
Abstract
Purpose
Telangiectatic capillaries (TelCaps) are large capillary microaneurysms that can be found in diabetic patients. Focal laser photocoagulation is the standard treatment for these lesions. In case of a lesion too close to the fovea, there is a risk of central scotoma and conventional laser should not be used. In this case, dynamic phototherapy (PDT) can be discussed.
Case report
Two patients with perifoveal TelCaps associated with diabetic macular edema were treated with PDT. There was persistent central macular edema in spite of a well-executed treatment with intravitreal injections (IVT). Both visual acuity and central macular thickness improved after PDT. This therapy seems to be a possible option in the absence of another therapeutic solution for the treatment of perifoveal TelCaps with promising results should be noted despite the difficulty accessibility to Verteporfin.
Conclusion
The management of perifoveal TelCaps is complex due to their impact on visual acuity, the therapeutic burden for patients, as well as the potential complications associated with focal laser. In the absence of other therapeutic options, the use of PDT may prove relevant in this indication.
Keywords
Introduction
Telangiectatic capillaries (TelCaps) are large microaneurysms that can be found in patients with diabetic macular edema (DME) and retinal venous occlusion (RVO). 1 These lesions are associated with chronic DME and can be the cause of resistance to properly administered intravitreal injection (IVT) treatment. 1 Focal laser photocoagulation is the standard treatment for these lesions. Unfortunately, this laser treatment is not always feasible, especially in the presence of TelCaps too close to the fovea. Laser photocoagulation treatment of TelCaps located less than 500–750 microns from the fovea may cause atrophic scarring lesions responsible for central scotomas.1–3 Minimum distance to be able to carry out laser photocoagulation treatment still remains highly debated, however, a minimal limit of 500 µm from the fovea is generally accepted.
Photodynamic therapy (PDT) is a non-invasive therapeutic method used in the treatment of benign and oncological diseases. 4 It is based on the injection of a photosensitive compound accumulating in pathological tissues. Photosensitising molecules absorb light of the appropriate wavelength triggering a photocytotoxic reaction only within pathological tissues. 4 Various photosensitizers used today are derived from porphyrins. 5
In ophthalmology, PDT has been shown to be effective targeting other rapidly growing vascular structures. 5 In medical retina, PDT can be used in cases of exudative age-related macular degeneration, idiopathic polypoidal choroidal vasculopathy, high myopia, central serous chorioretinitis, circumscribed choroidal haemangioma and choroidal metastases. 6
There were only two cases in the literature describing the efficacy of full-fluence PDT on TelCaps in chronic DME. In both cases, PDT improved visual acuity and significantly reduced central macular thickness. 7 To our knowledge, no study has shown angiographic images of TelCaps occlusion after PDT.
We describe here the results of half-fluence PDT treatment in two diabetic patients with perifoveolar TelCaps (present in the pericentral ring). In both cases, the TelCaps were less than 1000 microns from the centre.
Case report
Case 1
A 68-year-old diabetic patient, followed in our centre for DME, was treating with IVT of dexamethasone implant (DEX-I). Best corrected visual acuity (BCVA) was 60 letters EDTRS (20/63 Snellen). Despite three IVT of DEX-I, neither functional nor anatomical improvement was observed. The patient has no history of high blood pressure and has well-controlled diabetes (glycated haemoglobin at 6.5%).
Spectral-domain optical coherence tomography (SD-OCT) showed DME and TelCaps near the centre of the fovea. Indocyanin green angiography (ICGA) was performed showing late hyperfluorescence of the TelCaps which is few microns from the fovea. (Figure 1). Conventional focal laser photocoagulation was not feasible due to the proximity of the lesion to the fovea. Half-fluence PDT (25 J/mm2, spot size 1500 microns) was chosen due to persistent DME and loss of BVCA.
