
Abstract
Background
This study aimed to evaluate dynamic thiol/disulfide homeostasis in the tear fluid of patients with type 2 diabetes and to investigate its relationship with the presence of diabetic retinopathy (DR), considering it as a potential biomarker of oxidative stress.
Methods
A total of 96 individuals were included in the study. Participants were divided into three groups: 32 patients with diabetic retinopathy (Group 1, DR (+)), 31 patients with diabetes but without retinopathy (Group 2, DR (–)), and 33 healthy volunteers (Group 3). All participants underwent a comprehensive ophthalmological examination, including best-corrected visual acuity, slit-lamp biomicroscopy, and fundus evaluation. Tear samples were collected using Schirmer strips and stored in phosphate-buffered Eppendorf tubes at −80 °C until analysis. Total thiol, native thiol, and disulfide levels were analyzed using a spectrophotometric method. Patients with a history of intraocular surgery, trauma, glaucoma, or systemic diseases other than diabetes were excluded.
Results
There were statistically significant differences between the groups in terms of total thiol, disulfide, disulfide/total thiol, and disulfide/native thiol ratios (p < 0.001). Total thiol levels were significantly lower, while disulfide levels and ratios were significantly higher in the DR (+) group. No significant difference was found in native thiol levels (p = 0.194). HbA1c and fasting blood glucose levels were significantly higher in the DR (+) group compared to the other groups (p < 0.001). Central macular thickness was also significantly greater in the DR (+) group (p < 0.001). Correlation analysis revealed a positive and significant relationship between HbA1c and fasting blood glucose (r = 0.551; p < 0.01), whereas no significant correlation was found between central macular thickness and glycemic parameters.
Conclusion
The increased disulfide levels and disulfide ratios in the tear fluid of patients with diabetic retinopathy suggest a shift in thiol/disulfide homeostasis toward oxidative stress. These tear-based biomarkers may serve as valuable tools for the early diagnosis and monitoring of diabetic retinopathy.
Introduction
Diabetic retinopathy (DR) is one of the leading causes of irreversible vision loss in middle-aged and elderly individuals worldwide. 1 Structural and functional changes in retinal vessels due to chronic hyperglycemia are associated with mechanisms such as oxidative stress, inflammation, and endothelial dysfunction. 2 Oxidative stress, in which reactive oxygen species (ROS) cause cellular damage by failing to inhibit the antioxidant defense system, plays an important role in the pathophysiology of DR. 3
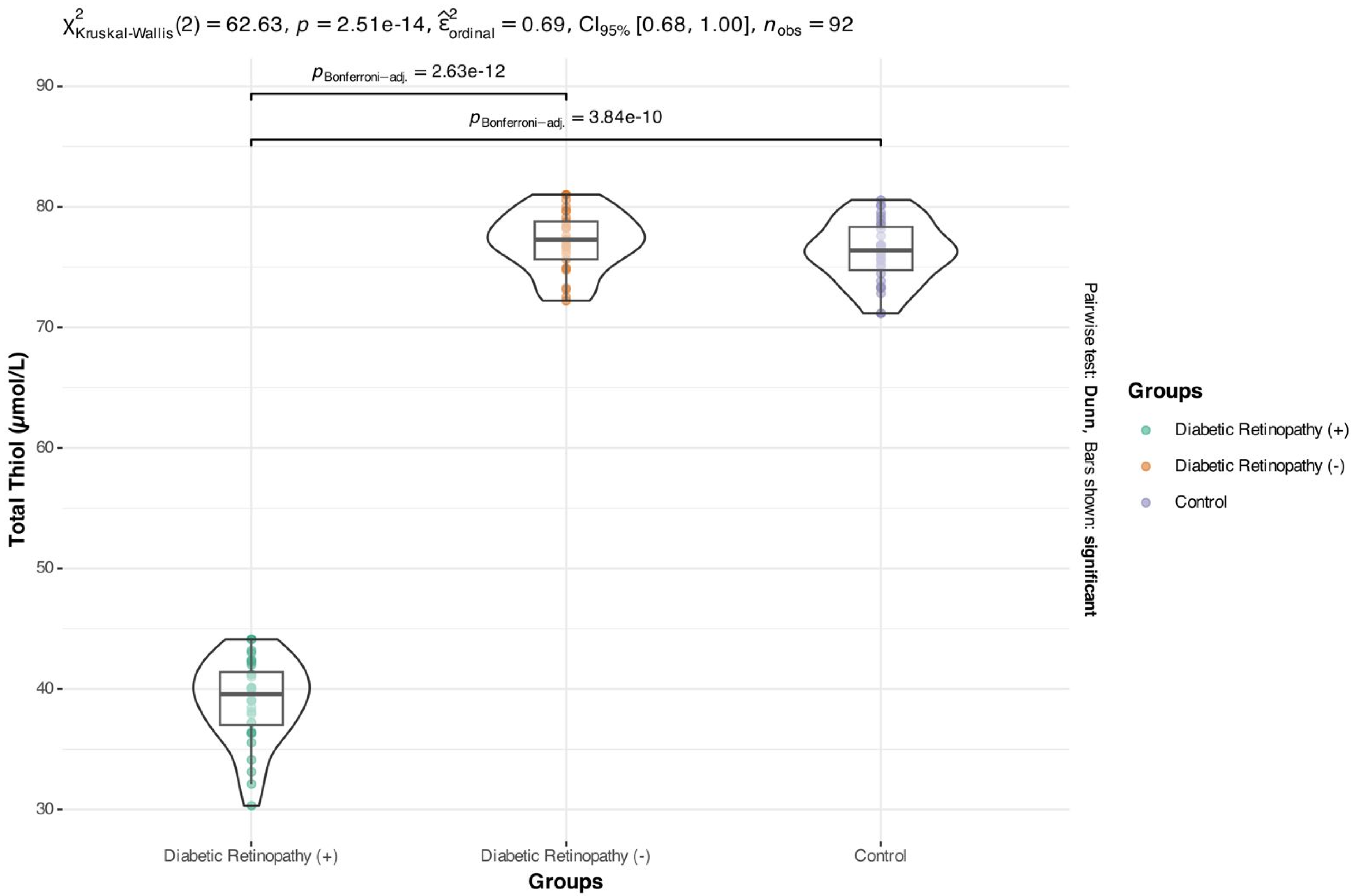
Comparison of total thiol levels among the study groups (μmol/L).
