
Abstract
Purpose
Ocular involvement is exceedingly uncommon, and to date, no conjunctival hibernoma has been reported in humans. We present the first such case in a patient with von Hippel–Lindau (VHL) syndrome.
Case report
A 32-year-old woman with genetically confirmed type 1 VHL disease presented with a long-standing, progressively enlarging, painless subconjunctival mass in her only functional eye. Systemic history included multiple cerebellar hemangioblastomas, bilateral nephrectomy for renal cell carcinoma, and an endolymphatic sac tumor. Ophthalmic examination revealed a firm, elevated, subepithelial nodular lesion on the bulbar conjunctiva of the left eye, partially prolapsing beyond the palpebral fissure. The lesion was non-tender, non-ulcerated, and showed no surface inflammation. The eye had phthisis bulbi and residual retinal hemangioblastoma. Orbital magnetic resonance imaging demonstrated a 1.2 × 0.9 × 0.7 cm homogeneous, well-circumscribed lesion, hyperintense on T2-weighted fat-suppressed images, confined to the conjunctiva without scleral, orbital, or bony involvement. Surgical excision revealed a cream-gray, lobulated mass composed of multivacuolated eosinophilic cells with granular cytoplasm. Immunohistochemistry showed strong S-100 positivity and low Ki-67, consistent with hibernoma. Despite a positive deep margin, the patient declined further surgery; no recurrence was observed at three months.
Conclusion
This is the first documented case of conjunctival hibernoma in humans and the second reported association with VHL. Conjunctival hibernoma should be considered in the differential diagnosis of vascular conjunctival lesions, particularly in patients with VHL.
Keywords
Introduction
Hibernomas are rare benign tumors composed of brown adipose tissue, typically arising in the thigh, back, or neck. 1 Ocular involvement is exceedingly rare, and no prior case of conjunctival hibernoma has been reported in humans. We describe the first such case, occurring as a subconjunctival lesion confined to the bulbar conjunctiva in a patient with von Hippel–Lindau (VHL) syndrome.
Case report
All procedures adhered to the tenets of the Declaration of Helsinki. Written informed consent was obtained from the patient for clinical care, use of de-identified data, and publication of clinical images. Data were collected, handled, and reported in a manner compliant with the Health Insurance Portability and Accountability Act Privacy Rule; all patient identifiers were removed prior to analysis and manuscript preparation. A 32-year-old female patient with a genetically confirmed diagnosis of VHL disease presented with a long-standing, progressively enlarging, painless mass on the conjunctiva of her left eye. Her clinical phenotype was consistent with type 1 VHL, and her systemic history included multiple neurosurgical procedures for cerebellar hemangioblastomas, bilateral nephrectomy surgeries for clear cell renal cell carcinoma (RCC), and a right-sided endolymphatic sac tumor. She had never received chemotherapy or radiotherapy. A strong family history of RCC was present, including her father and multiple paternal cousins. Ocular history was significant for multiple retinal hemangioblastomas in both eyes, which required repeated laser and surgical treatments. The right eye had been enucleated due to intractable secondary glaucoma following extensive retinal hemangioblastoma involvement. The remaining left eye had poor visual acuity and a history of multiple glaucoma surgeries.
On ophthalmologic examination, a firm, elevated, subepithelial nodular lesion was noted on the bulbar conjunctiva of the left eye, partially prolapsing beyond the palpebral fissure. The lesion was non-tender and non-ulcerated, with no signs of surface inflammation (Figure 1). The eye had phthysis bulbi and retinal hemangioblastoma, and there was no orbital involvement on clinical palpation. Orbital magnetic resonance imaging demonstrated a 1.2 × 0.9 × 0.7 cm well-circumscribed, homogeneous soft-tissue lesion confined to the bulbar conjunctiva. On T2-weighted fat-suppressed axial sequences, the lesion appeared hyperintense relative to extraocular muscles and clearly delineated from adjacent scleral and orbital structures, without evidence of intraorbital extension, fat infiltration, or bony involvement. The mass was completely excised and submitted for histopathologic analysis.

Slit-lamp image of a conjunctival hibernoma in a patient with von Hippel–Lindau syndrome external image of the left eye showing a firm, elevated, lobulated subconjunctival mass prolapsing beyond the palpebral fissure. The lesion displays a smooth surface with prominent vascular structures, mimicking a vascular tumor.
