
Abstract
Study purpose
to compare single- site viscotrabeculotomy in one eye and double-site rigid probe viscotrabeculotomy in the other eye of the same patient with Primary congenital glaucoma to evaluate the effect of the extent of angle treatment on success rate in the study's locality.
Patients and Methods
This prospective randomized study included 70 eyes of 35 children diagnosed with bilateral PCG who attended Mansoura Ophthalmic Center from June 2021 to July 2023. For each patient, one eye underwent single-site rigid probe viscotrabeculotomy (Group S: 35 eyes) and the fellow eye underwent double- site rigid probe viscotrabeculotomy (Group D: 35 eyes). At one-year follow up, complete success was defined as IOP >5 mmHg and ≤16 mmHg without any further IOP-lowering medications and qualified success when IOP ≤16 mmHg with using IOP-lowering medications. Failure was defined as IOP more than 16 mmHg despite the use of IOP-lowering medications, the need for other glaucoma surgery to control IOP or hypotony.
Results
Single-site rigid probe viscotrabeculotomy showed a one-year complete success rate of 88.57% and for double-site viscotrabeculotomy was 91.43% but the difference was not statistically significant (p-value 0.9). There were no major complications in both groups, hyphema was the most common complication and was self-limited
Conclusion
Single-site viscotrabeculotomy shows comparable results to double-site viscotrabeculotomy in PCG preserving more than half of the angle in the former for a second possible angle surgery in recurrent cases.
Key messages
Congenital glaucoma is a major potential cause of blindness in the area Angle surgery is the first line of treatment for most authors; different techniques have been adopted to target a larger extent of the angle with different results between authors. This study evaluates double- site rigid probe viscotrabeculotomy as a method for increasing the extent of the treated angle and comparing this with single- site viscotrabeculotomy in this study's locality
Introduction
Congenital glaucoma presents from birth to three years of age and is secondary to abnormal differentiation of trabecular meshwork (TM) and anterior chamber angle. This leads to subsequent hindrance to aqueous humor drainage. Below the age of 3 years, the growth of the eye increases in response to high intraocular pressure IOP. 1 Children affected with congenital glaucoma usually present with enlarged eyes (buphthalmos), corneal edema, corneal opacity, and Descemet's membrane rupture (Haab's striae). 2
Other signs at presentation include bluish sclera secondary to scleral thinning with ocular stretching, iris atrophy, abnormally deep anterior chamber, and in more advanced cases progressive glaucomatous optic atrophy may be present. In addition, diminished vision and visual field contraction can occur and be noticed in older children. If primary congenital glaucoma is left untreated, the loss of vision usually occurs. 2
Surgery is the definitive treatment. If early diagnosis and treatment occur, better vision can be expected for more than 50% of patients. Children are at a higher risk of failure and complications post-filtering surgery than adults, mostly due to ocular enlargement and aggressive healing. 3
As the trabecular pathway of aqueous humor drainage represents the major way of drainage, this part may present significant resistance to aqueous drainage in primary congenital glaucoma eyes. 4 Angle surgery either ab-externo trabeculotomy or ab-interno goniotomy has comparable success rates. Corneal clarity is important for goniotomy, while trabeculotomy is indicated in eyes with inadequate clarity. 5 Longer incisions in Schlemm's canal can increase the magnitude of the reduction of intraocular pressure. 6 Thus, modifications in trabeculotomy were done including GAAT, circumferential suture trabeculotomy, flexible illuminated microcatheter, and 2-site trabeculotomy using the rigid probe trabeculotome. 5
Viscotrabeculotomy is one modification in which viscoelastic is injected in Schlemm's canal before trabeculotomy and to form the anterior chamber. Many authors reported that using viscoelastic lowers the incidence of postoperative hyphema and improves the overall success of the procedure possibly by acting as a barrier separating trabeculotomy cleft edges and decreasing fibroblastic proliferation at the site of trabeculotomy. One drawback of the use of viscoelastic in trabeculotomy is the possibility of postoperative IOP spikes that are usually self-limited.7,8,9
As angle surgery is the basic line of treatment of PCG, this study was conducted to compare the postoperative outcomes of single-site viscotrabeculotomy in one eye and double-site rigid probe viscotrabeculotomy in the other eye of the same patient to evaluate the effect of the extent of angle treatment on success rate in the study's locality.
Patients and methods
This study was a prospective randomized comparative trial conducted in Mansoura Ophthalmic Centre, Mansoura University, Egypt, from June 2021 to July 2023. The study included all children presented with bilateral PCG during the survey. Thirty-five patients were included, one eye for every patient received single-site rigid probe viscotrabeculotomy (Group S), and the other eye received double-site metal probe viscotrabeculotomy (Group D). Randomization was done using the closed envelope method for the type of surgical intervention of the more severely affected eye of each of the 35 children, and the second eye received the other intervention 1–2 weeks later.
The Research Local Ethical Committee approved the research protocol of this study. Informed consent was taken from the parents or the caregivers before being enrolled in the study.