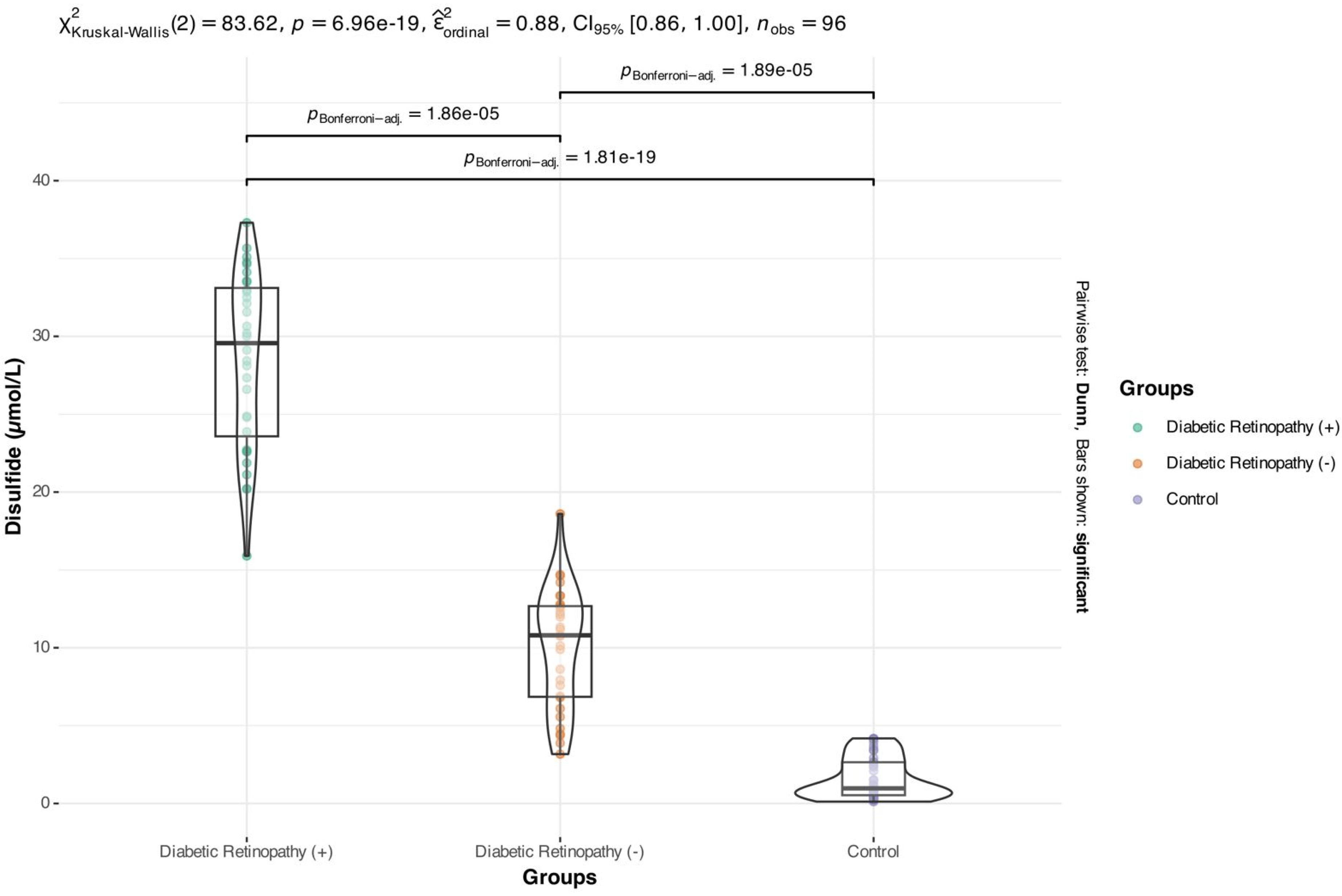
Comparison of disulfide levels among the study groups (μmol/L).