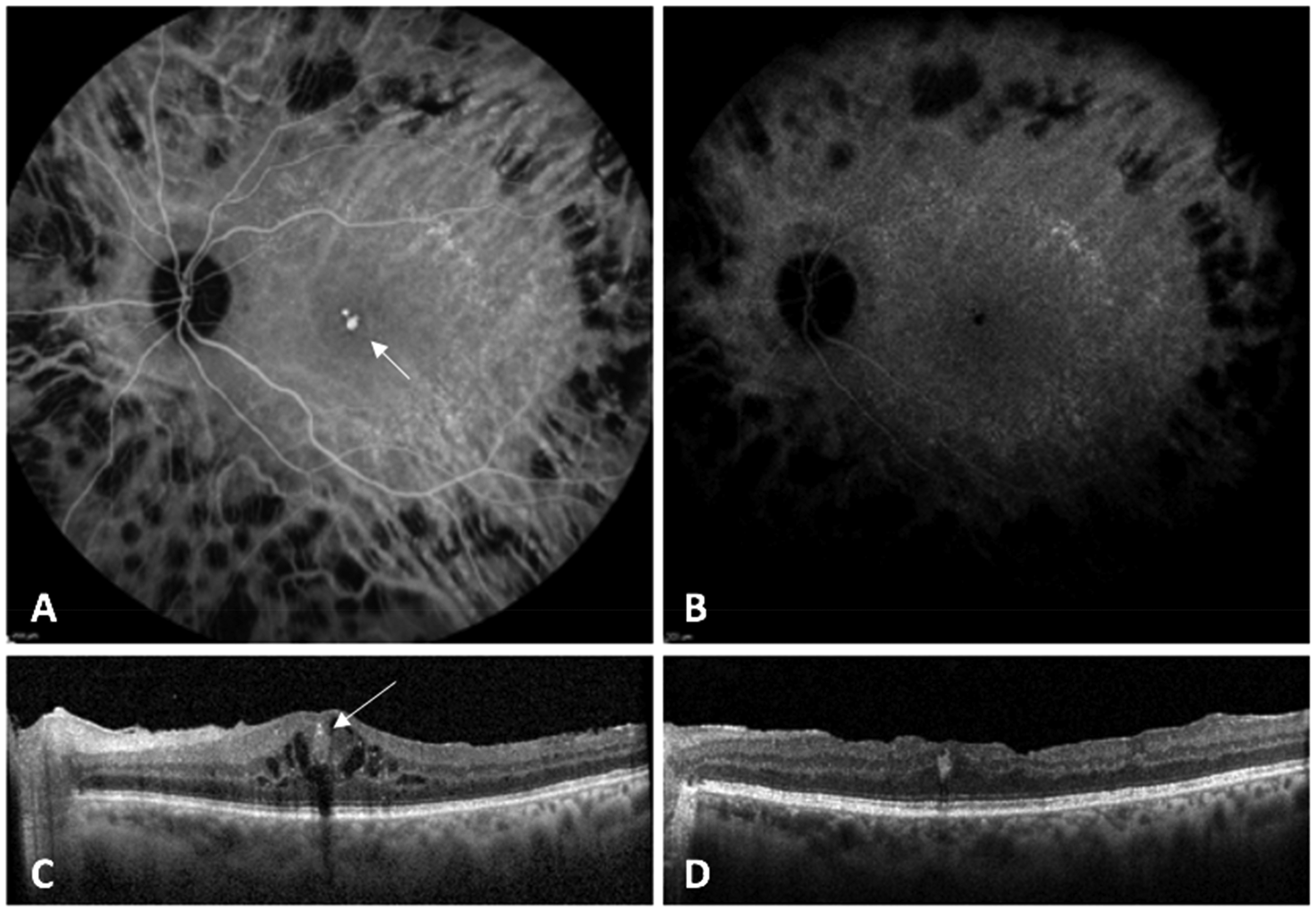
Multimodal imaging case 1 at baseline and 3 months after the PDT treatment: A: ICGA highlighting the central hyperfluorescence at baseline (6:30 min, middle phase); B: ICGA highlighting the disappearance of central hyperfluorescence at 3 months (7:30 min, middle phase); C: SD-OCT showing of intra-retinal edema next to ovoid lesion with hyperreflective shell, hyporeflective content and posterior shadow cone at baseline; D: SD-OCT showing the disappearance of intra-retinal edema and reduction in size of the occluded lesion at 3 months (ICGA: indocyanine green angiography, SD-OCT: Spectral Domain Optical Coherence Tomography, PDT: Photodynamic Therapy).
At 1 months following PDT treatment, BVCA increased to 70 letters (20/40 Snellen) and CMT was 424 µm (decreased of 56 µm). SD-OCT showed a hyperreflective TelCaps meaning its occlusion.
At 3 months, BVCA improved to 72 letters (20/40 Snellen), and CMT was 401 µm (decreased of 23 µm) without any exsudative sign on SD-OCT. ICGA did not find any hyperfluorescence, indicating successful occlusion of the TelCaps (Figure 1).
Eighteen months after the PDT, BCVA continues to increase to 80 letters (20/25 Snellen), with no DME recurrence. No further IVT were required during follow-up. No retinal atrophy was observed after PDT.
Case 2
A 84-year-old diabetic patient, was referred to our centre for DME resistant to both anti-VEGF and DEX-I IVT treatment. BVCA was 50 letters EDTRS (20/100 Snellen). SD-OCT shows DME and epiretinal membrane, as well as TelCaps. ICGA demonstrated a late hyperfluorescence confirming TelCaps (Figure 2). Although these TelCaps are located approximately 900 microns from the fovea, PDT treatment was preferred for this elderly patient because of the inability to maintain a still head position, which increases the risk of foveal atrophy in the event of laser focal inaccuracy. Half-fluence PDT (25 J/mm2, spot size 1500 microns) was chosen as a treatment option due to persistent DME and loss of BVCA, before possible epiretinal membrane surgery.

