
Abstract
Introduction
To present a novel surgical technique for the treatment of a steep-walled filtering bleb following an Ahmed glaucoma valve implant. The primary aim was to alleviate the patient's discomfort and address associated corneal thinning, complications that can arise from this condition.
Methods
Case report and surgical technique. This case report describes a 29-year-old female who developed a dysesthesic filtering bleb following the implantation of a glaucoma drainage device. The employed surgical technique to address this complication involved the drainage of aqueous from the bleb using a 30-G needle, which effectively reduced its height. Subsequently, a compression suture was applied to maintain an appropriate bleb size.
Results
With the presented surgical technique, the ultimate control of an overhigh filtering bleb associated to a glaucoma drainage device was possible. Following the procedure, the patient's symptoms and the corneal thinning linked to the bleb's excessive size were successfully managed. Furthermore, the anatomy of the filtering bleb was preserved, and an optimal intraocular pressure outcome was achieved.
Conclusions
The removal of aqueous and the application of a compression suture are two surgical techniques traditionally used for managing the hypertensive phase of glaucoma drainage devices and for alleviating discomfort from blebs after classical filtering surgery, respectively. In the case presented, the combination of these two techniques effectively reduced the size of an excessively high filtering bleb associated with a glaucoma drainage device. This approach successfully resolved the patient's discomfort and corneal issues related to this complication.
Keywords
Introduction
A 29-year-old Caucasian woman previously diagnosed with pars planitis of unknown etiology, was referred to our center (Fundación Oftalmológica de la Comunidad Valenciana, FOM, Valencia, Spain) under the suspicion of bilateral steroid-induced glaucoma. During the initial assessment, her intraocular pressure (IOP) measured using Godmann applanation tonometry, was 60 mmHg in the right eye (OD) and 30 mmHg in the left eye (OS) despite maximum medical treatment (topical beta-blocker, topical alpha-2-agonist, topical carbonic anhydrase inhibitor and oral carbonic anhydrase inhibitor with potassium supplement). Gonioscopy examination revealed a very narrow angle, rated as grade 1 according to the Shaffer grading system. The angle was highly pigmented with peripheral anterior synechiae encompassing 360° of the angle circumference. Optic nerve optical coherence tomography (OCT) indicated a clinically significant thinning of the retinal nerve fiber layer, more pronounced in OD. Additionally, anterior OCT (CASIA 2, Tomey, Nagoya, Japan) confirmed the diagnosis of a narrow angle with anterior synechiae. Fundus examination showed an optic disc excavation with a ratio of 1:1 OD and of 0.4:1 OS. The patient also presented a subcapsular cataract in both eyes. Visual acuity (VA) was recorded as hand movement OD and 0.50 (logMAR notation) OS.
IOP was above normal limits despite maximal medical treatment. Therefore, a glaucoma surgery was indicated. The most appropriated procedure was a glaucoma drainage device (GDD) in combination with cataract surgery. The patient underwent surgery first on OD because it had a higher IOP, followed by OS one week later. Phacoemulsification and intraocular lens implantation were first performed following the conventional technique. Subsequently, an Ahmed glaucoma valve (New World Medical Inc, Cucamonga, Calif) was implanted superotemporally without complications. To cover the tube and ensure its stability, a Tutoplast (Tutogen Medical Inc, Clifton, NJ) fascia lata patch graft was used. The tube was positioned in the posterior chamber, specifically within the retropupillary space.
The day after surgery, the IOP was significantly reduced, registering at 8 mmHg OD and 10 mmHg OS. A postoperative treatment regimen was prescribed that included an antibiotic drop (quinolone drop) three times a day during 10 days, and a steroid drop (dexamethasone) in a tapering regimen: 1 drop every 1 h for the first week, every 2 h for the next 2 weeks, then every 3 h for the following month, every 4 h for another month, every 6 h for another month, every 8 h for another month, every 12 h for another month and, finally, every 24 h until the completion of 1 year. The filtering bleb was elevated and had a good vascularization, the anterior chamber was properly formed and the tube was correctly positioned in the retropupillary space, indicating a successful surgical outcome.
