
Abstract
Objective
To evaluate the safety and efficacy of MicroPulse Transscleral Laser Therapy (MicroPulse TLT) with the Revised P3® Delivery Device.
Design
Prospective, single-surgeon, interventional study in a tertiary hospital setting.
Participants
Sixty-two eyes of 40 patients with refractory glaucoma.
Methods
All subjects received 360-degree MicroPulse TLT treatment (2500 mW, 31.33% duty cycle) over a total of 240 s (8 sweeps; n = 20), 300 s (10 sweeps; n = 22), or 200 s (10 sweeps; n = 20). Participants were followed up for 6 months to assess changes in intraocular pressure (IOP), glaucoma medication burden, and best-corrected visual acuity (BCVA). Surgical success was defined as a reduction of IOP ≥ 30% from baseline and between 6–18 mmHg at last follow-up with no additional anti-glaucoma medications or secondary reinterventions.
Results
Surgical success was achieved in 72.7% (300 s group), 75.0% (240 s group), and 80.0% (200 s group) of eyes. Mean IOP was significantly reduced (p < 0.001) by 49.0% (300 s group), 45.66% (240 s group), and 39.8% (200 s group) at 6 months. With all groups combined, the mean number of glaucoma medications was significantly reduced by 17.8% (p = 0.005), and no significant changes in BCVA were observed at 6 months. Complications were minimal, including four eyes with IOP spikes, one eye with hyphema, and one eye with cystoid macular edema (CME), all of which resolved. Two eyes of the total sample (3.2%) required secondary glaucoma surgery before 6 months.
Conclusions
Second-generation MicroPulse TLT at fluence values of 154–229 J/cm2 appears to be a safe and effective option for IOP reduction in refractory glaucoma.
Keywords
Introduction
Glaucoma is the leading cause of irreversible blindness worldwide, affecting 80 million individuals, with this statistic expected to increase to 111 million by the year 2040. 1 It is primarily managed through a stepwise treatment approach, using anti-glaucoma eyedrops as the first line treatment. However, when pharmacotherapy fails to decrease intraocular pressure (IOP) sufficiently, laser therapy or surgical intervention is indicated. 2 Trabeculectomy has historically been considered the “gold-standard” procedure but is limited by bleb-related complications such as blebitis, corneal erosion, conjunctival hemorrhage, and high reoperation rates3–5; therefore, there has been a push towards performing more minimally invasive surgeries to lower the IOP. In addition to subconjunctival bleb-forming procedures, current glaucoma treatment modalities consist of interventions directed at the trabecular meshwork or Schlemm's canal, suprachoroidal shunting procedures, or approaches aimed at diminishing aqueous production. 6
MicroPulse Transscleral Laser Therapy (MicroPulse TLT) is a tissue-sparing procedure which targets the ciliary body using repetitive pulses of infrared diode Cyclo G6® Laser (Iridex Corporation, Mountain View, CA, USA), with a wavelength of 810 nm to treat glaucoma by decreasing the production of aqueous humor. 7 The first-generation 700-micra fiberoptic handheld device was used for the treatment of refractory glaucoma and was shown to have a favorable safety profile to conventional transscleral cyclophotocoagulation (TSCPC). 7 However, some clinicians were reluctant to utilize this probe due to the risk of complications secondary to the use of 200J of energy per treatment. 8 Some studies reported no major postoperative complications,9–12 but most studies reported uncontrolled hypotony,9,10,12–16 anterior chamber inflammation,13–18 loss of BCVA greater than 2 lines,13–23 and even phthisis bulbi.16,18
In 2020, a second generation MicroPulse probe with a 600-micra diameter was introduced to the market (MicroPulse Revised P3® Delivery Device, Iridex Corporation, Mountain View, CA, USA). The predominant differences between the revised probe and its previous iteration include: 1) recession of the fiber tip with the addition of a fluid channel to enable consistent fiber immersion in fluid during treatment to improve coupling, hence delivering more energy in a more consistent fashion; 2) integration of concave “scleral-matching” footplate and “limbal-matching” footplate face curvature to improve probe stability; 3) reduction of the footplate size for easier placement for compromised eyes with limited exposure; 4) elongation of the stem to improve visualization of the treatment area; and 5) adjustment of the photon dispersion profile to a more perpendicular orientation than in the first generation, which ensures more focal laser to the target tissue (see Figure 1). 24 Overall, these modifications ensure more optimal tissue coupling between the delivery device and tissue, which facilitates a constant consistent pressure delivered from the footplate to the tissue.
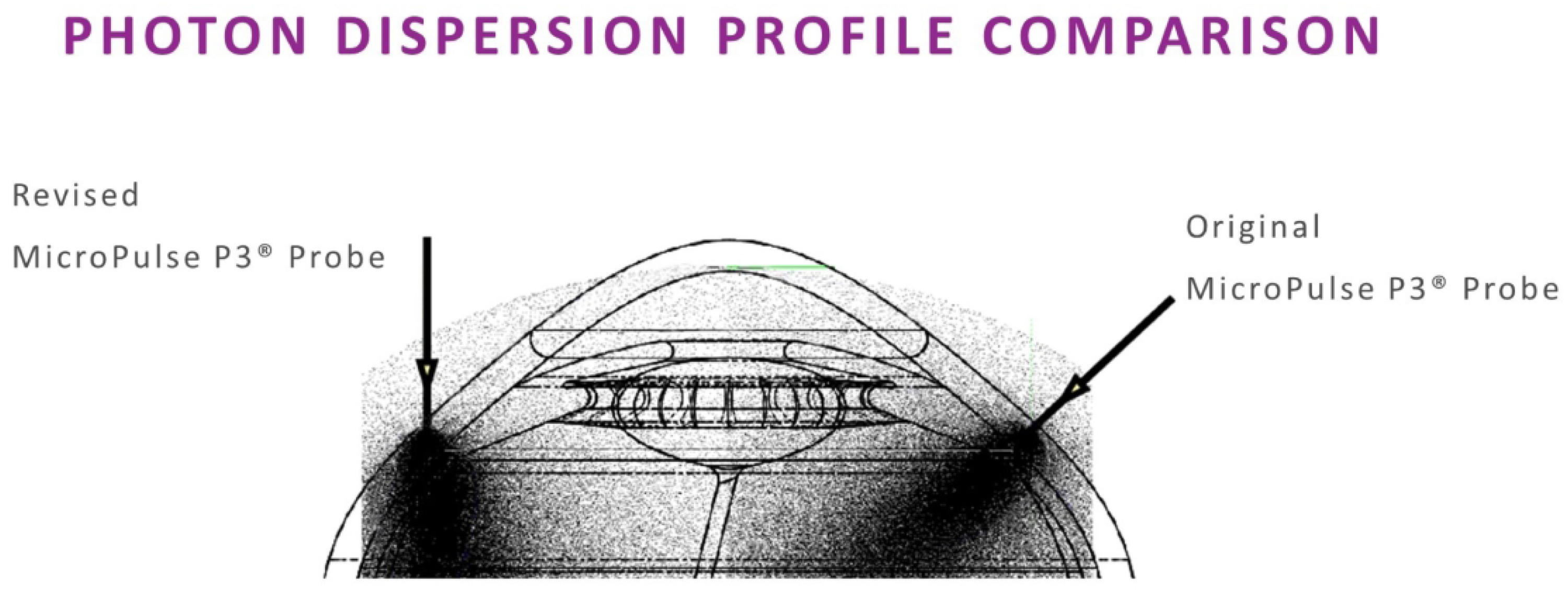
Comparison of photon dispersion profile between first and second generation MicroPulse P3 delivery device. Permission obtained from IRIDEX Corp.
