
Abstract
Purpose
Cerebrospinal fluid venous fistulas (CVFs) are a frequently underrecognized cause of cerebrospinal fluid (CSF) leaks, leading to intracranial hypotension and a wide range of symptoms, including visual disturbances. This case highlights the critical role of ophthalmologists in identifying CVFs as a cause of unexplained progressive vision loss.
Methods
We present the case of a 45-year-old woman who developed progressive visual field loss over 15 years, ultimately resulting in blindness in one eye. Early neuroimaging and testing were normal despite symptoms of orthostatic headaches, photophobia, and hearing loss. Advanced imaging eventually identified a CVF at the T8 level. Surgical correction was performed, and the patient's clinical response was assessed.
Results
Surgical repair of the CVF led to clinical improvement, halting further progression of symptoms.
Conclusions
CVFs should be considered in patients with unexplained visual disturbances, particularly when accompanied by symptoms of intracranial hypotension. Early suspicion and collaboration with neurologists and neuroradiologists are essential for timely diagnosis and intervention. Ophthalmologists play a pivotal role in guiding appropriate referrals, ensuring multidisciplinary care to prevent irreversible visual and systemic complications.
Keywords
Introduction
Cerebrospinal fluid (CSF) leaks, particularly those caused by cerebrospinal venous fistulas (CVFs), represent a complex and often underrecognized diagnostic challenge across various medical specialties. CVFs are abnormal connections between the subarachnoid space and nearby veins, causing unregulated CSF drainage and leading to intracranial hypotension. Although orthostatic headaches are the hallmark symptom, CVFs can present with a wide array of clinical features, frequently mimicking more common neurological and ophthalmological conditions.1,2
In this report, we present the case of a patient whose initial presentation was marked by isolated visual symptoms, including progressive visual field loss and eventual blindness in one eye. Despite normal findings on early neuroimaging and extensive investigations, the patient's symptoms persisted for years. It was only through advanced imaging techniques and a targeted diagnostic approach that a CVF was identified as the underlying cause, underscoring the potential for delayed diagnosis and mismanagement in such cases.
The aim of this report is to highlight the importance of recognizing CVFs as a potential cause of unexplained, progressive neurological and ocular symptoms. This case demonstrates how a delayed or incorrect diagnosis can lead to significant clinical deterioration and emphasizes the need for an interdisciplinary approach. By raising awareness among different specialists—such as neurologists, ophthalmologists, and radiologists—our goal is to promote earlier recognition, accurate diagnosis, and timely treatment to prevent irreversible damage.
Case report
A 45-year-old healthy, non-smoking woman with a history of episodic iron deficiency anemia and a first-trimester spontaneous abortion presented with a sudden onset of disturbed vision in her right eye (RE), specifically affecting her temporal visual field, and photophobia.
Upon initial examination, her visual acuity was found to be 20/20 (Snellen), with a normal intraocular pressure (15 mmHg), as well as a normal anterior segment, optic disc, and macula. A visual field test revealed a temporal scotoma (Figure 1(a)), optical coherence tomography (OCT) confirmed a normal foveal thickness and profile, and the retinal nerve fiber layer (RNFL) and ganglion cell complex (GCC) appeared normal. Pattern visual evoked potentials (PVEV) showed normal latency and morphology in the left eye (LE), but altered amplitude in the RE. Fluorescein angiography was also normal.