Six months after the surgery, the patient developed a high and translucent filtering bleb (Figure 1) on her OD. At this time, the IOP was 20 mmHg, and she was not on any antiglaucomatous medications. During the following weeks, the bleb enlarged further, leading to the formation of a significant corneal dellen (Figure 2). Consequently, the patient experienced several symptoms related to the filtering bleb, including pain, foreign body sensation, continuous tearing and mechanical ptosis that limited the spontaneous opening of the upper eyelid (Figure 3).
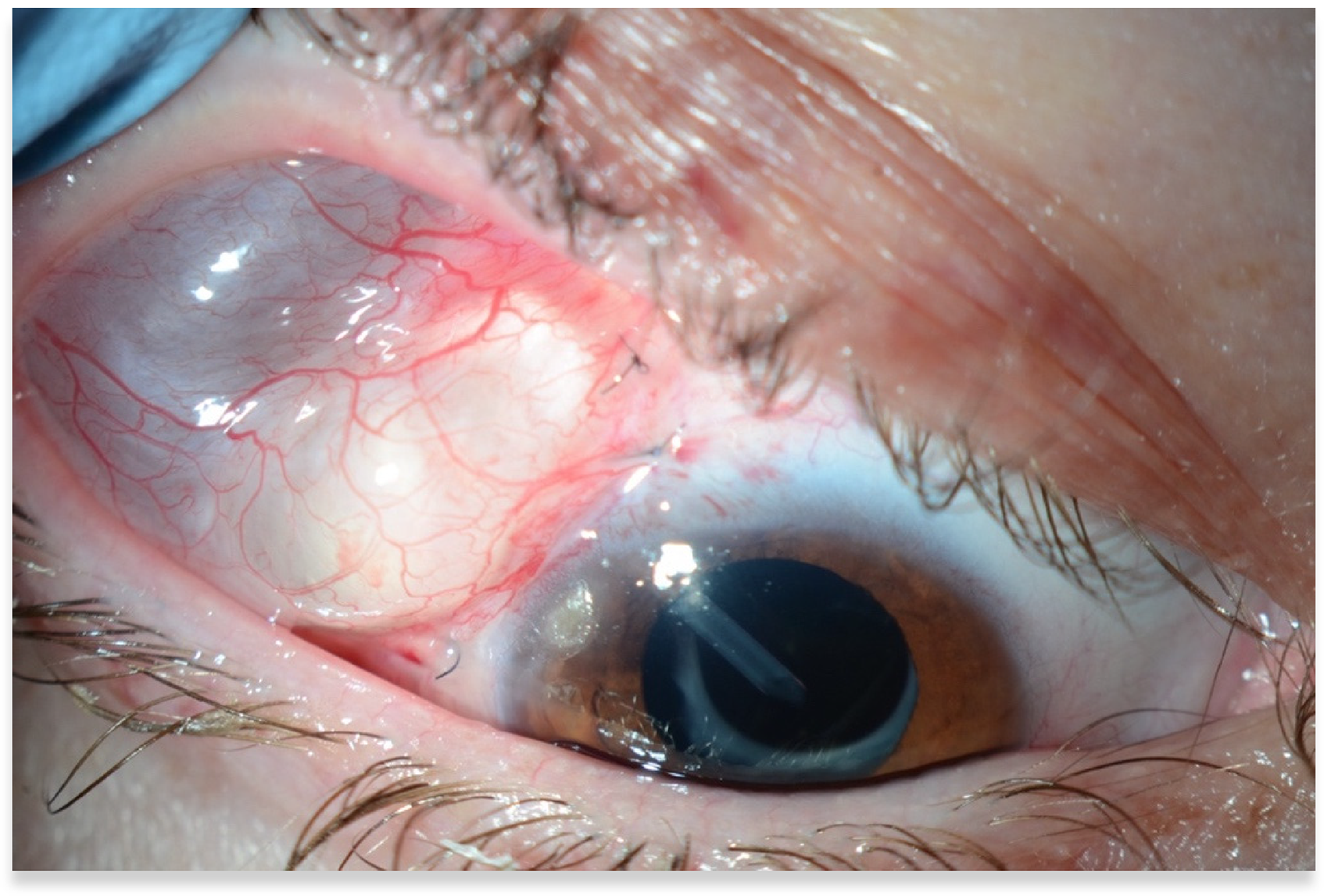
Od. Steep-walled superotemporal translucent bleb, with the tube visibly positioned in the retropupillary space.