The cases of PCG were diagnosed according to the diagnostic criteria defined in the last Childhood Glaucoma Research Network classification 10 in which two of the following criteria were required; intraocular pressure >21 mmHg, Haab's stria, corneal edema, horizontal corneal diameter ≥11 mm in new-born, > 12 mm in children <2 years old and >13 mm in any age, increased (>0.3) or asymmetric (>0.2) cup–disc ratio or progressive myopia or myopic shift with increased AL. In addition, Exclusion criteria included children with a history of previous ocular surgery or trauma, patients with recurrent glaucoma, secondary childhood glaucoma as glaucoma following cataract surgery, glaucoma associated with local ocular abnormalities or syndromes. Children with initially unilateral PCG at the time of presentation were excluded from the study even if subsequent follow -up demonstrated that the disease developed in the fellow initially free eye
The preoperative examination was done for all cases under sevoflurane inhalational general anaesthesia. The preoperative clinical data included the patient's age at the time of first presentation and at the time of surgery, gender, consanguinity, family history, systemic associations, and medical treatment details. A complete examination of the anterior segment included measuring the horizontal corneal diameter (white to white) using a surgical calliper; and measuring intraocular pressure using hand-held Perkins applanation tonometry (Haag–Streit, Harlow, UK), just after the induction of general anaesthesia as soon as the eyes became centralized.
Corneal clarity was assessed with the surgical microscope; the fundus was examined by binocular indirect ophthalmoscope when possible. In addition, the axial length was measured by A-scan Ultrasonography, and B-scan ultrasonography was used to exclude any intraocular pathology using Nidek US-4000/500 Echo scan. Severity was calculated before surgery according to Al-Hazmi et al. 2005. 11 This score classifies cases into mild, moderate, or severe according to IOP, corneal diameter, and corneal clarity
Single- site viscotrabeculotomy and double-site viscotrabeculotomy were compared in this study
Group S: Single-site rigid probe viscotrabeculotomy: Vicryl 7/0 corneal traction suture was taken. A superonasal conjunctival periotomy was performed followed by gentle diathermy. A 3 mm × 3 mm triangular scleral flap was made. A 2 mm radial incision was made from the grey zone to the white zone in the flap bed. An incision was made deeper with caution until the outer wall of Schlemm's canal was opened and aqueous humour was observed. Viscocohesive Viscoelastic (Healon) was used to dilate Schlemm's canal before trabeculotomy using a 30 gauge viscotrabeculotomy cannula. A metal trabeculotome was used to cannulate and dissect through the inner wall of SC in both directions into the AC. Healon was injected into the AC. The scleral flap and conjunctiva were then sutured with interrupted 10–0 nylon sutures with embedding of knots. Subconjunctival antibiotics (gentamicin) and steroids (dexamethasone) were lastly injected.
Group D: Double site metal probe viscotrabeculotomy (Figure 1): After performing the same technique in group A at the superonasal part with filling of the AC with Healon to prevent hypotony and facilitate the inferotemporal viscotrabeculotomy, a traction suture was subsequently passed through the lower corneal limbus to facilitate exposure of the lower sclera. An inferotemporal conjunctival periotomy and fashioning of an inferotemporal scleral flap were done. According to Schlemm's canal, Healon injection is followed by metal probe trabeculotomy by the same technique prescribed before. Tight closure of scleral flap and conjunctiva with 10/0 nylon suture and subconjunctival injection of antibiotics and steroids were done.

Steps of double- site viscotrabeculotomy: (A) vicryl 7/0 Corneal traction suture, (B) Superonasal conjunctival periotomy, (C) Gentle cautery of bleeding vessels, (D) Fashioning of superonasal trap door, (E) Radial incision to localize Schlemm's canal, (F,G) Left and right upper rigid probe trabeculotomy after Healon injection to dilate the canal of schlemm, (H) Closure of scleral flap and conjunctiva with interrupted 10/0 nylon sutures after filling the AC with Healon (I) Inferotemporal corneal traction suture, conjunctival periotomy and fashioning of inferotemporal trap door, (J,K) Left and right lower rigid probe trabeculotomy, (L) Closure of lower scleral flap and conjunctiva with interrupted 10/0 nylon sutures.
After either surgery, children were prescribed a fixed combination of tobramycin and dexamethasone 0.1% drops to be administered four times daily and gradually tapered over 4 weeks. The cases were followed under sevoflurane inhalational general anaesthesia at 1 week, 1 month, and every 3 months, for at least 12 months. Follow- up parameters at each visit included IOP, corneal diameter, corneal clarity, cup disc ratio, axial length, and refraction. Any postoperative complications, the addition, and the number of antiglaucoma medications were recorded.
The success rate was calculated at a one-year follow-up. IOP control was defined as Complete success when IOP >5 mmHg and ≤16 mmHg without any further IOP-lowering medication at the last follow- up visit. Qualified success when IOP ≤16 mmHg but with the use of IOP- lowering medications. Failure was defined as IOP of more than 16 mmHg despite the use of IOP lowering medication, needing other glaucoma surgery to control IOP or hypotony: IOP ≤5 mmHg persistent for more than two weeks (transient hypotony was not considered a failure).
