
Abstract
Background
To identify predictors of unplanned endothelial keratoplasty after phacoemulsification in Fuchs’ endothelial corneal dystrophy (FECD), and to assess postoperative best-corrected visual acuity (BCVA).
Methods
Retrospective single-centre case series of 50 eyes (39 patients) that underwent soft-shell phacoemulsification and monofocal intra-ocular lens implantation by one surgeon (2015–2021). The primary outcome was unplanned corneal decompensation requiring endothelial keratoplasty. Associations with specular-microscopy parameters and central corneal thickness (CCT) were examined with penalised logistic and Cox regressions adjusted for age, sex, and hypertonic-saline use. Postoperative BCVA was analysed using linear regression models also adjusted for baseline acuity.
Results
Mean age was 74 ± 8 years; 68% were women; median follow-up 32 (IQR 24–40) months. Four eyes (8%) required Descemet stripping endothelial keratoplasty a median 8 months after cataract surgery. Each 1 μm increase in pre-operative CCT raised the hazard of grafting by 2% (HR 1.02, 95% CI 1.00–1.04, P = 0.031); a threshold of ≥ 620 μm yielded an AUC of 0.91. Linear regression analyses of postoperative BCVA adjusted for preoperative BCVA showed no clear association between baseline and postoperative acuity.
Conclusions
Pre-operative CCT shows the strongest association of readily available metrics with post-phaco corneal failure in FECD; values above ∼600 μm may warrant counselling regarding combined or staged keratoplasty.
Keywords
Introduction
Fuchs’ endothelial corneal dystrophy (FECD) is the most common primary corneal endothelial dystrophy 1 and the leading indication for corneal transplantation worldwide. 2 It is a genetically complex and clinically heterogeneous, progressive condition characterised by accelerated endothelial cell loss, extracellular matrix deposition in the Descemet membrane, and impaired corneal deturgescence with age. 3 FECD typically causes bilateral visual impairment due to corneal oedema from the fifth decade of life. 4 Due to this late presentation, most patients with FECD also present with cataracts, further compounding their sight loss. 5 Cataract surgery in FECD patients, particularly the intraocular manipulation and ultrasonic energy from phacoemulsification, can further damage the endothelium,6,7 increasing the risk of corneal decompensation and painful bullous keratopathy, often necessitating keratoplasty.
The soft-shell technique, introduced by Arshinoff in 1999, combines dispersive and cohesive ophthalmic viscoelastic devices (OVDs) to protect the corneal endothelium during phacoemulsification. 8 This has led to widespread adoption of the soft-shell technique and its various iterations for cataract surgery in patients with FECD.9,10 While effective and widely adopted for FECD patients,11–13 some still develop refractory corneal oedema postoperatively, requiring corneal transplantation. The factors contributing to this complication remain poorly understood.
This study aimed to evaluate preoperative risk factors, including specular microscopy parameters and corneal pachymetry, for unplanned endothelial keratoplasty after phacoemulsification with the soft-shell technique in eyes with FECD.
Methods
Study design and participants
We retrospectively analysed consecutive FECD patients undergoing phacoemulsification with intraocular lens implantation by a single surgeon (FF) between 1st October 2015 and 30th September 2021 at a UK tertiary corneal service. All operations were undertaken with a soft-shell technique using DuoVisc® (Alcon, US), combining VISCOAT® (sodium chondroitin and sodium hyaluronate) and PROVISC® (sodium hyaluronate) OVDs. Monofocal lenses were implanted aiming for emmetropia. FECD was diagnosed by a corneal specialist via slit-lamp biomicroscopy and specular microscopy.
Selection criteria
Of 179 eyes with FECD identified, we excluded 116 without pre- and post-operative specular microscopy data, two with poor-quality specular microscopy reports, one with less than six months’ follow-up, two requiring vitrectomy for vitreous prolapse secondary to zonular weakness, and eight eyes scheduled for endothelial keratoplasty preoperatively. The final analytic sample comprised 50 eyes from 39 patients. Missing specular microscopy data were due to electronic medical record transitions in our hospital.
Data collection
Pre- and post-operative best-corrected visual acuity (BCVA) was measured at 0, 1, 3 and 6 months using a Snellen chart at six metres and converted to logarithm of the Minimum Angle of Resolution (logMAR). For post-operative assessments, the latest available BCVA was used, or earlier data if unavailable. Specular microscopy was performed using the NonCon Robo series microscope (Konan Medical, Japan) in semi-automatic mode by trained outpatient clinic staff. Central corneal thickness (CCT) was measured via contact pachymetry or specular microscopy; if both were available, their mean was used. Local hospital approval was obtained for this service evaluation project (No: 11238), adhering to UK governance and the Declaration of Helsinki.
Outcomes
The primary outcome was unplanned endothelial keratoplasty after cataract surgery. We also report results for any endothelial keratoplasty, irrespective of planning status, as a secondary analysis. Postoperative corneal decompensation/oedema was analysed separately as an exploratory outcome.
