
Abstract
Purpose
This study evaluated the safety and effectiveness of two models of intrastromal corneal ring segments (ICRS)—symmetric (uniform thickness and base width) and asymmetric (progressive thickness and base width)—for the treatment of oval phenotype keratoconus.
Methods
A prospective, randomized, controlled clinical study was conducted on 64 eyes from 47 patients, divided into two groups: Group 1 (33 eyes) received symmetric ICRS, and Group 2 (31 eyes) received asymmetric ICRS. Comprehensive ophthalmic evaluations, including visual acuity, corneal topography, tomography, and aberrometry, were performed preoperatively and at 1, 3, 6, and 12 months postoperatively.
Results
At 12 months, Group 2 demonstrated significantly greater reductions in K1, Km, Kmax, asphericity, vertical coma and spherical aberration, and most topographic indices compared to Group 1. Best-corrected visual acuity was higher in Group 2, reaching statistical significance at 6 months. No implant-related complications were observed in either group.
Conclusions
Asymmetric ICRS provided superior topographic, tomographic, and aberrometric outcomes compared to symmetric ICRS in the treatment of asymmetric keratoconus, leading to greater improvements in corneal regularity, asphericity, and cone inclination.
Keywords
Introduction
Intrastromal corneal ring segment (ICRS) implantation is a non-invasive and effective option for treating keratoconus (KC).1–4 Studies show that ICRS flattens the central cornea, shifts the apex centrally, preserves or corrects asphericity, and reduces surface irregularity. Consequently, it improves visual acuity, contact lens tolerance, and eyeglass use.4–7 Other advantages include safety, long-term stability, reversibility, and adjustability.8–10 The procedure does not compromise the visual axis or prevent future corneal transplants if needed.3,8
ICRS selection varies among nomograms, considering ectasia type, keratometry, refractive error, topographic astigmatism, corneal asphericity, pachymetry, posterior elevation, and higher-order coma aberration. Segments can be implanted alone or in pairs.5,11–15
Symmetric (standard) ICRS has uniform thickness and base width.2–4 In asymmetric keratoconus cases, these segments may not correct asymmetry effectively, as they induce uniform flattening. Asymmetric ICRS, with progressive thickness and base width, provides a more customized treatment for KC patterns such as oval phenotype, asymmetric bowtie, and asymmetric pellucid-like keratoconus.16–28
Oval phenotype KC, the most common form, features an asymmetrical pattern on the axial map, inferiorly displaced corneal apex, medium-to-high topographic astigmatism, medium-to-high keratometry, prolate or hiperprolate cornea, and “peninsula” pattern in posterior elevation map.11–15
In these cases, segments of 160° arc length are traditionally indicated, as they induce moderate changes in asphericity, keratometry, and topographic astigmatism.5,7,11–15
This study aimed to compare clinical, topographic, and tomographic changes after implantation of two different 160° ICRS models for treating oval phenotype keratoconus: symmetric (uniform thickness and base width) and asymmetric (progressive thickness and base width).
Materials and methods
This prospective, randomized clinical trial was conducted at the Goiânia Eye Institute (Brazil) from January 2019 to April 2021. It was approved by the ethics committee, adhered to the Declaration of Helsinki, and was registered under CONEP (#32212020.9.0000.5505). All procedures were performed using the manual technique by a single surgeon (B.A.N.) after written informed consent was obtained from all patients.
Randomization and stratification
Patients were stratified by age, sex, laterality, and number of segments (one/two), then randomly allocated 1:1 to two treatment groups. In bilateral cases, each eye was assigned to a different group to preserve internal validity, reduce bias, and ensure balance and comparability between groups.
Inclusion and exclusion criteria
Keratoconus stability was confirmed by serial corneal topographies over a minimum follow-up of two years. All eyes exhibited a stable topographic pattern consistent with the oval keratoconus phenotype. Inclusion criteria included BSCVA ≤0.3 LogMAR, contact lens intolerance, transparent cornea, Kmax ≤63 D, topographic astigmatism ≤5.5 D, anterior Q value between −0.5 and −1.3, and a “peninsula” pattern on posterior elevation. Minimum pachymetry was >400 µm, with ≥480 µm along the tunnel. Eyes with marked eccentricity or asymmetry were excluded. No segment exceeded 52% of corneal thickness along the tunnel path.
Exclusion criteria: prior ocular surgery (e.g., crosslinking), corneal opacities, glaucoma, cataract, retinal disease, herpetic keratitis, uveitis, autoimmune disease, uncontrolled allergy, or progressive keratoconus.
Study design and groups
A total of 64 eyes from 47 patients (23 men, 24 women) were included. Group 1 (n = 33) received symmetric ICRS; Group 2 (n = 31) received asymmetric ICRS with progressive thickness and base width. The mean age was 25.06 ± 4.82 years in Group 1 and 24.71 ± 4.66 years in Group 2. Seventeen patients underwent bilateral treatment and 30 were treated unilaterally.
In Group 1, 15 eyes received one segment and 18 received two. In group 2, 16 eyes received one segment and 15 received two. Segment selection followed the Ferrara ring standardized nomogram5,11–15 for the oval phenotype KC. (Supplementary Figure 1B)
Preoperative and follow-up evaluations
All patients underwent comprehensive ophthalmologic evaluation preoperatively and at 1, 3, 6, and 12 months postoperatively. Exams included UCVA, BSCVA, manifest and dynamic refraction, slit-lamp biomicroscopy, Goldmann tonometry, ultrasonic pachymetry, funduscopy, and corneal tomography (Pentacam®, Oculus, Germany).
KC severity was graded using the Belin ABCD classification: A (anterior curvature radius 3 mm from the thinnest point), B (posterior radius), C (thinnest pachymetry), and D (distance BSCVA). Visual acuities were converted to LogMAR for statistical purposes.
ICRS specifications
Both ICRS models featured a 5-mm optical zone and 160° arc, composed of PMMA with a prismatic triangular cross-section to minimize light scatter and mesopic halos.
