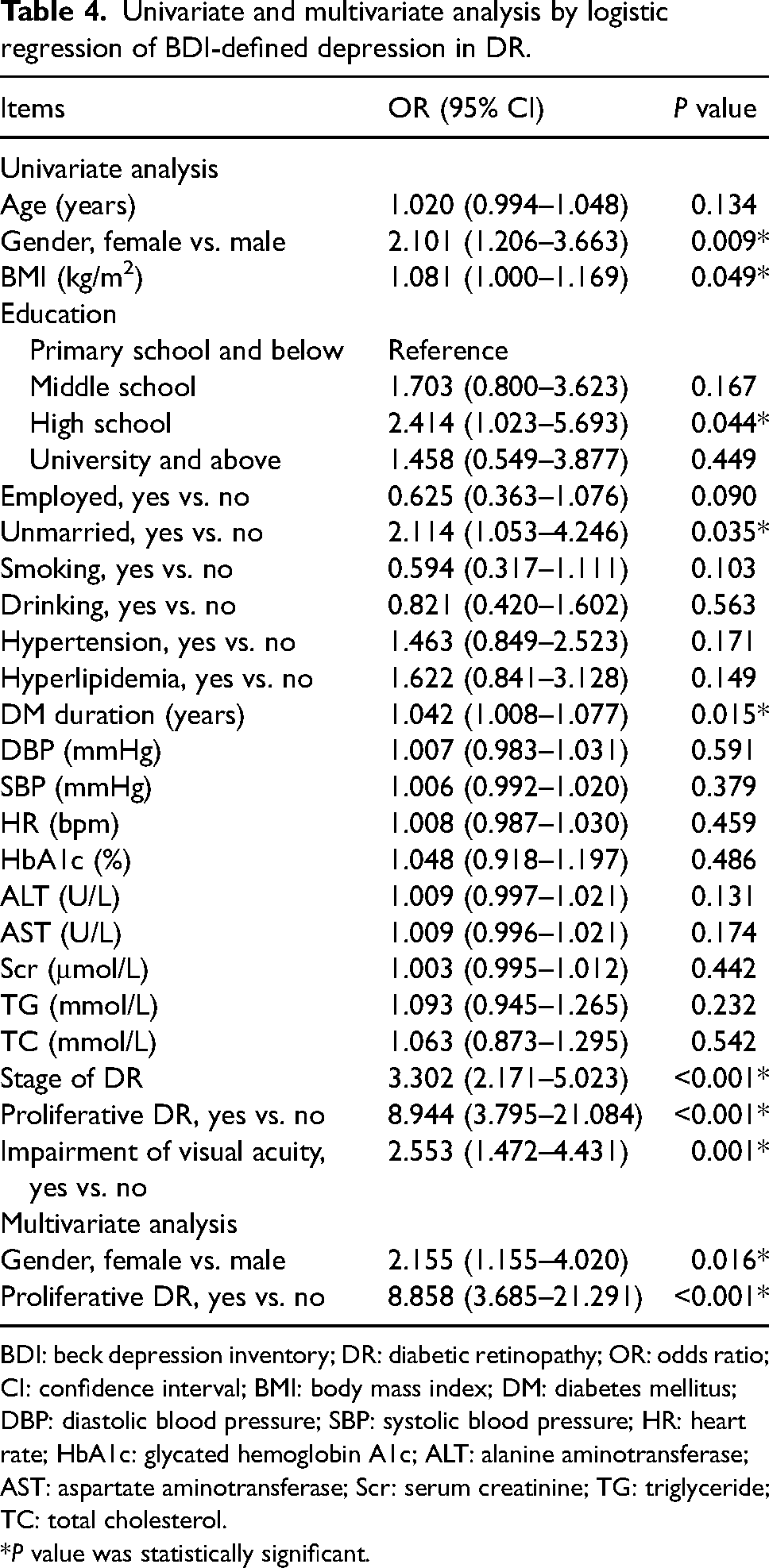
Based on univariate logistic regression analysis, gender (female versus male) (OR = 2.101, P = 0.009), BMI (OR = 1.081, P = 0.049), education (high school versus primary school and below) (OR = 2.414, P = 0.044), unmarried (yes versus no) (OR = 2.114, P = 0.035), DM duration (OR = 1.042, P = 0.015), higher stage of DR (OR = 3.302, P < 0.001), proliferative DR (yes versus no) (OR = 8.944, P < 0.001), and impairment of visual acuity (yes versus no) (OR = 2.553, P = 0.001) were linked with BDI-defined depression in DR patients. After the adjustment of variables, multivariate logistic regression analysis revealed that gender (female versus male) (OR = 2.155, P = 0.016) and proliferative DR (yes versus no) (OR = 8.858, P < 0.001) were independently related to BDI-defined depression in DR patients (Table 4).