Recent prospective studies have demonstrated a dose-dependent relationship associated with higher energy settings and improved IOP with both the first- and second-generation probe.25,26 Given the lack of consensus regarding the ideal treatment parameters for MicroPulse TLT, our study utilizes different treatment paradigms to assess the efficacy and safety profile of MicroPulse Revised P3 Delivery Device in the treatment of refractory glaucoma, under the longest durations and highest fluences reported to date. To the knowledge of the authors, this is the first prospective study in literature which reports outcomes of the second-generation MicroPulse probe utilizing these revised settings.
Methods
Study design
A prospective, interventional study was conducted at a tertiary hospital setting from January 2022 to June 2023. The study was approved by the Mayo Clinic Institutional Review Board (IRB) on November 11, 2019, and adhered to the tenets of the Declaration of Helsinki. The registration number of this study on the National Institute of Health (NIH) website https://clinicaltrials.gov/ is NCT05654493. Participants were followed up for 6 months by a single glaucoma subspecialist at Mayo Clinic in Jacksonville, FL. Informed consent was obtained from all patients.
Participants
Patients of both genders and of any race aged over 18 years, were deemed eligible for the current study if they had been diagnosed with refractory glaucoma (defined by an IOP above the target level or having evidence of disease progression with visual field deterioration despite maximal tolerated medical therapy) and/or were considered poor candidates for secondary incisional glaucoma surgery. The exclusion criteria consisted of patients with significant scleral thinning, concurrent eye infection or inflammation, and a history of intraocular surgery performed ≤2 months prior to enrollment. Significant scleral thinning was diagnosed in patients with >1 clock hours of involvement detected on transillumination and confirmed using Cirrus high-definition optical coherence tomography (HD-OCT) imaging before exclusion. Pregnant women and patients enrolled in other clinical trials were also excluded.
Procedure
Patients were enrolled to receive MicroPulse TLT and were randomly assigned into three groups with differing total treatment times (200, 240, or 300 s) and sweep numbers (8 or 10 sweeps). Participant randomization was performed using an online random number generator. 27 Participant enrollment and random assignment was performed by the primary investigator, and all subjects were blinded to the treatment arm to which they were assigned. Treatment parameters are summarized in Table 1. A single glaucoma surgeon (S.D.) carried out all MicroPulse TLT procedures. Patients were placed in a supine position and a lid speculum was placed after monitored anesthesia care with propofol injection. Topical lidocaine gel in conjunction with a viscous artificial tear (Goniosol) was used as a coupling agent. No peri- or retrobulbar blocks were performed. All patients were treated with 2500 mW with a wavelength of 810 nm and duty cycle of 31.3%. A sterile, single-use, revised MicroPulse P3 Probe was applied using steady pressure parallel to the visual axis and the fiber-optic tip was positioned approximately 3 mm posterior to the conjunctival limbus. Three and 9 o'clock hours, previous sites of glaucoma surgery (filtering and drainage implant areas), and places of scleral thinning were avoided. The probe was moved continuously along the limbus and slid back and forth 4 or 5 times per hemisphere, depending on the treatment group. Eyes under MicroPulse TLT for 300 s underwent total of 10 sweeps (300 s group), MicroPulse TLT for 240 s had a total of 8 sweeps (240 s group), and MicroPulse TLT for 200 s underwent a total of 10 sweeps (200 s group). The average arc length spanned was 22 mm. Patients were discharged with topical 1% prednisolone acetate QID followed by a tapering course over an additional 2 weeks. No preoperative glaucoma medication washout was performed.
Micropulse transscleral laser therapy treatment.
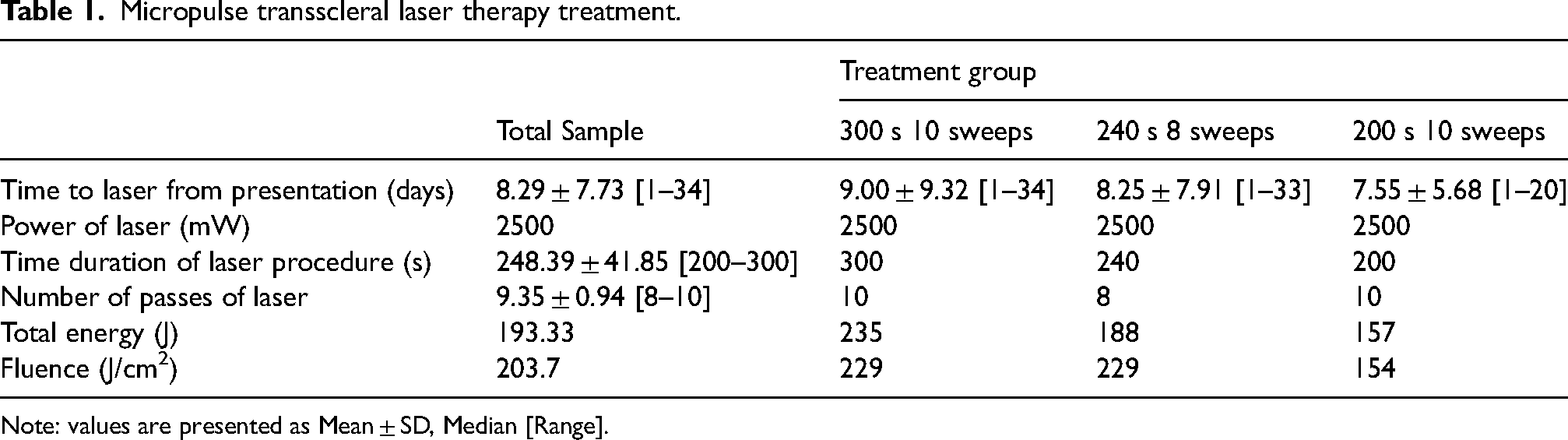
Note: values are presented as Mean ± SD, Median [Range].