Group 1 received symmetric Ferrara Rings (Ferrara Ophthalmics, Brazil)³ with a fixed base width (0.60 mm) and uniform thickness (0.15–0.25 mm). Group 2 received asymmetric AJL-Pro + segments (AJL Ophthalmic, Spain), which had progressive thickness (0.15–0.25 mm) and base width (0.60–0.80 mm) within a single segment.17–19 Segments were available in clockwise or counterclockwise configurations. The thinner and narrower end (0.15 mm thickness, 0.60 mm base) was positioned near the incision site, and the thicker and wider end (0.25 mm thickness, 0.80 mm base) was oriented toward the area of greatest ectasia. (Figure 1)
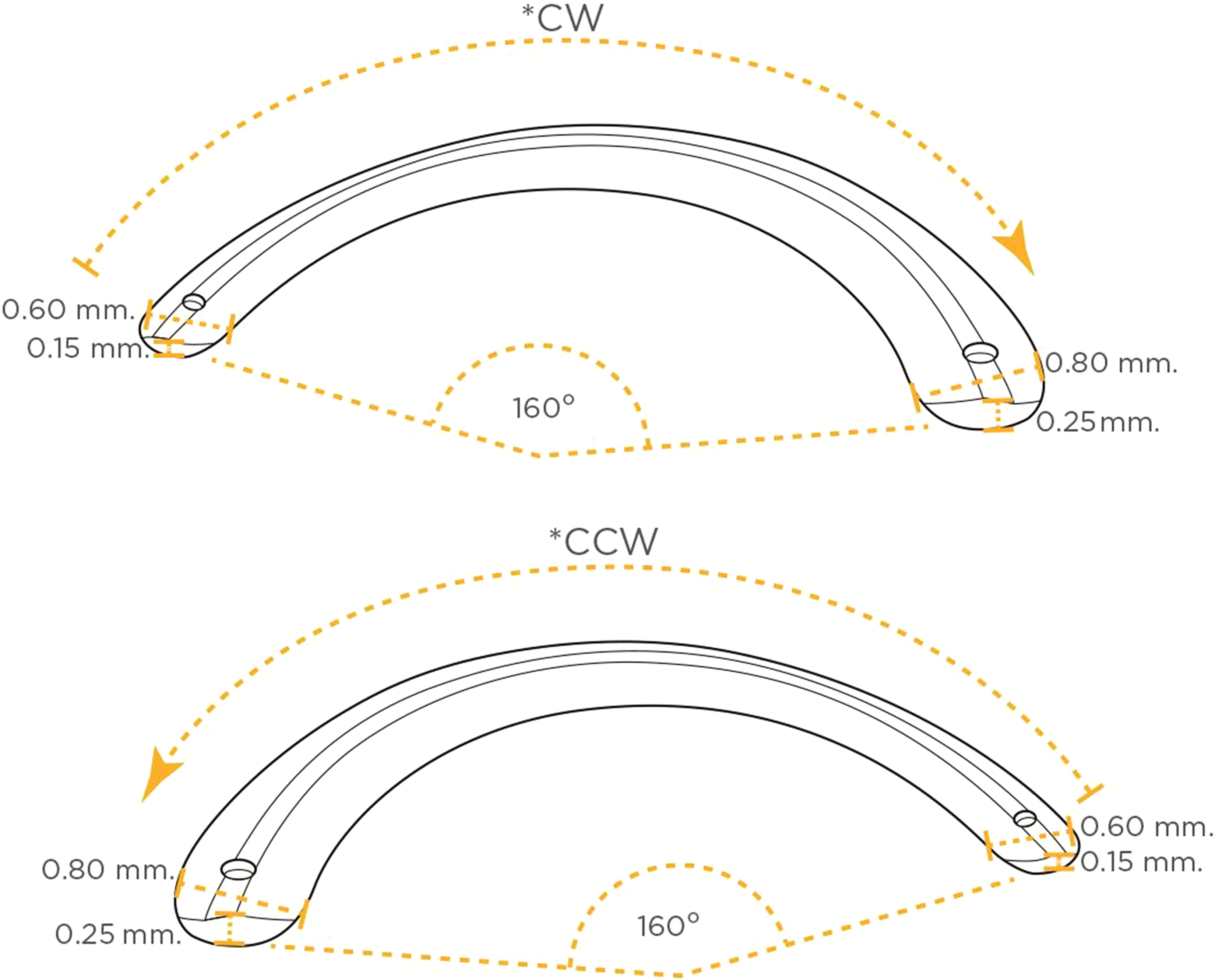
Geometry of the asymmetric 160° arc-length intrastromal corneal ring segments (ICRS), clockwise (*CW) and counterclockwise (*CCW), used in this study (AJL-Pro+, AJL Ophthalmic S.A., Vitoria, Álava, Spain).
Nomogram application
Surgical planning was based on the Ferrara Ring nomogram (Ferrara Ophthalmics, Belo Horizonte, Brazil).14,15 Segment selection considered keratoconus morphology, steepest meridian, corneal asphericity, topographic astigmatism, and minimum pachymetry along the tunnel path. Segments were positioned along the steepest meridian on axial topography. The optical goal was to achieve a postoperative Q value close to physiological levels (Q ≈ −0.23 ± 0.08), estimating ΔQ induced by each segment according to its arc length and thickness (final Q = preoperative Q – ΔQ). Alignment between topographic and coma axes is not used in this algorithm (Supplementary Figure 1A–D).
For oval keratoconus, the nomogram recommends 160° arc segments when anterior Q is less negative than −1.3, as applied in this study.5,11–15 In Group 1, segment thickness ranged from 0.15 to 0.25 mm. In Group 2, each asymmetric segment presented a progressive thickness profile within a single device.