Statistics
Statistical analyses were performed using R (Version 4.2.1, The R Foundation, Vienna, Austria). Baseline demographics and specular microscopy metrics were compared using t-tests and χ2 tests. Specular microscopy parameters, reflecting corneal endothelial health, were each analysed separately in multivariable logistic regression models. Because some patients contributed both eyes, within-patient clustering was considered. However, the number of outcome events was too small to support stable models accounting for subject-level clustering, so final models were adjusted for age, sex, and pre-operative hypertonic saline use only. Penalised maximum likelihood estimation was used to account for rare events. Optimal cut-off points for specular microscopy parameters were identified by maximising the Youden Index (sensitivity + specificity − 1). The term ‘optimal' is used in this statistical sense only and does not imply formal clinical, decision-analytic, or cost-utility optimisation. Time-to-event analyses were conducted with Cox models, incorporating the same covariates. The optimal cut-point for time-to-corneal transplantation was determined using maximally selected rank statistics to identify thresholds maximising differences between groups. The power analysis, based on a retrospective case series of 136 eyes with FECD, 14 used probabilities of 10% (p₁ = 0.1) progression to penetrating keratoplasty and 90% (p₀ = 0.9) no progression for eyes with preoperative corneal thickness ≥ 600 μm, showing a high power of 99.65% with our sample size of 50 at α = 0.05.
Results
Baseline characteristics
Fifty eyes of 39 patients with FECD met the inclusion criteria. These included two eyes with previous herpetic kerato-uveitis and one with band keratopathy. Median follow-up was 32 months (IQR 24–40). Preoperative median BCVA was 0.19 logMAR (IQR 0.16–0.35), equivalent to a Snellen BCVA of 6/9.6 (IQR 6/9.6–6/12) or 75 ETDRS letters (IQR 70–75). Median spherical equivalence was 0.3 dioptres (IQR −2.75 to 2.75).
Anatomical outcomes
Intraoperatively, one eye (2%) had an anterior capsule tear without complications. Postoperatively, two eyes developed cystoid macular oedema that resolved with topical treatment. Corneal oedema occurred in 7 (14%) eyes, with seven cases improving after corticosteroid and hypertonic saline treatment. Four eyes required Descemet stripping endothelial keratoplasty (DSAEK) following corneal decompensation post-surgery. The median time from cataract surgery to transplantation was 8 months (IQR 7–9). Median postoperative spherical equivalence was 0.06 dioptres (IQR −0.34 to 1.00). Baseline demographics and specular microscopy measurements are summarised in Table 1.
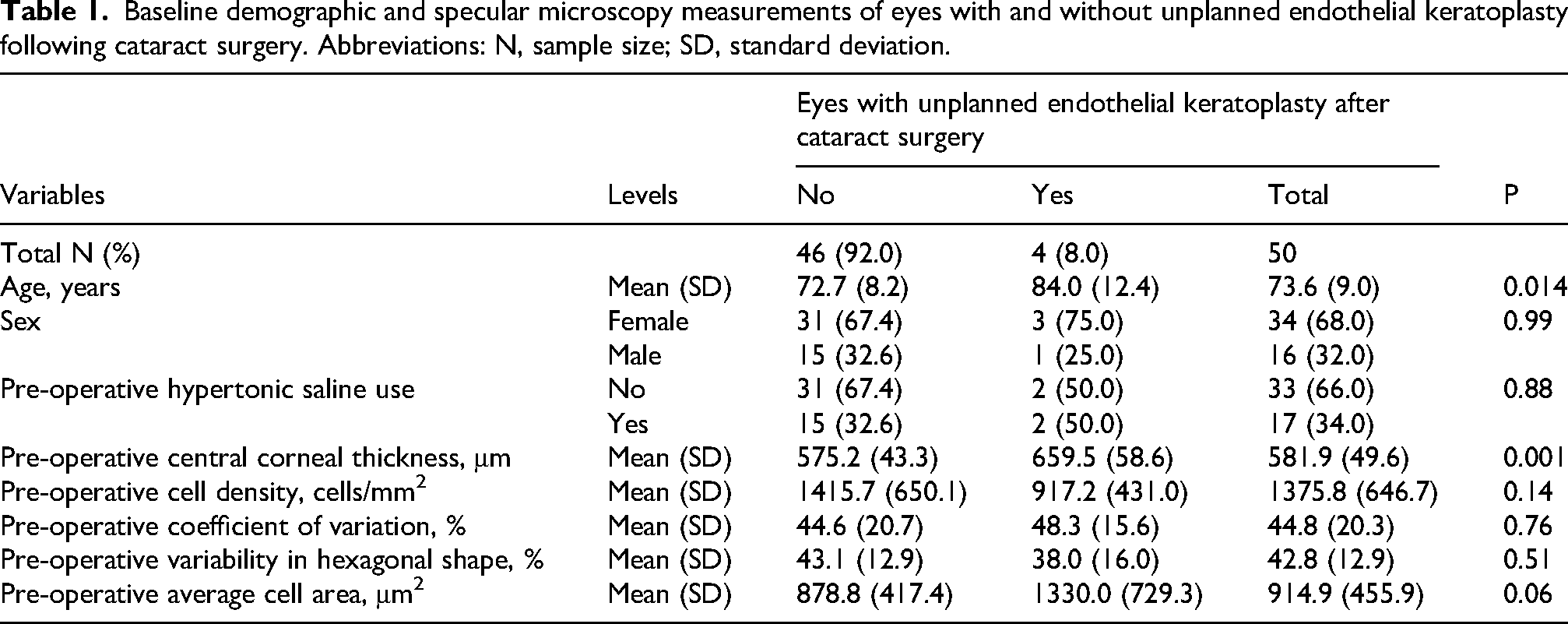
Baseline demographic and specular microscopy measurements of eyes with and without unplanned endothelial keratoplasty following cataract surgery. Abbreviations: N, sample size; SD, standard deviation.