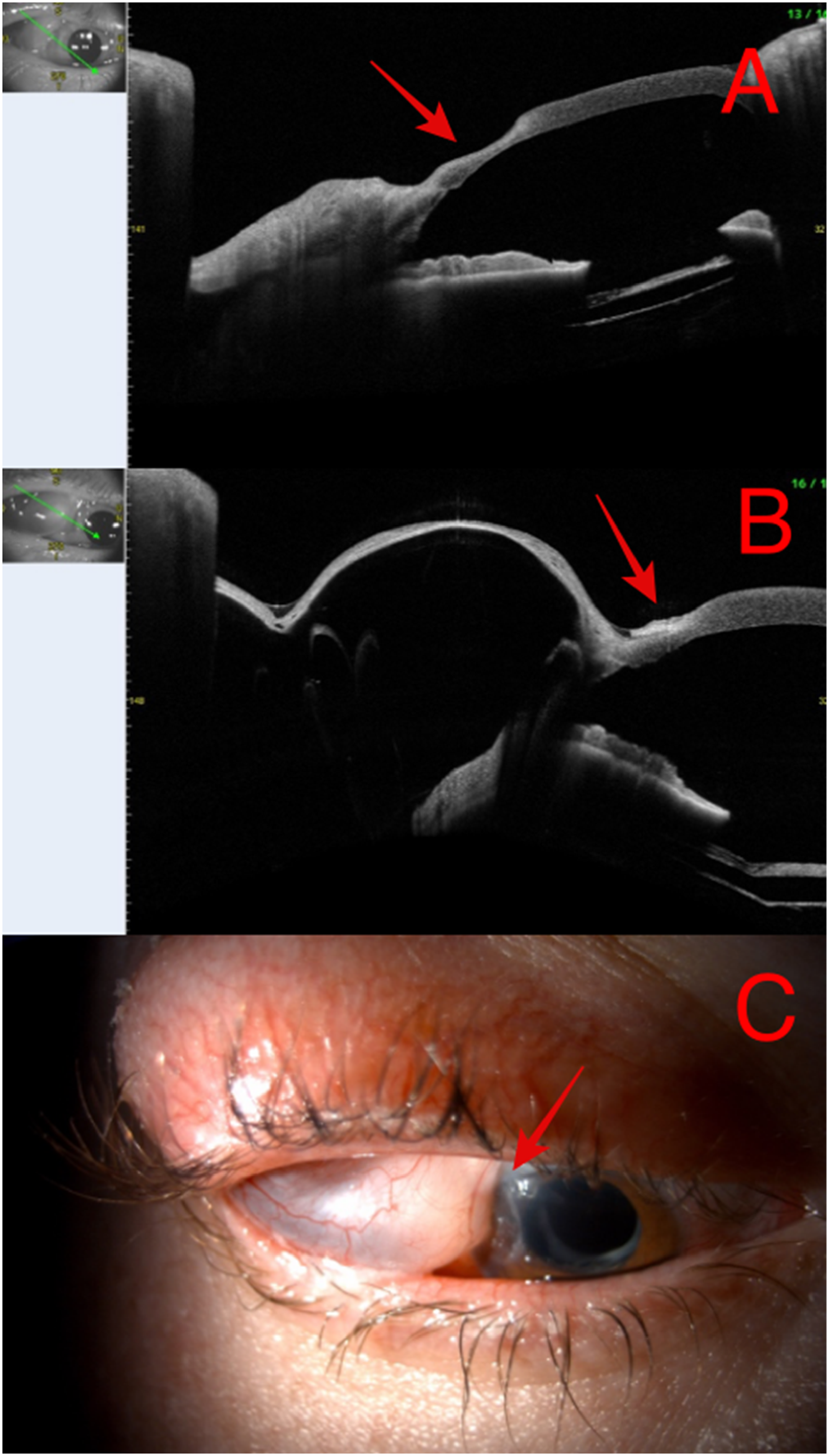
Corneal dellen associated with a steep-walled filtering bleb. Image A: anterior segment optical coherence tomography (AS-OCT) shows corneal thinning, indicated by a red arrow, corresponding to the corneal dellen. Imagen B: AS-OCT, red arrow points the corneal dellen adjacent to the steep-walled filtering bleb. Imagen C: red arrow points the corneal dellen as viewed under slit lamp examination, providing a direct visualization of the thinning area adjacent to the bleb.