Surgical procedure
Procedures were performed under topical anesthesia with 2% pilocarpine to induce miosis. After applying a lid speculum and antisepsis with 2.5% povidone-iodine, the visual axis was marked with a Sinskey hook and gentian violet. A square diamond knife, set to 80% stromal depth, was used to create a corneal incision on the steepest meridian. Tunnel dissection was performed with a Suarez spreader, followed by clockwise and/or counterclockwise spatulas depending on the number of segments. Segments were inserted with modified McPherson forceps and positioned using a Sinskey hook. 4
Postoperative care
A bandage contact lens was applied immediately and removed on the first postoperative day. Patients received 0.5% moxifloxacin (Vigamox®, Alcon, USA) and 0.1% dexamethasone (Maxidex®, Alcon, USA) four times daily for 10 days. Preservative-free artificial tears were recommended as needed for up to three months. All patients received counseling to strictly avoid eye rubbing.
Statistical analysis
Statistical analyses were performed using STATA 14.0 (StataCorp LP, College Station, TX, USA). Descriptive statistics included frequencies, means, and standard deviations. Multilevel mixed-effects models assessed outcomes over time. Statistical significance was defined as p < 0.05.
A post hoc sample size analysis was conducted using Cohen's d to estimate effect size. Based on 33 study variables, a two-tailed test (α = 0.05, power = 80%) yielded a minimum required sample size of 26.7 per group (95% CI: 18.5–28.7), indicating that the final sample size was statistically adequate despite variation in effect sizes.
Results
A total of 64 eyes from 47 patients (23 men, 24 women) were included. Mean age at surgery was 25.06 ± 4.82 years in group 1 and 24.71 ± 4.66 years in group 2. Group 1 included 16 right eyes (48.5%) and 17 left eyes (51.5%), while group 2 had 16 right eyes (51.6%) and 15 left eyes (48.4%). In group 1, 15 eyes (45.5%) received one ICRS and 18 eyes (54.5%) received two. Among single-segment cases, 11 eyes (33.3%) had 200 μm segments, and 4 (12.1%) had 250 μm. Among two-segment cases, 9 eyes (27.3%) received 200 μm segments, 5 (15.2%) received 150 μm, and 4 (12.1%) received one 150 μm and one 200 μm segment. Group 2 received AJL Pro + ICRS: 16 eyes (51.6%) with one segment, 15 (48.4%) with two.
There were no significant differences between groups in sex (p = 0.205), age (p = 0.8084), laterality (p = 0.81), or number of implanted segments (p = 0.81).
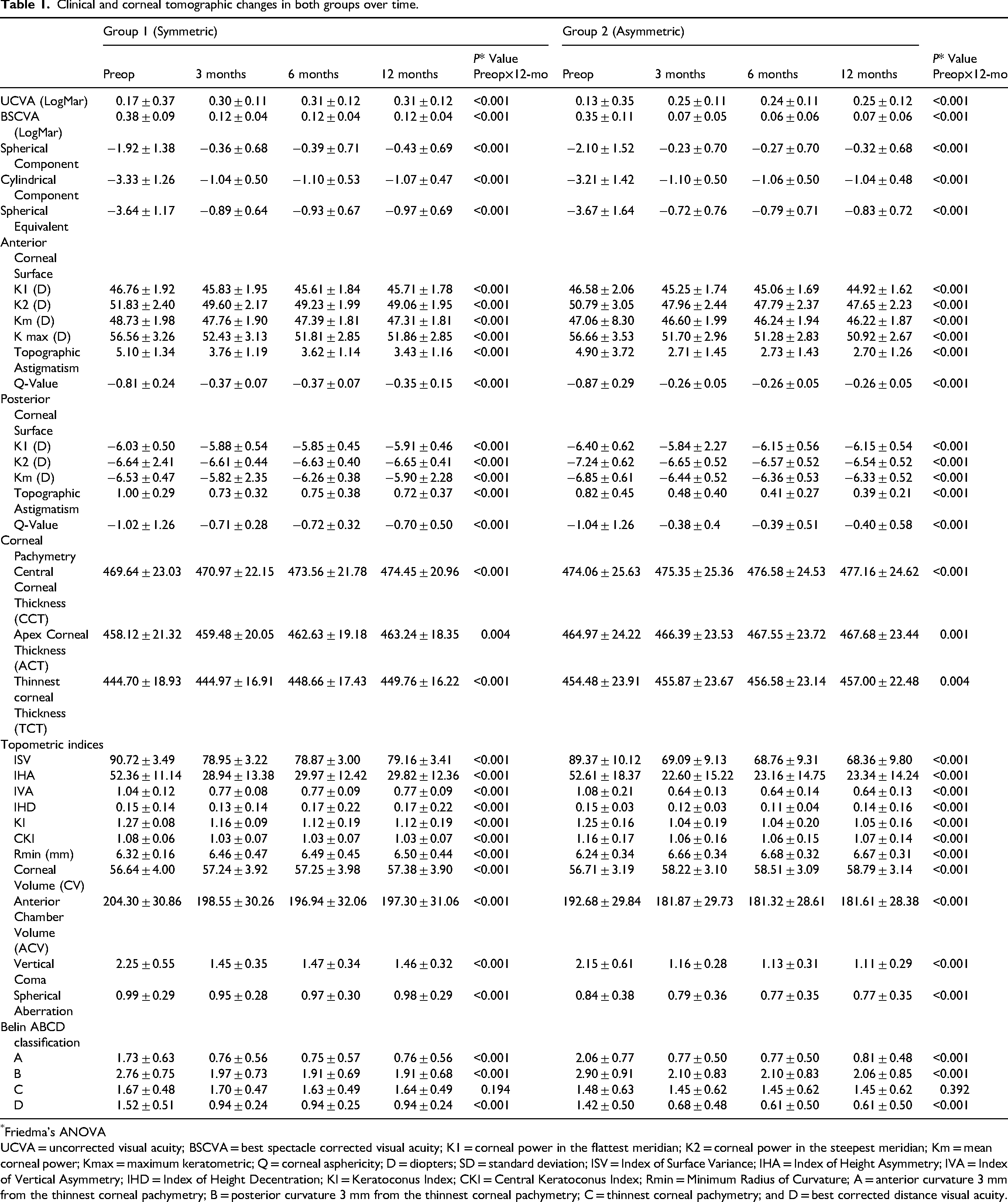
Clinical and tomographic changes at 3, 6, and 12 months postoperatively are presented in Table 1.
