
Abstract
Purpose
To systematically evaluate retinal and choroidal structural alterations measured by optical coherence tomography (OCT) in individuals with a history of retinopathy of prematurity (ROP) compared with healthy controls, and to identify sources of heterogeneity across studies.
Methods
A PROSPERO-registered systematic review (CRD42023422605) was conducted in accordance with PRISMA guidelines. PubMed, Scopus, and EMBASE were searched from inception through July 26, 2023. Human observational studies reporting OCT-derived retinal or choroidal thickness metrics in ROP with healthy controls were included. Random-effects meta-analyses were performed using standardized mean differences (SMD) and weighted mean differences. Meta-regression and subgroup analyses explored heterogeneity.
Results
Eleven studies (1,019 participants; 351 ROP, 668 controls) were included. Compared with controls, eyes with ROP demonstrated significantly thinner macular ganglion cell–inner plexiform layer (GCIPL) thickness (SMD −1.07; p = 0.002) and thinner superior and temporal perifoveal retina, alongside significantly increased foveal retinal thickness (SMD 1.41; p < 0.0001). No significant difference was observed in subfoveal choroidal thickness. Substantial heterogeneity was present across most outcomes (I2 frequently >75%). Meta-regression identified younger age at imaging as significantly associated with greater foveal thickening (p = 0.002). OCT platform and geographic location also contributed to variability.
Conclusions
Individuals with prior ROP exhibit persistent, layer-specific and region-specific macular alterations consistent with disrupted neurovascular development and foveal hypoplasia. However, substantial methodological heterogeneity limits transportability of thickness-based biomarkers. Standardized, age-aware prospective OCT studies are required before structural metrics can be adopted for clinical risk stratification or longitudinal surveillance.
Introduction
Retinopathy of prematurity (ROP) impacts the maturation of retinal blood vessels in preterm infants, often leading to enduring visual impairment regardless of spontaneous regression or treatment.1,2 ROP is a major contributor to childhood blindness and predisposes patients to increased risk of glaucoma, strabismus, retinal detachment, and cataracts. Although the pathogenesis of ROP is still under investigation, a plausible explanation implicates inappropriate oxygenation of the outer retina which results in the formation of aberrant blood vessels. Classically, ROP occurs in two phases: vaso-obliterative and vaso-proliferative. The vaso-obliterative phase involves vasoconstricting retinal vasculature as a response to oxygen therapy and inadequate development of retinal vessels. The vaso-proliferative phase, vascular endothelial growth factor (VEGF) and insulin-like growth factor-1 (IGF-1) play a role in the development of abnormal and friable blood vessels as a compensation for retinal avascularity. These blood vessels may predispose the infant to sequelae such as vitreous hemorrhage or retinal detachment.3–8
While ROP studies traditionally implicate the retina, 9 emerging evidence suggests that choroidal involvement may play a substantial role in the pathogenesis of ROP. This is attributed to the choroid's crucial function in nourishing the retinal pigment epithelium and photoreceptors, the disruption of which may be responsible for delayed retinal vascularization and ultimately pathologic angiogenesis.10,11
Macular development involves a complex process, with inner retinal cells undergoing centrifugal displacement and photoreceptors experiencing centripetal displacement at an early age. This developmental journey begins around 24 to 26 weeks of age and extends until approximately 4 years of age when foveal development is complete. Premature neonates likely experience disruption in this intricate process, leading to changes in retinal thickness due to disruption of the lateral migration of inner retinal cells.12–14 Early identification of these structural changes may elucidate additional pathologic mechanisms in ROP as well as serve as a bridge to novel therapies and screening tools.