Data collection and follow-up
Clinical data was recorded within electronic medical records using a standardized data collection form. Pre-operative data of interest included the following: age, gender, race, laterality, type of glaucoma, severity, procedure date, number of glaucoma medications, prior eye or laser surgery in the treated eye, lens status, IOP, imaging of anterior (ciliary body, angle) and posterior segment structures (optic nerve and fovea), and best-corrected visual acuity (BCVA). Glaucoma severity was classified according to the International Classification of Diseases 10 (ICD-10) definition. 28 The following post-operative data was collected: IOP, number of glaucoma medications, changes to anterior segment structures (ciliary body, angle, nerve, and fovea), BCVA, laser settings (power, time superior and inferior, duty cycle), and complications related to the procedure (iritis, corneal edema, hyphema, vitreous hemorrhage, vision loss, cataract progression or hypotony maculopathy). Total energy (J) and fluence (J/cm2) were also recorded for each treatment group. Total energy was calculated from the product of duty cycle, laser power (W), and exposure duration, while fluence was calculated from the product of laser power (W), duty cycle, and dwell time (s) divided by area (cm2). The spot diameter from the revised probe was measured to be 600 μm, corresponding to an area of 0.0028 cm2. 29
Follow-up visits were set at 1, 3, and 6 months post-MicroPulse TLT laser intervention. Intraocular pressure, glaucoma medications, and BCVA were recorded at every follow-up visit. Intraocular pressure was measured using Goldmann Applanation Tonometry (GAT), and BCVA was assessed using a Snellen eye chart at 20 feet. Changes to the structure of the ciliary body, angle, nerve, and fovea were assessed in an observational manner using Cirrus HD-OCT imaging and ultrasound biomicroscopy (UBM) examination by the study's principal investigator (S.D.) at months 3 and 6.
Outcome measures
The primary outcome measure of this study was surgical success at the final follow-up visit (6 months). Surgical success was defined as a reduction of IOP ≥ 30% from baseline and between 6–18 mmHg, with no additional anti-glaucoma medications or secondary glaucoma surgical reinterventions required. 30 All eyes which did not meet surgical success were considered failures. Secondary outcome measures of success included changes from baseline in the number of glaucoma medications taken, BCVA, anterior (ciliary body, angle) and posterior segment structures (optic nerve, fovea), and visual fields at 6 months. The frequency of MicroPulse TLT-related complications and number of secondary glaucoma surgical reinterventions required throughout the follow-up period were also assessed.
Statistical analysis
Statistical analysis was performed using the software SPSS v25.0 software (IBM Corporation, NY). Descriptive statistics were expressed as the mean ± standard deviation for continuous variables, and frequency (percentage) for categorical variables. A paired sample t-test was performed for the primary analysis to compare mean IOP reduction from baseline to all the three time points (1, 3, 6 months). Within groups comparison of reduction of topical medications was performed and p-values were derived using Wilcoxon Signed-Ranks tests for each follow-up time point (1, 3, 6 months). A paired sample t-test was also performed to compare change in BCVA (logMAR) from baseline to all three time points (1, 3, 6 months). Intergroup comparisons were performed using the Kruskal-Wallis test.
Results
Patient demographics are reported in Table 2, and a diagram depicting the flow of eyes through each stage of the study can be found in Figure 2. A total of 62 eyes from 40 patients met inclusion criteria and were enrolled in this study. The 300 s, 240 s, and 200 s groups consisted of 22, 20, and 20 eyes, respectively. Most eyes were Caucasian (51 eyes, 82.3%) with 33 eyes from female subjects (53.2%). Primary open angle glaucoma (POAG) was the most common diagnosis, affecting 57 eyes (91.9%), and the majority of eyes had severe-stage glaucoma (39 eyes, 62.9%). The mean number of prior glaucoma laser procedures for all eyes was 1.27 ± 1.22 and was similar across all groups. Cataract surgery was the most common prior ocular procedure, having been performed in 50 eyes (80.6%). Differences in baseline values for IOP, topical medications, and LogMAR were found to be statistically significant between groups.
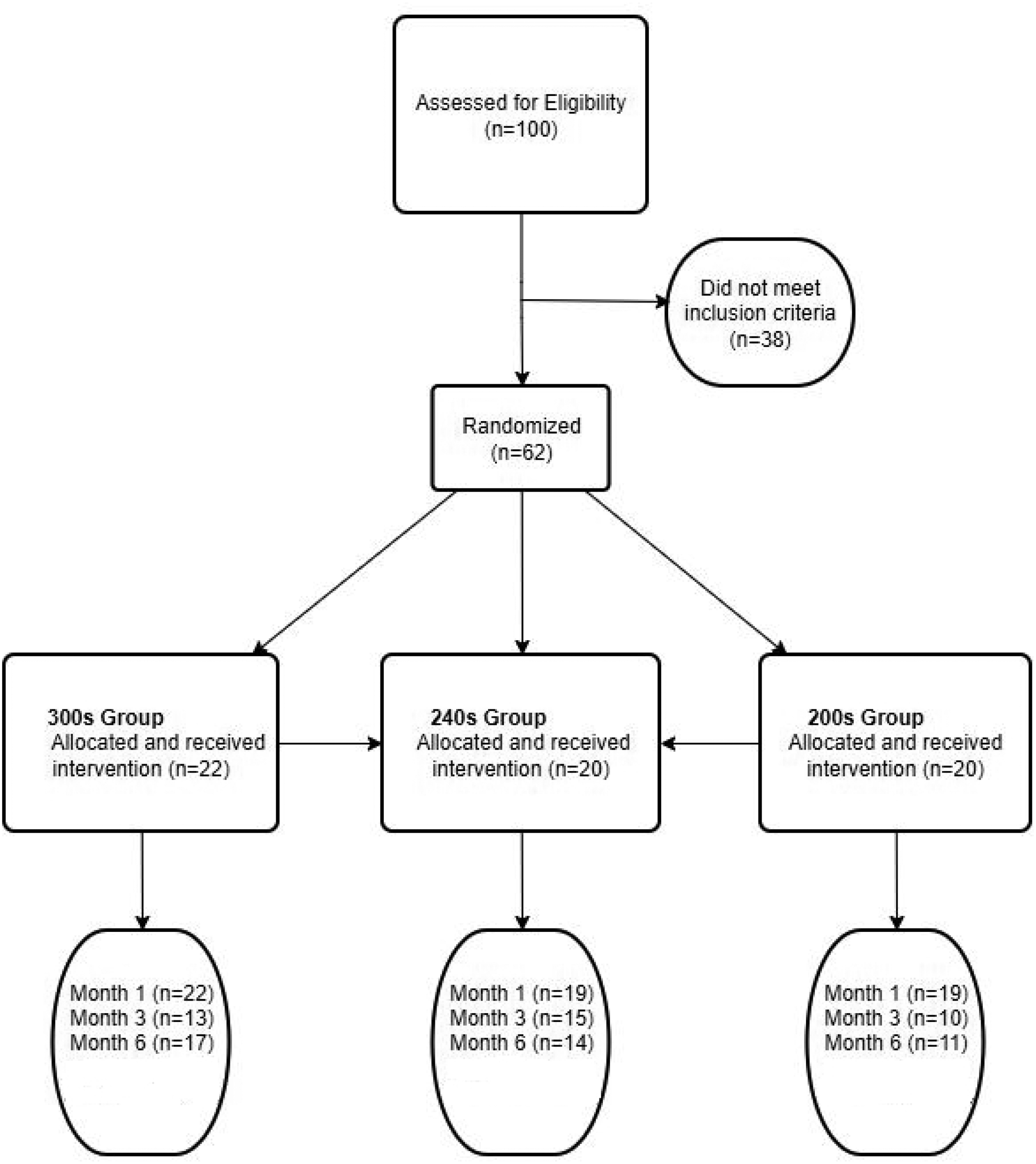
CONSORT flow diagram showing flow of eyes (n) through each stage of the clinical trial.