Clinical and corneal tomographic changes in both groups over time.
Friedma's ANOVA
UCVA = uncorrected visual acuity; BSCVA = best spectacle corrected visual acuity; K1 = corneal power in the flattest meridian; K2 = corneal power in the steepest meridian; Km = mean corneal power; Kmax = maximum keratometric; Q = corneal asphericity; D = diopters; SD = standard deviation; ISV = Index of Surface Variance; IHA = Index of Height Asymmetry; IVA = Index of Vertical Asymmetry; IHD = Index of Height Decentration; KI = Keratoconus Index; CKI = Central Keratoconus Index; Rmin = Minimum Radius of Curvature; A = anterior curvature 3 mm from the thinnest corneal pachymetry; B = posterior curvature 3 mm from the thinnest corneal pachymetry; C = thinnest corneal pachymetry; and D = best corrected distance visual acuity.
Both groups had a significant reduction in all parameters compared to baseline values (p < 0.001). The variations (delta values) in clinical and corneal tomographic parameters before and 12 months after surgery are summarized in Table 2.
Variation in clinical and tomographic parameters (delta values) in both groups, before and 12 months after surgery.
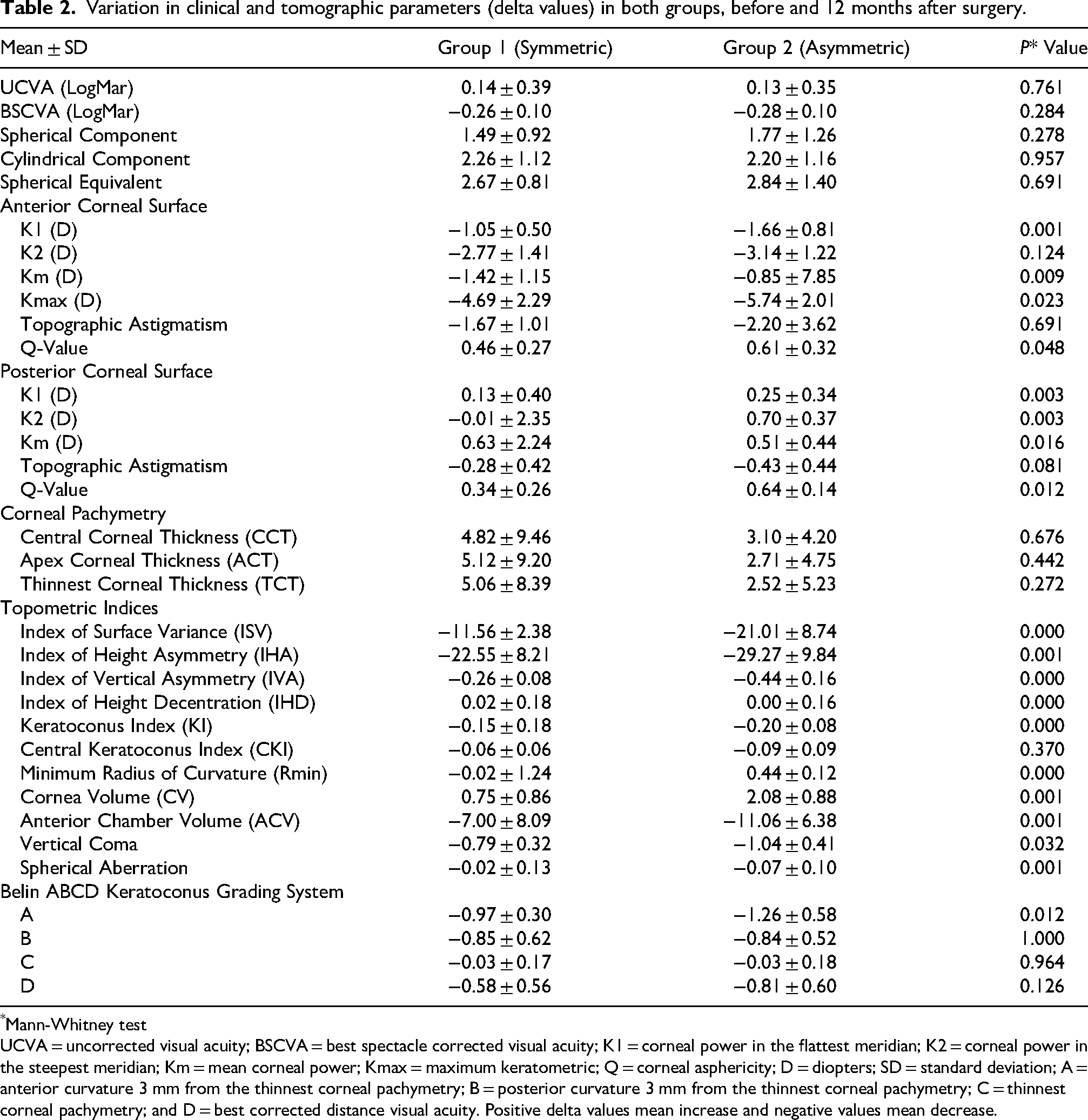
Mann-Whitney test
UCVA = uncorrected visual acuity; BSCVA = best spectacle corrected visual acuity; K1 = corneal power in the flattest meridian; K2 = corneal power in the steepest meridian; Km = mean corneal power; Kmax = maximum keratometric; Q = corneal asphericity; D = diopters; SD = standard deviation; A = anterior curvature 3 mm from the thinnest corneal pachymetry; B = posterior curvature 3 mm from the thinnest corneal pachymetry; C = thinnest corneal pachymetry; and D = best corrected distance visual acuity. Positive delta values mean increase and negative values mean decrease.
At the final postoperative visit, there were statistically significant changes in manifest sphere, cylinder, and spherical equivalent in both groups compared to preoperative values, but no significant differences between the groups (Table 2).