Statistical analysis
The data was analyzed using the Statistical package for Social Science (IBM Corp. Released 2017.), IBM SPSS Statistics for Windows, Version 25.0. Armonk, NY: IBM Corp.). The Chi-Square test was used to examine the relationship between two qualitative variables. Fisher Exact/ Monte-Carlo test was used to measure the relationship between two qualitative variables when the expected count is less than 5 in more than 20% of cells. Student T Test was used to assess the statistical significance of the difference of parametric variables between the two study group means. Mann Whitney Test was used to evaluate the statistical significance of the difference of a non-parametric variable between two study groups. ANOVA Test was used to measure the statistical significance of the difference of parametric variables between more than two study groups’ means. Kruskal-Wallis Test was used to assess the statistical significance of the difference of a non-parametric variable between more than two study groups. The log- rank test is used to test the null hypothesis that there is no difference between the populations in the probability of an event at any time point. A p -value is considered significant if <0.05 at a confidence interval of 95%.
Results
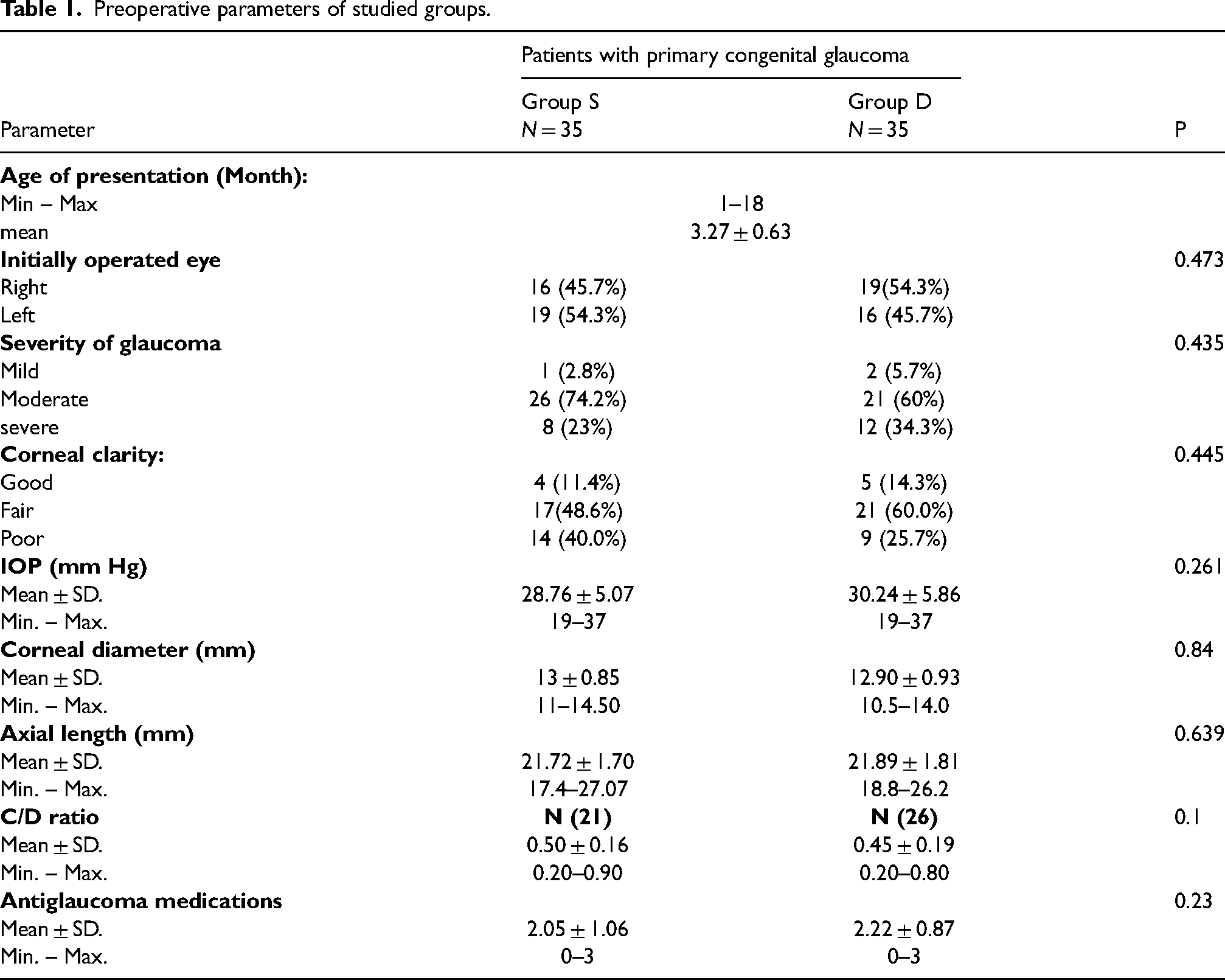
This study was a prospective, randomized interventional trial held at Mansoura Ophthalmic Center between June 2021 and June 2023. Among the 35 children (aged 3.27 ± 0.63 months at presentation to the center), 19 were males and 16 were females. The family history of PCG was negative in all cases. Consanguinity was positive in 8 children (22.8%). Most of the studied cases had moderate severity of the diseases with no significant difference between the two groups. (Table 1) listed preoperative ocular parameters in both groups that had no significant differences. All children completed the one-year follow- up visits.
