
Abstract
Purpose
To present the clinical and multimodal imaging features of three patients diagnosed with stellate multiform amelanotic choroidopathy (SMACH), a recently described, rare chorioretinal entity.
Methods
Case series.
Results
All patients, aged 5, 10, and 38 years, presented with unilateral, yellowish choroidal lesions extending from the fovea toward the temporal macula. Multimodal imaging was used for diagnosis. Structural disorganization of the subfoveal choroid with irregular, undulating hyperreflective alterations of the retinal pigment epithelium/Bruch's membrane complex with focal protrusions was noted in all patients, while subretinal fluid (SRF) was present in two patients at presentation on optical coherence tomography (OCT). No patient had systemic findings. The first and the third cases received intravitreal bevacizumab injections and the SRF persisted with fluctuations in both patients. In the second case, although there was no SRF initially, it occurred with fluctuations during follow-up. Throughout the follow-up periods, visual acuities remained stable in all patients without any additional treatment.
Conclusion
SMACH should be considered in the differential diagnosis of choroidal structural disorganization, particularly in young patients. Notably, one patient was 5 years old, which represents the youngest age reported to date. Multimodal imaging modalities are essential for the recognition of the disease and a confirmed diagnosis of SMACH may prevent unnecessary treatments such as intravitreal injections and photodynamic therapy.
Introduction
Multimodal imaging continues to enhance our understanding of retinal diseases. Findings that were previously interpreted as indicators of “established” conditions have now been shown to reflect distinct pathologies.1,2 Observations once considered incidental are now recognized as complex manifestations of specific pathologies.3,4 Furthermore, perceptions of recently identified conditions are evolving and remain subject to revision.
Stellate multiform amelanotic choroidopathy (SMACH) is a recently redefined clinical entity. It was initially described under the term serous maculopathy associated with nonspecific choroidopathy, characterized by subretinal fluid (SRF), retinal pigment epithelium (RPE) alterations, and choroidal thickening. However, subsequent clinical observations demonstrated that serous maculopathy was not a universal finding. In contrast, a distinctive dendriform (stellate) choroidal lesion was consistently observed in all reported cases. To more accurately capture these hallmark features—stellate, multiform, amelanotic choroidal lesions—the entity was reclassified as “stellate multiform amelanotic choroidopathy,” while preserving the SMACH acronym. This change aimed both to prevent misclassification and to emphasize the most consistent and defining multimodal imaging characteristics. The current description highlights unilateral, yellowish dendriform amelanotic choroidal lesions with stellate finger-like projections, associated RPE hypo-/hyperpigmentary changes, variable SRF, absence of intraocular inflammation, and long-term morphological stability as the core diagnostic features.5–7
However, the multimodal imaging features of SMACH frequently overlap with those of other chorioretinal disorders, including central serous chorioretinopathy (CSC), inflammatory diseases such as Vogt–Koyanagi–Harada (VKH) disease, hereditary macular dystrophies, and even amelanotic choroidal tumors.8–10 This considerable diagnostic overlap highlights the clinical challenge of distinguishing SMACH from more common conditions and underscores the importance of accurate classification in preventing misdiagnosis and unnecessary interventions. A thorough synthesis of clinical and multimodal imaging features is therefore essential to differentiate SMACH and optimize therapeutic decision-making.
Given the limited number of reports and the ongoing uncertainty surrounding its clinical spectrum, the present article aims to describe the clinical course and multimodal imaging findings of three patients with SMACH, including a notably young patient. By providing detailed follow-up and differential diagnostic considerations, this report seeks to broaden current knowledge and increase awareness of this rare condition.