Baseline patient demographic and clinical factors.
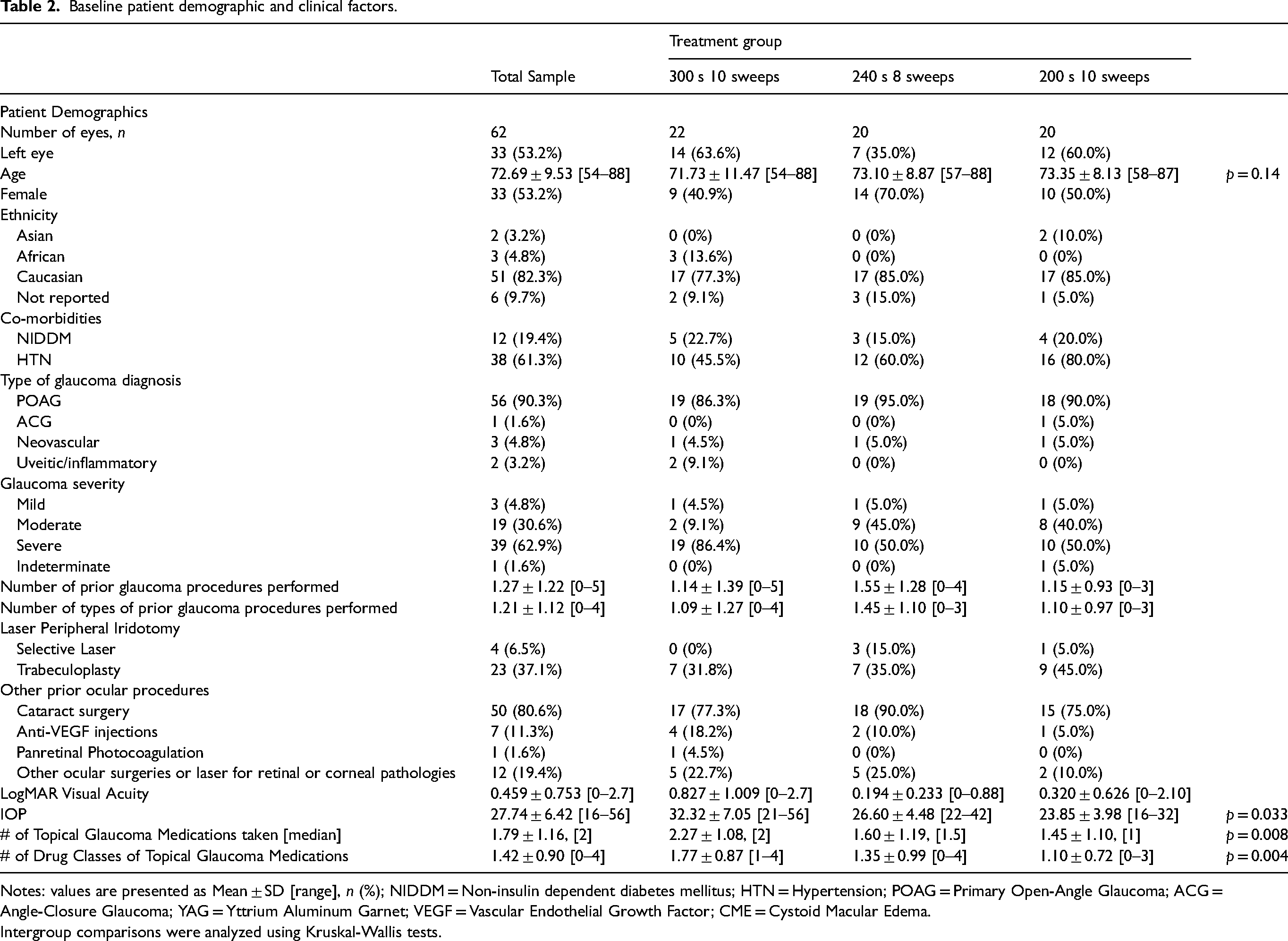
Notes: values are presented as Mean ± SD [range], n (%); NIDDM = Non-insulin dependent diabetes mellitus; HTN = Hypertension; POAG = Primary Open-Angle Glaucoma; ACG = Angle-Closure Glaucoma; YAG = Yttrium Aluminum Garnet; VEGF = Vascular Endothelial Growth Factor; CME = Cystoid Macular Edema.
Intergroup comparisons were analyzed using Kruskal-Wallis tests.
Mean time from MicroPulse TLT to last follow-up visit for each group is displayed in Supplementary Table 1, and changes from baseline in IOP at each post-operative timepoint can be found in Figure 3 and Supplementary Table 2. IOP reductions from baseline were between 36.1 to 49.8% with the highest reductions seen in the 300 s group at all timepoints. Furthermore, statistically significant reductions from baseline in mean IOP (in absolute units and percentages) were seen within and between all three groups at all three timepoints (1, 3, 6 months). Surgical success was achieved in 72.7% (300 s group), 75.0% (240 s group), and 80.0% (200 s group) of eyes.