UCVA improvement was greater in group 2 than in group 1, though not statistically significant (p = 0.761). (Supplementary Figure S2)
Group 2 demonstrated better BSCVA throughout the follow-up period, with a statistically significant difference at 6 months (p = 0.025). (Supplementary. Figure S3)
Group 2 showed a significantly greater reduction in anterior K1, Km, Kmax (Supplementary Figure S4), and Q-value. (Supplementary Figure S5) For the posterior corneal surface, it also showed a significantly greater reduction in K1, K2, Km, and Q-value. Both groups exhibited a significant decrease in anterior and posterior topographic astigmatism compared to preoperative values, with no statistically significant differences between groups (Tables 1 and 2).
A significant increase in central corneal thickness (CCT), apex corneal thickness (ACT), and thinnest corneal thickness (TCT) was observed in both groups at 12 months (Table 1), with no differences between groups. Group 2 had a significantly greater reduction in the index of surface variance (ISV), index of height asymmetry (IHA), index of vertical asymmetry (IVA), index of height decentration (IHD), and keratoconus index (KI). No significant difference was found in the Central Keratoconus Index (CKI) between the groups (Table 2).
The minimum radius of curvature (Rmin) increased significantly more in group 2 than in group 1 throughout the follow-up, with a significant difference between groups at 12 months (Table 2). Corneal volume (CV) increased, and anterior chamber volume (ACV) decreased more significantly in group 2 than in group 1. Similarly, group 2 exhibited a greater reduction in vertical coma (Supplementary Figure S6) and spherical aberration. (Table 2)
All parameters of the Belin ABCD grading system for keratoconus classification showed a significant reduction compared to preoperative values in both groups. After 12 months, parameter A (3 mm anterior curvature of the thinnest corneal pachymetry) was significantly more reduced in group 2 than in group 1 (p = 0.012), while the other parameters remained similar between groups (p > 0.05). (Table 2)
For patients who had both eyes treated, one eye received the symmetric ICRS and the other the asymmetric ICRS.
After 12 months, group 2 showed better results than group 1, with significant differences in the spherical component, anterior corneal surface K1, Km, Kmax, and Q-Value, posterior corneal surface K2, topographic astigmatism, and Q-value. Group 2 also had significantly better outcomes in ISV, IHA, IVA, IHD, KI, CKI, Rmin, vertical coma, and spherical aberration. (Table 3)
Comparative results between the evaluated periods for each group, over time.
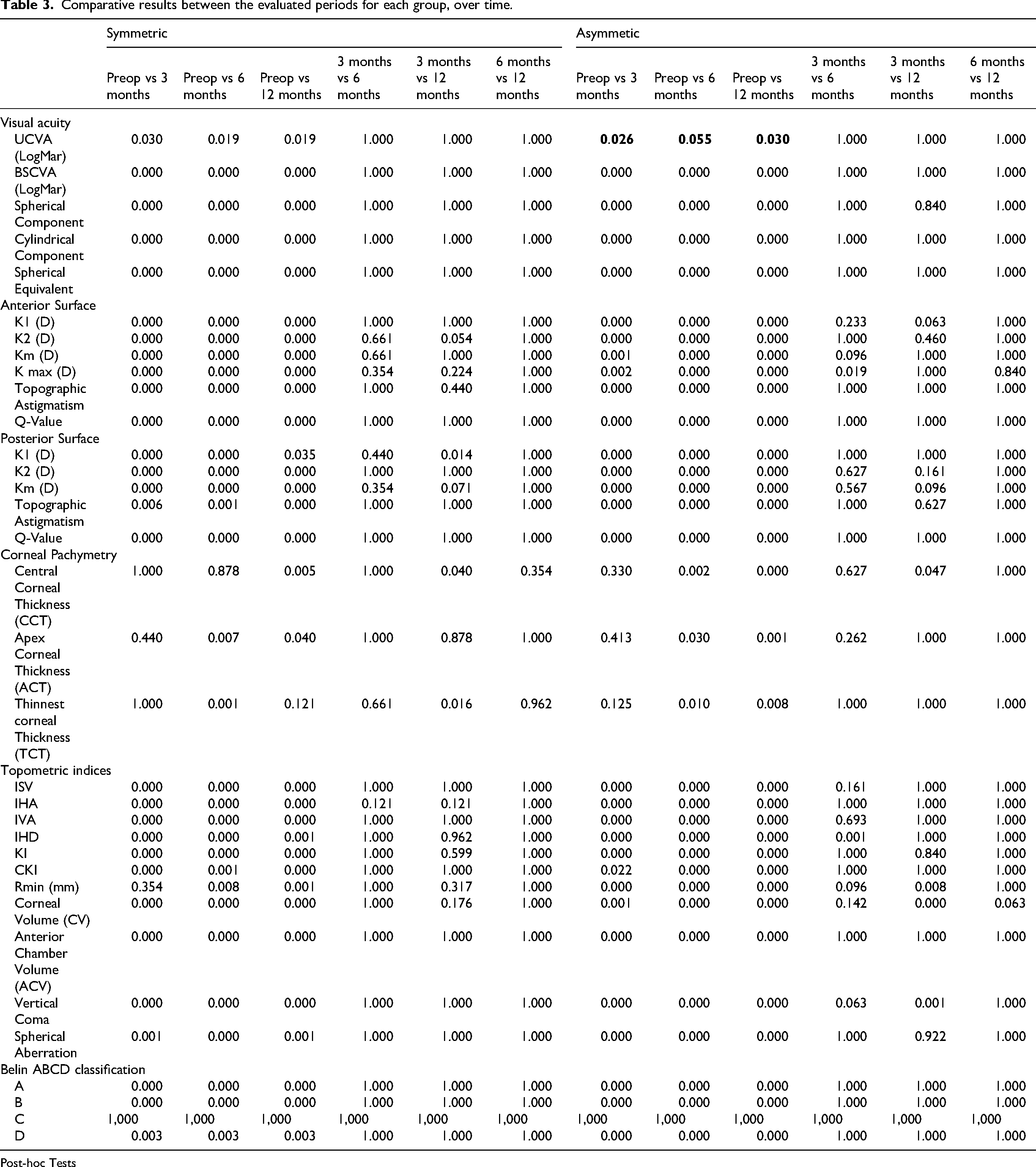
Post-hoc Tests
No intraoperative or postoperative complications were reported in this series of patients.