Case reports
Case 1
A 5-year-old male patient was referred for further evaluation of his right eye. The patient had a history of hyperopic anisometropia. He had been wearing corrective glasses since the age of one and undergoing occlusion therapy for the right eye. He was a carrier of thalassemia and had no relevant family history. On examination, he had alternating esotropia. The best corrected visual acuity (BCVA) was 20/32 in the right eye and 20/63 in the left eye. Anterior segment examinations were normal in both eyes. The right eye showed a subfoveally located, yellowish-orange choroidal lesion extending superotemporally with finger-like projections beneath nonspecific hypopigmentary and hyperpigmentary changes of the RPE (Figure 1A). Optical coherence tomography (OCT) showed prominent disorganization of the choroid below SRF and anterior protrusion of RPE and Bruch membrane complex (Figure 2A). No signs of macular neovascularization (MNV) were present in OCT-angiography (OCTA) and fluorescein angiography (FFA) (Figure 1C). Indocyanine green angiography (ICGA) revealed a well-demarcated hypofluorescent lesion centered at the macula, exhibiting a dendriform, stellate configuration (Figure 3). En face OCT imaging demonstrated a well-defined hyporeflective stellate lesion centered at the macula, with multiple finger-like extensions. Irregular hyporeflective foveal spots were evident, corresponding to the hypocyanescent areas on ICGA (Figure 4A). The suspected initial diagnoses were CSC, Best vitelliform macular dystrophy and choroidal osteoma. The electrooculogram was normal in both eyes, and BEST1 gene analysis revealed no pathogenic variants, excluding Best vitelliform macular dystrophy. Ocular ultrasonography and orbital computed tomography showed no evidence of choroidal osteoma. Since CSC was initially suspected and verteporfin was not available for photodynamic therapy, a single intravitreal bevacizumab injection was administered as an alternative treatment. However, because there was no reduction in SRF and multimodal imaging findings confirmed the diagnosis of SMACH, further injections were not continued. To the best of our knowledge, this is the youngest case of SMACH to be reported in the literature. Throughout the follow-up, a single intravitreal injection of bevacizumab was given; however, no reduction in SRF was observed in the first month. During the four-year follow-up period, SRF persisted with fluctuations, the underlying fibrous-like choroidal lesion did not change, and visual acuity remained stable.