Optical coherence tomography (OCT), an in vivo imaging modality, provides high-resolution images of the cross-sections of the retina and allows for the accurate measurement of the thickness of the retinal and choroidal layers which has been utilized in ocular 15 and systemic diseases. 16 The underlying pathophysiology of ROP and its subtle consequences on visual function in these patients can be better understood by using OCT to detect retinal abnormalities. Recent research on OCT measurements of the retina and choroid in patients with ROP has been promising; however, results have not been consistent. For instance, a study by Fieß et al. demonstrated that subfoveal choroidal thickness (SFCT) in patients with ROP is significantly increased compared to control eyes while studies by Lavric et al. 17 and Ulusoy et al. 18 found decreased SFCT in ROP patients compared to controls. Given the rarity of OCT-based structural data in ROP and the methodological diversity across studies, a systematic review with cautious quantitative synthesis may still provide value by identifying consistent directional trends, sources of heterogeneity, and gaps for future standardized studies.
Methods
This study employed the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) checklist, which aims to enhance the quality of reporting systematic reviews and meta-analyses. The study protocol was created by two authors (SF and SJ), who also registered it with the registration number CRD42023422605 at PROSPERO (the International Prospective Register of Systematic Reviews).
Search strategy
To find relevant studies, we conducted a systematic search of electronic databases such as PubMed, Scopus, and EMBASE between July 26, 2023, and the date of inception. We employed various combinations of keywords associated with “retinopathy of prematurity” and “optical coherence tomography”; Table S1 contains the whole list of search strings that were used for every database. There were no restrictions on the time, language, or place of the literature search. We also manually searched the selected papers’ and reviews’ reference lists to further evaluate relevant research.
Selection criteria
Studies that satisfied the following criteria and evaluated OCT measurements of the retinal layers and choroid in ROP patients with varying degrees of disease severity were included: 1) human observational studies using a cross-sectional, cohort, or case-control design; 2) OCT used to measure the thicknesses of the choroidal and retinal layers; and 3) a minimum of five participants in each study group. The following were excluded from consideration: (1) abstracts from conference proceedings, in vitro, histopathologic, and animal research; (2) lack of a healthy control group; (3) studies unrelated to ROP and OCT. (4) studies not supplying data in the form of standard error (SE) or mean and standard deviation (SD). The research identification and eligibility assessment process were carried out independently by two reviewers (SF and SJ), and any disagreements were resolved via consensus.
Data extraction
A customized database was created by two reviewers (SF and SJ) after they separately extracted the following information from the included studies: first author, publication date, study location, study design, eye selection method (i.e., choosing one or both subjects’ eyes for analysis), model of OCT applied, inclusion and exclusion criteria for study participants, characteristics of study groups including sample size, male percentage, mean age, mean intraocular pressure (IOP), refractive error (in Diopters), axial length, best corrected visual acuity, and reported OCT metrics of retina and choroid. Where available, OCT acquisition parameters, including scan protocols, segmentation definitions, and measurement regions, were extracted; however, reporting of these parameters was inconsistent across studies, limiting the ability to harmonize measurements across cohorts. Data extraction criteria were determined a priori and consensus between reviewers resolved any ambiguities on data extraction.
Quality assessment
For case-control and cohort studies, the Newcastle-Ottawa scale (NOS), which has been validated by the Cochrane Handbook, was employed as a measure for quality assessment.19,20 NOS assesses research in three quality domains: selection, comparability of case and control groups, and exposure for case-control studies and outcome for cohort studies with the highest values of eight and nine, respectively. The quality of the research was evaluated independently by two writers (SF and SJ), and differences were settled through consensus.
Statistical analysis
Stata version 16 (StataCorp, College Station, TX) was used to conduct a meta-analysis on every OCT metric that was published in three or more different publications. Hedges’ g was used to compute the weighted mean difference (WMD) and standardized mean difference (SMD), which were used to report the degree of difference between the compared groups along with the associated 95% confidence interval (CI). Given anticipated clinical and methodological diversity across studies, random-effects models were used throughout to provide conservative estimates that account for between-study variability, regardless of I2 magnitude 20 Additionally, the funnel plot and Egger's test were utilized to detect potential publication bias. In the event of publication bias, the trim-and-fill technique was employed to modify the effect size for the bias discovered.21,22 Given the small number of studies per outcome, publication bias assessments were considered exploratory and interpreted with caution. Similarly, subgroup analyses and meta-regression were performed to investigate potential sources of heterogeneity; however, these analyses are inherently underpowered and should be interpreted cautiously, particularly in the context of multiple tested variables and limited study-level data. A statistically significant p-value was defined as one that was less than 0.05.