Discussion
The symmetric ICRS, characterized by uniform thickness and base width, has proven effective in the management of keratoconus.1–7 However, even with advancements in technology, surgical techniques, and nomogram development, results remain suboptimal in patients with asymmetric KC.17–28 This is because symmetric segments create uniform corneal flattening, while asymmetric KC requires a more localized approach—greater flattening in the more protruded regions and less in the flatter areas. 28
To address asymmetric keratoconus phenotypes, the AJL Pro + ICRS was developed, featuring progressive thickness and base width. This design allows a more customized approach for asymmetric KC phenotypes, including the oval shape, asymmetric bowtie, and pellucid-like forms. The segments gradually increase in thickness and width from one end to the other, enhancing corneal flattening at the thicker end. This asymmetry enables more precise reshaping in irregular cases, representing a significant advancement over conventional symmetric rings.17–19
In this study, we evaluated clinical, topographic, and tomographic outcomes after the implantation of two ICRS models—symmetric and asymmetric—both with a 160° arc length, in eyes diagnosed with oval-type keratoconus.
Below we present two representative cases. Both patients received bilateral ICRS implantation. In the right eyes, two symmetric AFR5 SI 160/200 segments (5 mm diameter, 160° arc, 200 μm thickness) were implanted. In the left eyes, two AJL Pro + asymmetric segments (5 mm diameter, 160° arc, progressive thickness from 150 to 250 μm and base width from 600 to 800 μm) were inserted—one oriented clockwise (AS CW 160/150/250) and the other counterclockwise (AS CCW 160/150/250).
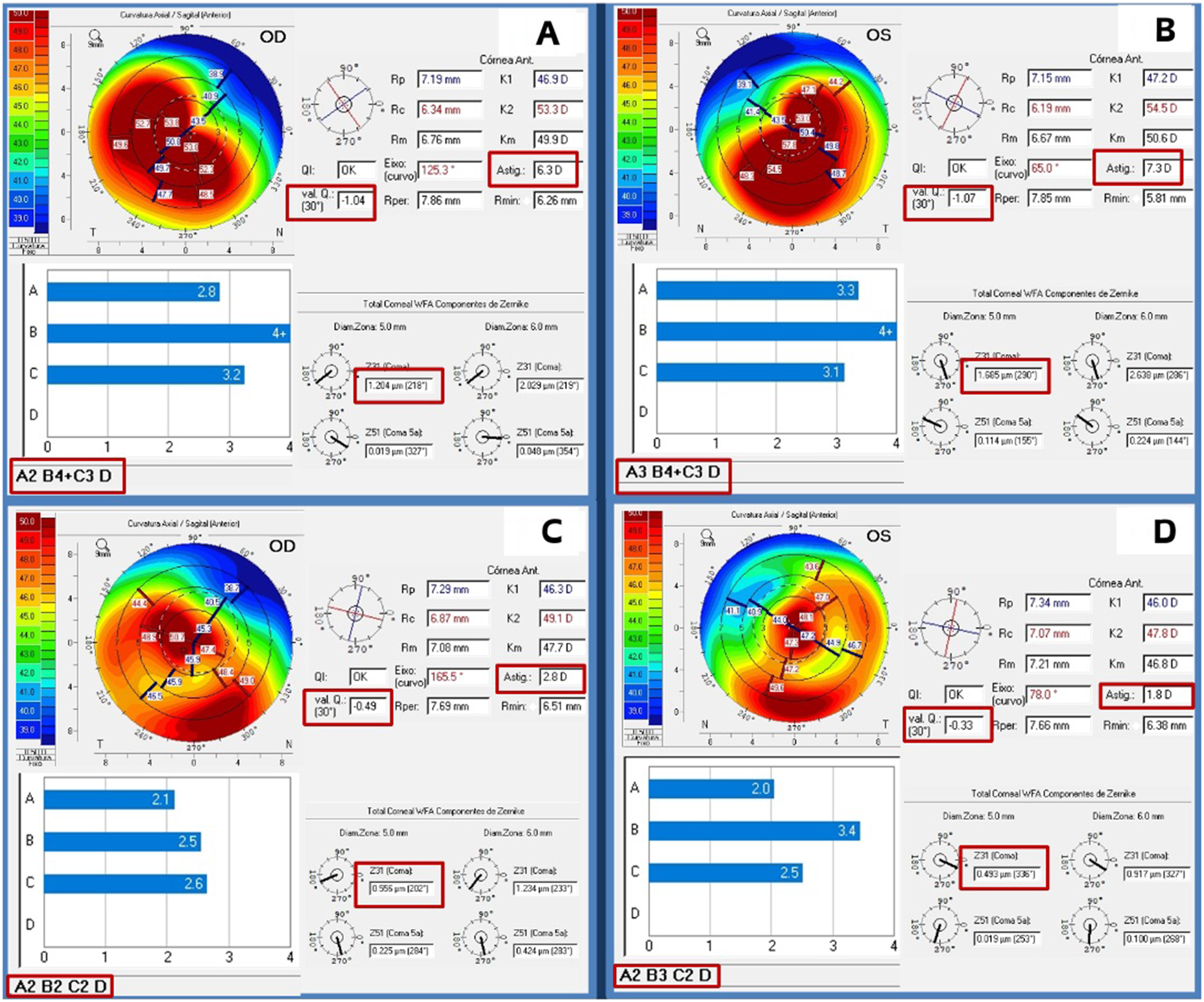
A–D. Pentacam imaging of a 25-year-old female patient.