Gross examination showed a nodular, cream-gray, well-defined mass. Microscopy revealed multivacuolated eosinophilic cells with granular cytoplasm, arranged within a lobular and well-circumscribed architecture. Immunohistochemistry showed strong S-100 positivity in vacuolated cells, CD31, CD34, and smooth muscle actin (SMA) positivity in the vascular components, and negativity for CD68 and pan-cytokeratin. The Ki-67 proliferation index was low (Figure 2). These findings confirmed the diagnosis of subconjunctival hibernoma. The deep margin was positive, and although a more extensive excision was recommended, the patient declined further intervention. At the three-month follow-up, there was no clinical evidence of recurrence.
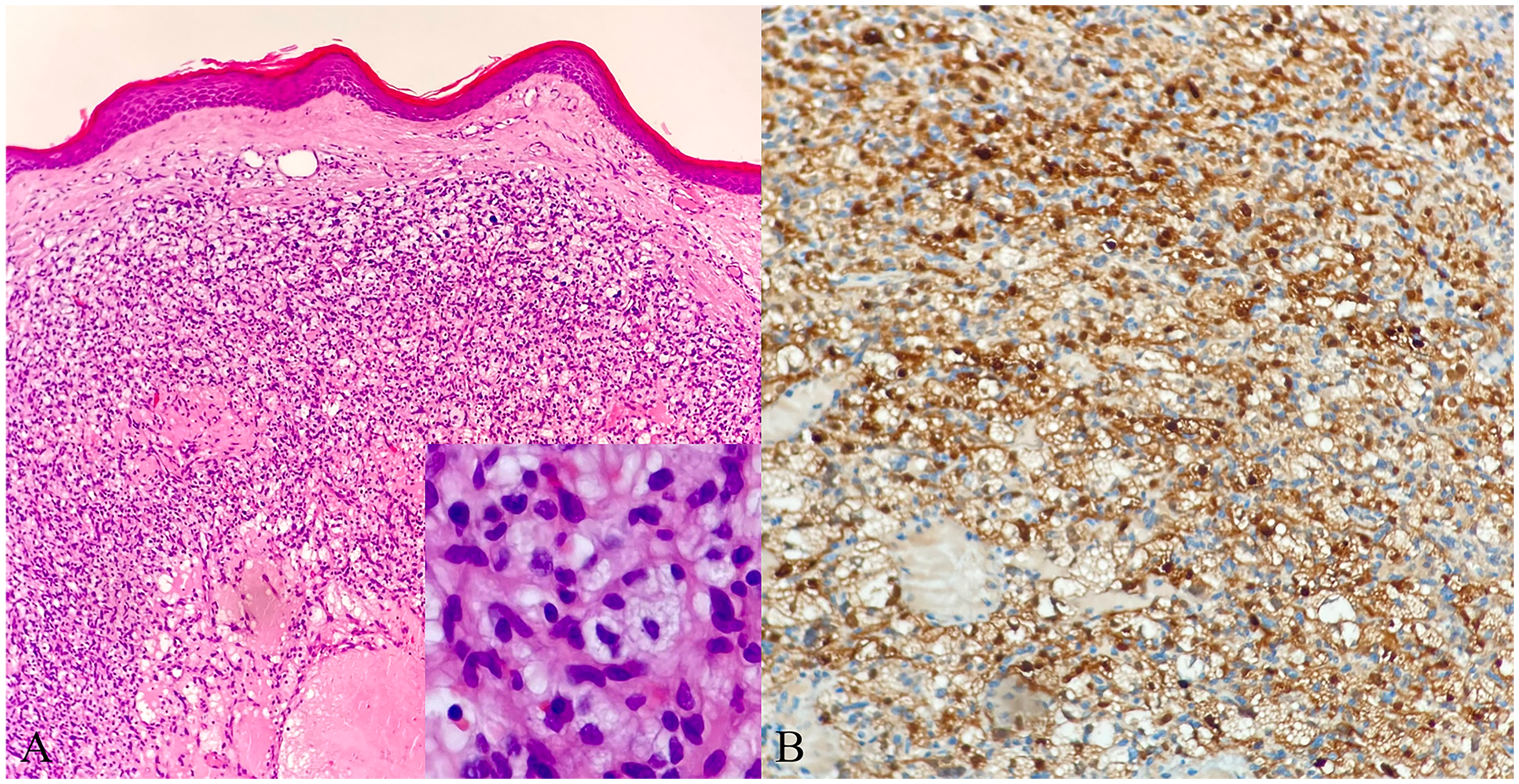
Histopathologic and immunohistochemical features of conjunctival hibernoma (A) low-power photomicrograph (hematoxylin–eosin, original magnification ×40) showing a well-circumscribed lobular lesion of multivacuolated cells with abundant granular cytoplasm beneath the conjunctival epithelium. Inset: high-power view (×400) highlighting multivacuolated cytoplasm and distinct cell borders. (B) Immunohistochemical stain for S-100 (×100) demonstrating strong, diffuse cytoplasmic positivity in tumor cells; CD31/CD34/smooth muscle actin (SMA) highlights the vascular/perivascular components (not shown).