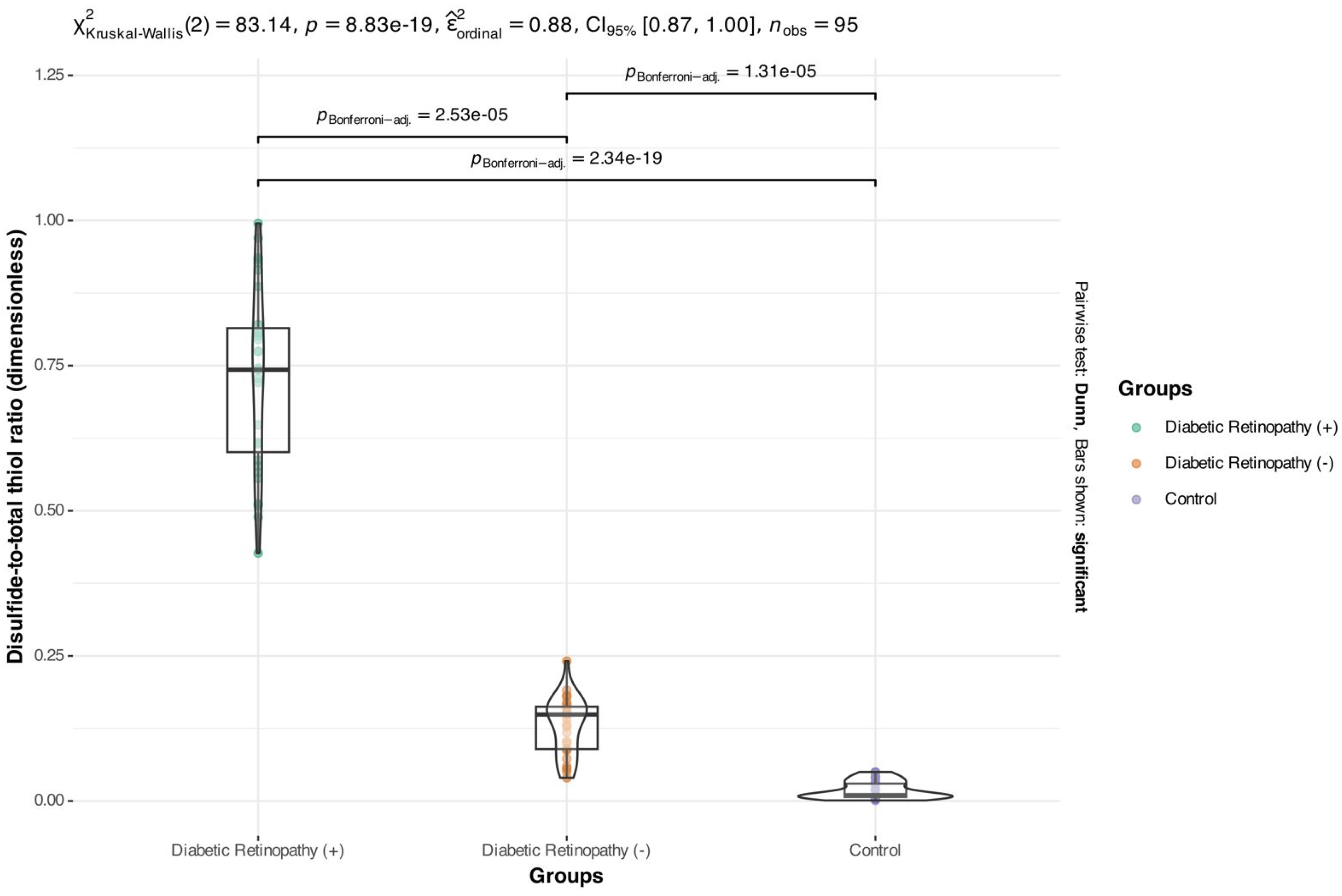
Disulfide-to-total thiol ratio in the study groups (ratio; dimensionless).
