
Abstract
Purpose
To report the short-term results of direct selective-laser trabeculoplasty (DSLT) in clinical practice.
Methods
Retrospective review of patients treated with DSLT between December 2023 and May 2024 with ≥ 6 months follow-up. Eyes were divided according to the indication for DSLT: first-line treatment (group 1); treatment-burden reduction (group 2) and additional intraocular pressure (IOP) lowering effect (group 3). Success was defined as a decrease of ≥ 20% from baseline-IOP with no additional treatment, or as a reduction in hypotensive drugs with stable IOP.
Results
Seventy-six eyes from 44 patients were included. In group 1 (20 eyes) mean IOP dropped from 26.50 ± 2.70 mmHg at baseline to 20.35 ± 3.37 mmHg six months after DSLT (p < 0.001). No eye required topical treatment. In group 2 (28 eyes), mean baseline IOP was 15.36 ± 4.34 mmHg and remained stable at 14.75 ± 4.15 mmHg (p = 0.214). Mean number of hypotensive drugs dropped from 2.00 ± 0.72 to 1.07 ± 1.24 (p < 0.001). In group 3 (28 eyes), mean IOP dropped from 20.21 ± 5.42 mmHg to 16.54 ± 4.37 mmHg (p < 0.001), with mean number of drugs remaining stable: 1.71 ± 0.76 at baseline and 1.57 ± 0.88 six months after DSLT (p > 0.05). There were no serious adverse events. Success rates were 55% in group 1, 57.1% in group 2 and 39.3% in group 3.
Conclusions
DSLT produced an IOP reduction of almost 25% in naive eyes and 17% in already-treated eyes. It can also reduce treatment burden with a stable IOP. These results support DSLT as an option at all stages of glaucoma, although the duration of its effect remains to be proven.
Keywords
Introduction
The Laser in Glaucoma and Ocular Hypertension (LiGHT) Trial 1 reported that selective laser trabeculoplasty (SLT) provided a better disease control compared to medical treatment, with a better cost-effectiveness, and led to the inclusion of SLT as a first line option in the main treatment guidelines for glaucoma.2–4 However the use of SLT in clinical practice, especially in Europe, is lower than expected. We believe this may be because correct SLT must be performed by a trained ophthalmologist using a goniolens and is relatively time consuming and difficult to fit in busy practices.
Direct selective laser trabeculoplasty (DSLT) was developed to avoid the use of a goniolens and to reduce the time for treatment application. The External Automatic Glaucoma Laser system, Belkin Eagle (BELKIN Laser Ltd., Yavne, Israel), directs the laser energy, almost completely automatically, through the limbus to the trabecular meshwork in a treatment that lasts approximately 2 s. A multicentre, randomised study is on-going to test the hypothesis that DSLT is effective and not inferior to SLT in reducing intraocular pressure (IOP) in open angle glaucoma. 5 However, the results have not yet been published and scarce information is currently available on DSLT, with only one report on results in clinical practice. 6 The aim of this study is to report the short term results of the application of DSLT in clinical practice in a wide spectrum of patients.
Methods
This study adhered to the tenets of the Declaration of Helsinki and was approved by our Ethics Committee, which waived the requirement for individual informed consent.
All patients undergoing DSLT in our center from the time the Eagle Device became available in December 2023 until July 2024 were identified from the device´s memory and evaluated for inclusion in the study. Their clinical records were reviewed in order to include treated eyes in one of the three study groups depending on their attending physician´s indication for DSLT. Eyes which had not received any previous treatment were included in group 1 (naive eyes); eyes in which the main purpose for DSLT was to decrease treatment burden were included in group 2 and eyes already treated with hypotensive drugs in which an additional IOP-lowering effect was desired were included in group 3. Eyes in groups 2 and 3 did not undergo a medication wash-out period before receiving DSLT. All eyes with at least six months follow-up were included in the study.
In SLT, the percentage of IOP reduction in the first treated eye has been shown to be predictive of response in the fellow eye. 7 Therefore, including both eyes after DSLT might lead to bias, since this similar response may also be expected. However, since the aim of this study was not to define exact IOP reduction but to provide clinicians with early feed-back on clinical results, the decision was taken to analyse both eyes.
DSLT treatment was performed with the Belkin Eagle by a glaucoma specialist. An α-adrenergic drop was applied 45 min before the procedure, followed by anesthetic drops 10 and 5 min before laser application. IOP was checked once approximately one hour after treatment, in order to detect IOP spikes. Non-steroidal anti-inflammatory drops (NSAID) were prescribed thrice daily for a week.