Univariate and multivariate analysis by logistic regression of BDI-defined depression in DR.
BDI: beck depression inventory; DR: diabetic retinopathy; OR: odds ratio; CI: confidence interval; BMI: body mass index; DM: diabetes mellitus; DBP: diastolic blood pressure; SBP: systolic blood pressure; HR: heart rate; HbA1c: glycated hemoglobin A1c; ALT: alanine aminotransferase; AST: aspartate aminotransferase; Scr: serum creatinine; TG: triglyceride; TC: total cholesterol.
*P value was statistically significant.
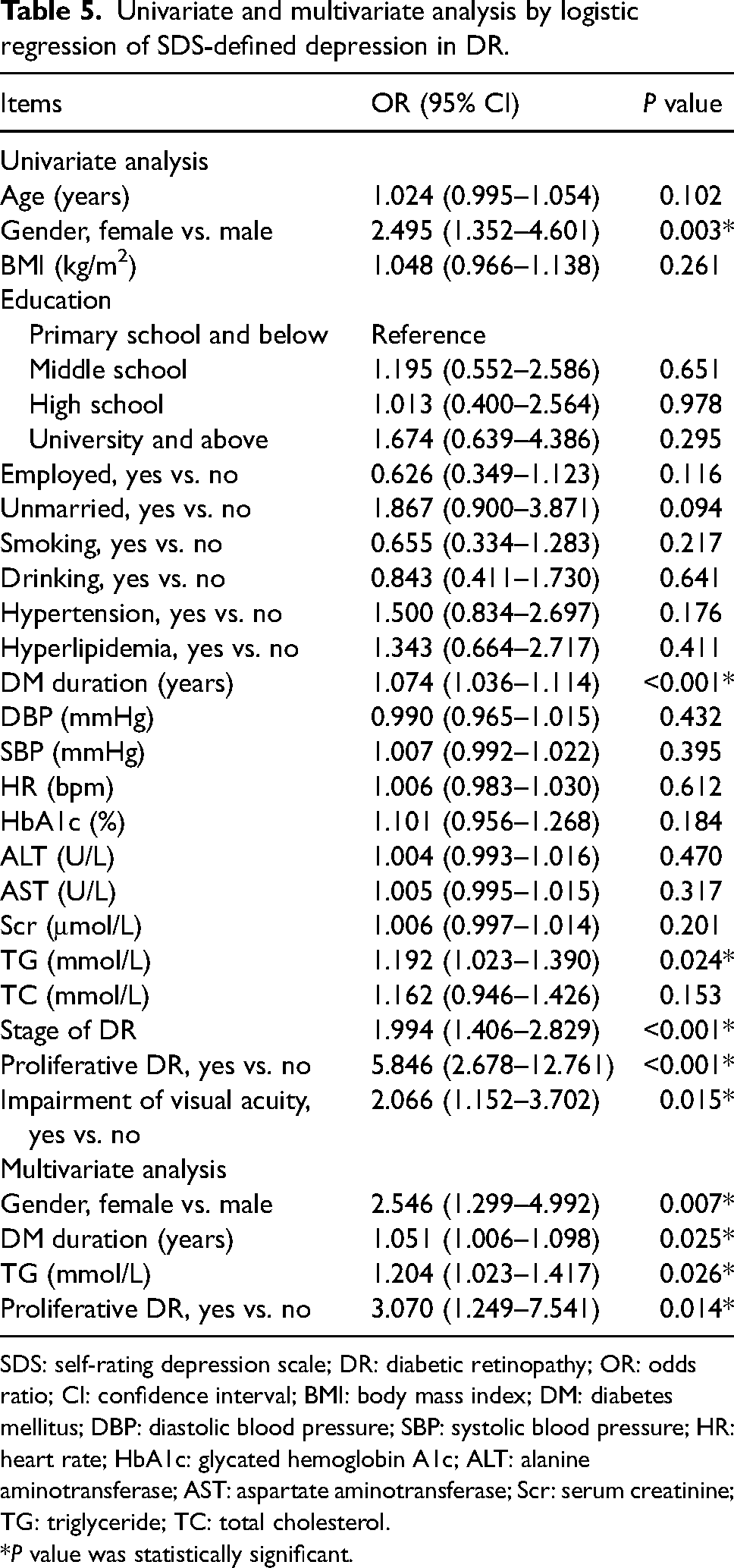
Gender (female versus male) (OR = 2.495, P = 0.003), DM duration (OR = 1.074, P < 0.001), TG (OR = 1.192, P = 0.024), higher stage of DR (OR = 1.994, P < 0.001), proliferative DR (yes versus no) (OR = 5.846, P < 0.001), and impairment of visual acuity (yes versus no) (OR = 2.066, P = 0.015) were related to SDS-defined depression in DR patients. After adjusting for variables, gender (female versus male) (OR = 2.546, P = 0.007), DM duration (OR = 1.051, P = 0.025), TG (OR = 1.204, P = 0.026), and proliferative DR (yes versus no) (OR = 3.070, P = 0.014) were independently associated with SDS-defined depression in DR patients (Table 5).
Univariate and multivariate analysis by logistic regression of SDS-defined depression in DR.