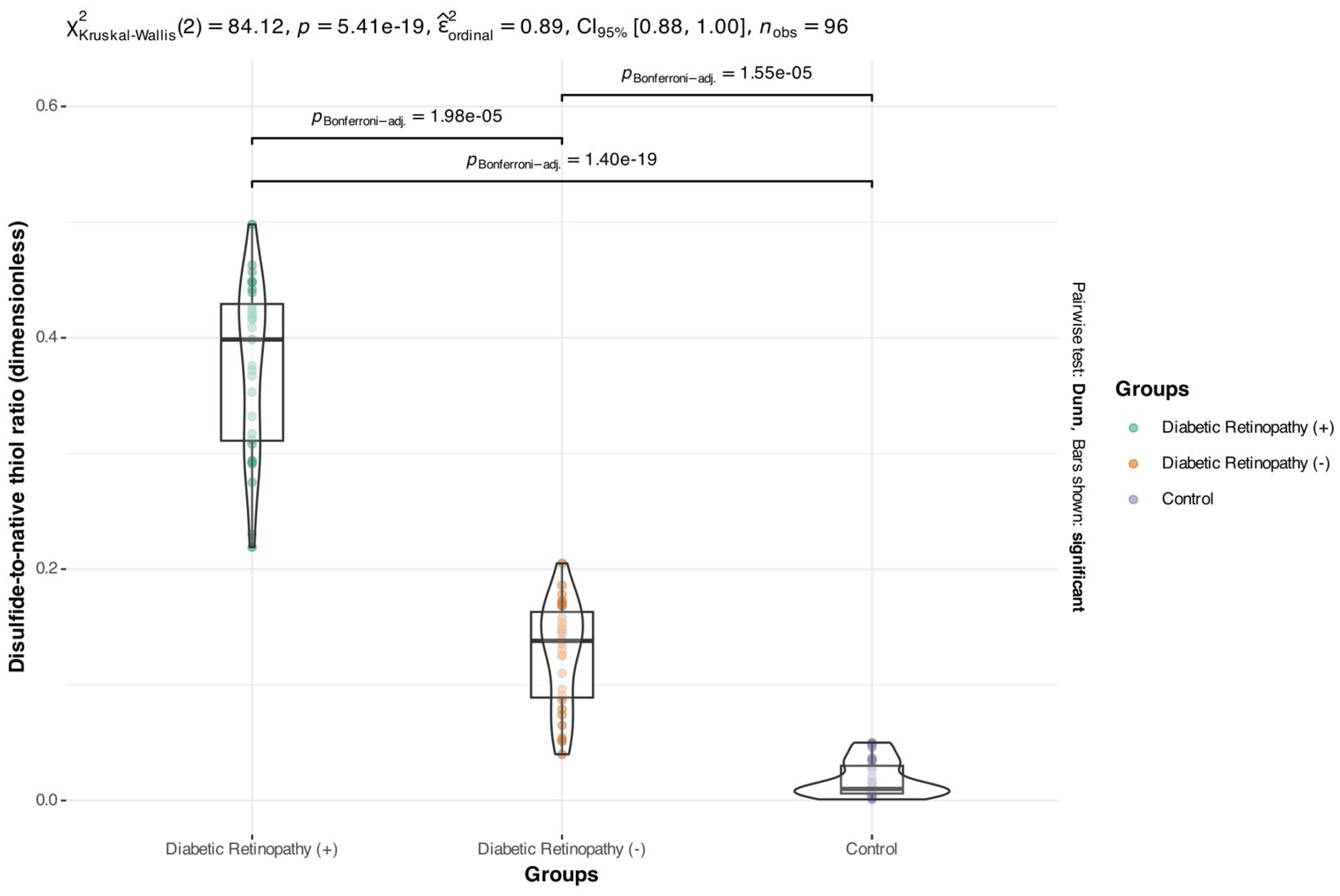
Disulfide-to-native thiol ratio in the study groups (ratio; dimensionless).
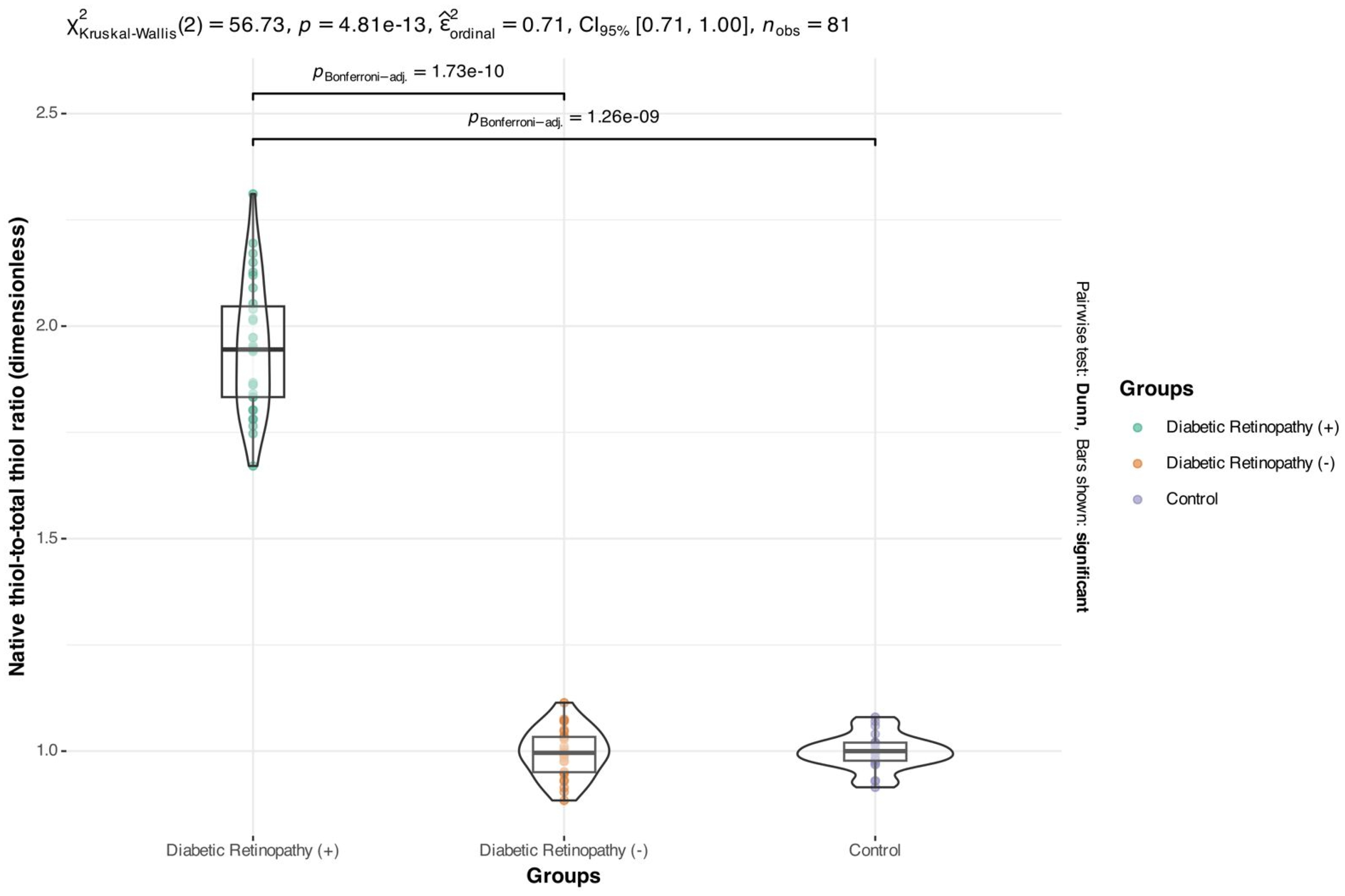
Native thiol-to-total thiol ratio in the study groups (ratio; dimensionless).