Preoperative parameters of studied groups.
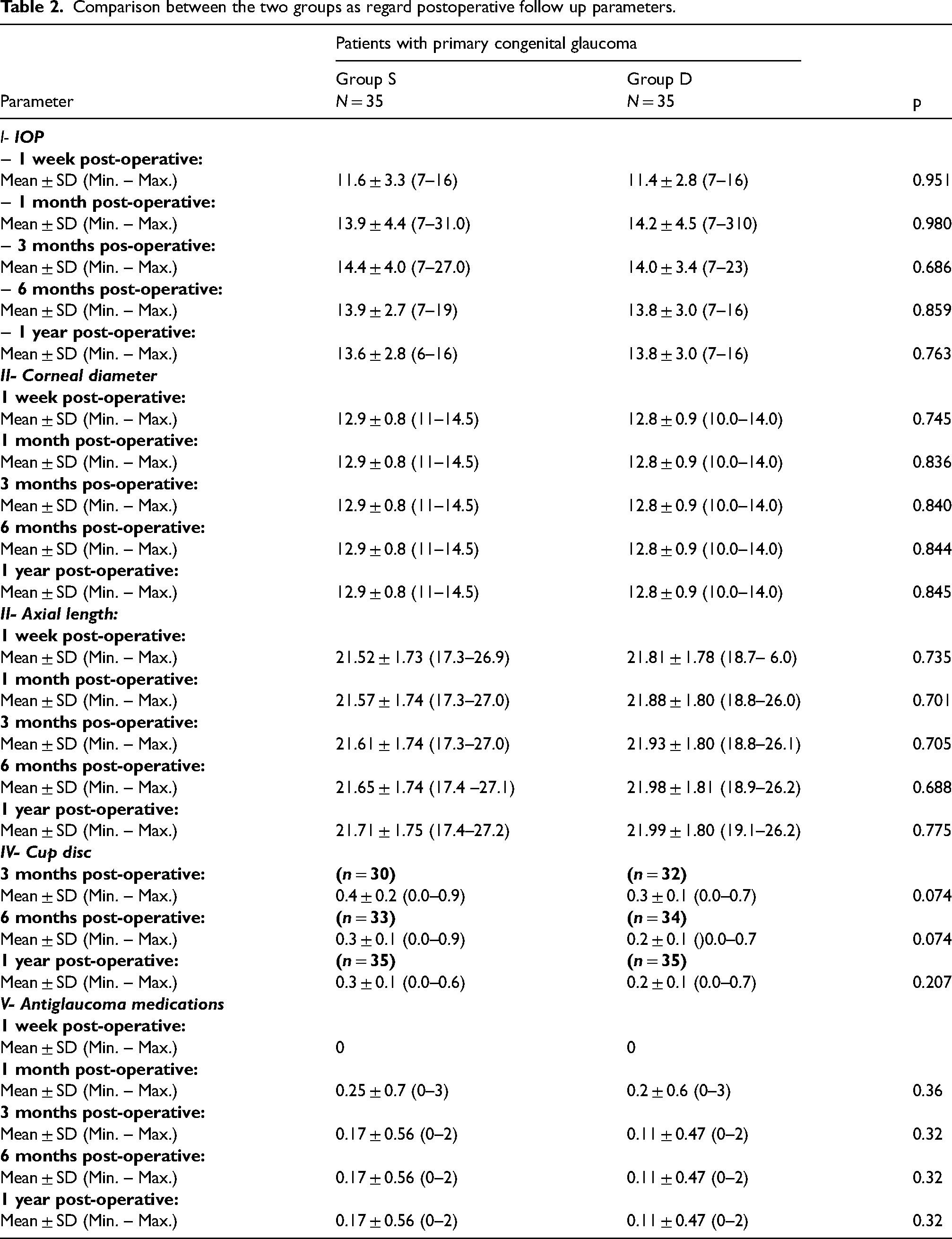
IOP significantly reduced at 1 week postoperatively compared to preoperative values in both groups and remained until one-year follow-up. Postoperative one- year follow-up values were (13.61 ± 2.80) mm Hg for group S and (13.82 ± 2.96) mm Hg for group D with no statistical difference between the two groups. The preoperative corneal diameter was (13 ± 0.85) and (12.90 ± 0.93) mm for groups S and D respectively. Postoperative