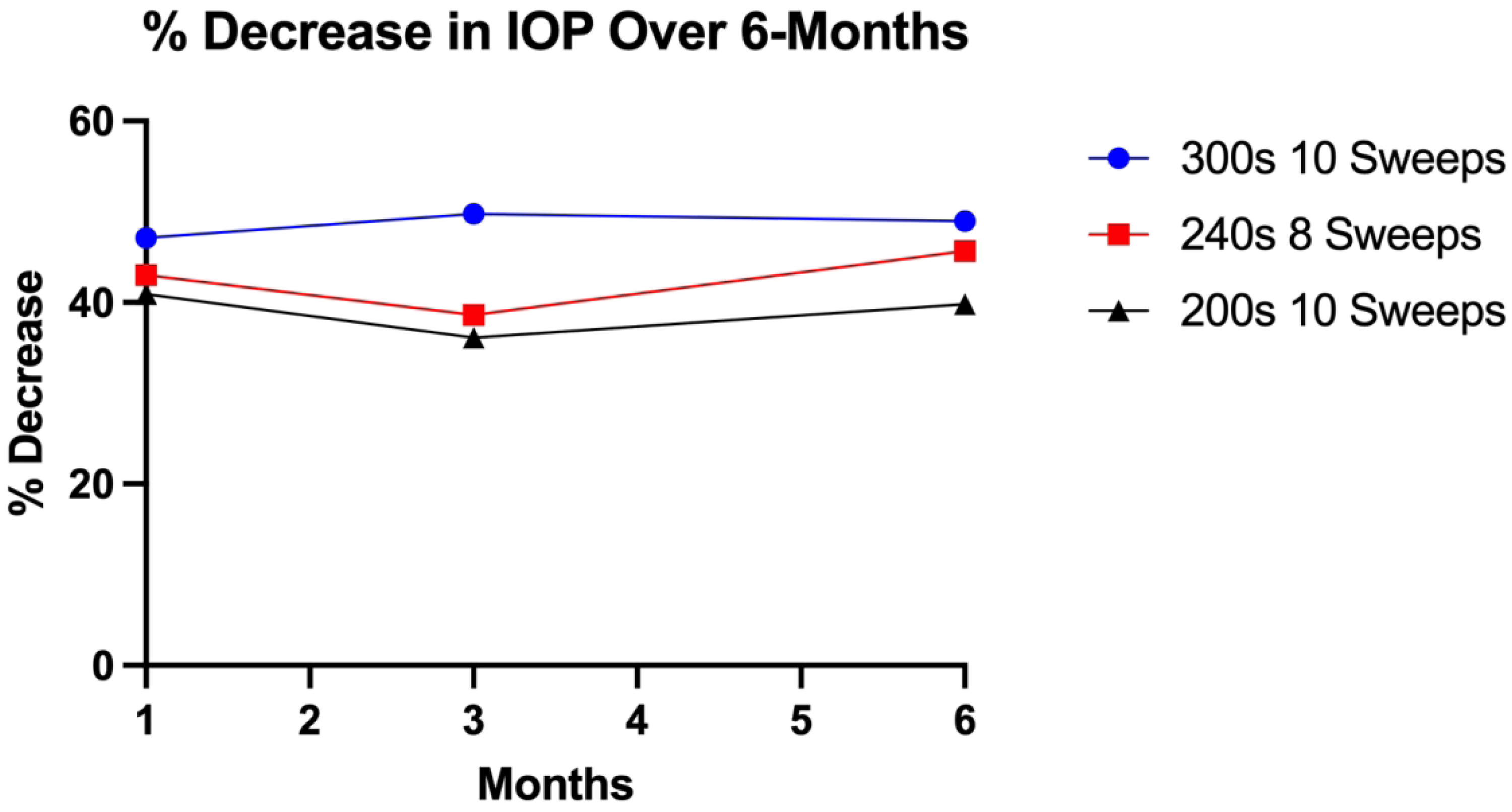
Line graph showing the percentage decrease in intraocular pressure at 1-, 3-, and 6-month follow-up timepoints for each group. IOP – Intraocular pressure.
Changes from baseline in BCVA (in logMAR) at each postoperative timepoint can be found in Figure 4 and Supplementary Table 3. Overall, there were no significant changes in visual acuity in the total sample at any of the three time points (1, 3, 6 months). Transient reductions in visual acuity prior to 6 months were linked to cystoid macular edema, IOP spikes, and hyphema; however, all these cases resolved by the 6-month mark. Nine of 42 eyes (21.4%) assessed at 6 months showed a decrease in visual acuity by ≤2 Snellen lines. At 6 months, only 2 of 37 eyes demonstrated a reduction in visual acuity >2 Snellen lines. In one case, the decline was attributed to lens subluxation associated with aging, while the other involved a patient with limited visual potential (baseline visual acuity of 20/300). Both instances were deemed unrelated to the MicroPulse TLT procedure. One eye in the 240 s group experienced significant improvement in visual acuity at 6 months (p = 0.025).
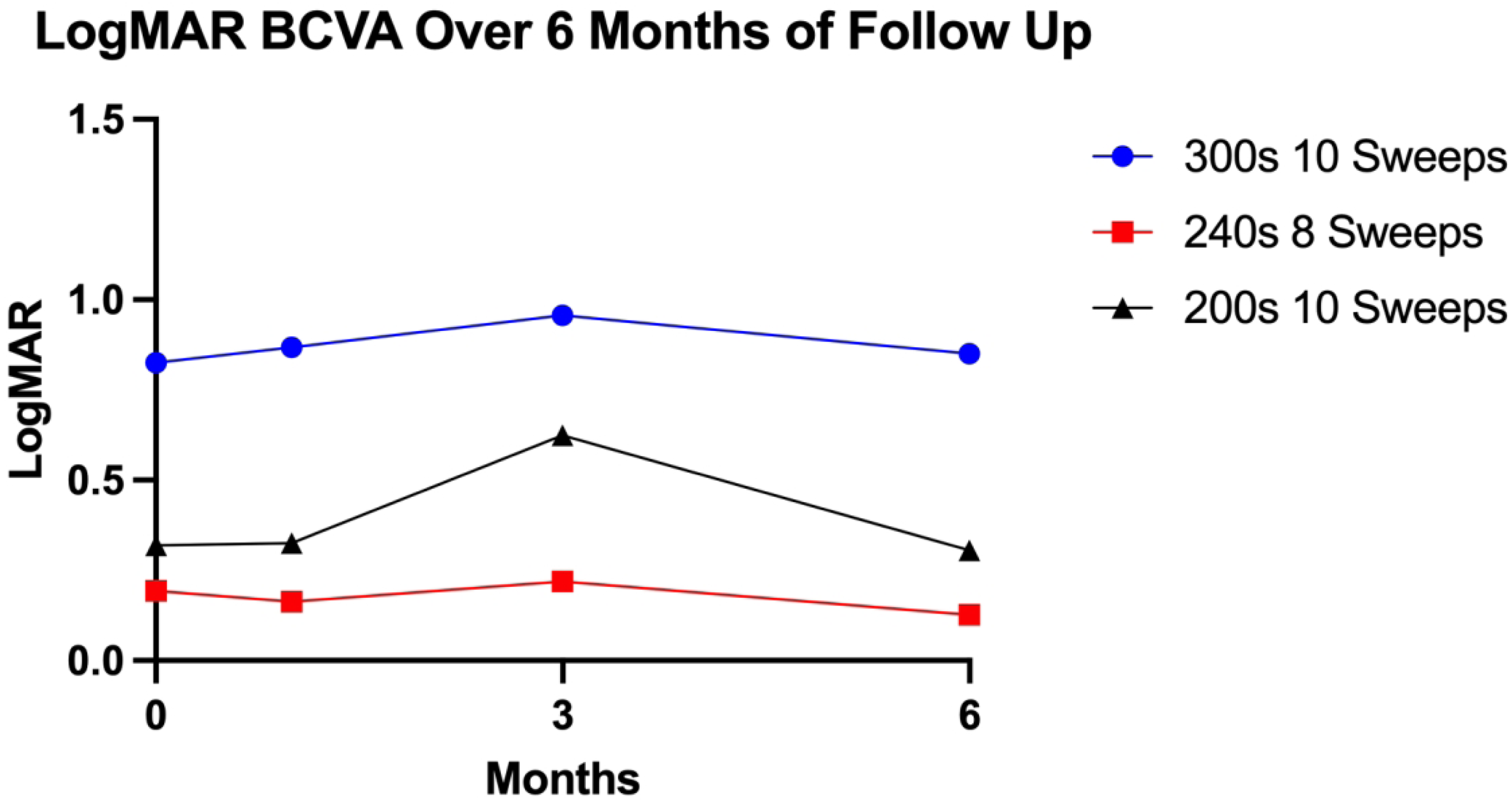
Line graph showing the change in LogMAR best corrected visual acuity at baseline, 1-, 3-, and 6-month follow-up timepoints for each group. BCVA – Best corrected visual acuity.