SDS: self-rating depression scale; DR: diabetic retinopathy; OR: odds ratio; CI: confidence interval; BMI: body mass index; DM: diabetes mellitus; DBP: diastolic blood pressure; SBP: systolic blood pressure; HR: heart rate; HbA1c: glycated hemoglobin A1c; ALT: alanine aminotransferase; AST: aspartate aminotransferase; Scr: serum creatinine; TG: triglyceride; TC: total cholesterol.
*P value was statistically significant.
The ability of the combination of independent factors to identify anxiety and depression in DR patients
Proliferative DR exhibited an acceptable capability to distinguish DR patients with BAI-defined anxiety from those without, with an area under curve (AUC) of 0.626 (95%CI: 0.551–0.700) (Figure 2(a)). Meanwhile, proliferative DR also had an acceptable ability to differentiate DR patients with SAS-defined anxiety from those without, with an AUC of 0.656 (95% CI: 0.577–0.735) (Figure 2(b)). The combination of female and proliferative DR showed an acceptable ability to distinguish DR patients with BDI-defined depression from those without, with an AUC of 0.696 (95% CI: 0.624–0.769) (Figure 2(c)). In addition, the combination of female, DM duration, TG, and proliferative DR displayed good ability in differentiating DR patients with SDS-defined depression from those without, with an AUC of 0.741 (95% CI: 0.664–0.819) (Figure 2(d)).