Preoperative specular microscopy and corneal transplantation risk
Preoperative central corneal thickness was significantly higher by 84 μm in eyes requiring unplanned endothelial keratoplasty (660 ± 59 μm vs. 575 ± 43 μm, P = 0.001). Age was also significantly greater in this group (84.0 ± 12.4 years vs. 72.7 ± 8.2 years, P = 0.014). No other significant baseline differences were observed (Table 1).
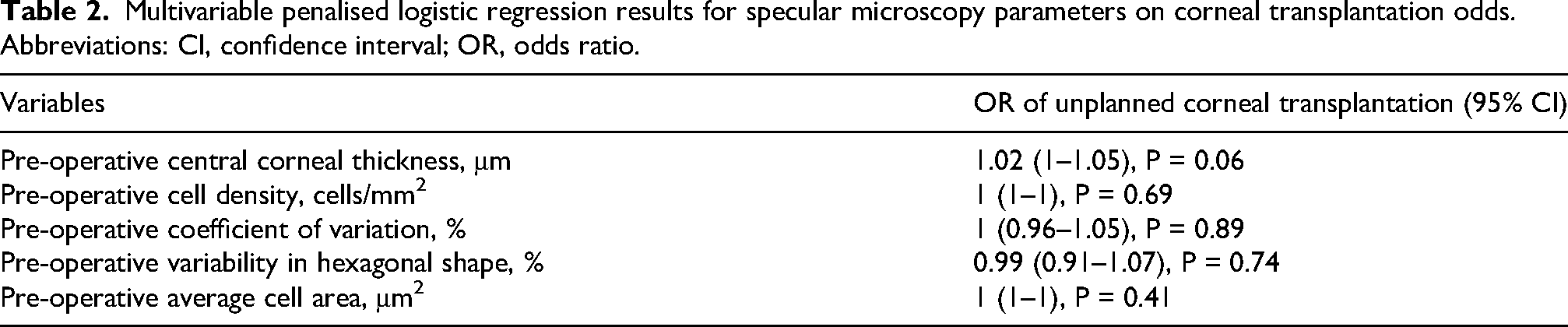
The multivariable penalised logistic regression suggests that preoperative CCT may influence unplanned corneal transplantation, with an odds ratio (OR) of 1.02 per micron increase (95% CI 1.00–1.05, P = 0.06) (Table 2). As the confidence interval includes 1, this finding is not statistically significant, though it hints at possible clinical relevance and warrants further study. The Youden Index identified an optimal preoperative CCT threshold of ≥ 620 μm for predicting transplantation (Figure 1). In contrast, confidence intervals for cell density, coefficient of variation and hexagonality suggest these parameters have negligible or uncertain effects on unplanned transplantation risk (Table 2).
Multivariable penalised logistic regression results for specular microscopy parameters on corneal transplantation odds. Abbreviations: CI, confidence interval; OR, odds ratio.