Changes from baseline in the number of glaucoma medications at each postoperative timepoint can be found in Figure 5 and Supplemental Table 4. Overall, a statistically significant reduction in the number of topical medications from baseline was found at each follow-up point (1, 3, 6 months) for the total sample. Within groups, significant medication reduction was reported for the 300 s group at 6 months (p = 0.049) and for the 200 s group at 1 month (p = 0.015). All groups showed a decrease in the number of medications at all other time points but did not reach statistical significance. No statistical difference was found in medication reduction when comparing between groups at any timepoint.
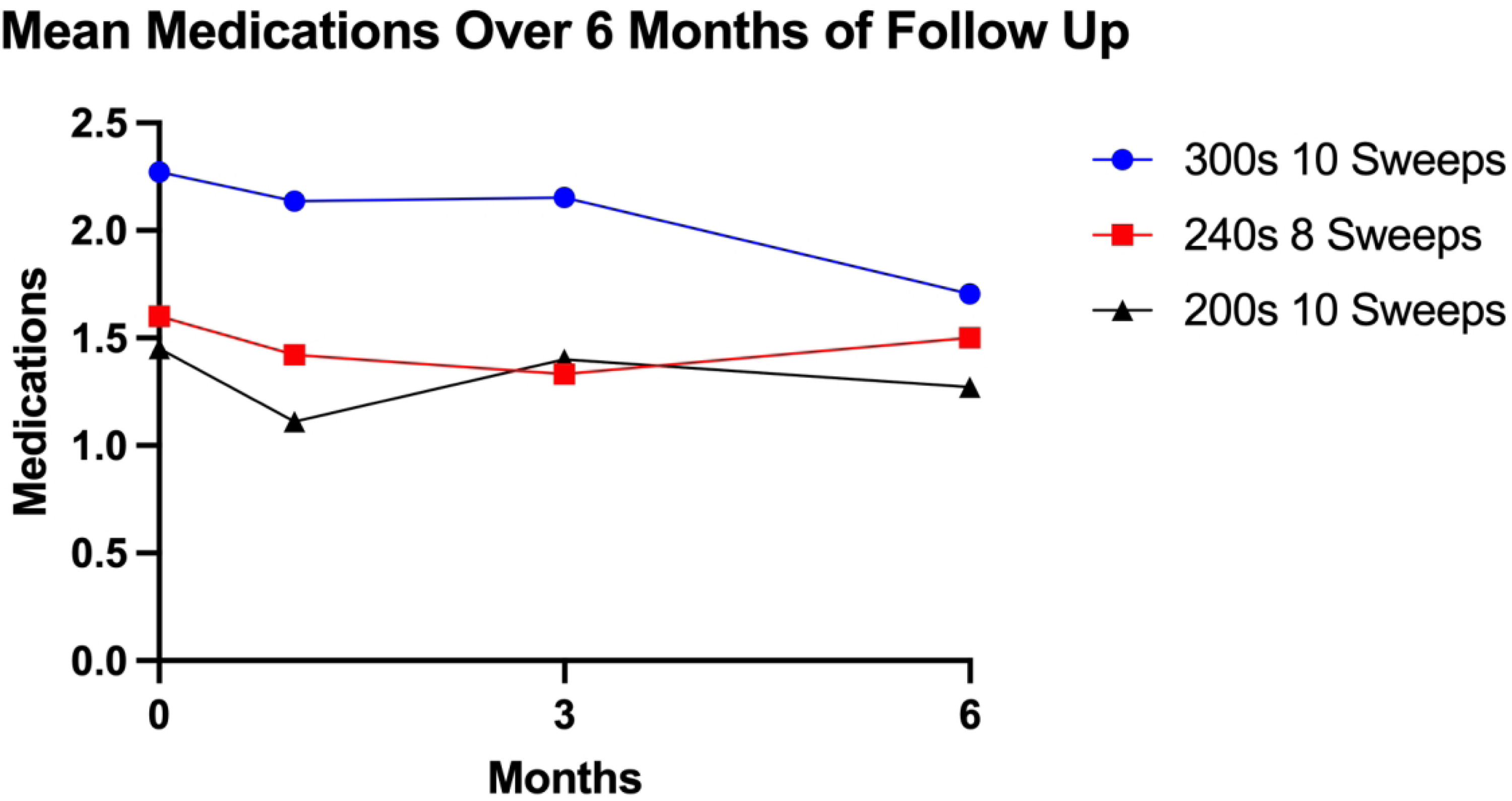
Line graph showing the change in anti-glaucoma medications used at baseline, 1-, 3-, and 6-month follow-up timepoints for each group.