Multimodal imaging case 2 at baseline and 3 months after the PDT treatment: A: ICGA highlighting the central hyperfluorescence at baseline (10 min, middle phase) B: ICGA highlighting the decrease of central hyperfluorescence at 3 months (5:30 min, middle phase) C: SD-OCT showing intra-retinal edema next to ovoid lesion with hyperreflective shell, hyporeflective content and posterior shadow cone at baseline D: SD-OCT showing decrease of intra-retinal edema and reduction in size of the partially occluded lesion at 3 months E: SD-OCT showing foveal intra-retinal edema at baseline F: SD-OCT showing persistent foveal intra-retinal edema at 3 months (ICGA: indocyanine green angiography, SD-OCT: Spectral Domain Optical Coherence Tomography, PDT: Photodynamic Therapy).
At 1 months following PDT, BVCA increased to 60 letters (20/63 Snellen) and CMT was 447 microns (decreased of 57 µm) with decrease of DME. The TelCaps was not totally occluded on the SD-OCT.
At 3 months, BVCA improved to 70 letters (20/40 Snellen) and CMT was 421 microns (decreased of 26 µm). SD-OCT showed almost complete disappearance of exsudative signs and ICGA demonstrated a decrease in hyperfluorescence with a decrease in size and intensity of the TelCaps without complete disappearance. It should be noted the appearance of a new TelCaps in the inferomacular area but without involvement in the DME pathophysiology. No retinal atrophy was observed after PDT. The patient was lost to follow-up after this consultation. To our knowledge, he did not benefit from further IVT or surgery on his epiretinal membrane following PDT.
Discussion
We report the successful use of PDT treatment for perifoveal TelCaps in two patients with recalcitrant DME despite good compliance with IVT therapy. These cases suggest that TelCaps alone were responsible for the persistent DME. Targeting these vascular abnormalities contributed to the resolution of the edema. The use of PDT in this indication is off label. PDT promotes thrombosis in neovascular structures, leading to their occlusion and subsequent reduction of macular exudation. However, the exact mechanism of action is not fully understood. The effects of PDT are thought to be related to the interaction of singlet oxygen with lipids in endothelial cytoplasmic membranes. 7
In both cases, the patients did not require further IVT despite a high therapeutic burden prior to PDT. Case 1 showed complete TelCaps occlusion, while case 2 had persistent hyperfluorescence on late ICGA but still showed anatomical and functional improvement. Notably, partial occlusion has also been reported in DME cases treated with IVT anti-VEGF therapy alone. 8 IVT alone has been shown to significantly reduce the number and size of TelCaps. However, in the case of large TelCaps, additional laser photocoagulation is often required. 8 In case 2, no further treatment was pursued due to the overall improvement in DME and the patient's age.
Another case series has previously reported the efficacy of full fluence PDT in the treatment of TelCaps in DME. 7 However, without ICGA, the efficacy of PDT could not be thoroughly evaluated. In our cases, we used half-fluence PDT and systematically performed ICGA, which confirmed complete TelCaps occlusion in case 1 and partial occlusion in case 2.
Focal laser photocoagulation has shown efficacy in the treatment of TelCaps but is associated with photoreceptors alteration and death. 3 Complications include central scotomas, deterioration of colour and night vision, reduced contrast sensitivity, accidental foveal burns and progressive enlargement of laser scars over time. 9 Perifoveolar TelCaps can be treated with navigated laser in some cases, but this technology is not available in all centres. Although it has been shown to be effective, no large trials have evaluated this treatment modality. 10
Subthreshold micropulse laser is an another alternative and adjuvant treatment for DME. 9 This treatment modality demonstrates a high safety profile because repetitive laser pulses allow tissue cooling, preventing thermal burns. 9 Subthreshold micropulse laser may be an alternative treatment for macular diseases such as DME as suggested by some case series. 9 However, long term follow-up data are lacking and its role in the management of DME remains to be defined.
The optimal treatment for DME associated with TelCaps is controversial. Only one comparative trial of TelCaps treatment is currently underway, with initial results expected in the next few months. 2 The aim of this study is to evaluate whether ICGA-guided targeted laser in combination with standard IVT treatment can reduce the number of injections during the first year of treatment compared to IVT alone. The results of this study may contribute to the standardisation of focal laser treatment parameters.
With these two cases, we present an alternative treatment for perifoveolar TelCaps in patients ineligible for conventional laser photocoagulation. This approach has only been reported once in the literature and larger studies are needed to further evaluate the potential role of PDT in this indication. In addition, the issue of verteporfin accessibility will also be considered.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical statement
This study was conducted in accordance with the principles outlined in the Declaration of Helsinki.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Patient consent
All patients received oral and written information and gave ther informed consent.