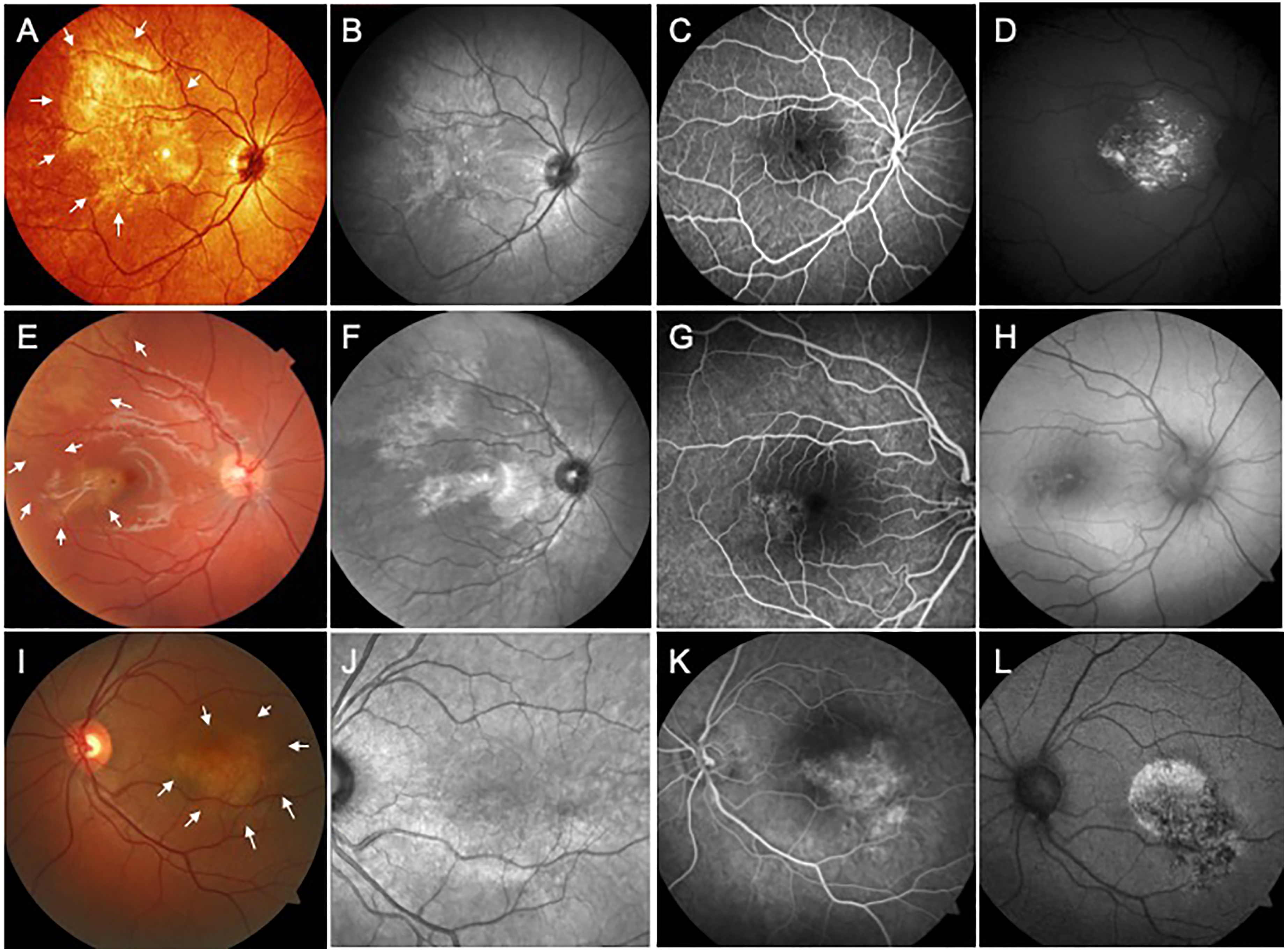
Multimodal imaging findings of the three cases. A-D. Case 1. A. Multicolor fundus imaging of the right eye demonstrates a yellowish, dendriform choroidal lesion extending from the fovea to the supratemporal macula. Finger-like extensions are visible along the inferior border of the lesion (white arrows). B. In the near-infrared reflectance (NIR), the lesion appears hyperreflective with characteristic finger-like projections extending radially. C. The late phase of fluorescein angiography (FA) reveals granular hypofluorescence and hyperfluorescence associated with retinal pigment epithelium (RPE) changes, particularly in the inferior parafoveal area. D. Blue-light fundus autofluorescence (FAF) image reveals scattered hyperautofluorescence in the fovea linked to subretinal fluid. E-H. Case 2. E. Fundus photograph shows a hypopigmented lesion temporally adjacent to the fovea that resembles torpedo maculopathy. Note that the lesion extends superior temporal to the macula (white arrows). F. The lesion appears hyperreflective in the NIR, with distinctive radial finger-like projections. Also, the superior temporal extension of the lesion is more apparent in this image. G. Granular hypofluoresce and hyperfluorescence patterns are seen in the inferotemporal parafoveal region during the late phase of FA, which correspond to RPE alterations. H. Blue-light FAF shows speckled hyperautofluorescence co-localizing with RPE mottling. I-L. Case 3. I. The fundus photograph demonstrates a yellowish, dendriform choroidal lesion located inferior to the fovea (white arrows). J. NIR imaging shows the hyperreflective lesion located in the inferior part of the macula, along the fovea and inferior major vascular arcade. K. The late phase of FA demonstrates granular hypofluorescence and hyperfluorescence associated with RPE alterations. L. Blue-light FAF reveals speckled hyperautofluorescence in the fovea associated with subretinal fluid. Note the hypoautofluorescent regions due to RPE atrophy.