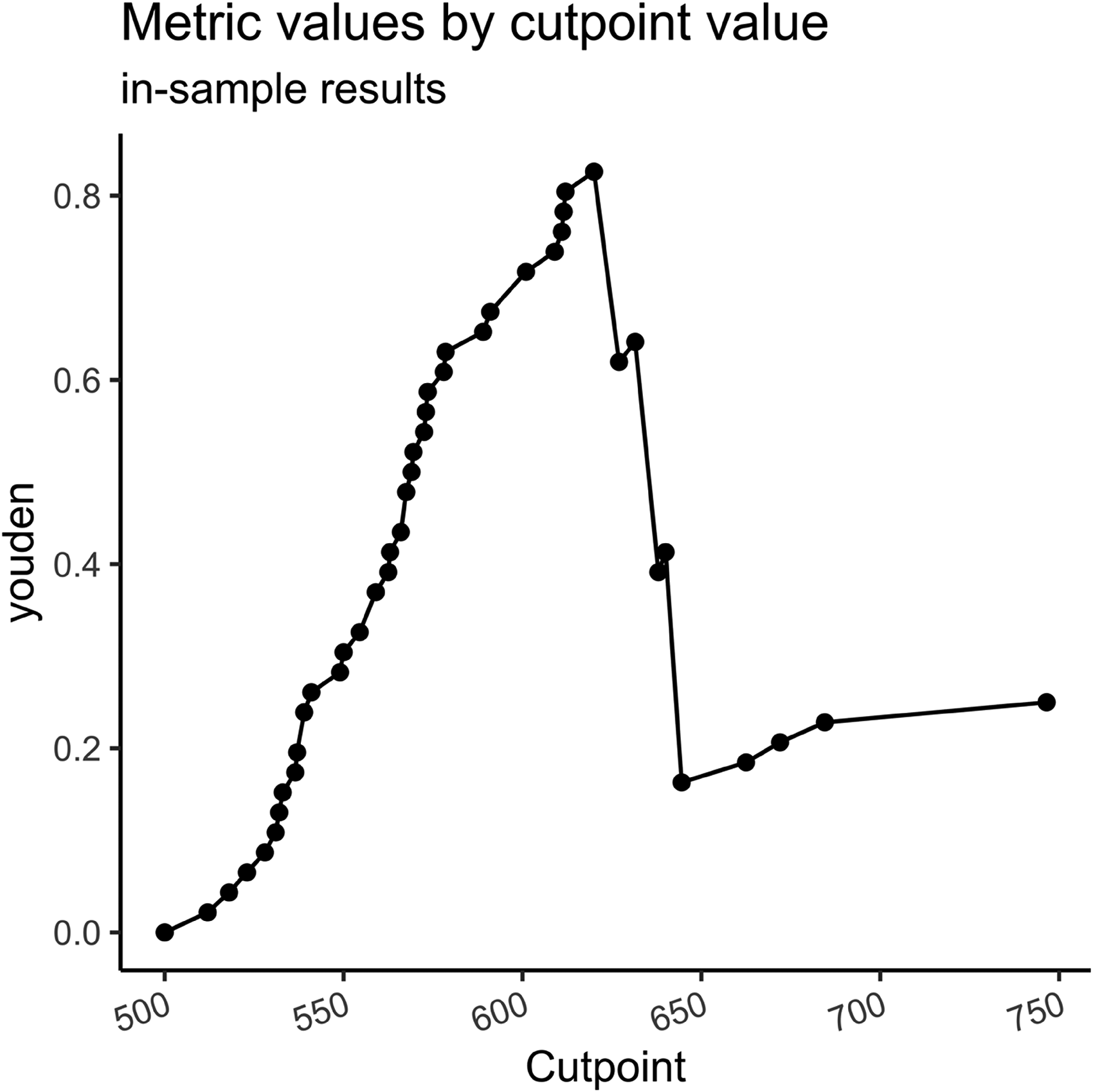
Selection of ‘optimal’ cut-points for preoperative central corneal thickness (CCT) for unplanned corneal transplantation, based on the Youden index. In the final analytic sample of 50 eyes, there were 4 positive and 46 negative cases; the cut-point was 620 μm, with an area under the curve (AUC) of 0.91.
Preoperative specular microscopy and corneal decompensation risk
Preoperative CCT was significantly higher by 40 μm in eyes developing postoperative corneal decompensation/oedema (616 ± 56 μm vs. 576 ± 47 μm, P = 0.049), and preoperative average cell area was also significantly greater (1295 ± 607 μm² vs. 853 ± 402 μm², P = 0.016). Preoperative cell density was lower in the decompensation/oedema group (945.1 ± 481 cells/mm² vs. 1446 ± 647 cells/mm², P = 0.06), but this difference was not statistically significant. Other baseline parameters, including preoperative coefficient of variation (P = 0.95) and variability in hexagonal shape (P = 0.26), showed no significant differences between the two groups (Supplemental Table 1).
Multivariable testing for postoperative corneal decompensation indicated an OR for preoperative CCT of 1.01 (95% CI 0.99–1.03, P = 0.20) per micron. Although the confidence interval overlaps 1, it includes values suggesting a potential positive relationship or no effect, leaving its role inconclusive. The OR for average cell area (1, 95% CI 1–1.01, P = 0.05) suggests a minimal effect with a confidence interval slightly above 1, hinting at a possible association. Other parameters showed no clear or clinically relevant effect (Supplemental Table 2).