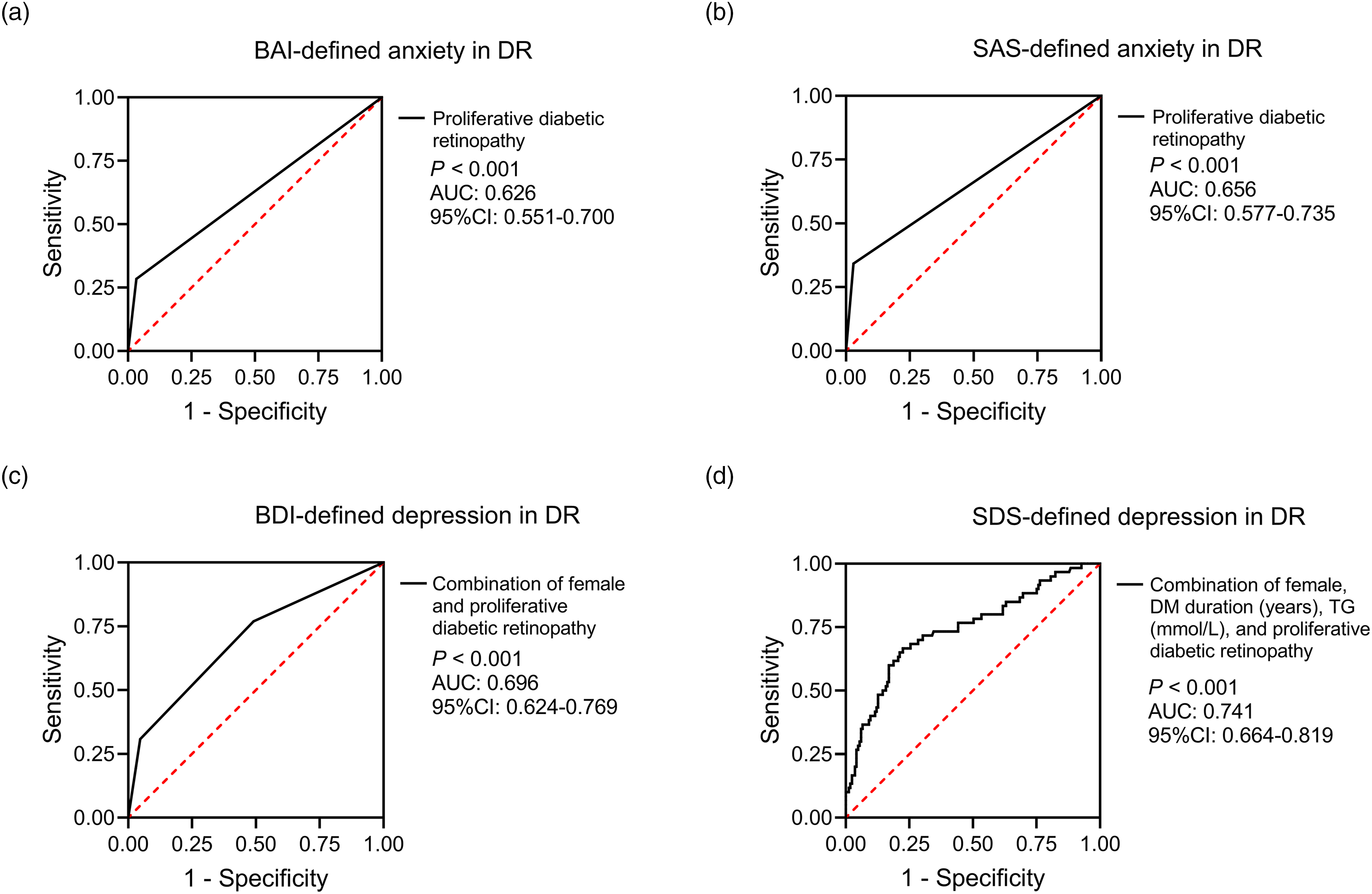
ROC curves for identifying anxiety and depression by independent factors in DR patients. The ability of proliferative DR to differentiate DR patients with BAI-defined anxiety from those without (a); the ability of proliferative DR to distinguish DR patients with SAS-defined anxiety from those without (b); the ability of female plus proliferative DR to differentiate DR patients with BDI-defined depression from those without (c); the ability of female plus DM duration plus TG and proliferative DR to distinguish DR patients with SDS-defined depression from those without (d).
The ability of BCVA values to identify anxiety and depression in DR patients
BCVA values had acceptable abilities in differentiating DR patients with BAI-defined anxiety, SAS-defined anxiety, BDI-defined depression, and SDS-defined depression from those without, with AUCs of 0.684 (best cut-off value: 0.550), 0.692 (best cut-off value: 0.350), 0.681 (best cut-off value: 0.350), 0.646 (best cut-off value: 0.175), respectively (Supplementary Table 1).