Thiol groups are important antioxidants that protect the structural integrity and function of proteins. Thiol-disulfide homeostasis is considered a dynamic and reversible indicator of oxidative stress. 4 While thiols convert to disulfides in an oxidative environment, the opposite occurs in a reducing environment. Disruption of this homeostatic balance can trigger cell damage and inflammatory processes. In recent years, the evaluation of the thiol-disulfide balance in plasma or serum samples as a biomarker for various systemic diseases (e.g., diabetes, cardiovascular diseases, and rheumatic diseases) has increased.5–10
Tears are a vital biological fluid that provides information about the local ocular microenvironment and can be obtained non-invasively. 11 Measuring oxidative stress markers in the tears of diabetic patients could provide insight into the diagnosis and monitoring of specific complications, especially retinopathy. However, data on thiol/disulfide homeostasis in tears is limited, and few studies address this issue in the literature. 12
The aim of this study was to measure dynamic thiol/disulfide homeostasis parameters in the tears of patients with type 2 diabetes and to evaluate the association between these parameters and the presence of diabetic retinopathy. The data obtained may contribute to monitoring oxidative stress with biomarkers and the early detection of DR.
Materials and methods
This prospective observational study was conducted with the approval of the Uşak University Ethics Committee (approval no. 07.11.2024/473-473-20). The study included 96 patients presenting to the ophthalmology outpatient clinic with visual complaints. Participants were divided into three groups: type 2 diabetic patients with diabetic retinopathy (DR (+) group; n = 32), type 2 diabetic patients without diabetic retinopathy (DR (-) group; n = 31), and healthy subjects without systemic disease (control group; n = 33). In line with previously published percentage-based measurement values for the parameters under investigation, a priori power analysis using the G*Power software (effect size = 0.385, power = 90%, α = 0.05) indicated that a minimum of 90 participants would be required for adequate statistical power.
The inclusion criteria were a diagnosis of type 2 diabetes mellitus (DM) and consent to the study protocol. Patients who had undergone previous ocular surgery, had glaucoma, uveitis, or ocular surface disease, or had systemic inflammatory or autoimmune diseases were excluded.
All patients underwent a comprehensive ophthalmological examination, which included a best-corrected visual acuity test, a slit lamp examination, a dilated fundus examination, and applanation tonometry. Diabetic retinopathy was diagnosed based on fundus retinal findings and fundus fluorescein angiography. Macular thickness was measured using optical coherence tomography (OCT-HS 100, Canon Europe N.V., Japan).
Tear samples were obtained by placing Schirmer paper strips in the inferior conjunctival fornix of the right eye for a maximum of five minutes. To ensure methodological consistency and avoid inter-eye variability, only the right eye was sampled. This approach has been commonly used in previous tear biomarker studies and minimizes potential bias from asymmetrical ocular involvement. Care was taken to avoid stimulating tears, using topical anesthetics, or applying other eye drops. Lighting and room temperature were also taken into consideration. The ocular surface was not damaged. Tear samples were collected by one person, SD. A test result of 15–20 mm was considered sufficient for biochemical analysis. The Schirmer strips were stored in Eppendorf tubes containing 2 ml of phosphate buffer at −80 °C and subsequently diluted with 500 μL of pre-chilled saline.
The Schirmer strips were stored in phosphate-buffered Eppendorf tubes at −80 °C and diluted with 500 μL of pre-chilled saline.