Results
The 11 studies included in the qualitative synthesis were identified through the screening procedure. 861 studies were found through the main literature search, including 266 articles from PubMed, 329 articles from Embase, and 446 items from Scopus. 465 items were excluded by human and automatic duplication elimination. 346 studies were excluded during the first round of the research selection process based on the aforementioned selection criteria. 39 studies were excluded because the whole text was not available, there were no healthy controls, and other reasons, as shown in Figure 1. Ultimately, 11 articles totaling 351 cases and 668 controls were included in the current meta-analysis. Table S2 depicts the primary characteristics of all the included studies. Of the 11 included studies in this meta-analysis, 3 measured average macular ganglion cell-inner plexiform (GCIPL) layer thickness,23–25 4 measured subfoveal choroidal thickness,17,18,26,27 7 measured foveal retinal thickness (RT),18,24,25,28–31 4 measured the average parafoveal RT,24,28,30,31 3 measured average perifoveal RT,28,30,31 and 3 measured superior, inferior, temporal and nasal parafoveal and perifoveal RT24,28,29 in patients with ROP vs. healthy controls.
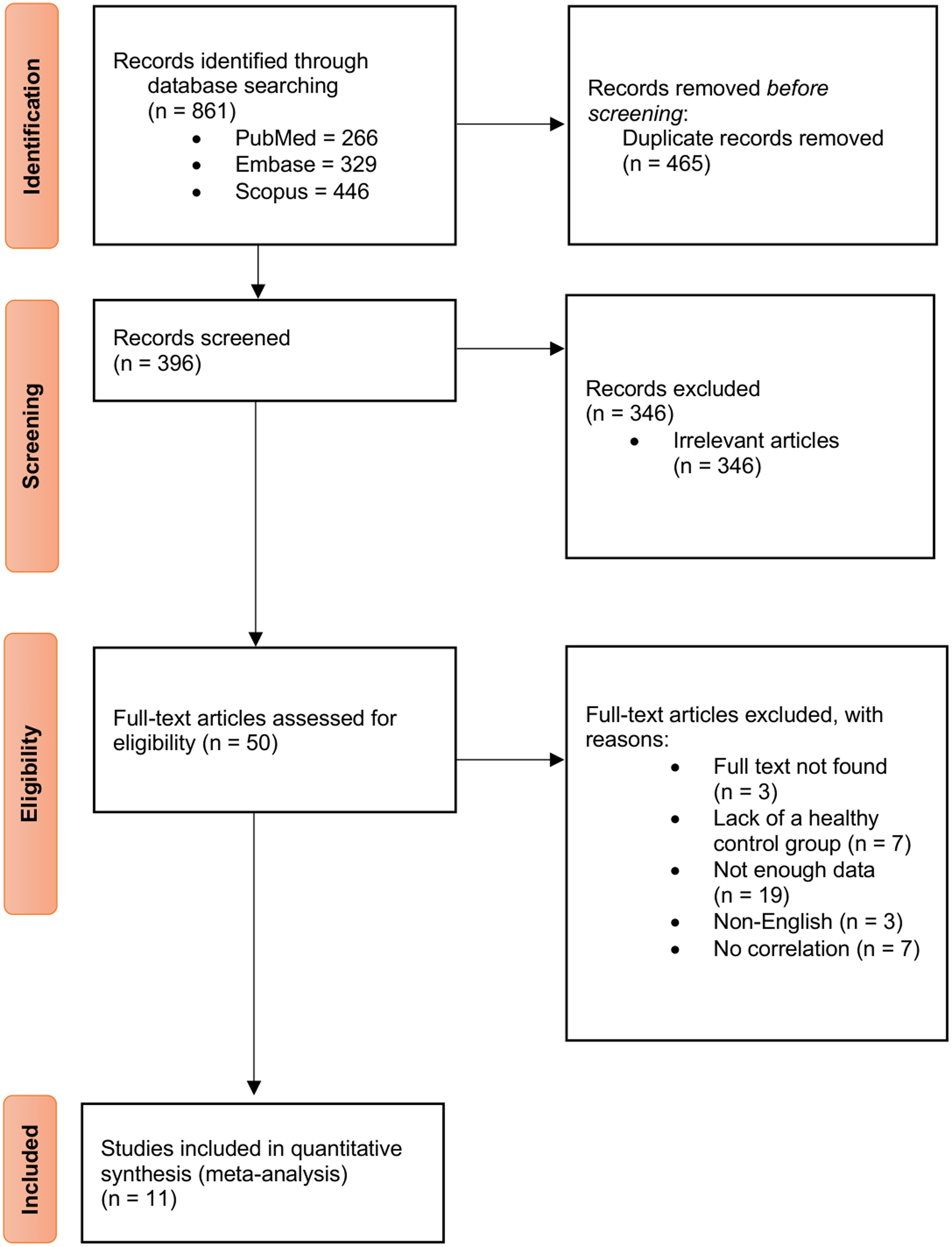
Flowchart of the study selection process.