one-year follow-up values were (12.88 ± 0.81) and (12.77 ± 0.93)mm and the difference was not statistically significant between groups S and D. In addition, axial length and cup disc ratio showed no statistically significant change between both groups during the follow- up period. (Table 2) (Figure 2)
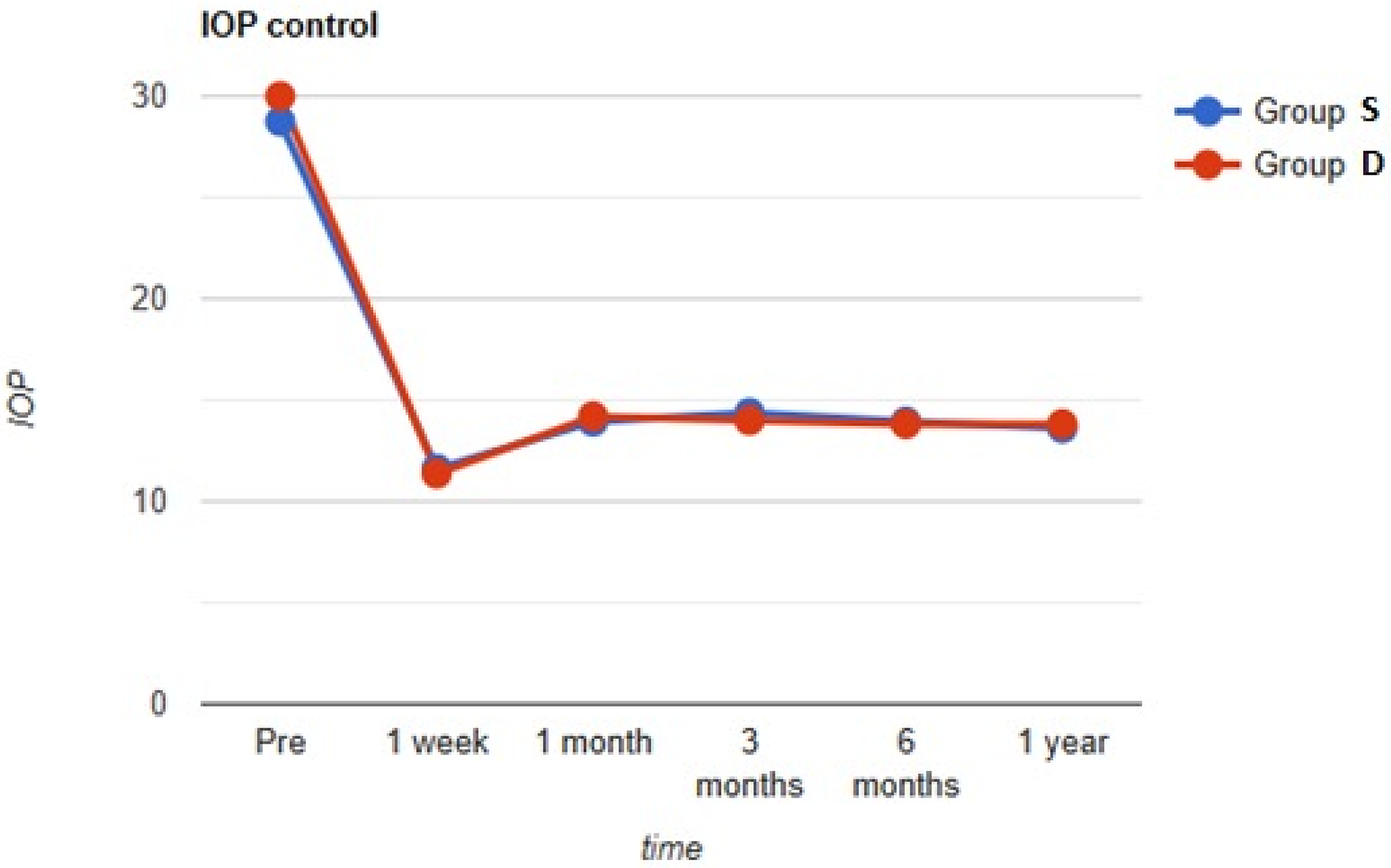
Line chart of IOP control in both groups during the follow up period.
Comparison between the two groups as regard postoperative follow up parameters.