Optical coherence tomography images of all three cases. A-B. Case 1. A. Spectral-domain optical coherence tomography (OCT) B-scan through the fovea reveals a hyperreflective fibrous-like lesion of the choroid (white arrows), causing a slight anterior protrusion of the RPE and subretinal fluid. B. Four years later, a follow-up spectral-domain OCT B-scan was conducted. Note the ongoing RPE modification in the subretinal fluid. The choroidal lesion is hyperreflective and located in the inner choroid. The choroidopathy appears to be non-progressive. C-D. Case 2. C: The inner choroid exhibits hyperreflective fibrous-like alterations on the OCT B-scan (white arrows), which causes anterior protrusion and RPE modification. No SRF was observed in Case 2 at baseline. D. The choroidal lesion has been stable for five years. Note the subretinal fluid in the OCT B-scan. E-F. Case 3. E. In OCT, fibrous-like choroidal lesion in the inner choroid and subretinal fluid is observed (white arrows). F. SRF persisted with decreasing during the six-month follow-up period.
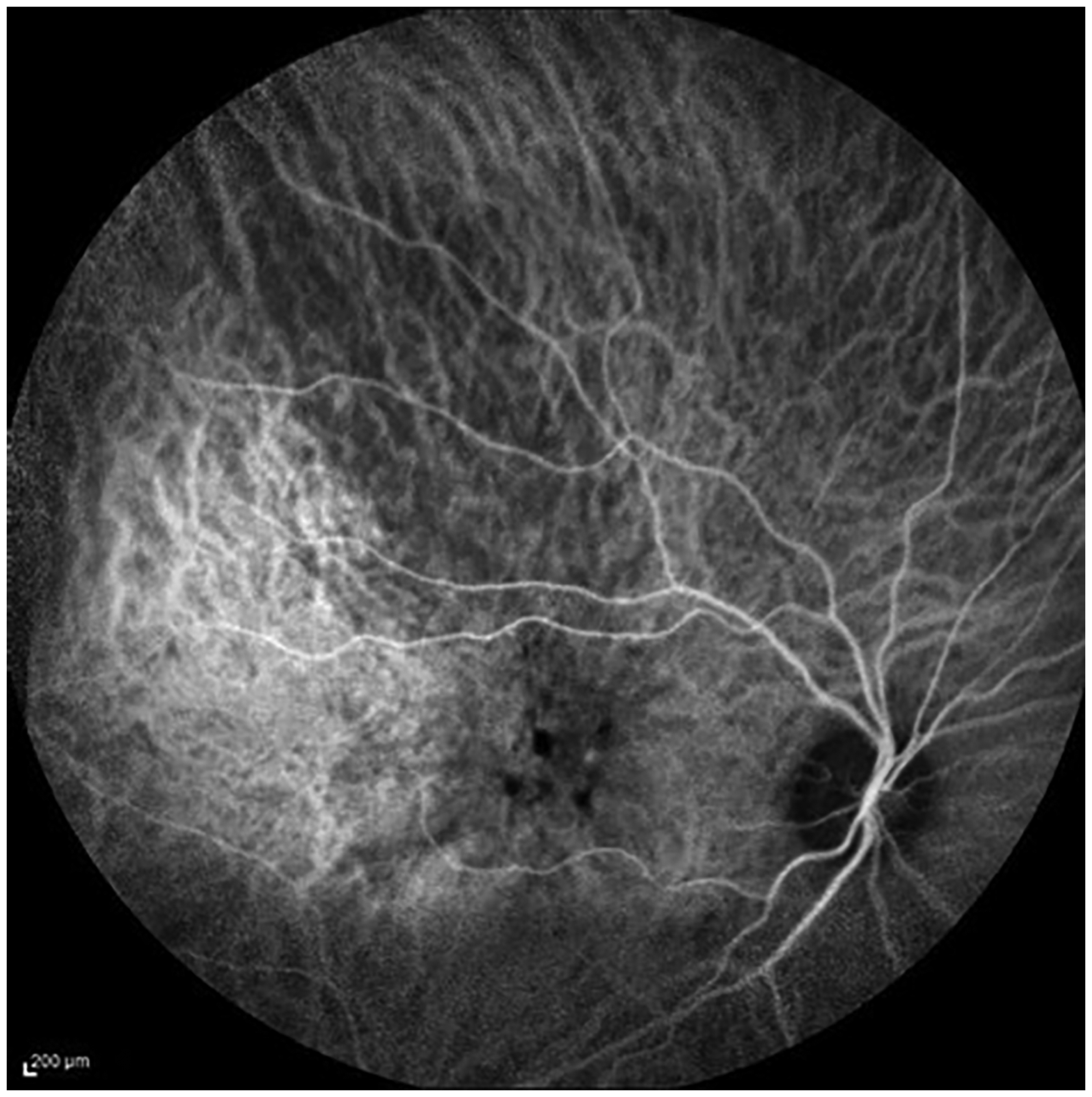
Case 1, indocyanine green angiography (ICGA) revealed a well-demarcated hypofluorescent lesion centered at the macula, exhibiting a dendriform, stellate configuration. The lesion demonstrated multiple finger-like hypofluorescent extensions radiating outward, consistent with a branching pattern. Within the foveal area, several irregular, dark hypofluorescent spots were observed, representing the most prominent component of the lesion. Surrounding the lesion, the choroidal vasculature appeared relatively preserved, although a masking effect was evident overlying the hypofluorescent areas. No hyperfluorescent leakage, hot spots, or signs of active intraocular inflammation were detected throughout the angiographic sequence.