All the studies reported their data in a mean ± SD format. One study matched their participants in terms of both age and sex, 18 while fives studies matched the ROP and control groups according to age17,27–30 and five studies did not match under any criteria.23–26,31 Six studies performed OCT measurements on a participant's single eye,23–25,27–29 while the remaining five studies examined both participant's eyes. OCT with Heidelberg Spectralis was used in five studies,26,27,29–31 Zeiss Cirrus HD-OCT was used in three studies,23–25 Optovue RTVue OCT was used in two studies and DRI OCT Triton was used in the remaining one study17,18,28 (Table S2). Three investigations were carried out in Germany, and the remaining studies were done in Hungary, Japan, Turkey, Taiwan, South Korea, Spain, and Slovenia. Across most outcomes, substantial heterogeneity was observed (I2 often >75%), indicating marked variability in effect sizes across studies.
Average macular GCIPL thickness
Three studies evaluating GCIPL thickness in 217 control eyes and 80 ROP eyes were evaluated in this meta-analysis.23–25 Patients with ROP demonstrated a substantial reduction in the average macular GCIPL thickness (SMD, −1.07; 95% CI, −1.78 to −0.37; p = 0.002; I2 = 82.22%) and an absolute decrease of 10.33 µm (95% CI, −17.41 to −3.25; p = 0.003; Table 1) compared to healthy controls.
Differences in OCT measurements between ROP patients and controls.