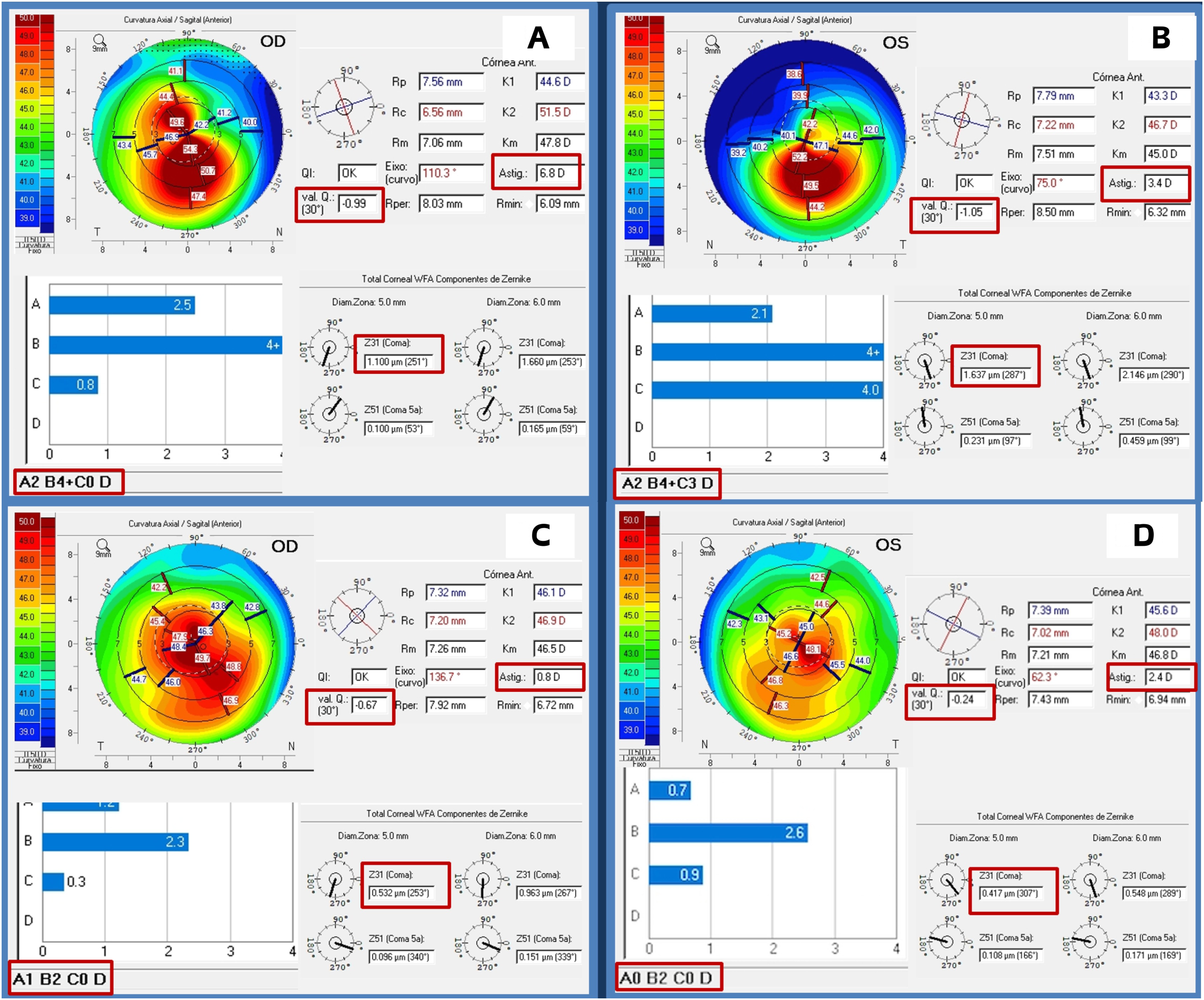
A–D. Pentacam imaging of a 30-year-old male patient.
At the 12-month follow-up, all eyes demonstrated marked improvement across all evaluated parameters, including reduced asymmetry and central corneal regularization. Notably, eyes implanted with asymmetric segments (left eyes) achieved superior outcomes in BCVA, refractive correction, keratometry, anterior corneal asphericity (Q value), and coma.
These findings align with Oteyza et al., 16 who used a finite element model to compare symmetric and asymmetric ICRS, concluding that asymmetric segments produce greater flattening in their thicker portion and result in a more uniform central optical zone. They also noted that segment thickness had a greater impact on corneal flattening than base width. Our results support these conclusions, showing improvement in both parameters by correcting asymmetry in asymmetric keratoconus.
Sardiña et al. 17 analyzed 31 eyes with “croissant” or “snowman” keratoconus patterns treated with AJL Pro + and reported anterior corneal flattening, particularly along the steepest meridian, along with improved refraction, prolate shape, and BSCVA. They also observed changes in posterior curvature and astigmatism without complications. Similarly, our group 2 (asymmetric ICRS) showed greater reductions in K1, Km, Kmax, Q value, vertical coma, and spherical aberration. Posterior K2 was significantly lower at 3 and 6 months and leveled by 12 months. While both groups improved in UCVA and BSCVA, group 2 achieved slightly better gains and significantly higher BSCVA at 6 months, suggesting greater effectiveness of asymmetric ICRS.
At one year, group 2 maintained lower values of posterior K2 and Km. Posterior astigmatism decreased in both groups, confirming the influence of ICRS on posterior corneal shape.
Kammoun et al. 18 reported that 94.3% of 35 eyes treated with AJL Pro + gained at least one line of BSCVA within three months, alongside improvements in keratometry, astigmatism, spherical aberration, and coma. Our results are comparable, with greater keratometric flattening in group 2.
Benlarbi et al. 19 also observed improved UCVA and BSCVA in 33 eyes treated with AJL Pro + at six months. About 87% achieved a spherical equivalent between +1.5D and −1.5D, and vertical coma reduction was associated with epithelial thickening along the segment track, reinforcing the visual benefits of this approach in oval keratoconus.
In our cohort, patients with asymmetric ICRS reached more physiological anterior Q values. Both groups showed increased corneal thickness at the apex, thinnest point, and center—reflecting epithelial remodeling—as described by Benlarbi et al. 19 and Coskunseven et al. 21
Group 2 also demonstrated a greater increase in total corneal volume and a larger reduction in anterior chamber volume compared to preoperative values and group 1. This may reflect the greater PMMA volume present in the thicker distal portion of asymmetric segments, which are strategically placed in steep and thin corneal areas, inducing deeper geometric changes.