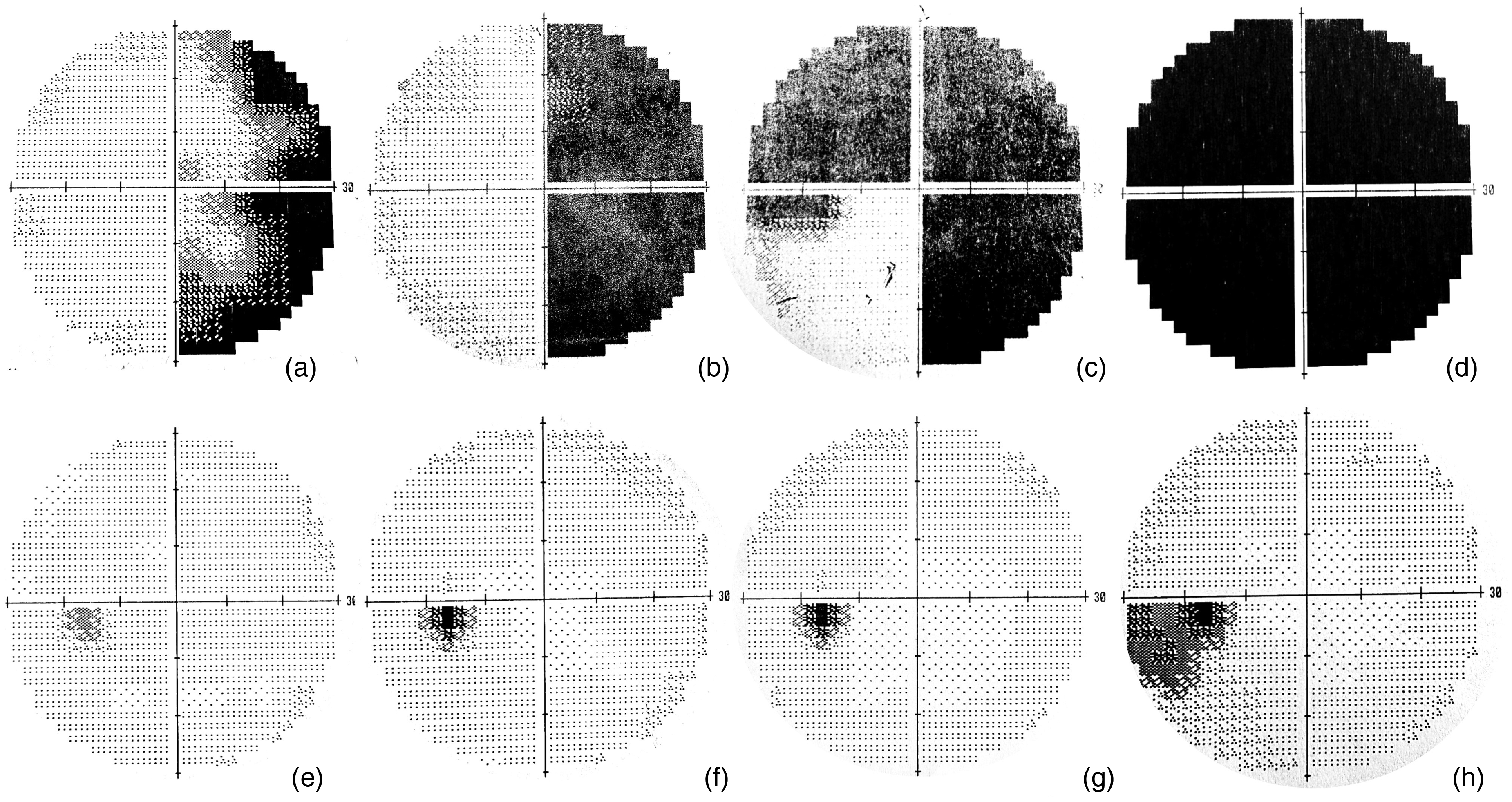
Longitudinal visual-field assessments of the right and left eyes. (a) Visual-field of the right eye at initial presentation, showing a sensitivity defect in the temporal hemifield extending between the central 10° and 30°; (b) Visual-field of the right eye at 1-month post-presentation, demonstrating temporal hemianopia; (c) Visual-field of the right eye at 3 months post-presentation, showing progression of hemianopia with involvement of the superior nasal quadrant; (d) Visual-field of the right eye at 5 months post-presentation, demonstrating complete vision loss; (e, f, g) Visual-field assessments of the left eye during follow-up visits over subsequent years, showing no significant changes; (h) Visual-field of the left eye 12 years after the initial presentation, revealing an inferotemporal quadrant defect between the central 10° and 30°.