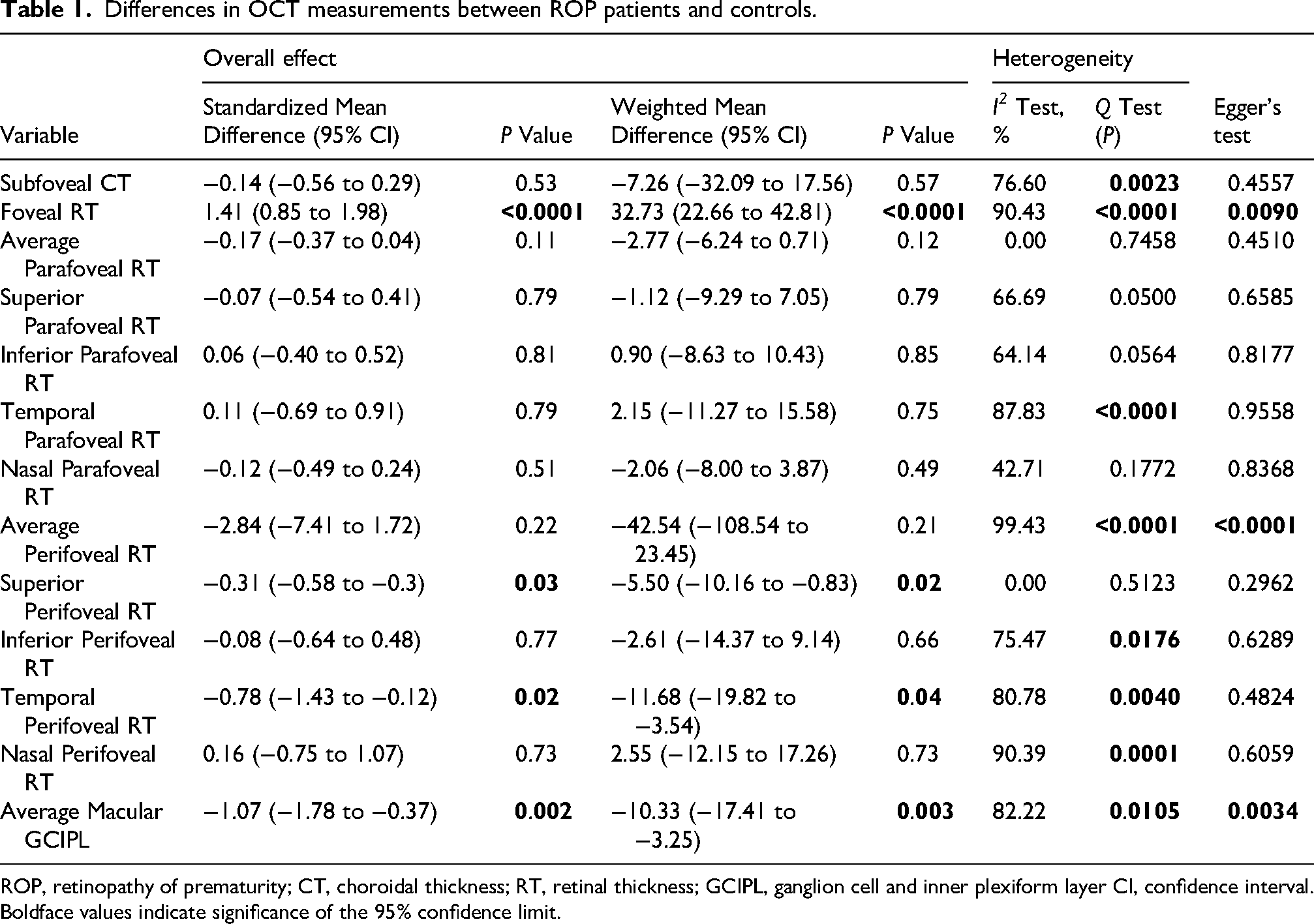
ROP, retinopathy of prematurity; CT, choroidal thickness; RT, retinal thickness; GCIPL, ganglion cell and inner plexiform layer CI, confidence interval.
Boldface values indicate significance of the 95% confidence limit.
Subfoveal choroidal thickness
Four studies evaluating the thickness of the subfoveal choroid in 384 control eyes and 163 ROP eyes were evaluated.17,18,26,27 These studies’ analysis revealed that there was not a significant difference in subfoveal choroidal thickness (SFCT) between ROP patients and control subjects. (SMD, −0.14; 95% CI, −0.56 to 0.29; p = 0.53; I2 = 76.60%; Figure S1).
