
Abstract
Diabetic retinopathy (DR) remains a leading cause of vision loss worldwide, yet the extent to which contemporary DR clinical trials reflect the demographics of affected populations is unclear. Large population-based studies have demonstrated substantial variation in DR prevalence and outcomes by race/ethnicity and socioeconomic status (SES), raising concerns about the external validity and equity of trial-derived evidence.1,2
We reviewed diabetic retinopathy clinical trials and randomized controlled trials indexed in PubMed between January 2020 and April 2024, restricted to articles categorized as “Clinical Trial” or “Randomized Controlled Trial.” A total of 332 eligible studies were assessed for reporting of participant sex, race/ethnicity, SES, insurance status, and sexual orientation. This analysis was descriptive and intended to characterize demographic reporting practices rather than to perform a formal systematic review.
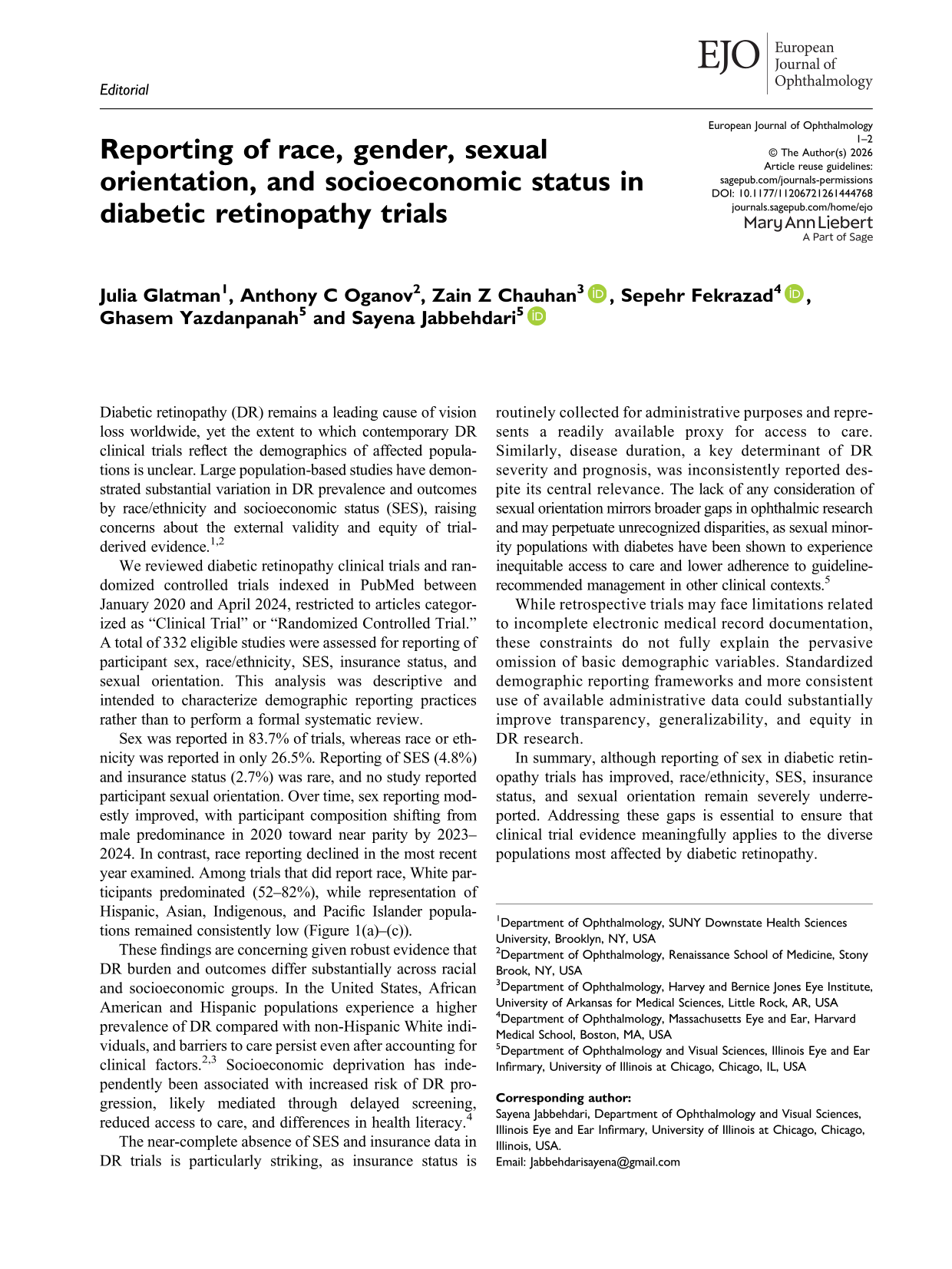
Sex was reported in 83.7% of trials, whereas race or ethnicity was reported in only 26.5%. Reporting of SES (4.8%) and insurance status (2.7%) was rare, and no study reported participant sexual orientation. Over time, sex reporting modestly improved, with participant composition shifting from male predominance in 2020 toward near parity by 2023–2024. In contrast, race reporting declined in the most recent year examined. Among trials that did report race, White participants predominated (52–82%), while representation of Hispanic, Asian, Indigenous, and Pacific Islander populations remained consistently low (Figure 1(a)–(c)).