Mechanical ptosis induced by the superotemporal step-walled filtering bleb.
The surgical technique for the treatment of a steepwalled dysesthesic filtering bleb of an Ahmed glaucoma implant is presented.
Methods
Surgical technique
The technique started with the aspiration of aqueous humor from the filtering bleb using a 30-G needle introduced via the anterior aspect of the bleb. To maintain this diminished size, a compression suture using a 7-0 polyglactin 910 (Vicryl ®) was placed. The suture was configured in an X-shape (Figure 4): the suture thread was first passed along one side of the bleb, then crossed to the opposite side, and this pattern was repeated in reverse. This specific suture configuration effectively created a simple net over the bleb, which served to prevent further enlargement.
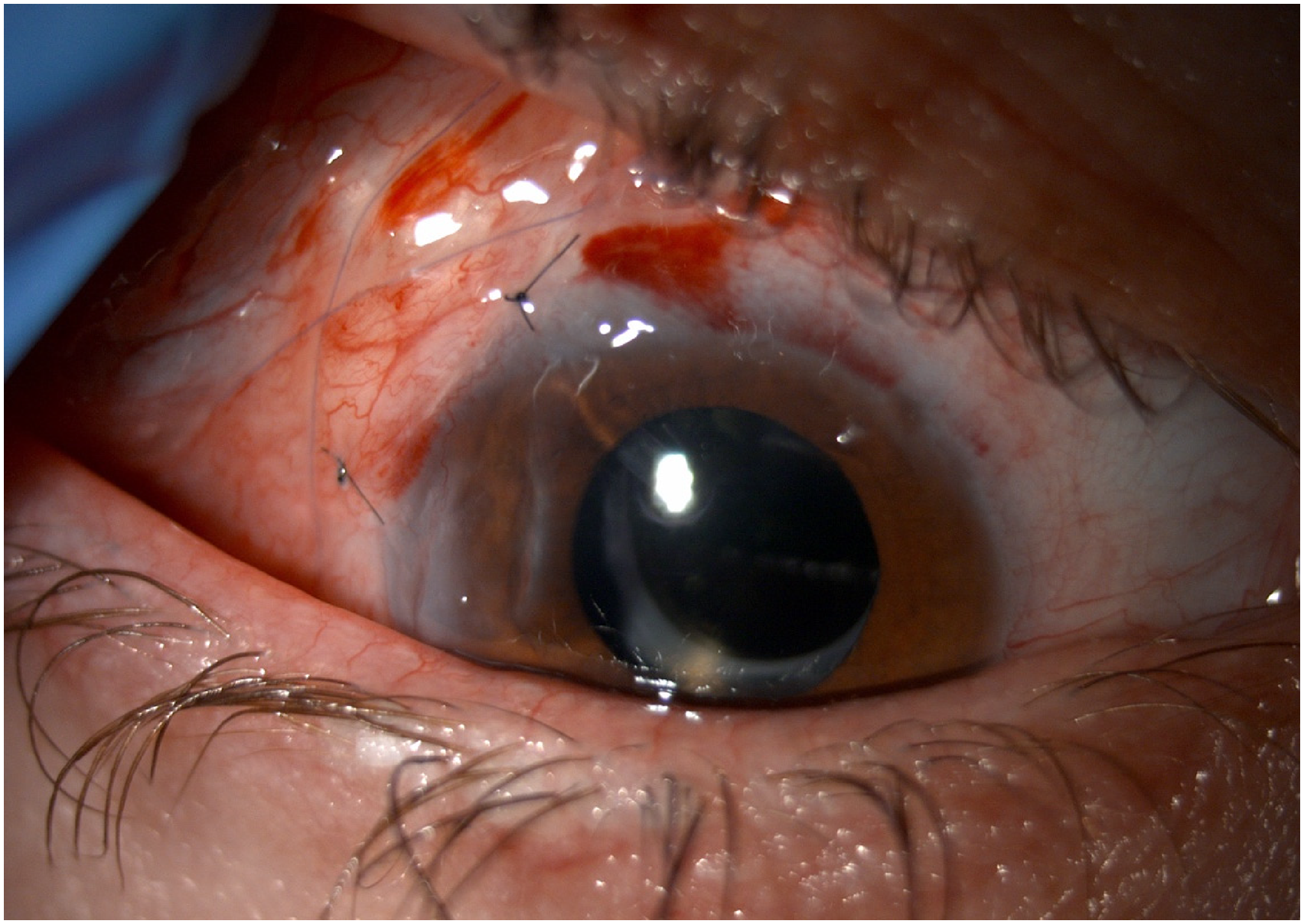
X shape compression suture over the filtering bleb.
Results
After the surgery, the size of the bleb was successfully reduced. The compression suture was fully absorbed by two months post-surgery, yet the bleb size remained stable, and the IOP was maintained at 12 mmHg without the need for antiglaucomatous medication (Figure 5).
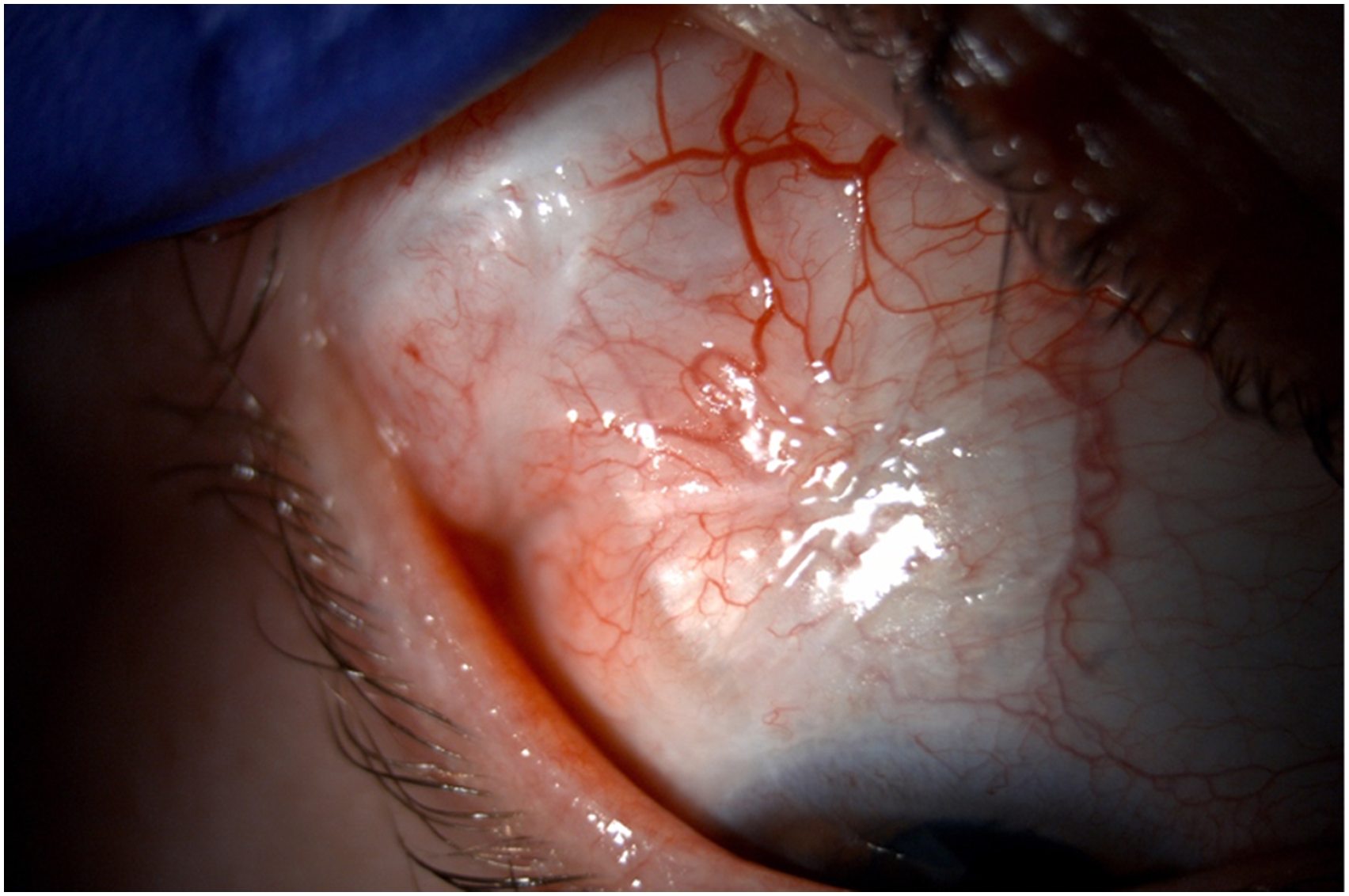
Aspect of the filtering bleb 1 month after the surgical procedure.
However, three months after the procedure, the patient presented with an elevated IOP of 32 mmHg, prompting the prescription of a topical combination of beta-blocker and carbonic anhydrase inhibitor.
Over the next three years of follow-up, the patient´s IOP remained within normal limits, varying from15 to 21 mmHg, with the prescribed topical treatment.VA remained unchanged from the initial assessment (hand movement).
Discussion
Bleb dysesthesia refers to the burning, tearing, pain, or ocular discomfort often associated with mitomin C-created filtering blebs after classic filtering surgery. 1 Treatments options to manage these symptomatic blebs have include lubricants, Nd:YAG laser, argon laser, compression sutures to flatten the bleb, bleb window cryopexy, surgical excision, bleb reduction or sutureless revision.2–7 Although varied techniques have been reported, there is no definitive “best” surgical approach. 8