A diagnosis of posterior ischemic optic neuritis was made, and she was treated with intravenous methylprednisolone (250 mg every 6 h for 3 days), followed by oral prednisone (1 mg/kg/day) tapered over a few weeks.
One month later, her visual field defect had progressively worsened (Figure 1(b)). Given the patient's lack of response to corticosteroids and the absence of systemic symptoms, an extensive diagnostic workup was conducted. Optic neuritis typically presents with rapid vision loss, reduced contrast sensitivity, color vision defects, visual field loss, retrobulbar pain (often severe and worsened by eye movements), and photopsias. In this case, however, only a visual field defect was present, and OCT revealed normal RNFL and GCC, excluding significant neuroaxonal injury. Routine blood tests, including a complete blood count, metabolic panel, ESR, and CRP, were normal, ruling out systemic inflammation and infectious causes. Immunological tests (ANA, ENA panel, rheumatoid factor, sarcoidosis markers, and antiphospholipid antibodies) and infectious screenings (syphilis, HIV, and tuberculosis) were negative, excluding autoimmune and infectious etiologies. MRI of the brain and orbits with contrast showed no demyelinating lesions, optic nerve abnormalities, or compressive pathologies, ruling out multiple sclerosis, neuromyelitis optica spectrum disorder, and compressive optic neuropathies. Metabolic, nutritional, and toxic causes were excluded based on normal laboratory results and the absence of systemic symptoms or relevant history. With negative findings across all tests and poor steroid responsiveness, a diagnosis of exclusion was reached. Despite the absence of definitive vascular risk factors, a non-vasculitic vascular optic neuropathy was considered as the most plausible explanation.3–5
Three months after her initial presentation, the patient had lost three-quarters of her visual field in the right eye (Figure 1(c)). CSF analysis revealed hypogammaglobulinemia and hyperproteinorrachia, but immunoelectrophoresis was negative.