Topometric indices—ISV, IVA, IHA, and CKI—showed more significant improvement in group 2, both from baseline and relative to group 1. The Rmin index also increased more in group 2, indicating more effective reduction of the cone area.
These findings suggest that asymmetric ICRS with variable thickness and base width are more effective than symmetric rings in treating asymmetric keratoconus. This design improves topographic, tomographic, and aberrometric parameters by enhancing regularity, asphericity, and cone morphology. AJL Pro + appears particularly suited for the oval phenotype, enabling targeted flattening with tailored implantation.
To our knowledge, this is the first large-scale, prospective, randomized controlled trial comparing symmetric and asymmetric ICRS in oval keratoconus with 12-month follow-up.
This study demonstrated consistent and positive results, but certain limitations must be acknowledged. Although less precise than femtosecond laser in terms of tunnel geometry and implantation depth, the manual technique has demonstrated consistent clinical effectiveness and remains a cost-effective option, corroborating findings reported by other authors.29,30
Surgical planning relied on the Ferrara Ring nomogram, which has proven clinical value. However, it lacks fixed thresholds for all parameters and does not account for axis dissociation between refractive, topographic, and coma axes. Still, the recommended implantation along the steepest meridian yielded reliable outcomes, including asymmetric cases.
This manuscript did not include subgroup comparisons between eyes receiving one or two segments due to space limitations, but these data will be presented in a forthcoming study with a larger and more stratified sample to offer deeper biomechanical insights.
Although the Ferrara nomogram has not been validated for asymmetric segments and is not universally applicable to all ring types, it remains a widely used and structured tool in clinical settings. The lack of a dedicated nomogram for asymmetric segments highlights a valuable area for future development. In this study, one nomogram was used for all cases to ensure uniform selection criteria and reduce variability, especially since all eyes shared features typical of the oval phenotype keratoconus.
All included cases were selected based on consistent morphological criteria. Although no standardized topographic classification was initially applied, this was addressed through supplementary tables detailing topographic, tomographic, and ABCD classification data. The broader lack of standardized classification systems in the literature underscores the relevance of the methodology used in this work.
Finally, although long-term data were beyond this study's scope, the 1-year follow-up results were robust and reproducible. Future studies should explore the long-term stability and durability of these promising outcomes.
Supplemental Material
sj-jpg-1-ejo-10.1177_11206721251372378 - Supplemental material for A randomized controlled trial of symmetric versus asymmetric intrastromal corneal ring segments for asymmetric keratoconus
Supplemental material, sj-jpg-1-ejo-10.1177_11206721251372378 for A randomized controlled trial of symmetric versus asymmetric intrastromal corneal ring segments for asymmetric keratoconus by Belquiz Amaral Nassaralla, Jordana Sandes Barbosa Soares and Mauro Campos in European Journal of Ophthalmology
Supplemental Material
sj-tif-2-ejo-10.1177_11206721251372378 - Supplemental material for A randomized controlled trial of symmetric versus asymmetric intrastromal corneal ring segments for asymmetric keratoconus
Supplemental material, sj-tif-2-ejo-10.1177_11206721251372378 for A randomized controlled trial of symmetric versus asymmetric intrastromal corneal ring segments for asymmetric keratoconus by Belquiz Amaral Nassaralla, Jordana Sandes Barbosa Soares and Mauro Campos in European Journal of Ophthalmology
Supplemental Material
sj-tif-3-ejo-10.1177_11206721251372378 - Supplemental material for A randomized controlled trial of symmetric versus asymmetric intrastromal corneal ring segments for asymmetric keratoconus
Supplemental material, sj-tif-3-ejo-10.1177_11206721251372378 for A randomized controlled trial of symmetric versus asymmetric intrastromal corneal ring segments for asymmetric keratoconus by Belquiz Amaral Nassaralla, Jordana Sandes Barbosa Soares and Mauro Campos in European Journal of Ophthalmology
Supplemental Material
sj-tif-4-ejo-10.1177_11206721251372378 - Supplemental material for A randomized controlled trial of symmetric versus asymmetric intrastromal corneal ring segments for asymmetric keratoconus
Supplemental material, sj-tif-4-ejo-10.1177_11206721251372378 for A randomized controlled trial of symmetric versus asymmetric intrastromal corneal ring segments for asymmetric keratoconus by Belquiz Amaral Nassaralla, Jordana Sandes Barbosa Soares and Mauro Campos in European Journal of Ophthalmology
Supplemental Material
sj-tif-5-ejo-10.1177_11206721251372378 - Supplemental material for A randomized controlled trial of symmetric versus asymmetric intrastromal corneal ring segments for asymmetric keratoconus
Supplemental material, sj-tif-5-ejo-10.1177_11206721251372378 for A randomized controlled trial of symmetric versus asymmetric intrastromal corneal ring segments for asymmetric keratoconus by Belquiz Amaral Nassaralla, Jordana Sandes Barbosa Soares and Mauro Campos in European Journal of Ophthalmology
Supplemental Material
sj-tif-6-ejo-10.1177_11206721251372378 - Supplemental material for A randomized controlled trial of symmetric versus asymmetric intrastromal corneal ring segments for asymmetric keratoconus
Supplemental material, sj-tif-6-ejo-10.1177_11206721251372378 for A randomized controlled trial of symmetric versus asymmetric intrastromal corneal ring segments for asymmetric keratoconus by Belquiz Amaral Nassaralla, Jordana Sandes Barbosa Soares and Mauro Campos in European Journal of Ophthalmology
Footnotes
Ethical considerations
This study was approved by the National Research Ethics Commission (CONEP) under registration number 32212020.9.0000.5505. It was conducted following approval by the institutional ethics committee and in accordance with the tenets of the Declaration of Helsinki.
Consent to participate
Written informed consent was obtained from all participants prior to their inclusion in the study. All participants provided written informed consent after receiving a detailed explanation of the procedures, risks, and potential benefits.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Data availability statement
Anonymized data from this study are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.