The patient of this report exhibited bleb dysesthesia attributed to a steep-walled filtering bleb resulting from an Ahmed glaucoma implant. Bleb dysesthesia associated with GDDs has not been extensively documented, as this complication has traditionally been associated to conventional glaucoma filtering surgeries, particularly trabeculectomy. Its occurrence appears to be correlated with the usage of antimetabolites in such surgical procedures.1,3
GGDs, also termed as tube shunts or aqueous shunts, are conduits transporting aqueous from within the eye to the subconjunctival space.9,10 The ultimate end result is to create a drainage bleb over the tube plate. There have been described 3 distinct phases of bleb development. The initial stage of the bleb is the hypotensive phase and occurs before the aqueous reaches the plate surface, and is due to the conjunctival reaction to the plate, lasting from 7 to 10 days. The succeeding phase occurs after aqueous reaches the plate surface and it is named the hypertensive phase, which is due to the patient´s tissue reaction to the presence and concentration of cytokines in the aqueous, reaching its peak between weeks 5 to 6 after surgery. This phase is very important in the prognosis of the surgery. It does not occur in every patient but, in those in which occurs, its development has been shown to result in a higher incidence of bleb fibrosis. Thus, lowering the pressure during this phase is important, as this will reduce the accumulation of cytokines that may produce bleb fibrosis and possible failure of the bleb, compromising the success of the glaucoma surgery. This phase is followed by a stable stage. 11
During the hypertensive phase of aqueous shunts, the initiation of pressure-lowering medications is recommended when the intraocular pressure (IOP) exceeds the threshold typically deemed high, usually greater than 21 mmHg. Digital massage could be indicated along with the topical medication. In the cases in which pressure does not decrease with the above measures, bleb