By five months post-presentation, she had completely lost vision in her RE (Figure 1(d)). Another MRI was negative, and she was diagnosed with non-arteritic ischemic optic neuropathy.
Over the next twelve years, she underwent multiple surgeries under spinal anesthesia, including uterine polyp removal and knee lipoma excision. Regular neurological and ophthalmological examinations remained unremarkable.
Over the next twelve years, neurological and ophthalmological examinations remained unremarkable (Figure 1(e)–(g)), until further visual disturbances developed in the left eye (Figure 1(h)
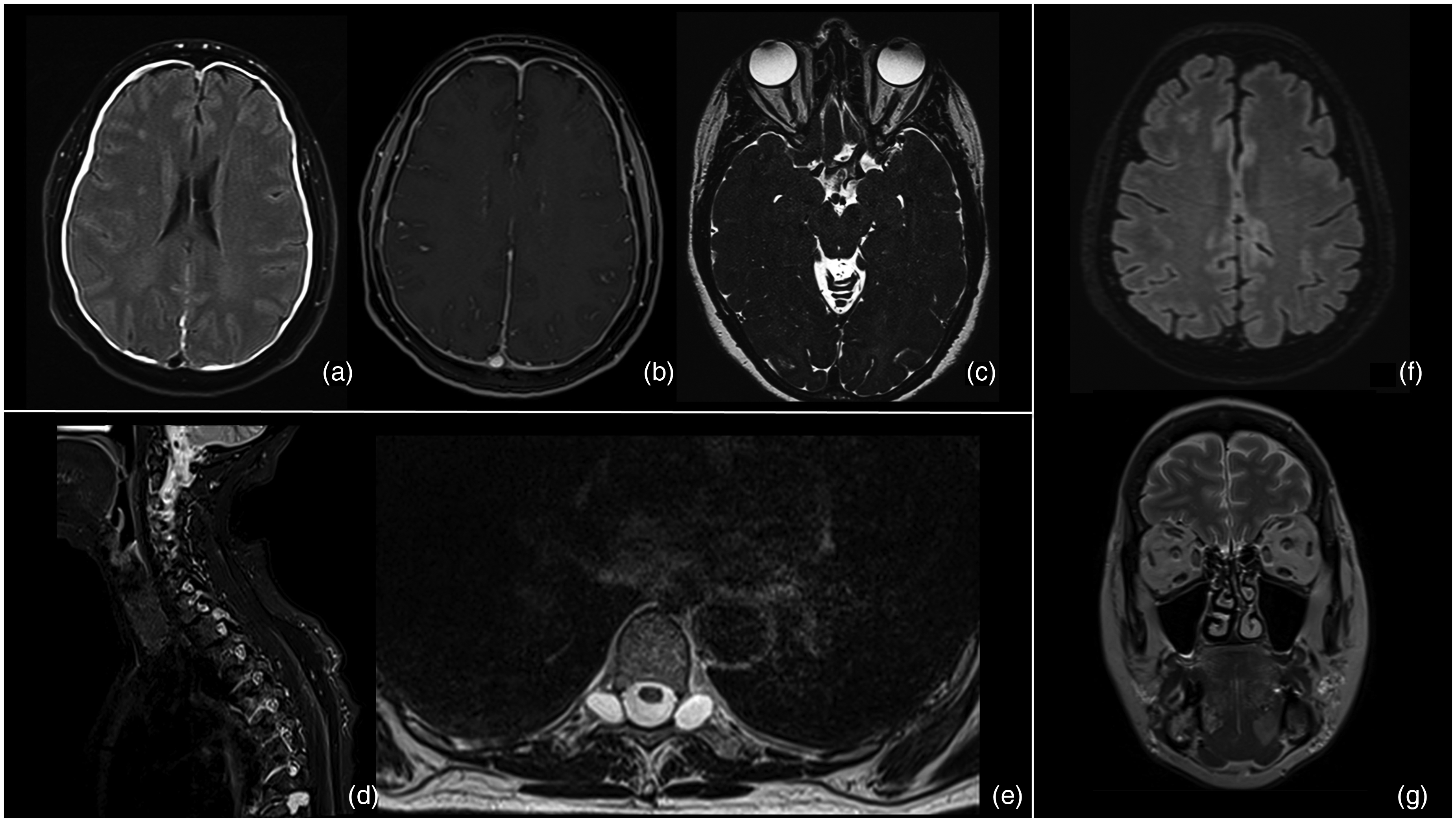
Neuroradiological imaging findings. (a, b) Axial T2-weighted FLAIR and T1-weighted VIBE sequences after gadolinium administration, respectively, demonstrating bilateral subdural hematoma and diffuse meningeal enhancement; (c) T2-weighted SPACE sequence showing collapsed optic nerve sheaths; (d, e) Axial T2-weighted FSE and sagittal T2-weighted STIR sequences depicting large perineural cysts at the T9-T10 level; (f) Post-operative axial T2-weighted FLAIR sequence showing resolution of the bilateral subdural hematoma; (g) Post-operative coronal T2-weighted TSE sequence demonstrating restored cerebrospinal fluid in the optic nerve sheaths.
In suspect of CSF hypotension syndrome conservative management was applied. 5-months follow-up MRI confirmed chronic subdural hematomas with diffuse meningeal enhancement and poor perineural CSF signal in the optic nerve sheath. No additional imaging was performed and suspecting CSF-leakage, she was empirically treated with an epidural blood patch using 20 ml of autologous blood at the L2-L3 level. This treatment led to the resolution of her orthostatic headaches.
Despite this, her symptoms recurred two months later. MRI showed persistent meningeal enhancement and reduced subdural hematoma thickness. She received a second blood patch, this time with 30 ml of autologous blood at the L1-L2 and L3-L4 levels. However, her orthostatic headaches, photophobia, and hearing loss persisted, as did the meningeal enhancement on MRI.