Biochemical analysis
Disulfide bonds were reduced to form free functional thiol groups. The unused reducing sodium borohydride was consumed and removed with formaldehyde. All thiol groups (including reduced and native thiol groups) were determined after reacting with 5,5′-dithiobis-(2-nitrobenzoic) acid. The difference between total and native thiol levels was divided by two to determine the dynamic disulfide amount. After determining the levels of natural and total thiols, the amounts of disulfides, the percentage ratios of disulfides to total thiols, disulfides to natural thiols, and natural thiols to total thiols were calculated. 4
We determined total and native thiol-disulfide levels using Rel Assay Diagnostics kits (lot numbers KM2201N and KM2201 T, respectively). Absorbance was measured at 620 nm using a Multiskan FC Microplate Photometer (Thermo Fisher Scientific, Waltham, MA). Concentrations were calculated according to the following formula: [(H₂O absorbance - sample absorbance) / (H₂O absorbance - calibrator absorbance) ] × calibrator concentration. After the concentration calculations were performed, the disulfide levels were determined using the following formula: Total thiol - natural thiol)/2.
Statistical analysis
The NCSS (Number Cruncher Statistical System) 2007 program (Kaysville, Utah, USA) was used for statistical analysis. Descriptive statistical methods, such as mean, standard deviation, median, frequency, percentage, minimum, and maximum, were used to evaluate the study data. The Shapiro-Wilk test was used to evaluate the distribution of the data. The Kruskal-Wallis test was used to compare quantitative data that did not show a normal distribution among three or more groups. The Mann-Whitney U test was used to compare the two groups. Spearman correlation analysis was used to evaluate the relationships between quantitative data. The statistical significance level was accepted as p < 0.05.
Results
A total of 96 individuals were included in the study: 32 with diabetic retinopathy (DR +), 31 without diabetic retinopathy (DR -), and 33 healthy controls. There was no statistically significant difference in mean age between the groups (p = 0.250) (Table 1).
Demographic, clinical, and biochemical characteristics of the study groups.
Values are presented as mean ± standard deviation. p < 0.05 was considered statistically significant.
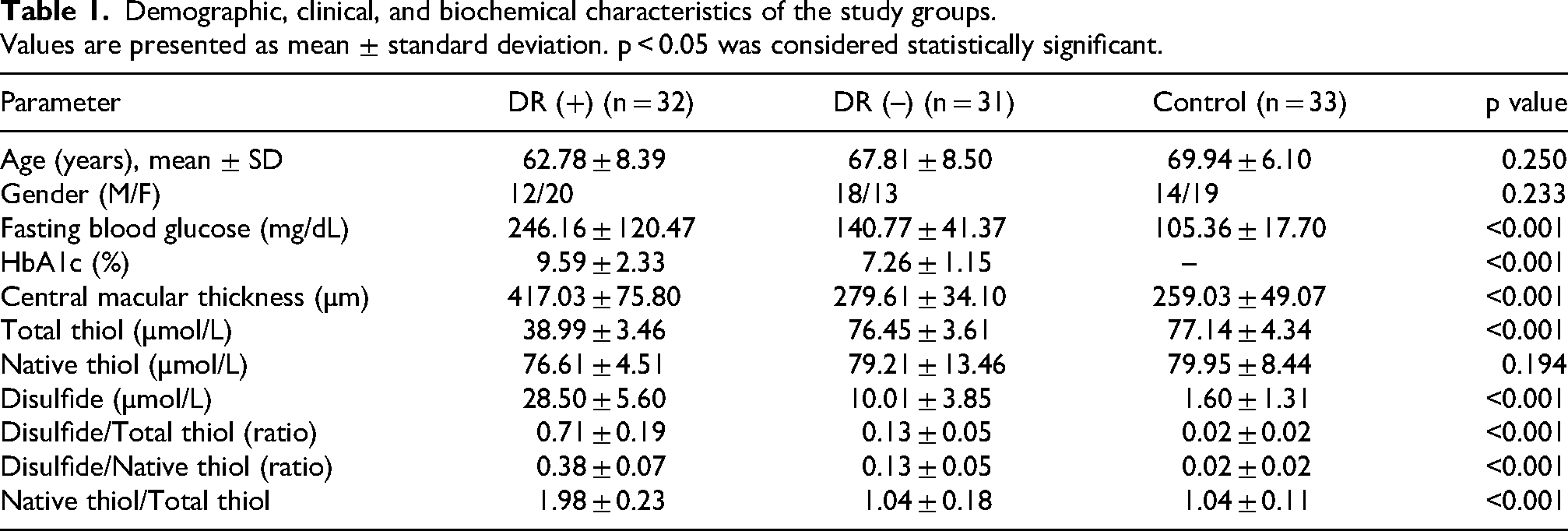
Comparisons of thiol-disulfide homeostasis parameters revealed that total thiol levels were significantly lower in the DR (+) group (DR (+): 38.99 ± 3.46 μmol/L; DR (–): 76.45 ± 3.61 μmol/L; control: 77.14 ± 4.34 μmol/L; p < 0.001) (Graphic 1). Disulfide levels were significantly higher in the DR (+) group (DR (+): 28.5 ± 5.6 μmol/L; DR (–): 10.01 ± 3.85 μmol/L; Control: 1.6 ± 1.31 μmol/L; p < 0.001) (Graphic 2). Native thiol levels did not differ significantly between groups (p = 0.194).