DSLT treatment consists of the application of 120 laser pulses of preset 3 ns and a preset 400 μm spot size, with an energy of 1.8 mJ delivered to the limbus through a full 360 degrees. The laser is applied almost completely automatically by the Eagle system, with only the operator's rough alignment of the eye and approval of the device's automatically acquired target. The actual laser application lasts for about 2 s. Laser power was not modified according to trabecular meshwork pigmentation.
In eyes with previous bleb-dependent glaucoma surgery, the area of the limbus adjacent to the bleb was unselected prior to treatment so that no laser was applied in this region; in eyes with previous I-Stent implantation the quadrant were the stents were implanted (usually the inferior nasal) was also unselected.
Data collected from the medical records included age, gender, treated eye, diagnosis, grade of glaucoma according to the Hodapp classification, previous ocular surgeries, as well as IOP and number of hypotensive drugs employed prior to DSLT treatment. After DSLT, patients are seen approximately one week and one, three and six months after treatment. Intraocular pressure and number of hypotensive drugs employed at each of these visits, as well as the presence of any side-effects were also collected.
Change from baseline IOP and number of hypotensive drugs was evaluated for each group. Success was defined as a decrease of at least 20% in IOP from baseline with no additional treatment, or else as a reduction in the number of hypotensive drugs with a maintained IOP, six months after treatment. The Wilcoxon test was used to evaluate differences in IOP and number of drugs between baseline and each visit for each group.
Results
Seventy six eyes from 44 patients (19 men, 25 women) received DSLT during the study period and had a follow-up of at least six months. Their ages ranged from 48 to 91 years, with a mean of 71.68 years and a standard deviation of 10.33 years. Twenty eyes were included in group 1, 28 eyes in group 2 and 28 eyes in group 3. Diagnosis, previous glaucoma surgery, lens status and Hodapp classification and visual field parameters are included in Table 1.