Fourteen years after the first onset of symptoms, the patient underwent a third blood patch with 20 ml of autologous blood, which resulted in symptom regression and partial improvement of meningeal enhancement.
Nine months later, her symptoms recurred again, with MRI findings similar to those initially observed.
Fifteen years after the onset of her symptoms, dynamic myelography revealed a CSF-venous fistula at T8, leading to another surgical intervention, leading to surgical dural repair and consequent clinical and neuroradiological resolution (Figure 2(f) and (g)). Post-operative recovery halted further visual deterioration.
Discussion
Cerebrospinal fluid venous fistulas (CVFs) are a challenging and often under-recognized cause of CSF leaks, resulting in significant volume depletion and complex clinical presentations that are frequently misdiagnosed. CVFs are abnormal connections between the spinal subarachnoid space and nearby veins, allowing CSF to leak into the venous system without regulation. The most widely recognized etiopathogenesis involves the rupture of arachnoid granulations, structures responsible for CSF reabsorption located within meningeal invaginations at the interface between the subarachnoid space and venous plexuses along radicular nerve root exits. Under normal conditions, the pressure gradient between the CSF and venous plexuses facilitates a gradual and controlled outflow. However, in presence of abnormal communication with one or more segments of the complex vertebral venous system—most commonly involving the epidural vertebral venous plexus or segmental veins—this controlled mechanism is disrupted, resulting in an uncontrolled escape of CSF. This leakage can lead to a decrease in CSF volume, resulting in intracranial hypotension. 6 Clinically, they are characterized by a variety of symptoms that mimic other neurological conditions, further complicating the diagnostic process. 6 Although CVFs have only been recently identified, they have quickly become recognized as a common cause of spinal CSF leaks in cases of SIH, particularly in patients where no visible leak is detected on initial spinal imaging. 6
In the case we presented, the patient initially exhibited progressively worsening ocular symptoms, including a visual field defect that eventually led to vision loss in the right eye, accompanied by photophobia. Following the exclusion of ocular causes, a comprehensive evaluation was undertaken to investigate potential etiologies of optic neuropathy, encompassing ischemic, inflammatory, and neurodegenerative conditions. However, the patient's clinical profile and imaging findings indicated that these diagnoses were improbable.
The relationship between ocular alterations, optic neuropathy, and intracranial hypotension, particularly the imbalance between intraocular pressure (IOP) and the pressure in the subarachnoid space (SAS) of the optic nerve, has been the focus of extensive research in recent years.7,8
According to Zada et al., ocular symptoms associated with intracranial hypotension encompass a range of visual disturbances, including blurred vision, double vision, and visual field deficits. These symptoms are occasionally accompanied by photophobia, visual acuity deficits, nystagmus, and ophthalmoplegia. According to the authors, the underlying mechanisms for these visual disturbances may involve the stretching of the optic complex over the pituitary fossa or vascular congestion affecting the optic nerves and tracts.2,9
Although orthostatic headache is the most commonly associated symptom of intracranial hypotension, an interesting meta-analysis published by D'Antona et al. in 2021 highlighted the variability in clinical presentation. The study found that headache was present in 97% of patients, with the majority(92%) being orthostatic. Notably, 3% of patients did not report any headache, which is a critical finding for managing complex cases. 1 Furthermore, the authors analyzed the pooled estimates of ocular symptoms, dividing them into photophobia, diplopia, and other visual symptoms, including visual loss. The proportions were 11% (95% CI, 5%–16%) for photophobia, 6% (95% CI, 3%–10%) for diplopia, and 14% (95% CI, 7%–21%) for other visual symptoms. These findings emphasize the need to consider ocular symptoms in diagnosing intracranial hypotension, even in the absence of a headache. 1
An important confounding factor in our case was the initial neuroimaging, including MRI, which failed to reveal any abnormalities, thereby hindering the identification of the underlying issue. This absence of radiological findings is a well-documented challenge in cases of CSF hypotension, often leading to delayed diagnosis and intervention.6,10 Intracranial hypotension typically presents with characteristic signs on MRI, such as brain sagging, which may present as acquired cerebellar tonsillar ectopia, reduced mamillopontine distance, effacement of the basal cisterns, slumping of the pons against the clivus, and downward displacement of the splenium of the corpus callosum. Additional common signs include pachymeningeal enhancement, subdural collections, venous engorgement, and pituitary gland enlargement. 1 However, D’Antona et al. showed that in 19% of cases brain MRI results are normal, further complicating the diagnostic process and prolonging the duration of symptoms before appropriate treatment is initiated. 1
Additionally, the diagnosis of CVFs presents further challenges. Unlike dural tears, which were the first described cause of intracranial hypotension and often result in the pooling of CSF in the epidural space, most CVFs do not cause such fluid accumulation. 6 The absence of epidural fluid makes conventional anatomical imaging techniques, not effective in identifying CVFs.