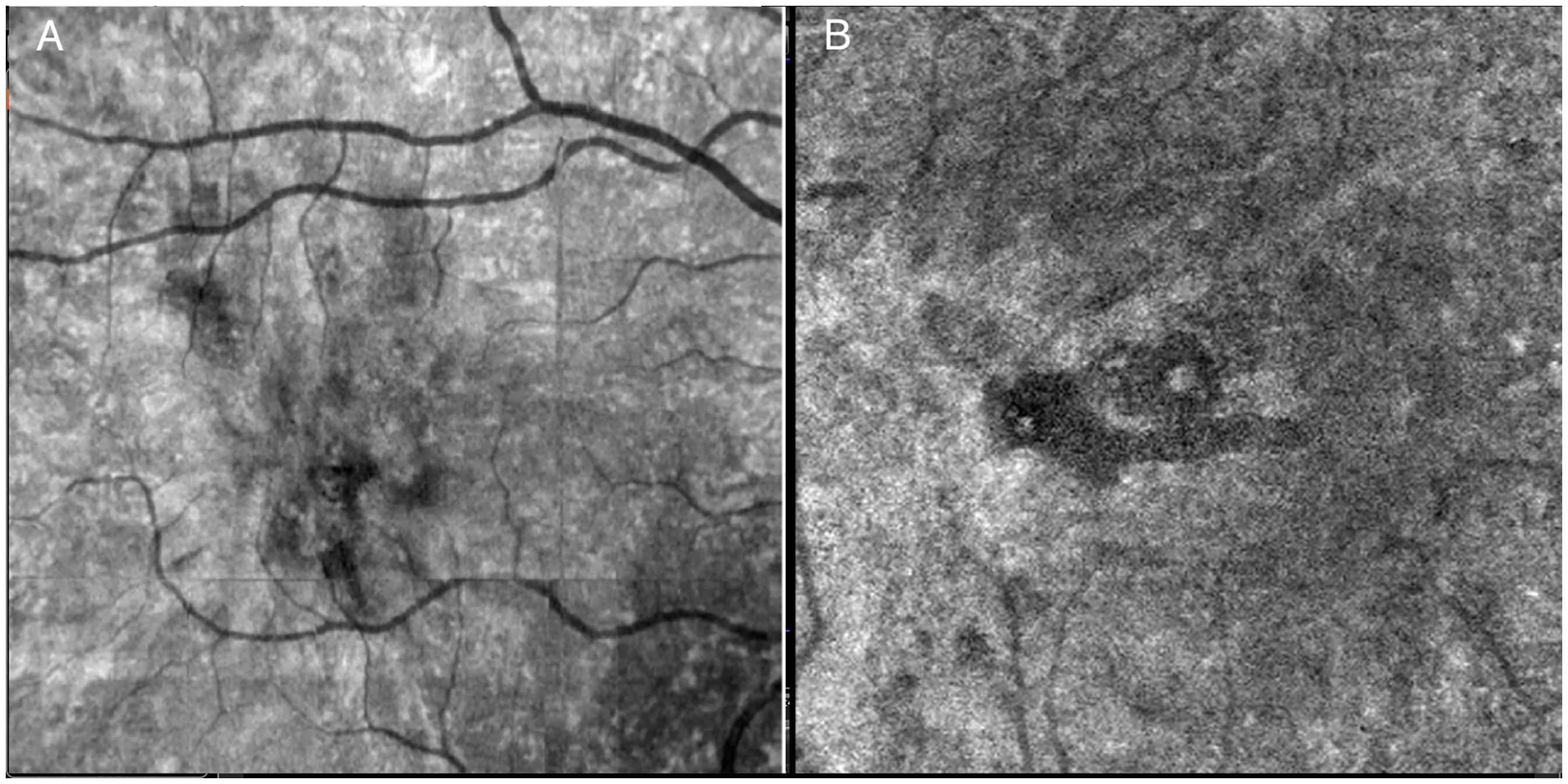
A. Case 1, en face optical coherence tomography (OCT) imaging demonstrated a well-defined hyporeflective stellate lesion centered at the macula, with multiple finger-like extensions. B. Case 2 En face OCT demonstrated a localized, irregularly bordered hyporeflective lesion at the macula, with heterogeneous internal reflectivity and indistinct peripheral extensions, suggestive of focal choroidal structural alteration.
Case 2
A 10-year-old female, initially diagnosed with torpedo maculopathy, was referred for a second opinion. BCVA was 20/20 bilaterally, with unremarkable anterior segment findings. Fundus examination of the right eye revealed a hypopigmented lesion temporal to the fovea, with subfoveal extension featuring a characteristic narrow apex directed toward the fovea. However, the lesion atypically exhibited dendriform peripheral extensions rather than the classic temporal wedge-shaped tail 10 and this feature corresponded to the stellate nature of SMACH (Figure 1E). Near-infrared reflectance (NIR) imaging further demonstrated superior extension of the lesion, exceeding its ophthalmoscopically apparent dimensions (Figure 1F). OCT showed hyperreflective fibrous-like changes in the inner choroid, and partial preservation of the overlying ellipsoid and interdigitation zones. There was an anterior protrusion of RPE and Bruch membrane complex. While there was no SRF at presentation, some subretinal fluid was present at the end of 5-year follow-up (Figure 2C and 2D). No evidence of MNV was detected on angiography (Figure 1G). En face OCT demonstrated a localized, irregularly bordered hyporeflective lesion at the macula, with heterogeneous internal reflectivity and indistinct peripheral extensions, suggestive of focal choroidal structural alteration (Figure 4B). Systemic and radiological evaluations were unremarkable. Throughout the five-year follow-up period, the patient maintained stable BCVA without any treatment and SRF showed fluctuations. The underlying choroidal disorganization remained unchanged.