Postoperative complications are listed in Table 3. No adverse events were reported intraoperatively while performing the MicroPulse TLT. Following the procedure, adverse events were minimal. IOP spikes (defined as an increase in IOP by 25% greater than baseline) that were suggestive of steroid response occurred in three eyes in the 300 s group within 1 month and in one eye of the 200 s group at 3 months post-operatively. In the 300 s group, one eye developed hyphema and one eye developed cystoid macular edema. Secondary glaucoma surgical interventions before the 6-month post-operative timepoint included implantation of an Ahmed glaucoma valve FP7 (New World Medical, Rancho Cucamonga, CA, USA) in one eye in the 300 s group and a Xen gel stent (Allergan Inc., CA, USA) in one eye in the 200 s group. Both eyes had a history of multiple glaucoma procedures and IOPs continued to be uncontrolled following MicroPulse TLT. Additionally, no structural changes, including ciliary body thinning or damage, peripheral anterior synechiae, cyclodialysis, hypotony maculopathy or other posterior findings, for any eye were visualized on the Cirrus HD-OCT or UBM scans at months 3 and 6 post-operatively.
Adverse events after MicroPulse transscleral Laser therapy.
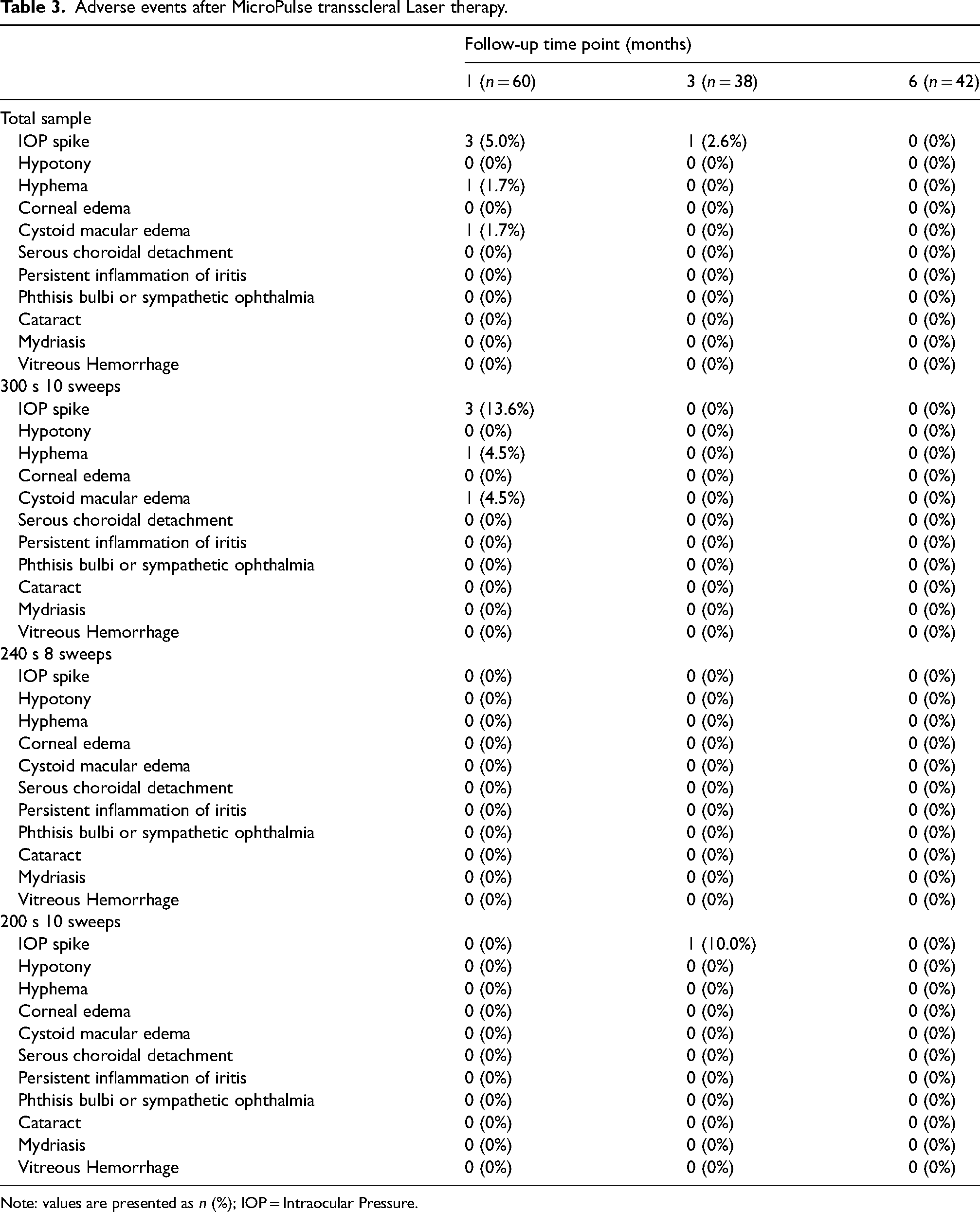
Note: values are presented as n (%); IOP = Intraocular Pressure.
Discussion
This study reports safety and efficacy outcomes of the second-generation MicroPulse TLT, up to 6 months post-operatively. To our knowledge, this is only the second prospective study on the MicroPulse Revised P3 Delivery Device and the first which evaluates MicroPulse TLT outcomes with 300-, 240-, and 200-s treatment durations. Additionally, outcomes following 3 differing MicroPulse TLT treatment times have not previously been reported. In this study, all three treatment times resulted in surgical success in over 70% eyes in all three groups at 6 months post-operatively, with the highest success rate being 80% in the 240 s group. Significant reductions in IOP were seen at all three timepoints in all three groups, with the 300 s group experiencing the largest reduction in IOP at 6 months (−16.06 mmHg; −49.0%); however, this may possibly be due to the significantly higher baseline mean IOP within this group (32.32 mmHg). Likewise, the 300 s group had the only statistically significant reduction in anti-glaucoma medications at 6 months (−0.41; p = 0.049), although it should be noted that this group consisted of 19 (86.4%) severe glaucoma patients compared to 10 (50%) in the other two groups.
Overall, the second-generation Micropulse TLT demonstrated an excellent safety profile across all three groups as all adverse events were temporary, and no vision-threatening complications occurred, despite the use of longer fluence and treatment durations. The 300 s treatment group did experience more transient postoperative complications (including hyphema, IOP spikes, and cystoid macular edema) compared with the other groups but these events were largely associated with patients diagnosed with secondary glaucomas (including pseudoexfoliative, neovascular, and uveitic types) or those undergoing treatment changes, such as alterations in antiglaucoma medication use. Similarly, although a trend suggested that patients with longer treatment durations and energy levels were more likely to require secondary glaucoma surgery, this was mainly attributed to the presence of secondary glaucomas and more severe glaucoma in these individuals.