Baseline characteristics of eyes receiving direct selective-laser trabeculoplasty.
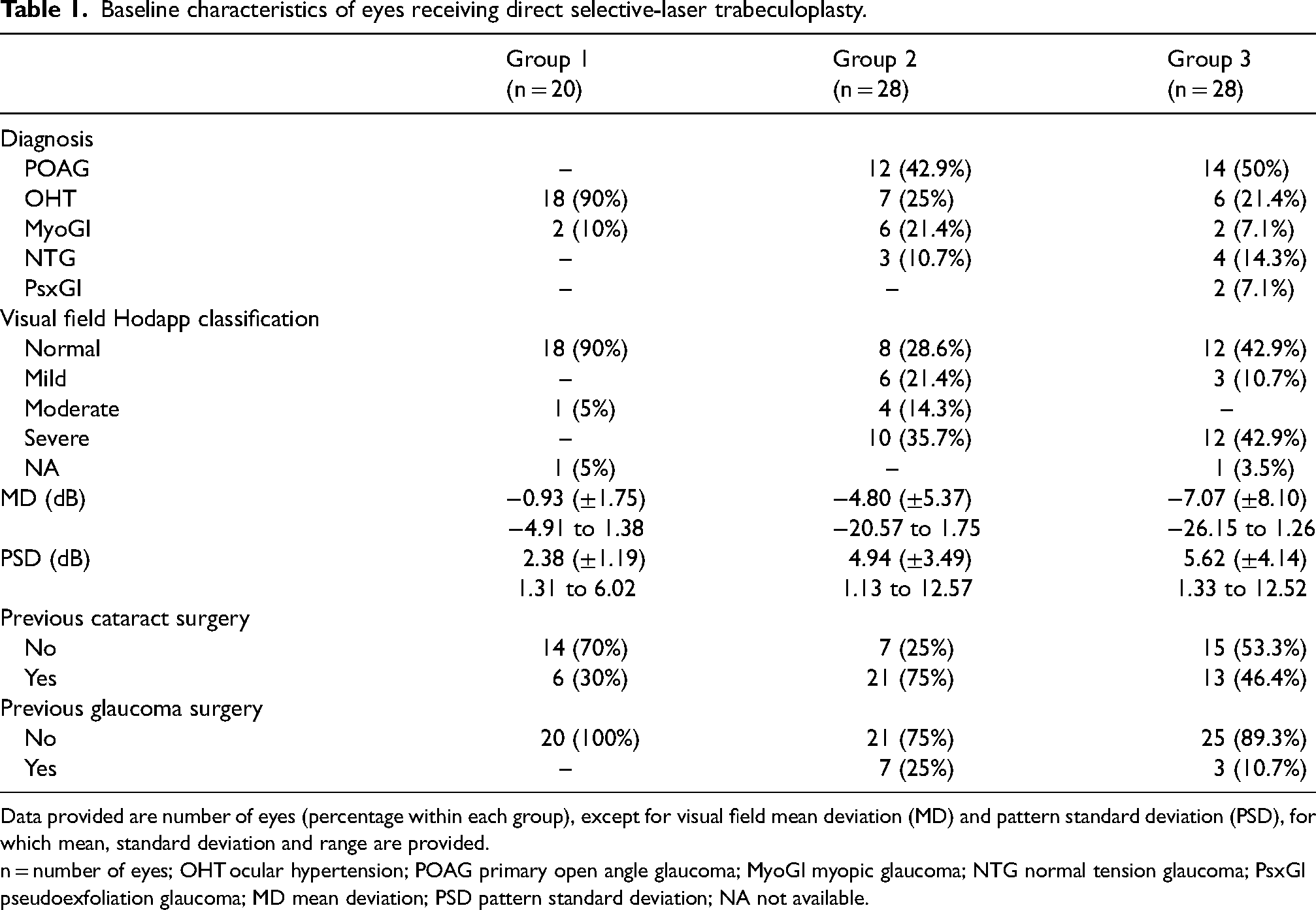
Data provided are number of eyes (percentage within each group), except for visual field mean deviation (MD) and pattern standard deviation (PSD), for which mean, standard deviation and range are provided.
n = number of eyes; OHT ocular hypertension; POAG primary open angle glaucoma; MyoGl myopic glaucoma; NTG normal tension glaucoma; PsxGl pseudoexfoliation glaucoma; MD mean deviation; PSD pattern standard deviation; NA not available.
Mean IOP and number of hypotensive drugs at baseline and for each time-point are recorded in Table 2. For groups 1 and 3, IOP was significantly decreased from baseline at all time-points, p ≤ 0.001 for all comparisons. In group 2, IOP was significantly reduced from baseline one week (p = 0.021) and three months (p = 0.015) after treatment, but not at the one month (p = 0.321) and six month visits (p = 0.214). As regards the number of IOP drugs, in group 2 the difference compared to baseline was statistically significant at all time-points (p < 0.002 for all comparisons); for group 3, there was a statistically significant decrease only one month after the procedure (p = 0.021), but not at other time-points (p > 0.05).
Intraocular pressure (IOP) values and number of hypotensive drugs used before (baseline) and after direct selective-laser trabeculoplasty.
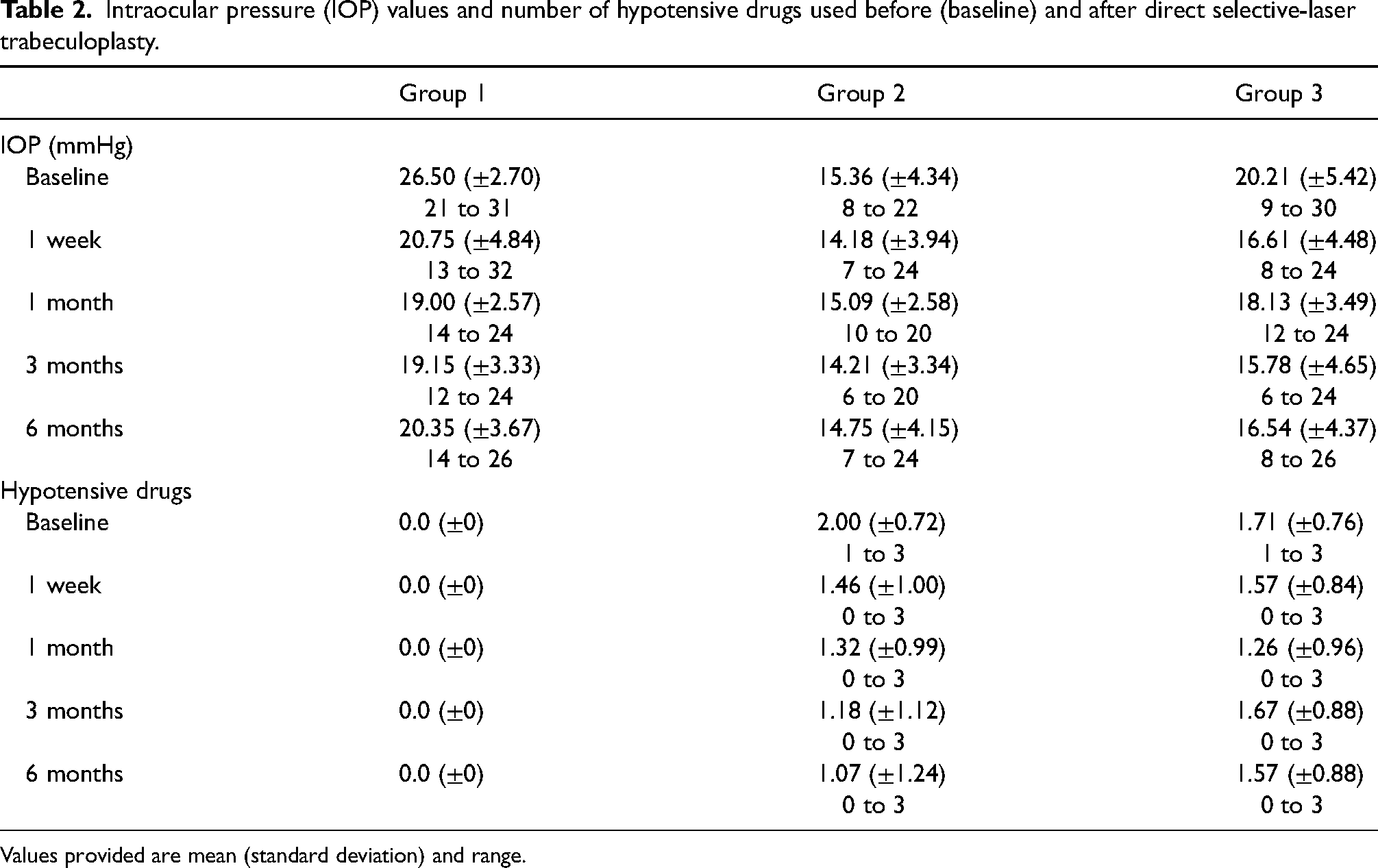
Values provided are mean (standard deviation) and range.
Six months after DSLT, mean IOP reduction from baseline was 23.43% for group 1, 1.64% for group 2 and 16.76% for group 3. In group 1, success rate was 55%, with 11 eyes achieving a reduction in IOP of more than 20%. In 7 naïve eyes the IOP reduction ranged between 11% and 19% and in another eye IOP reduction six months after DSLT was only 8%. However, no hypotensive drug was prescribed in any case up until the six-month visit. For group 2, success rate was 57.1%, since hypotensive drug medication could be reduced in 16 eyes maintaining target IOP. In 7 eyes, there was no change in hypotensive drugs, with IOP change ranging between ±10% from baseline. In three eyes, reduction of hypotensive drugs after