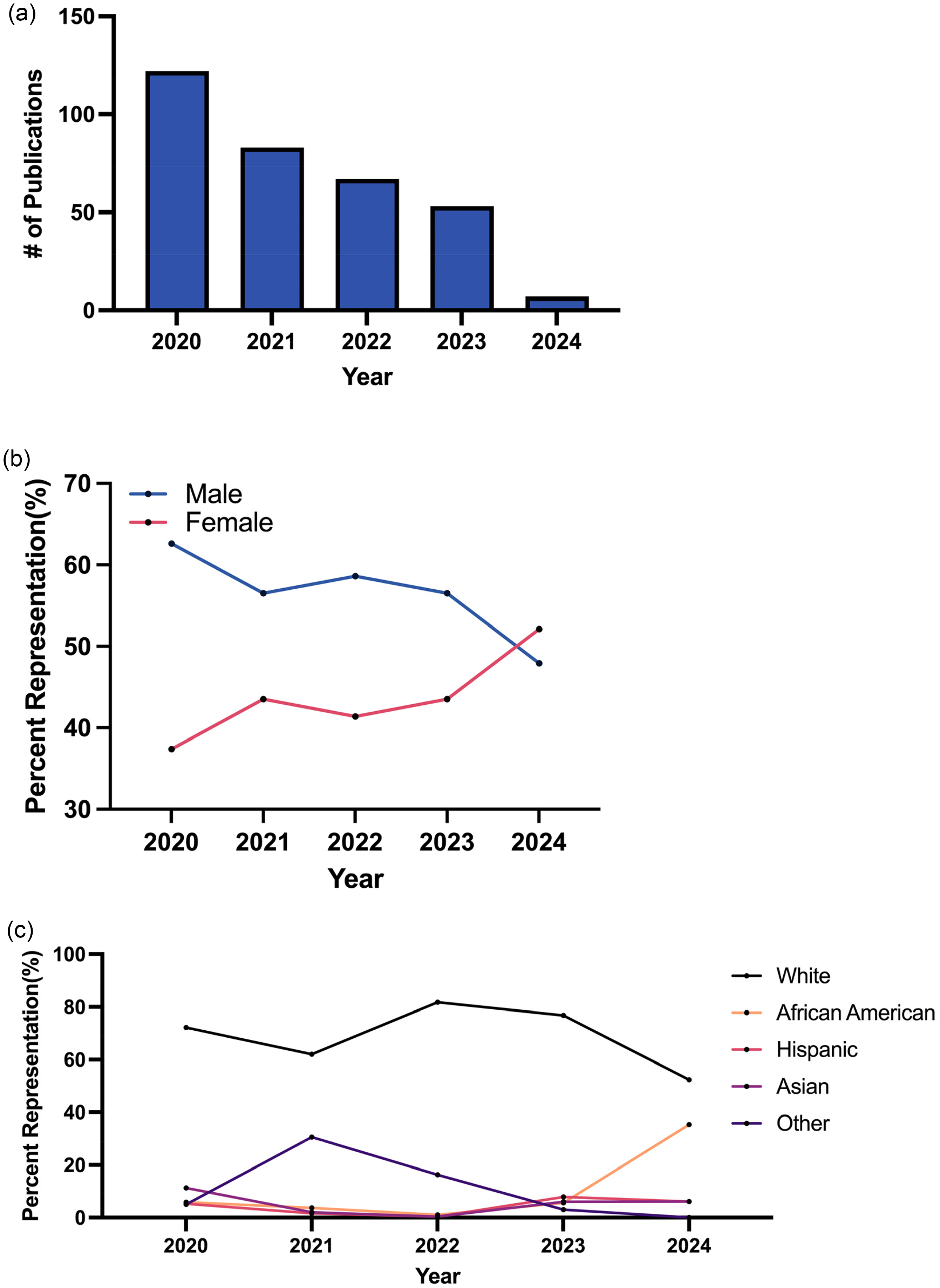
Demographic reporting in diabetic retinopathy trials (2020–2024). (a) Frequency of demographic variable reporting. (b) Sex distribution over time. (c) Racial composition among studies reporting race/ethnicity.
These findings are concerning given robust evidence that DR burden and outcomes differ substantially across racial and socioeconomic groups. In the United States, African American and Hispanic populations experience a higher prevalence of DR compared with non-Hispanic White individuals, and barriers to care persist even after accounting for clinical factors.2,3 Socioeconomic deprivation has independently been associated with increased risk of DR progression, likely mediated through delayed screening, reduced access to care, and differences in health literacy. 4
The near-complete absence of SES and insurance data in DR trials is particularly striking, as insurance status is routinely collected for administrative purposes and represents a readily available proxy for access to care. Similarly, disease duration, a key determinant of DR severity and prognosis, was inconsistently reported despite its central relevance. The lack of any consideration of sexual orientation mirrors broader gaps in ophthalmic research and may perpetuate unrecognized disparities, as sexual minority populations with diabetes have been shown to experience inequitable access to care and lower adherence to guideline-recommended management in other clinical contexts. 5
While retrospective trials may face limitations related to incomplete electronic medical record documentation, these constraints do not fully explain the pervasive omission of basic demographic variables. Standardized demographic reporting frameworks and more consistent use of available administrative data could substantially improve transparency, generalizability, and equity in DR research.
In summary, although reporting of sex in diabetic retinopathy trials has improved, race/ethnicity, SES, insurance status, and sexual orientation remain severely underreported. Addressing these gaps is essential to ensure that clinical trial evidence meaningfully applies to the diverse populations most affected by diabetic retinopathy.