Currently, there are two studies in prior literature which have reported the outcomes of MicroPulse TLT with the Revised P3 Delivery Device. In their single-blinded randomized controlled trial (RCT), Balendiran et al., 25 reported 6-month outcomes of the second-generation MicroPulse TLT under total treatment durations of 120 s (6 sweeps) and 100 s (6 sweeps). The authors observed a significantly greater reduction in the 120 s group at month 3 (32.2% vs 4.1% decrease; p = 0.007) and month 6 (37.8% vs 3.6% decrease; p = 0.021) when compared to the 100 s group, with no vision-threatening complications or changes in BCVA reported throughout the follow-up period. 26 The comparably higher percentage IOP reduction observed in our total sample at month 3 (36.1–49.8% decrease) and month 6 (39.8–49.0% decrease) may suggest longer treatment times to be more efficacious. However, comparison is limited by differing study designs (single-blinded RCT vs non-blinded RCT) and the patient inclusion criteria for both studies (POAG patients only vs various glaucoma types). In a second study, Akiyama et al retrospectively assessed 40 patients with varying glaucoma types receiving second-generation MicroPulse TLT over a total treatment duration of 100 s and reported a comparably lower mean percentage IOP reduction of 26% at 3 months post-operatively. 31 However, these authors did not report the total number of sweeps applied during the treatment procedure.
Prior prospective MicroPulse TLT studies using the first-generation P3 probe reported mean IOP reductions of 34.6%-49.9% at 6 months.7,32,33 In their retrospective study, Akiyama et al compared clinical outcomes between the original and revised MicroPulse P3 probes and did not find significant differences in IOP reduction, glaucoma medication reduction, or BCVA changes between both devices, through 3 months. 31 However, the study reported significantly lower pain levels for the procedure, compared to patients receiving MicroPulse TLT with the original P3 probe in another study by Tan et al (No pain: 68.4% vs 94.1%; Mild pain: 5.9% vs 26.3%; Moderate pain: 0% vs 5.3%).31,32 It was hypothesized that the revised probe may cause less patient discomfort due to an additional fluid channel at the device tip, thereby preventing the protrusion from making contact with the conjunctiva. 31
From a surgeon's perspective, the Revised P3 Delivery Device possesses numerous advantages over the first-generation probe. This second-generation probe was designed to address the ergonomic flaws of the original probe, with the aim of increasing energy delivery without compromising safety and efficacy outcomes. Unlike the protruding, rounded tip of the original probe, the revised probe has a recessed tip to allow for smoother gliding across the conjunctiva, minimizing any resultant trauma. The revised probe is also angled to direct laser delivery away from the limbal tissues and is positioned 3 mm posterior to the subconjunctival limbus, leading to better visualization of the treatment area and more consistent energy delivery. The footplate surface is concave to enhance stabilization, keeping the probe angled to the scleral surface. The original probe faced difficulties with maintaining a perpendicular position to the globe which led to less consistent laser delivery and treatment outcomes. 24 The enhancements of the Revised P3 Delivery Device are expected to improve surgical dexterity and reduce the significant complications seen with the first-generation probe, thereby positioning the device as a promising option for the treatment of refractory glaucoma. Furthermore, Agnifili et al. investigated the mechanisms of action of MicroPulse TLT with the first-generation probe, focusing on its beneficial modifications in the sclera that enhance uveoscleral aqueous humor outflow. Their study showed a significant increase in intra-scleral hypo-reflective space, with the superior, inferior, and total areas (S-MISHA, I-MISHA, and T-MISHA) increasing by 50% (p < 0.001), and a reduction in scleral reflectivity (S-SR, I-SR, and T-SR), particularly in successful treatments. These changes were associated with a median IOP reduction of 21% in failures and 38% in successes. 34 Building on the enhancements of the second-generation probe, it could be hypothesized that the refined 600-micra design would allow for more accurate scleral targeting, potentially resulting in more consistent and significant improvements in uveoscleral outflow and a greater overall reduction in IOP.
Despite its prospective design, this study possesses several limitations. Changes in anterior segment structures were measured subjectively rather than quantitatively; therefore, the precision and accuracy of these findings is limited. This study is also a relatively short-term one, with a few eyes having incomplete follow-up. The significant loss to follow-up observed over 6 months can be attributed to several factors, including patient non-compliance leading to reduced communication with physicians, difficulty attending follow-up visits, and the occurrence of adverse events or difficulties related to the COVID-19 pandemic leading to the delay of follow-up visits. Two patients also underwent secondary glaucoma surgeries prior to 6 months, which impacted their participation in the study. However, although a similar number of eyes from each group were analyzed at each timepoint and the sample size remained large enough at each timepoint to reach statistical significance for IOP reduction outcomes. Another significant limitation was the imbalance in baseline IOP, LogMAR, and glaucoma medication use between the three groups. As a result, intergroup comparisons of IOP and medication outcomes are limited. Despite this, we believe that reporting clinical outcomes from the longest treatment durations and highest fluence values to date adds valuable insights to the literature, enhancing the understanding of the efficacy of MicroPulse TLT when applied at higher energy levels. Regardless of the lack of clinically meaningful intergroup comparison, our study demonstrates that MicroPulse TLT with the Revised P3 Delivery Device can be safely performed at a fluence as high as 229 J/cm2 without causing significant long-term vision-affecting complications, through 6 months. Larger scale and longer-term prospective studies on the second generation MicroPulse TLT are currently ongoing.
Conclusion
Second-generation MicroPulse TLT, performed under fluence values ranging from 154–229 J/cm2, appears to be a safe and effective treatment option for patients with refractory glaucoma up to 6 months post-operatively. Both significant IOP reduction and reduced medication burden are observed, with an excellent intra- and post-operative safety profile.
Supplemental Material
sj-docx-1-ejo-10.1177_11206721251340102 - Supplemental material for Safety and efficacy of MicroPulse transscleral laser therapy with the revised P3 delivery device: A randomized controlled trial
Supplemental material, sj-docx-1-ejo-10.1177_11206721251340102 for Safety and efficacy of MicroPulse transscleral laser therapy with the revised P3 delivery device: A randomized controlled trial by P. Connor Lentz, Isabella V. Wagner, Devesh Kumar, Nithya Boopathiraj, Bryan C. H. Ang, Abhimanyu Ahuja, Leticia Checo, Darby D. Miller and Syril Dorairaj in European Journal of Ophthalmology
Footnotes
Acknowledgments
We would like to thank Ms. Joyce Baker for her generous contributions to the Department of Ophthalmology, Mayo Clinic, Florida, United States.
Data sharing statement
The author's institution does not permit data sharing. Any queries should be directed to the corresponding author (S.D.).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Patient consent
Informed consent was obtained from all participants. All patient data and images have been deidentified and there is no personal identifying information within this report.
ORCID iDs
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.