the three month visit led to an increase of more than 10% in IOP at the six month visit. In both eyes of one patient, a new hypotensive drug was introduced three months after DSLT leading to a decrease in IOP of approximately 40% six months after treatment. In group 3, success rate was 39.3%, with 6 eyes achieving a reduction of at least 20% from baseline IOP without adding hypotensive drugs. In 5 eyes, IOP was maintained reducing the number of hypotensive drugs. In 3 eyes, adding a new hypotensive drug lead to a decrease of approximately 20% from baseline IOP. In 9 eyes, DSLT achieved an IOP reduction of between 10 and 20% without adding further medication. In four eyes, hypotensive drugs were reduced at the three month visit, leading to an increase of more than 10% in IOP at the six month visit.
As regards adverse effects, no IOP spikes were detected. One patient had bilateral punctate keratitis after treatment which resolved with increased application of artificial tears. This patient had already been diagnosed with dry eye disease. One patient reported ocular pain during treatment application and her dry eye disease also worsened the first month after treatment. Another patient reported photophobia during the first week after treatment, which resolved after one month.
Discussion
The LiGHT trial reported that SLT is a safe and effective technique as a first-line treatment for open angle glaucoma and ocular hypertension. In the trial, SLT provided superior IOP stability to hypotensive drops, at a lower cost and with almost three quarters of patients (74%) successfully controlled with no additional treatment for at least 3 years after laser application. 1 However, in spite of being included as a first-line option in the main treatment guidelines for glaucoma2–4 and of extensive evidence of its effect, 8 SLT is still not widely used in clinical practice. The reasons are difficult to determine, but some of the factors that may influence this are: an inertia (specially in general ophthalmologists) towards treatment with hypotensive drops, the time it takes to explain the laser procedure to patients, the time necessary to apply it and the cost for patients in private practice settings.