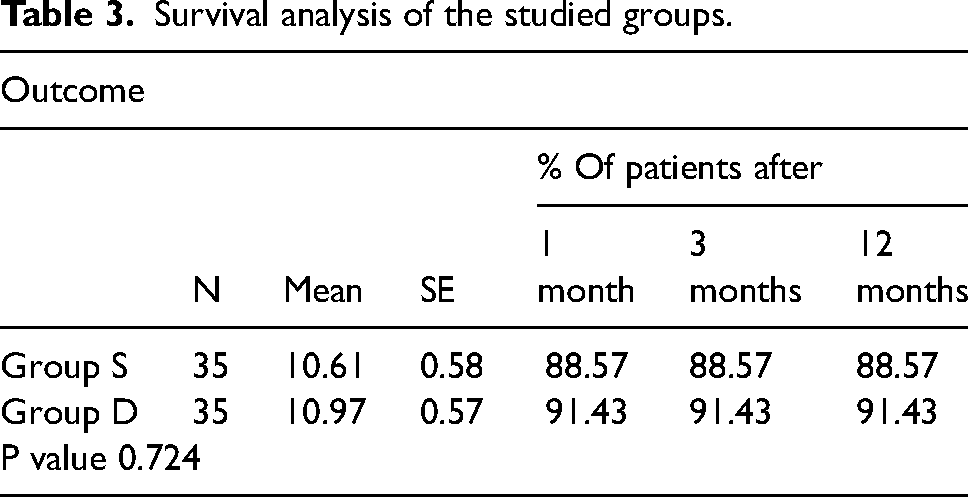
The complete success rate was 88.57% (31 eyes) for Group S and 91.43% (32 eyes) for Group D. Qualified success was 8.57% (3 eyes) for Group S and 5.71% (2 eyes) for Group D and the difference was not statistically significant (P value 0.9). Total success in both groups was 97.14%. One eye in each group (2.86%) showed a recurrence of glaucoma with the need for surgery. (Table 3) (Figure 3)
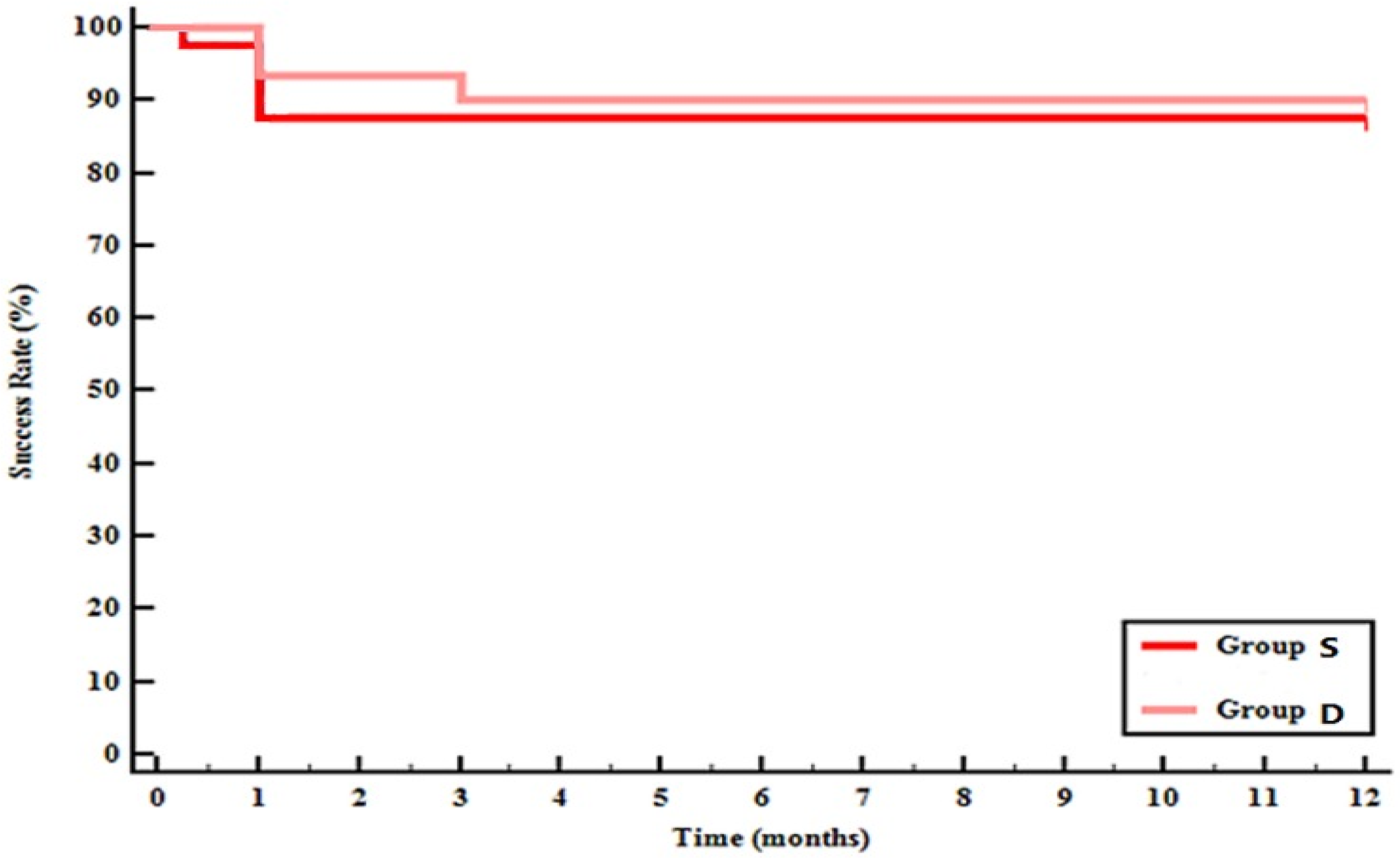
Kaplan Meier survival analysis of the different studied groups.
Survival analysis of the studied groups.
Preoperative anti-glaucoma medications were 2.05 ± 1.06 in group S and 2.22 ± 0.87 in-group D where up to three antiglaucoma medications were used. No anti-glaucoma medications were needed at the first- week follow- up. By the 1-month follow- up, anti-glaucoma use was 0.25 ± 0.7 in group S and 0.2 ± 0.6 in-group D. This decreased to 0.17 ± 0.56 in group S and 0.11 ± 0.47 in group D for the subsequent follow- up visits after surgically managing failed cases.