Time-to-event analyses
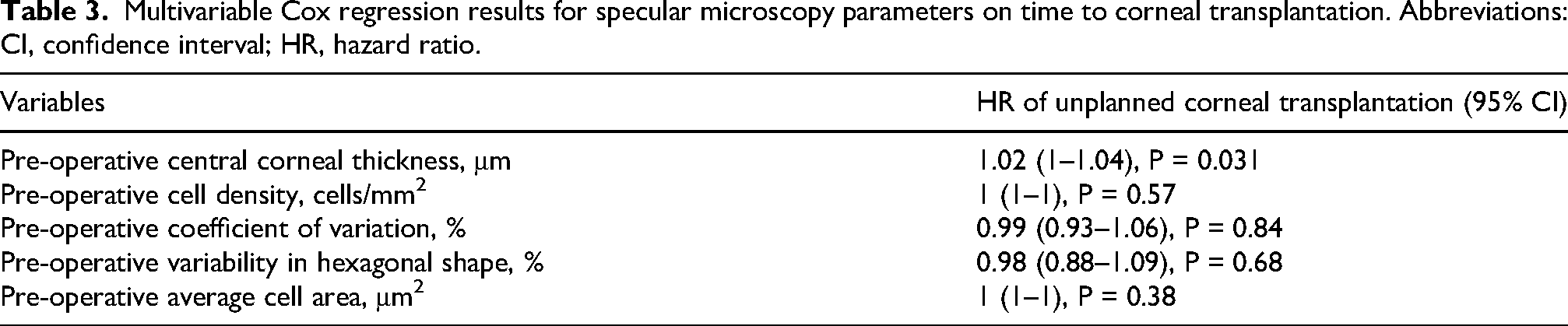
The multivariable Cox regression indicated that higher preoperative CCT was associated with a shorter time to unplanned corneal transplantation, with a hazard ratio (HR) of 1.02 (95% CI 1–1.04, P = 0.031) per micron. The confidence interval suggests a potential positive relationship, though the lower bound at 1 indicates the possibility of no effect cannot be excluded. Proportional hazards testing showed no significant violation of the proportionality assumption (P = 0.45 unadjusted, 0.52 adjusted), indicating that the Cox model is appropriate for the data. The optimal preoperative CCT threshold for this outcome was ≥ 612 μm (Figures 2 and 3). We could not exclude clinically relevant effects on time to transplantation for other specular microscopy parameters (Table 3).