Case 3
A 38-year-old emmetropic male was referred with an initial diagnosis of choroidal osteoma in his left eye. BCVA was 20/20 in the right eye and 20/100 in the left eye. The patient reported incidentally noticing decreased vision in his left eye several years prior to presentation. Anterior segment examinations were normal in both eyes. Funduscopy of the right eye was unremarkable. However, in the left eye, he had a juxtafoveal amelanotic lesion in the posterior pole. Hyperreflective finger-like projections of the lesion were somewhat unclear but extended radially in a stellate configuration both superiorly and temporally (Figure 1I). Fundus autofluorescence image showed hypoautofluorescent and hyperautofluorescent speckled areas co-localized with the choroidal lesion (Figure 1L). OCT-scan through the fovea showed SRF with disruption of the ellipsoid and interdigitation zones. The underlying choroid showed hyperreflective fibrous-like changes in the inner choroid and there was an outward protrusion of the posterior curvature of the RPE and Bruch membrane complex next to the choroidal lesion. Notably, the outer choroidal vasculature beneath the lesion appeared preserved. (Figure 2E). Ocular ultrasonography and computed tomography ruled out choroidal osteoma, challenging the initial diagnosis. In this case, three monthly intravitreal bevacizumab injections were administered due to the presence of subretinal fluid involving the fovea, decreased visual acuity, and a flat irregular pigment epithelial detachment. Following the injections, the subretinal fluid decreased but persisted. In addition, multimodal imaging findings confirmed the diagnosis of SMACH; therefore, intravitreal injections were not continued. At the end of the six-month follow-up, visual acuity was 20/63, and SRF persisted with decreasing.