There were no major complications in any case, transient hyphema was noticed in most cases and resolved before the first follow- up visit in all cases. Shallow anterior chamber occurred in one eye (2.86%) of the single site viscotrabeculotomy group and resolved spontaneously within 2 weeks follow- up. Drawn pupil was noted in 2 cases (5.7%) of the single-site viscotrabeculotomy group and 1 case (2.86%) of the double- site viscotrabeculotomy group, but none of them was significant or required any surgical intervention.
In this study, recurrent glaucoma occurred in one eye in the single -site VT group and was managed by inferior viscotrabeculotomy. One eye in the double site VT group showed recurrence and was managed by trabeculectomy augmented with ologen matrix. Both showed IOP control after the second surgical intervention. Both eyes with recurrent PCG presented with elevation of IOP and corneal edema before the 1-month follow- up visit with the failure to control IOP with topical medications. The second surgical intervention was performed at 2 months after the primary surgery to exclude the possibility of early IOP spikes.
Discussion
The success rate was comparable in the single- site viscotrabeculotomy group and the double- site viscotrabeculotomy group with no statistically significant difference between the two groups in the current study. Paired eye design of bilaterally presented children was adopted in this study as a trial to limit the possible effects of genetics, consanguinity, and age at the onset of glaucoma on the success rate of both groups.
The procedural difficulty in performing the inferotemporal viscotrabeculotomy was that the globe becames softer after superonasal viscotrabecuolotomy. This may cause difficulty in creating the lower scleral flap, which can be avoided by sufficiently pressurizing the anterior chamber with Healon at the end of the superior VT as we did in the cases.
The authors appreciated the double -site viscotrabeculotomy as an economical effective substitute for illuminated microcatheters and a safer technique than suture trabeculotomy (risk of false passage). 12 In addition, it can be used in cases with opaque cornea where GAAT and other Ab interno techniques are difficult.
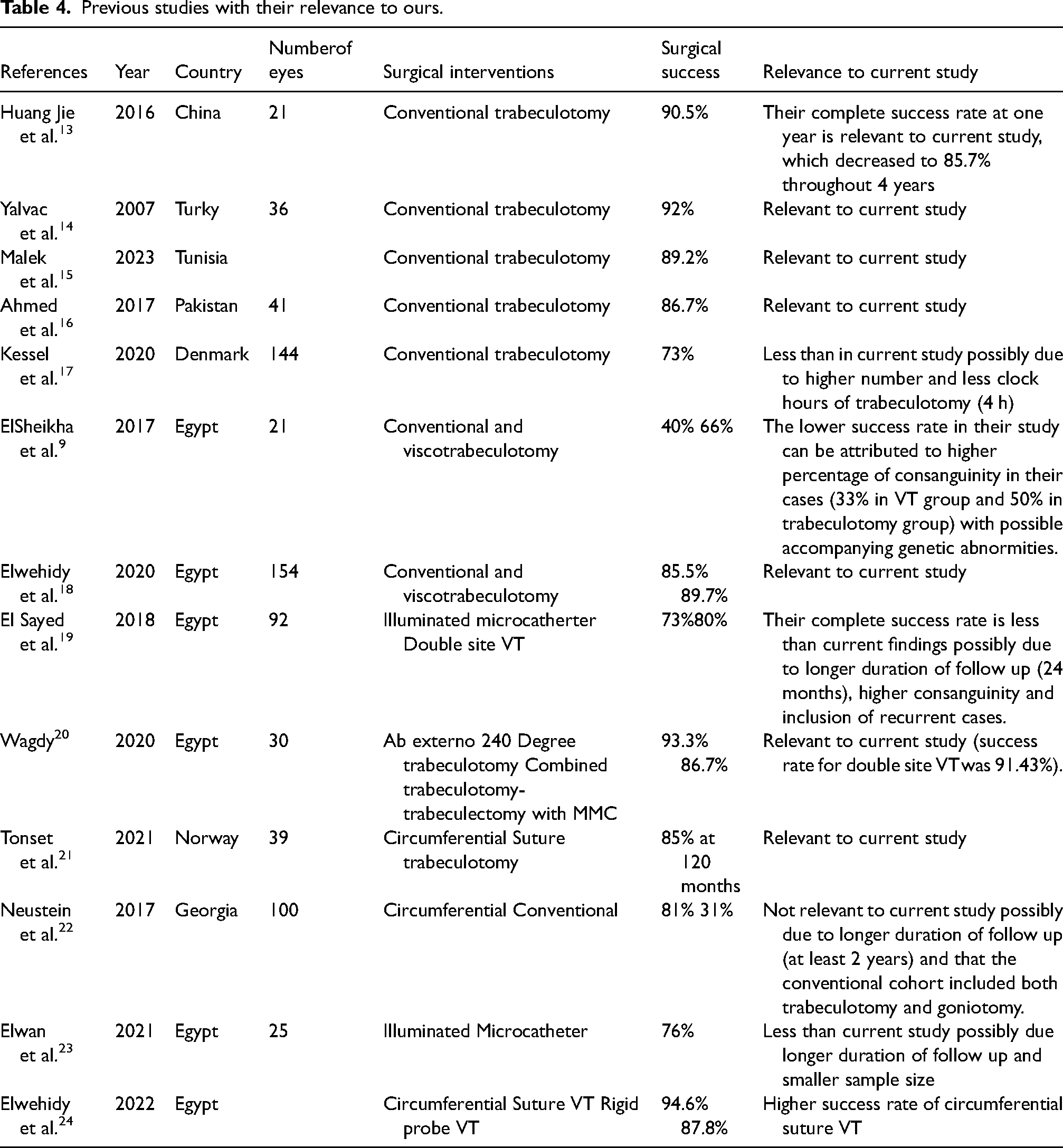
Many authors studied the outcomes of traditional trabeculotomy and its various modifications that are relevant to this study. For traditional trabeculotomy, Jie et al (2016) in China conducted a retrospective study of five-year duration on PCG children (21 eyes) and reported a one-year success rate of 90.5%. 13 Yalvac et al (2007) in Turkey reported the success rate of 92.0% in one year. 14 Malek et al (2023) reported a success rate of 89.2% in Tunisian children. 15 Ahmed et al (2017) from Pakistan reported success rate of 86.7%. 16 Kessel et al (2020) reported success rate of 73% which is less than current study that can be attributed to the less degree of trabeculotomy performed (4 clock hours only). 17
For viscotrabeculotomy, Tamcelik N & Ozkiris A (2008) compared viscotrabeculotomy (group 1)to traditional trabeculotomy (group 2) where the success rates for group 1 and group 2 were 91.3% and 68.6%, respectively(p = 0.02). 7 ElSheikha et al (2015) from Egypt reported a success rate of 66% in viscotrabeculotomy compared to 40% when trabeculotomy was performed without the use of viscoelastic material. The lower success rate in their study can be attributed to a higher percentage of consanguinity in their cases (33% in the VT group and 50% in trabeculotomy group). 8 Elwehidy et al (2020) also reported a five-year success rate to be 89.74% which is relevant to our findings. 18