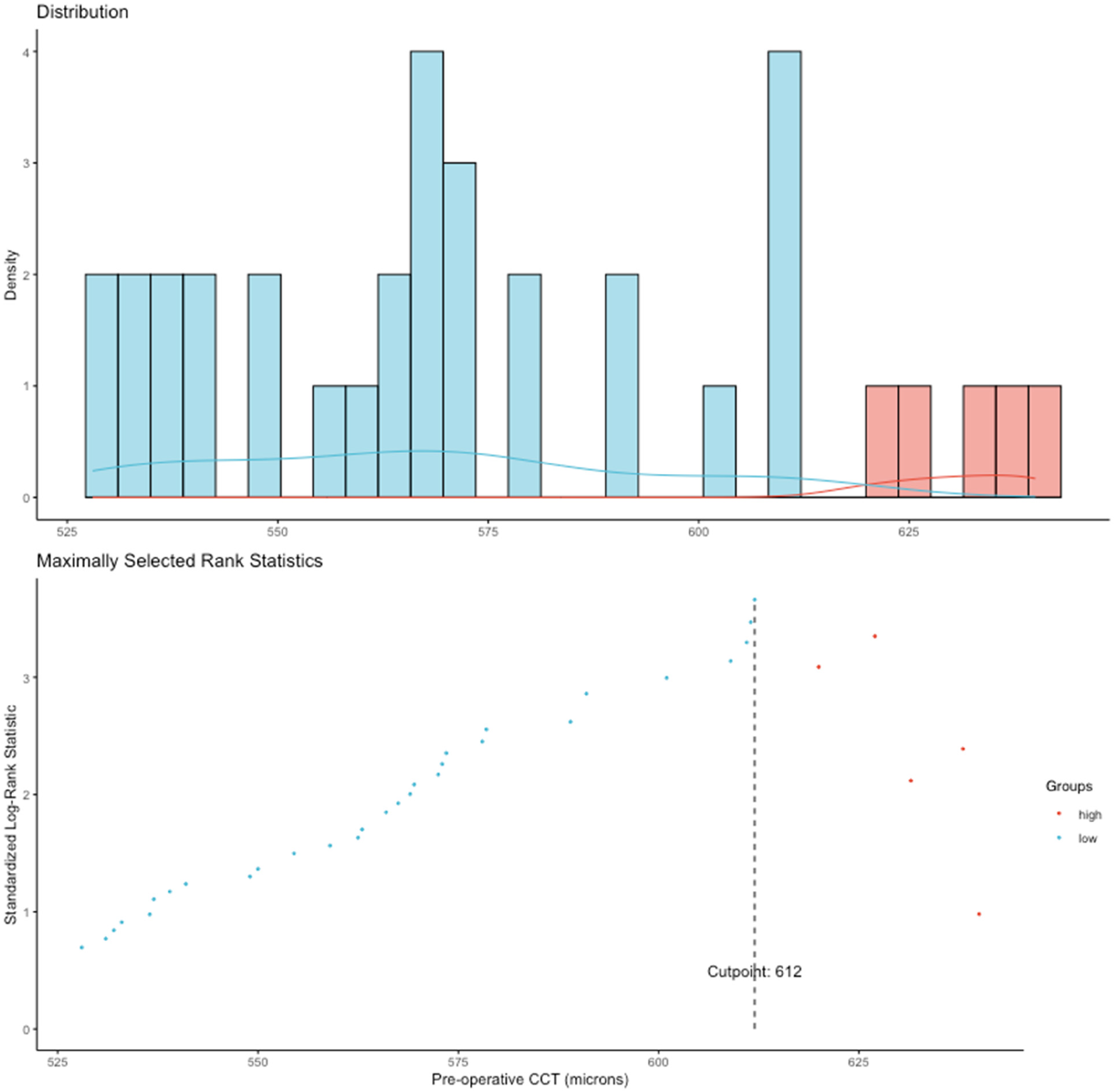
Selection of the ‘optimal' cut-point for preoperative central corneal thickness (CCT) for time to unplanned corneal transplantation in the final analytic sample of 50 eyes, using maximally selected rank statistics. In this sample, the cut-point identified was 612 μm. Abbreviation: CCT, central corneal thickness.
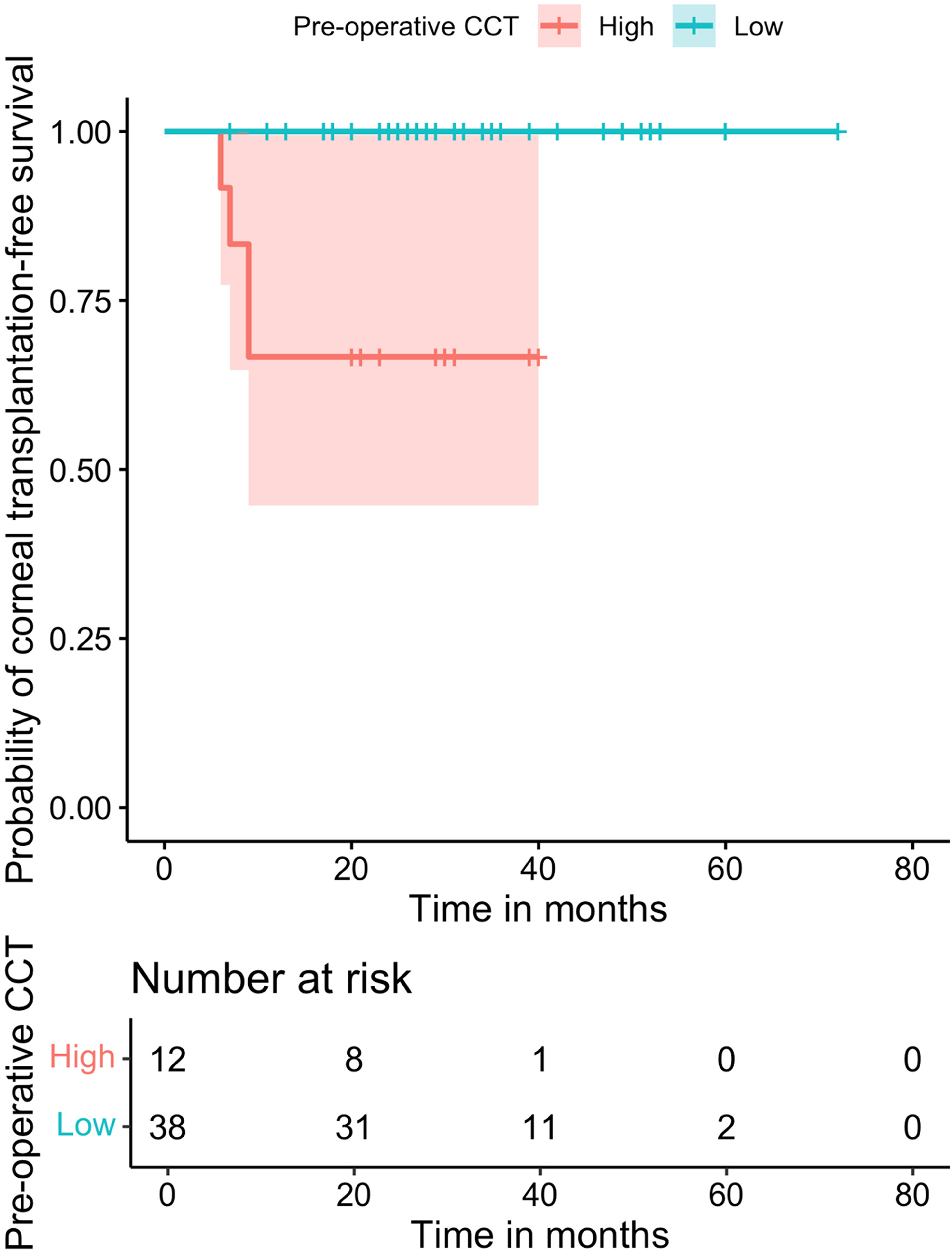
Kaplan-Meier plot of unplanned corneal transplantation-free survival after cataract surgery stratified by the statistically derived preoperative CCT cut-point of 612 μm in the final analytic sample of 50 eyes. The shaded area represents the 95% confidence interval. Abbreviation: CCT, central corneal thickness.