revision with needling of the bleb is an option for both nonvalved and valved implants with encapsulated blebs and, only in the case of the nonvalved implants, stent removal and/or suturelysis should be considered. Surgical excision of the encapsulated bleb has been recommended in cases that do not respond to needling. 12 As an alternative method, it has been described the removal of aqueous from the bleb, that can be simply done using a 30-G needle, resulting in immediate lowering of the IOP. 11
To reduce the size of the symptomatic, elevated filtering bleb in the reported case, this method described for managing the hypertensive phase following GDD implantation was employed. This technique involved the aspiration of aqueous humor from the filtering bleb using a 30-G needle. This resulted in an immediate reduction of the size of the bleb without an excessive manipulation of this structure. To maintain the reduced size of the bleb, this technique was combined with a compression suture. This conjunctival compression technique has been described for the addressing of the bleb discomfort following classic filtering surgery. 13 Therefore, the presented surgical technique is combination of two procedures: one that is described for the control of the hypertensive phase associated to the GDDs, and another that is described for the management of symptomatic blebs related to the use of antimetabolites during classic filtering surgery.
Following the surgical intervention, there was a successful reduction in the size of the bleb. Over the subsequent three-year follow-up period, the patient's symptoms resolved completely, there was no further progression of corneal thinning, and IOP remained within normal limits with the topical antiglaucomatous treatment (Figure 5).
It is important to note that the conjunctival compression technique, previously described for addressing discomfort associated with blebs following classical filtering surgery, focuses on revising blebs that are accompanied by normal or low intraocular pressure. 