Discussion
To our knowledge, this is the first documented case of (sub)conjunctival hibernoma in a human. Only one prior report exists in veterinary literature describing a subconjunctival hibernoma in a dog, and a single case of eyelid hibernoma has been reported in humans.2,3 Hibernomas are known to express brown fat markers such as S-100 and UCP1. While UCP1 staining was not performed, the histopathologic and immunohistochemical findings were consistent with brown fat differentiation.
They are typically slow-growing and asymptomatic, but their vascular appearance may raise suspicion for more aggressive tumors.4,5 In our patient, the lesion's prominent vasculature mimicked a vascular tumor, warranting surgical excision and histopathologic evaluation. Although the patient declined re-excision, ongoing clinical monitoring was recommended due to the positive deep margin and the potential for local persistence, despite the tumor's benign behavior.
The association between hibernoma and VHL has been described only once, in a case of adrenal hibernoma with bilateral pheochromocytomas. 6 VHL disease is characterized by dysregulation of the hypoxia-inducible factor (HIF) pathway, which promotes angiogenesis and mesenchymal tumor development through epithelial-to-mesenchymal transition. 7 Given the lesion's vascular nature and the patient's VHL background, this tumor may plausibly have originated from perivascular brown fat precursors, as previously suggested in ultrastructural studies in both rodents and humans. 4
At the molecular level, loss of functional pVHL leads to stabilization of HIF-α and persistent activation of its downstream target genes, even under normoxic conditions. 8 In adipocytes, this dysregulation alters normal adipogenic differentiation and tissue architecture. Experimental studies further indicate that HIF signaling, including HIF-1β-dependent pathways, plays a crucial role in adipocyte differentiation and metabolism. 9
Moreover, animal studies demonstrate that adipocyte-specific deletion of VHL results in hypertrophic brown adipocytes but reduced white adipose tissue, suggesting a depot-specific regulatory effect of VHL–HIF signaling on adipogenesis. In VHL-deficient mouse models, HIF-2α activation has been associated with increased angiogenesis, inflammatory changes, and altered lipid metabolism, establishing a microenvironment favorable for proliferative brown adipose differentiation. 9
Although the association between hibernoma and VHL remains speculative, the dysregulation of the HIF pathway in VHL could plausibly influence mesenchymal differentiation and vascular proliferation, creating a microenvironment favorable for brown adipose-derived tumorigenesis. 10 Nevertheless, given the single-case nature of this observation, a causal relationship cannot be established.
This case expands the phenotypic spectrum of both VHL-associated tumors and hibernomas and highlights the need to consider rare mesenchymal neoplasms in the differential diagnosis of vascular-appearing conjunctival lesions in syndromic patients.
Conclusion
Conjunctival hibernoma, though exceptionally rare, should be included in the differential diagnosis of vascularized conjunctival lesions, particularly in patients with VHL syndrome.
Footnotes
Acknowledgements
None.
Ethical approval and informed consent
Ethical approval was not required or pursued because the study involved no patient participation, human data, or animal experiments.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data sharing is not applicable to this article as no new data were created or analyzed.
Proprietary interest statement
The authors report no proprietary or commercial interests related to this manuscript.