Visual outcomes
Linear regression analyses examining postoperative BCVA with adjustment for preoperative BCVA showed no clear association between baseline and postoperative acuity. In all eyes, the coefficient for preoperative BCVA was 0.14 (95% CI –0.09 to 0.37, P = 0.24) in the model adjusted for baseline acuity only, and 0.10 (95% CI –0.15 to 0.35, P = 0.42) after additional adjustment for age, sex, and preoperative hypertonic saline use. In eyes not requiring corneal transplantation, the corresponding coefficients were 0.10 (95% CI –0.08 to 0.28, P = 0.28) and 0.15 (95% CI –0.05 to 0.35, P = 0.14), respectively.
Discussion
In this single-centre, single-surgeon retrospective cohort, pre-operative CCT exceeding 600 μm was associated with a higher likelihood of time to corneal decompensation requiring endothelial keratoplasty after soft-shell phacoemulsification (HR 1.02 per 1 μm increase, 95% CI 1.00–1.04, P = 0.031), yet the confidence intervals around this hazard and the overall odds of unplanned keratoplasty requirement (OR 1.02, 95% CI 1.00–1.05, P = 0.06) suggest that CCT alone is an imperfect predictor.
CCT is an attractive biomarker because it is quick and inexpensive to measure, and increases with FECD progression even before overt oedema is visible on slit-lamp examination. 15 Our optimal thresholds of 612–620 μm are similar to the 640 μm suggested by Seitzman et al. for choosing isolated cataract surgery over combined cataract extraction and corneal transplantation. 14 In settings without advanced imaging, these thresholds may help risk stratification, but clinicians should interpret CCT in the context of individual patient characteristics and surgical plans. Other parameters, such as ECD and variability in hexagonal shape, showed no consistent association with corneal transplantation or decompensation risk in our study (Tables 2, 3 and Supplemental Table 2).
Multivariable Cox regression results for specular microscopy parameters on time to corneal transplantation. Abbreviations: CI, confidence interval; HR, hazard ratio.
Nevertheless, the predictive power of specular microscopy measurements such as CCT is constrained by physiological diurnal fluctuations and inter-population variability. The thresholds we have identified are therefore likely to vary across studies and populations. The quality of images and data can also vary depending on the corneal location imaged, with factors like corneal oedema and thickened Descemet's membrane further complicating the process. Irregularities such as guttae, a hallmark of FECD visible on slit-lamp through retro-illumination, 16 may be missed in subtle corneal oedema and distort measurements.17,18 Thus, specular microscopy results should be interpreted with caution, especially in advanced FECD, and considered within the broader context of disease progression and surgical outcomes.
Some of these limitations can be overcome using advanced imaging, such as Scheimpflug tomography (Pentacam, Galilei) for generating automated three-dimensional maps of the entire cornea. Features such as loss of parallel isopachs, rapid pachymetric progression, and subtle posterior-surface depression signal subclinical oedema, which correlate with faster FECD progression,19,20can be readily identified. Acquisition is rapid and automated, so complexity is low; the principal barrier to its routine use outside tertiary or referral corneal units remains capital cost. Where tomography is unavailable, referral for Scheimpflug imaging should be considered when pachymetry approaches these thresholds.
Alternatively, in vivo confocal microscopy can be used to provide en face, sub-cellular views of the endothelium, even in oedematous corneas, 21 having been shown to predict the need for endothelial keratoplasty with 63% sensitivity and 94% specificity. 22 Its uptake is limited by operator dependence and inter-user variability, 23 but when available it complements tomography by offering direct endothelial assessment.
Our 8% rate of DSAEK (four of 50 eyes) compares favourably with earlier series,13,22 likely reflecting exclusion of eyes scheduled for keratoplasty and consistent use of the soft-shell technique by a single experienced surgeon. We did not assess intraoperative phacoemulsification energy or cataract severity, and all cases were sequential rather than combined procedures. The relative merits of sequential versus combined cataract surgery and endothelial keratoplasty remain unresolved, with a recent meta-analysis showing no significant outcome differences. 24 Similarly, despite theoretical benefits of femtosecond laser-assisted cataract surgery (FLACS) in reducing endothelial cell loss, its advantage over conventional phacoemulsification remains unresolved.25,26
Limitations of our study include the retrospective design, modest sample size, exclusion of cases lacking good-quality specular data, and absence of formal Krachmer grading of FECD severity and cataract classification. 16 We also lacked phaco-energy metrics, which might confound endothelial outcomes, although the single-surgeon setting reduces procedural heterogeneity.