14 Typically, this approach results in an IOP increase. In the presented case, there was an increasement of the IOP three months after the procedure, that was successfully controlled with topical antiglaucomatous medication during the next three years of follow up. This increasement could be because the compression suture induced some grade of fibrosis. The reduction in the bleb´s size after the suture could also be involved, because the area through which the aqueous humor drained, was smaller after this surgical technique. We informed the patient about this possible consequence, and she decided to undergo the procedure, as the symptoms were very uncomfortable and incompatible with their daily lives.
With the mentioned procedure, it was possible to control the size of an enlarged filtering bleb secondary to a GDD. This was effective in relieving the patient´s symptoms and in resolving the corneal dehydration related to the excessively high bleb. It is important to consider that an IOP increasement could be induced, and to inform the patient about this possible consequence. Also, the patient reported in this case had a very low VA (hand movement) at the first appointment, that remained unchanged after the procedure. Patients with better visual acuity should be monitored for glaucoma progression because of this risk of IOP increasement.
To the best of the authors’ knowledge, the technique of aqueous removal aimed at reducing the size of a steep-walled filtering bleb causing patient discomfort has not been previously documented in the literature. Likewise, the use of a compression suture to address bleb dysesthesia in the context of GDDs has not been reported. This case represents the first documented case where both techniques have been employed concurrently in a single procedure. This novel combination may offer glaucoma specialists a valuable strategy for managing this rare, yet potentially challenging, complication associated with GDDs.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Compliance with Ethical standards
Informed consent was obtained from every patient previous to surgery and they were informed about the use of their data and images in this paper.