Discussion
Anxiety and depression are common symptoms in DR patients, which lead to a series of negative outcomes, such as decreased quality of life and deteriorated health conditions.8,9,33 Previous studies revealed that there were 13.5%–41.1% and 25.0%–40.5% of DR patients with anxiety and depression, respectively; however, these studies only used a single scale.9,10,12,13 Our study chose the BAI/BDI and SAS/SDS scales to assess anxiety and depression in DR patients. In our study, the prevalences (95%CI) of anxiety were 38.5% (32.4%–44.6%) and 32.0% (26.2%–37.8%) by BAI and SAS scales, while those for depression were 31.6% (25.8%–37.4%) and 25.1% (19.7%–30.5%) by BDI and SDS scales in DR patients, which were similar to these previous studies.9,10,12,13 In addition, one study found that the depression rate was higher in type 2 diabetes patients with DR than type 2 diabetes patients without DR. 34 Partly similar to this study, our study also revealed that anxiety and depression rates were increased in DR patients compared to NRDM patients (referring to DM patients without DR). 34 The possible explanation was as follows: The visual function of DR patients might be impaired 35 ; meanwhile, visual disabilities could increase the mental burdens of individuals.36,37 Thus, the anxiety and depression rates were higher in DR patients than in NRDM patients.
Considering that mental burdens are nonnegligible issues in DR patients, it is extremely important to explore anxiety- and depression-related factors for their management. In terms of the influence of different DR characteristics on anxiety and depression, some previous studies have disclosed that DR severity, visual acuity, diabetic macular edema, and proliferative DR were related to higher levels of anxiety or depression in DR patients.10,14,15 Moreover, one previous study exhibits that poor perceived social support is an anxiety- and depression-related factor in DR patients. 38 Another research reports that gender, salary, and laser treatment history are depression-related factors in type 2 DR patients. 39 The results of our study were partly similar to the findings of previous studies,14,15,39 which found that proliferative DR was independently related to BAI-defined and SAS-defined anxiety in DR patients. Additionally, proliferative DR, female, DM duration, and TG were independently associated with BDI-defined or SDS-defined depression in DR patients. It could be explained by the following points: (1) Proliferative DR reflected more severe disease conditions of DR patients, which might be related to increased anxiety and depression.14,40 (2) Females had a high sensitivity to sex hormone fluctuation that affected the modulation of mood and behavior, which could lead to the occurrence of depression. 41 (3) DR patients with longer DM duration had more complications (such as diabetic foot disease and cardiovascular disease) and worse health conditions, which might further increase their psychological burdens.42–44 (4) TG suppressed the secretion of melatonin from the pineal gland 45 ; meanwhile, the inhibition of melatonin might result in depression. 46 Notably, our study established four ROC models based on the combination of the independent factors of BAI-defined anxiety, SAS-defined anxiety, BDI-defined depression, and SDS-defined depression, respectively. Subsequently, it was identified that the value for identifying anxiety or depression of each model was good in DR patients. These predictive models could accurately screen DR patients with a high risk of anxiety or depression, which might contribute to timely providing treatment strategies for these patients. Thus, it was speculated that our predictive models might contribute to preventing anxiety and depression and improving the clinical management of DR patients.
The limitations of our study were as follows: (1) Our study only assessed anxiety and depression of DR patients at a single time point, and further studies were required to explore the long-term variation of anxiety and depression in DR patients. (2) All scales used in our study were self-evaluated, which might lead to a bias in results. (3) Our study was a single-center study, which might bias the results. (4) Due to the fact that the information on treatment and diabetic macular oedema of DR patients was not recorded in our study and we failed to backtrack these data, our study did not explore the influence of treatment methods and diabetic macular oedema on anxiety and depression in DR patients. (5) Although the diagnosis standard was the same, the diagnosis of DR patients and NRDM patients was made by multiple and different practitioners, which might cause inter-observer variability and affect the results of our study.
In conclusion, anxiety and depression are common in DR patients. Proliferative DR is an anxiety-related factor; while proliferative DR, female, DM duration, and TG are depression-related factors in these patients. Our study reveals the urgency of preventing anxiety and depression in DR patients; meanwhile, the identification of anxiety and depression-related factors may help prevent mental burdens and improve the management of DR patients. However, further longitudinal and multicenter studies are required for verification.
Supplemental Material
sj-docx-1-ejo-10.1177_11206721241300213 - Supplemental material for Prevalence and risk factors of anxiety and depression in diabetic retinopathy patients: A cross-sectional study using multiple scales
Supplemental material, sj-docx-1-ejo-10.1177_11206721241300213 for Prevalence and risk factors of anxiety and depression in diabetic retinopathy patients: A cross-sectional study using multiple scales by Hui Qiu in European Journal of Ophthalmology
Footnotes
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.