Discussion
In this case series of three patients with SMACH, we observed fluctuating subretinal fluid despite stable visual acuity during follow-up. Notably, one of the patients was 5 years old, representing the youngest case reported to date. Two patients demonstrated subfoveal involvement, a feature less frequently described in previous reports, which may account for the persistence of fluid. These findings highlight the diagnostic challenges of SMACH, underscore the importance of multimodal imaging for accurate recognition, and emphasize the potential to avoid unnecessary interventions such as intravitreal anti-VEGF injections or photodynamic therapy.
SMACH presents as a unilateral, yellowish-orange choroidal lesion with distinctive dendriform morphology, typically located in the posterior pole.5–7 The lesion exhibits variable dimensions and is invariably characterized by radially oriented, finger-like projections arranged in a stellate configuration. These pathological changes occur in conjunction with nonspecific hypopigmentary and hyperpigmentary alterations of the RPE. While SRF accumulation is frequently observed, it is not an absolute diagnostic requirement. Subfoveal involvement appears to be less frequently described in the literature, which may explain the persistence of subretinal fluid in our cases. Notably, all cases demonstrate an absence of active intraocular inflammation. 6
Cross-sectional OCT reveals consistent hyperreflective, fibrous-like changes within the inner choroid. The lesions typically lack optical shadowing, with posterior hypertransmission evident in cases exhibiting disruption of the RPE/Bruch's membrane complex. Importantly, the underlying outer choroidal vasculature and choroidal-scleral junction remain clearly visible in all instances. The imaging profile excludes pachychoroid-associated features, with no evidence of dilated Haller layer vessels (pachyvessels) or choriocapillaris compression. 7 Characteristic secondary changes include structural irregularities, thickening, and anterior protrusion of the RPE/Bruch's membrane complex.6,7
Multimodal imaging provides distinctive diagnostic features. OCT angiography demonstrates subtle choriocapillaris flow deficits precisely corresponding to the lesion location, without evidence of MNV. En face structural OCT and near-infrared reflectance imaging clearly depict the hyperreflective stellate projections. Fluorescein angiography almost always reveals granular hypofluorescence and hyperfluorescence patterns mirroring the RPE mottling, while indocyanine green angiography shows delayed filling during early phases and hypofluorescence in late stages, particularly in the radiating projections. In FA, late focal staining and focal leakage were also reported in some cases. 7
The clinical course of SMACH demonstrates remarkable stability, with lesions maintaining consistent dimensions and configuration throughout follow-up periods. Visual acuity typically remains preserved, though cases may exhibit spontaneous fluctuations in SRF accumulation. Therapeutic interventions, including photodynamic therapy and intravitreal anti-VEGF administration, have shown no appreciable effect on fluid resolution or lesion characteristics.5–7