Therefore, in patients with clinical suspicion of SIH and nonspecific visual disturbances or visual field defects not attributable to other ocular or neurological pathologies, a preliminary MRI of the brain and spine is recommended to search for typical signs of intracranial hypotension previously mentioned. However, if typical SIH signs are not identified on MRI despite highly suggestive clinical findings, advanced dynamic imaging techniques such as myelography-CT (myelo-CT) or digital subtraction angiography (DSA) myelography should be considered. These techniques involve the injection of contrast medium into the dural sac, followed by CT or DSA imaging, to accurately visualize potential fistula sites. 6
In our patient, large bilateral perineural cysts were identified as a significant risk factor, associated with thinning and dilation of the dural sheath, making it prone to spontaneous rupture. These ruptures can lead to CSF leaks, which may occasionally be temporary and self-resolving. 11 It is possible that an initial CVF spontaneously resolved, temporarily relieving symptoms but causing irreversible damage, as indicated by complete vision-loss in the RE. Interestingly, our patient showed hyperproteinorachia, which, although nonspecific, can occur in cases of SIH. 12 Elevated CSF protein levels in SIH may result from abnormal communication between the subarachnoid space and the venous system, allowing blood proteins to enter the CSF due to the substantial concentration gradient. Blood protein levels are 100–200 times higher than those in CSF, which may explain this observation. 13
Although rare, similar cases have been reported, highlighting the importance of considering CVFs in patients with unexplained visual symptoms, which may persist for months, and SIH, even when initial diagnostics are inconclusive.10,12,14
The consequences of such misdiagnoses are profound, as illustrated by this case, where the patient suffered irreversible vision loss. Beyond the physical implications, the emotional toll on patients enduring a prolonged and often frustrating search for a diagnosis is significant, involving consultations with multiple specialists and numerous inconclusive tests.
This case highlights the critical importance of a multidisciplinary approach, integrating the expertise of ophthalmologists, neurologists, and neuroradiologists in diagnosing and managing complex cases of CSF leaks. Expanding the differential diagnosis to include neurological causes, such as CSF, is essential for ophthalmologists managing unexplained, progressive visual loss. While ocular conditions are often prioritized, this case highlights the need to consider systemic and neurological etiologies that can mimic primary eye disorders. A broader diagnostic approach allows for the timely identification of serious conditions, such as CSF venous fistulas, and supports prompt referrals to neurology or radiology. Furthermore, this case underscores the value of advanced neuroimaging techniques, such as dynamic myelography, in identifying elusive CSF leaks and guiding effective treatment. Early recognition and intervention are crucial in preventing irreversible damage and improving patient outcomes in cases of CSF venous fistula.
Footnotes
Consent
Informed consent was obtained from the patient for publication of this case report and accompanying images.
Data availability statement
The data supporting the findings of this case report are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.