The Belkin Eagle is the first commercially available DSLT laser; it has received FDA (Food and Drug Administration) approval and the CE (European Conformity) mark. It has a highly automated treatment algorithm, therefore making laser application more standardized and less user-dependent and the procedure is very quick, since the actual laser treatment lasts approximately 2 s per eye. Together with the translimbal, contactless approach, these characteristics may help surmount the problems that may contribute to the limited application of SLT in clinical practice.
There is little published evidence on the results of DSLT. A dose-response study reported a decrease from baseline IOP of 22.1% and 22% three and six months after treatment in 13 eyes receiving DSLT with an energy of at least 1 mJ, with a mean reduction of 6mmHg after six months. 9 Recently, a short case series of 15 eyes treated with the Belkin Eagle reported a mean IOP reduction from 22.7 ± 4.4mmHg at baseline to 18.7 ± 4.2 mmHg four months after DSLT (p = 0.008). This series included both naïve and already treated eyes. Considering only the 8 eyes that maintained the same number of drugs at baseline and at 4 months, mean IOP reduction from baseline was 25.7%. 6
In our study, we decided to divide treated eyes in three groups, since treatment aims and expected results would be different for each group. In naïve eyes, we found a reduction from baseline IOP of almost 30% and 25% three and six months after DSLT, respectively. This is similar to the 30.5% reduction described in the LiGHT trial for eyes with a baseline IOP of between 25 and 30 mmHg two months after treatment. 10 However, the success rate in group 1 in our study six months after DSLT was 55%, lower than the 78.2% of SLT-treated eyes at target IOP without additional medications at 36 months in the LiGHT trial. 1
In our study`s group 2, DSLT was applied mainly to reduce treatment burden. There was a small reduction from baseline IOP, of approximately 5% and 2% three and six months after DSLT, respectively, with a statistically significant reduction in the mean number of hypotensive drugs, from 2.00 ± 0.72 at baseline to 1.07 ± 1.24 six months after treatment. Lee et al 11 and De Keyser et al 12 examined SLT as a replacement therapy in patients already receiving hypotensive drugs with well-controlled IOP. Both found that SLT decreased the number of drugs required for IOP control (mean change in medications was a decrease from 1.50 to 0.29 for De Keyser et al and from 2.3 to 1.5 for Lee et al). Thus, our results suggest that DSLT may have a similar effect as SLT in reducing treatment burden.
In group 3, DSLT was applied in already treated eyes with a baseline IOP of 20.21 ± 5.42 mmHg in search of an additional IOP lowering-effect. A reduction of 22% and 17% was achieved three and six months after treatment, with a success rate of 39.3%. In already treated patients, with a lower baseline IOP, a smaller effect for all interventions is to be expected. In fact, the reduction we found is slightly better than the 19% reduction after two months reported in the LiGHT trial for naïve eyes with an initial IOP of between 15 and 20 mmHg. 10
As regards adverse effects, no safety issues were identified. Three patients experienced symptoms that might be due to damage to the ocular surface; this has also been reported after SLT 13 and is probably produced by anterior chamber inflammation induced by the laser on the trabecular meshwork, as well as by the mechanical effect of the lid speculum during application. In SLT, topical NSAIDs have been reported to reduce patient-reported pain and anterior chamber inflammation with a positive effect on IOP reduction 14 and therefore we prescribed them after DLST. No signs or symptoms suggesting damage to the limbus were detected.
In summary, our results support that in naïve eyes, DSLT leads to an hypotensive effect that may be similar to that obtained by SLT. Additionally, in patients who do not tolerate medical therapy or do not comply with it, DSLT may be used to reduce treatment burden while maintaining target IOP. DSLT can also lower IOP in eyes already treated with several hypotensive drugs, as a step before surgery in patients who do not reach target IOP with maximum medical treatment. Thus, DSLT might be an option in every stage of disease progression.
These results must be interpreted with caution since this is a small short- term, retrospective study. We included both eyes of patients who received bilateral treatment and this may lead to bias if DSLT behaves like SLT, with a similar response to treatment in both eyes of a patient. Our study did not specifically evaluate trabecular meshwork pigmentation in order to determine if this influences the effect, as has been described for SLT. 15 Larger studies with longer follow-up periods will be necessary to confirm the duration of the IOP lowering effect, as well as whether repeat treatments may be performed. There is still much to be determined about the efficacy and safety of DSLT.
Footnotes
Consent to participate
The requirement for informed consent to participate has been waived by the relevant Ethics Committee.
Consent for publication
Not applicable.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical considerations
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of Hospital Clínico San Carlos (Reference 24/713-E) on October, 2024, with the need for written informed consent waived.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.