The differential diagnosis of SMACH requires careful consideration of several chorioretinal conditions.8–10 The absence of pachychoroid features distinguishes it from diseases within that spectrum. In our series, Cases 1 and 3 demonstrated relatively thick choroids. However, pachychoroid spectrum disorders are not defined solely by increased choroidal thickness. Their diagnosis requires additional features such as dilated Haller layer vessels (pachyvessels), choriocapillaris compression, and other pachychoroid-associated changes. None of these features were observed in our patients, supporting the diagnosis of SMACH rather than a pachychoroid spectrum disease. Unlike placoid chorioretinitis, SMACH shows no inflammatory activity or progressive expansion. Its unilateral presentation and lack of familial association differentiate it from inherited retinal disorders, while its stable nature contrasts with the progressive growth observed in choroidal tumors.6,7
The early detection and non-progressive behavior of SMACH lesions suggest a likely congenital origin, potentially representing a form of choroidal dysgenesis. This hypothesis is supported by our case series, which includes the youngest reported instance of this condition. The fibrotic thickening of the inner choroid may elevate hydrostatic pressure, disrupting the normal pressure gradient across Bruch's membrane. Additionally, structural alterations in the RPE/Bruch's membrane complex could impair both the outer blood-retinal barrier function and the fluid transport capacity of the RPE. This dual dysfunction may account for the persistence of SRF despite the absence of focal leakage points on angiography. Notably, the lack of inflammatory markers or vascular leakage suggests that fluid accumulation primarily results from mechanical and transport deficiencies, rather than exudative or inflammatory processes.6,7
This case series describes the clinical and multimodal imaging findings of three SMACH cases and compiles current data from the literature. All three cases have fluctuated SRF in some part of follow up periods, which could be mistaken for several of the aforementioned conditions; however, comprehensive multimodal imaging allowed definitive differentiation through the identification of stellate projections and localized fibrous choroidal architecture. While it is limited by a small sample size and the absence of long-term follow-up, it remains valuable as it highlights this rare and newly described condition, and documents its occurrence in younger patients than previously recognized (Table 1).
Demographic and clinical features of SMACH cases.
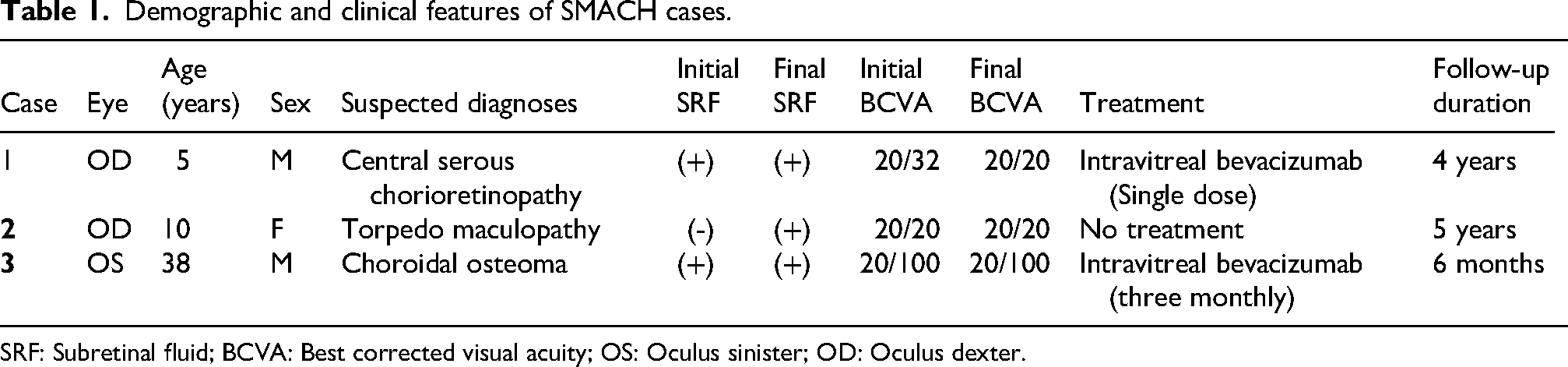
SRF: Subretinal fluid; BCVA: Best corrected visual acuity; OS: Oculus sinister; OD: Oculus dexter.
Collectively, these findings demonstrate that SMACH, originally classified as nonspecific choroidopathy with serous maculopathy, represents a broader disease spectrum with significant occult pathological features that extend beyond its initial phenotypic description. Clinicians should maintain a high index of suspicion for SMACH to avoid unnecessary diagnostic procedures and inappropriate therapeutic interventions. The use of various multimodal imaging techniques may facilitate the differentiation of SMACH from phenotypically similar conditions.
Footnotes
Informed consent
Written informed consent was obtained by authors from the third case and the parents of the first and second cases prior to submission of the case report.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.