The disulfide/total thiol ratio was 0.71 ± 0.19 in the DR (+) group. This ratio was significantly lower in the DR (–) group (0.13 ± 0.05) and lowest in the control group (0.02 ± 0.02; p < 0.001) (Graphic 3). Similarly, the disulfide-to-native thiol ratio was significantly higher in the DR (+) group (DR (+): 0.38 ± 0.07; DR (–): 0.13 ± 0.05; control: 0.02 ± 0.02; p < 0.001) (Graphic 4). The native thiol/total thiol ratio increased significantly in the DR (+) group (1.98 ± 0.23), with no significant difference observed between the other two groups (p < 0.001) (Graphic 5).
In terms of metabolic parameters, the average fasting blood glucose level was 246.16 ± 120.47 mg/dL in the DR (+) group. This level was significantly higher than in the DR (–) (140.77 ± 41.37 mg/dL) and control (105.36 ± 17.7 mg/dL) groups (p < 0.001). Similarly, HbA1c levels were highest in the DR (+) group (DR (+): 9.59 ± 2.33%; DR (–): 7.26 ± 1.15%; p < 0.001).
Central macular thickness was significantly higher in the DR (+) group (DR (+): 417.03 ± 75.8 μm; DR (–): 279.61 ± 34.1 μm; control: 259.03 ± 49.07 μm; p < 0.001). However, there was no statistically significant difference between the DR (–) and control groups in terms of this parameter (p = 0.090).
Correlation analysis revealed a positive and significant correlation between HbA1c and fasting blood glucose levels in the DR (+) group (r = 0.551, p < 0.01). However, no significant correlation was found between central macular thickness and glycemic parameters (HbA1c and fasting blood glucose) (p > 0.05). Similarly, no significant correlation was observed between central macular thickness and glycemic parameters in the DR (–) and control groups.
Discussion
In this study, we evaluated the thiol-disulfide homeostasis parameters in the tears of patients with type 2 diabetes and investigated the relationship between these biochemical changes and diabetic retinopathy. Our findings revealed that individuals with DR had significantly higher oxidative stress levels, which was reflected in the thiol-disulfide balance in tears. Specifically, disulfide levels and disulfide/thiol ratios increased while total thiol levels decreased. This indicates that the redox balance shifted towards the oxidative side.
It is well-known that chronic hyperglycemia-induced oxidative stress plays a fundamental role in the pathogenesis of DR. Ateş et al. reported that thiol oxidation increases in patients with type 1 diabetes, which may be due to hyperglycemia and chronic inflammation. 13 Unlike our study, theirs examined additional parameters indicating inflammation, such as C-reactive protein (CRP), and suggested that decreased thiol levels may be related to inflammatory processes.
Similarly, a study by Yuvacı et al. reported that serum disulfide levels were significantly higher in patients with type 2 diabetes in both the DR and non-DR groups than in healthy individuals. However, no significant difference was found in native and total thiol levels. 14 Interestingly, native thiol levels did not differ significantly across the groups. This may suggest that although total thiols decrease and disulfide levels increase, native thiols could be preserved through compensatory antioxidant mechanisms. Although total thiol levels decreased and disulfide levels increased in patients with DR, native thiol concentrations remained stable across groups. This pattern may indicate an early compensatory antioxidant response, where native thiols are preserved by increased conversion of total thiols into disulfide bonds. Tear film antioxidant mechanisms—primarily glutathione-dependent pathways—may transiently maintain native thiol availability despite heightened oxidative stress. Over time, this compensatory mechanism may become depleted, leading to progressive redox imbalance in advanced disease. This finding suggests that preserved native thiol levels may represent a transitional biochemical stage in the evolution of DR-related oxidative stress. Maintenance of native thiols might reflect the ongoing adaptive response of the ocular surface to oxidative stress. However, over time, such compensatory capacity may become exhausted, leading to further oxidative imbalance. This interpretation may partly explain why native thiol levels remain relatively stable, despite the observed increase in disulfide formation. These results suggest that antioxidant defense systems become inadequate over time in diabetes, disrupting the thiol-disulfide balance. Furthermore, the absence of a significant difference in disulfide levels according to DR presence suggests that this imbalance may be a general consequence of diabetes. Nevertheless, the manner in which this balance changes in local biological fluids, such as tears, and its relationship to the development of DR remain unclear.
A study examining thiol levels and advanced glycation end products (AGEs) in diabetic individuals with and without diabetic retinopathy found no significant relationship between thiol levels and disease status. However, a significant association was found between advanced glycation end products (AGEs) and diabetes and DR. 15
Another study examined thiol levels in the serum and aqueous fluids of individuals with type 2 diabetes and found a significant decrease in serum thiol levels in the DR and diabetic groups. However, no significant difference was found between the groups in aqueous fluids. 16
Yazici et al. evaluated glutathione levels, an important component of thiol metabolism, and reported that they were significantly lower compared to the control group. 17 Kalaycı et al. demonstrated that total thiol (TT), native thiol (NT), and disulfide (D) levels decreased in patients with DR and macular edema; however, there was no significant change in the D/TT or D/NT ratios. 18
In the study by Gülpamuk et al., patients were divided into three groups: diabetics without ocular involvement, patients with non-proliferative diabetic retinopathy, and patients with proliferative DR. Thiol-disulfide parameters were examined, and significant differences were found between the proliferative DR group and the other two groups. 19
This study evaluated thiol-disulfide homeostasis for the first time using tear samples, demonstrating that this fluid may provide clinically useful biomarkers. Another important observation of our study was the absence of a correlation between central macular thickness and thiol/disulfide parameters. This negative result suggests that oxidative stress status in tears may reflect systemic metabolic or retinal vascular processes rather than directly correlating with structural retinal changes such as macular thickness. It is possible that biochemical alterations in the tear film precede or occur independently of morphological retinal changes detectable by OCT. Longitudinal studies are warranted to clarify whether tear-based oxidative markers can serve as early indicators before structural changes become apparent. Biochemical changes in tears that are compatible with retinal structural parameters, such as central macular thickness, support the relationship between the thiol-disulfide balance and ocular tissues.