Other authors studied the outcomes of double- site trabeculotomy, El Sayed et al (2018) compared the results of microcatheter- assisted transluminal trabeculotomy and double- site metal probe trabeculotomy and reported a success rate of 73% and 80% respectively 19 (P: 0.3) . Wagdy (2020) conducted a study on 30 PCG eyes to compare Ab externo 240-degree trabeculotomy (double metal trabeculotomy) and combined trabeculotomy with trabeculectomy with MMC. He reported that the complete success rate at one year was higher in double- site trabeculotomy group (93.3%) than in CTT augmented with MMC group (86.67%). He advocated Ab externo 240-degree trabeculotomy because of its higher success rate and fewer bleb and mitomycin related complications. 20
Other modifications of the extent of trabeculotomy included 360-degree trabeculotomy. Tonset et al (2021) conducted a retrospective study on PCG cases that received circumferential trabeculotomy using prolene sutures and reported a success rate of 85% over a median 120 month follow- up period. 21 Neustein et al (2017) conducted a retrospective study on PCG children and reported postoperative success at the last follow-up in the circumferential vs. conventional cohorts to be 81% (47 of 58 eyes) vs. 31% (13 of 42 eyes), respectively (P < 0.0001). The difference in success rate reported for the conventional cohort than the current study (31% versus 88.57%) may be because they included goniotomy cases in their conventional group. 22 Elwan et al (2021) conducted a study on 25 PCG eyes to which illuminated microcatheter 360-degree trabeculotomy was performed and reported a 2-year complete success rate of 76% that was raised to 80% if adding qualified cases. 23 Elwehidy et al (2022) reported success rate for viscocircumferential suture trabeculotomy and rigid probe viscotrabeculotomy at 36 months follow up to be 86.8% and 78% respectively (p = 0.278) 24
Further details of the previous studies are listed in Table 4. In the current study, the extent of trabeculotomy did not significantly affect the outcome or the IOP at the last follow- up. A debate exists on whether increasing the degree of trabeculotomy should necessarily increase favor outcome or cause a more profound reduction in IOP. This study suggests that single site viscotrabeculotomy can achieve good IOP control after which an increase in the extent of angle opening will not affect the outcome. This is relevant to other studies that included eyes with recurrent PCG where authors reported no significant change in outcome when the angle surgery exceeded 120 degrees.25,26
Previous studies with their relevance to ours.
Limitation of the study included a short duration of follow up, a relatively small number of enrolled eyes, and using the surgical microscope to assess corneal condition. One other limitation of the study is that the more severely affected eye in every child was operated on first so; randomization was not applied for the eye but for the surgical procedure.
Primary congenital glaucoma still represents a challenge for ophthalmic surgeons. In a search for higher success rates and better control, modalities were performed, were enhanced, and were edited throughout the years. 8
Conclusion
In the current study, single -site viscotrabeculotomy shows a comparable outcome to double -site viscotrabeculotomy (in terms of success rate and mean IOP) at one year with preservation of more than half of the angle in the former for a second possible angle surgery in recurrent cases.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.