For clinicians practising without tomography, a CCT exceeding ∼600 μm may trigger frank counselling about the higher chance of postoperative corneal failure requiring combined or sequential endothelial keratoplasty. Prospective multicentre studies that combine oedema and endothelial cell health indices from more advanced imaging techniques can clarify whether a composite score can more accurately stratify FECD eyes before cataract surgery.
Supplemental Material
sj-docx-1-ejo-10.1177_11206721261445518 - Supplemental material for Soft-shell phacoemulsification in Fuchs’ endothelial dystrophy: Central corneal thickness as a predictor of post-operative keratoplasty
Supplemental material, sj-docx-1-ejo-10.1177_11206721261445518 for Soft-shell phacoemulsification in Fuchs’ endothelial dystrophy: Central corneal thickness as a predictor of post-operative keratoplasty by Boon Lin Teh, Nikolaos Tzoumas, Ana Luiza Mylla Boso, Yun Lin Ang, Panagiota Papadakou and Francisco C. Figueiredo in European Journal of Ophthalmology
Supplemental Material
sj-docx-2-ejo-10.1177_11206721261445518 - Supplemental material for Soft-shell phacoemulsification in Fuchs’ endothelial dystrophy: Central corneal thickness as a predictor of post-operative keratoplasty
Supplemental material, sj-docx-2-ejo-10.1177_11206721261445518 for Soft-shell phacoemulsification in Fuchs’ endothelial dystrophy: Central corneal thickness as a predictor of post-operative keratoplasty by Boon Lin Teh, Nikolaos Tzoumas, Ana Luiza Mylla Boso, Yun Lin Ang, Panagiota Papadakou and Francisco C. Figueiredo in European Journal of Ophthalmology
Supplemental Material
sj-docx-3-ejo-10.1177_11206721261445518 - Supplemental material for Soft-shell phacoemulsification in Fuchs’ endothelial dystrophy: Central corneal thickness as a predictor of post-operative keratoplasty
Supplemental material, sj-docx-3-ejo-10.1177_11206721261445518 for Soft-shell phacoemulsification in Fuchs’ endothelial dystrophy: Central corneal thickness as a predictor of post-operative keratoplasty by Boon Lin Teh, Nikolaos Tzoumas, Ana Luiza Mylla Boso, Yun Lin Ang, Panagiota Papadakou and Francisco C. Figueiredo in European Journal of Ophthalmology
Supplemental Material
sj-docx-4-ejo-10.1177_11206721261445518 - Supplemental material for Soft-shell phacoemulsification in Fuchs’ endothelial dystrophy: Central corneal thickness as a predictor of post-operative keratoplasty
Supplemental material, sj-docx-4-ejo-10.1177_11206721261445518 for Soft-shell phacoemulsification in Fuchs’ endothelial dystrophy: Central corneal thickness as a predictor of post-operative keratoplasty by Boon Lin Teh, Nikolaos Tzoumas, Ana Luiza Mylla Boso, Yun Lin Ang, Panagiota Papadakou and Francisco C. Figueiredo in European Journal of Ophthalmology
Footnotes
Acknowledgements
N/A
Ethical considerations
As per UK guidance, data collection is classified as an audit for the purpose of service evaluation, so Institutional Review Board approval and informed consent are not required. However, we obtained approval from the participating Hospital Trust (Project no: 11238) prior to data compilation and analysis, in line with national information governance procedures and adhering to the tenets of the Declaration of Helsinki.
Author contribution statement
Boon Lin Teh and Nikolaos Tzoumas collected, analysed, interpreted data, and drafted the manuscript. Ana Luiza Mylla Boso, Yun Lin Ang, and Panagiota Papadakou collected data. Francisco C. Figueiredo conceived and designed the study, analysed and interpreted data, and revised the manuscript.
Funding
The authors received no direct financial support for the research, authorship, and/or publication of this article. Nikolaos Tzoumas was supported by a National Institute for Health and Care Research (NIHR) Academic Clinical Fellowship (ACF-2021-01-008) and his research was funded in part by the Wellcome Trust (R127002). For the purpose of open access, the author has applied a CC BY public copyright licence to any Author Accepted Manuscript version arising from this submission.
Declaration of conflicting interest
All authors have nothing to disclose.
Data availability statement
The datasets generated and/or analysed during this study are available from the corresponding author upon reasonable request.
Writing assistance and third-party submissions
No medical writing or editorial assistance received during the writing of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.