Tears are an important biological fluid that protects the ocular surface, provides defense against infection, and maintains optical quality. It is known that the composition of tears can change as a result of systemic or local diseases. In retinal diseases, such as diabetic retinopathy, changes in tear biochemistry may indicate the progression of the disease.
Tear fluid differs from serum in protein content, electrolyte concentration, and enzymatic activity, all of which may affect thiol/disulfide measurement stability. Pre-analytical factors such as tear collection technique, Schirmer strip absorption variability, dilution ratios, and storage temperature may also influence assay reproducibility. Although standardized protocols were followed—including collection by a single investigator, avoidance of reflex tearing, and immediate freezing at −80 °C—minor variations are inevitable. To improve analytical reliability, all biochemical measurements were performed in triplicate, which minimized intra-assay variability. Furthermore, thiol/disulfide assays validated for serum may behave differently in low-protein matrices such as tears. Future studies incorporating duplicate analyses, inter-laboratory calibration, and matrix-specific validation are needed to optimize the reliability of tear-based thiol measurements.
According to our findings, the increase in HbA1c and fasting blood glucose levels observed in the DR (+) group appears to be related to a redox imbalance. Although no direct correlation was found between HbA1c and disulfide ratios, correlation analyses revealed a positive, significant relationship between HbA1c and fasting blood glucose levels. These results suggest that oxidative stress may be directly linked to glycemic control. 20
Recent studies have more clearly demonstrated the role of the thiol/disulfide balance in the pathogenesis of diabetic retinopathy. In their extensive sample study, Coşkun et al. reported that serum thiol levels decreased significantly as the DR stage progressed; this finding parallels the thiol decreases detected in tears in our study. 21 Systematic reviews on the use of tear biomarkers in diagnosing and monitoring diabetic ocular complications also emphasize this noninvasive fluid's potential. 22 Furthermore, increased oxidative stress parameters in vitreous and aqueous humor fluids suggest that the thiol/disulfide system is effective in both the systemic circulation and the local retinal microcirculation.2 °Consistent with this, Ertan et al. demonstrated altered thiol/disulfide homeostasis in patients with retinitis pigmentosa, further supporting the clinical relevance of this biochemical pathway in retinal diseases. 23 In this context, the increase in disulfide levels and shift in redox balance detected in tears in our study reflect a biochemical response specific to DR and suggest that these parameters may be potential biomarkers for early diagnosis and risk stratification in clinical applications. Additionally, our study is significant because no other study has examined the thiol/disulfide balance in the tears of diabetic patients. Noninvasive, easy, and reproducible tear sampling may facilitate clinical applications.
This study has several limitations. First, the relatively small cohort, particularly the limited number of patients in the DR (+) subgroup (n = 32), restricts the generalizability of our findings. Larger multicenter studies with more diverse populations are required to validate and extend these results. Additionally, due to the progressive nature of retinopathy, long-term prospective studies are necessary to evaluate how these biomarkers evolve throughout the disease process. However, it has not been possible to completely exclude local factors that may influence tear biochemistry, such as dry eye, ocular surface diseases, and contact lens wear. Finally, thiol/disulfide homeostasis measurements in tears have not yet been fully integrated or standardized for clinical use. This is another factor to consider in terms of interlaboratory consistency of results. Another limitation relates to the lack of inter-laboratory standardization for thiol/disulfide homeostasis assays. Although the automated spectrophotometric method developed by Erel et al. is validated and widely used, variations in kit batches, sample handling, and analytical protocols may lead to discrepancies across laboratories. This underscores the need for harmonized protocols and multicenter validation studies to ensure reproducibility and comparability of results, particularly if tear-based assays are to be translated into routine clinical practice.
Conclusion
Parameters of thiol/disulfide homeostasis in tears show significant biochemical changes that reflect increased levels of oxidative stress in diabetic retinopathy. Prospective studies with larger samples are needed to evaluate these parameters as biomarkers for the early diagnosis and monitoring of DR.
Footnotes
Statement of ethics
This study protocol was reviewed and approved by [Uşak University Ethics Committee], approval number [07.11.2024/473-473-20].
Author contributions
Suzan Doğruya, Funda Karabağ : Conceptualization, Methodology, Data curation, Writing- Original draft preparation,Visualization, Investigation, Supervision, Software, Validation, Writing- Reviewing and Editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data statement
The data generated in the present study may be requested from the corresponding author.