Foveal retinal thickness
Seven studies reported foveal retinal thickness (FRT) in 216 ROP eyes and 790 control eyes.24–26,28–31 When comparing the FRT of ROP patients to healthy controls, there was a significant increase (SMD, 1.41; 95% CI, 0.85 to 1.98; p < 0.0001; I2 = 90.43%; Figure S2), which is consistent with an absolute increase of 32.73 µm (95% CI, 2.66 to 42.81 µm; p < 0.0001; Table 1).
Average parafoveal and perifoveal retinal thickness
Four studies reported the average parafoveal retinal thickness (RT) with a total of 123 ROP subjects and 379 healthy controls24,28,30,31 and three studies reported the average perifoveal RT with a total of 99 ROP subjects and 319 healthy controls.28,30,31 The average parafoveal and perifoveal RT in ROP patients did not differ significantly from control subjects (SMD, −0.17; 95% CI, −0.37 to 0.04; p = 0.11; I2 = 0.0%) and (SMD, −2.84; 95% CI, −7.41 to 1.72; p = 0.22; I2 = 99.43%) when compared with healthy individuals, respectively.
Superior, Inferior, nasal, and temporal parafoveal retinal thickness
We identified three studies reporting the four quadrants of the parafoveal RT in 74 ROP patients and 163 patients in the control group.24,28,29 RTs of ROP cases in these regions did not significantly differ from controls: temporal (SMD, 0.11; 95% CI, −0.69 to 0.91; p = 0.79; I2 = 64.14%), superior (SMD, −0.07; 95% CI, −0.54 to 0.41; p = 0.79; I2 = 66.69%), inferior (SMD, 0.06; 95% CI, −0.40 to 0.52; p = 0.81; I2 = 64.14%), and nasal (SMD, −0.12; 95% CI, −0.49 to 0.24; p = 0.51; I2 = 42.71%)
Superior, Inferior, nasal, and temporal perifoveal retinal thickness
The same three studies reported the four quadrants of the perifoveal RT on the same 74 ROP patients and 163 control group patients.24,28,29 The analysis revealed that RT in the superior and temporal regions of individuals with ROP differed significantly compared to the control group. In the superior region, the SMD was −0.31 (95% CI, −0.58 to −0.03; p = 0.03; I2 = 0.0%). In the temporal region, the SMD was −0.78 (95% CI, −1.43 to −0.12; p = 0.02; I2 = 80.78%). Additionally, there was an absolute difference of −5.5 µm (95% CI, −10.16 to −0.83 µm; p = 0.02) and −11.68 µm (95% CI, −19.82 to −3.54 µm; p = 0.02) in the superior and temporal regions, respectively (Table 1). However, there was no statistically significant difference between ROP patients and controls in RT of the nasal and inferior perifoveal regions (SMD, 0.16; 95% CI, −0.75 to 1.07; p = 0.73; I2 = 90.39%), and inferior (SMD, −0.08; 95% CI, −0.64 to 0.48; p = 0.77; I2 = 75.47%).
Meta-regression
We conducted a univariate meta-regression analysis on seven studies24–26,28–31 that assessed the thickness of the foveal retina in participants with ROP and healthy individuals. The effect size of foveal retinal thickness analysis showed a significant negative association with the average age of individuals with ROP, as indicated in Table S3 (β, −0.0730198; p = 0.002). Nevertheless, there was no statistically significant link (p > 0.05) between the male percentage of participants, sample size, mean birth weight, mean gestational age, mean axial length (AL), and mean best corrected visual acuity (BCVA) of cases and the effect sizes of the analyses mentioned above.
Subgroup analysis
OCT model
An analysis of the variables mentioned above regarding the OCT device, comparing ROP subjects and controls, found that studies using the Carl Zeiss Meditec OCT (p < 0.0001), Heidelberg Spectralis OCT (p = 0.03), and Optovue RTVue OCT (p = 0.01) showed significantly higher values for foveal RT, which aligns with the overall findings. The information on the results of subgroup analysis based on matching cases and controls and the OCT model is available in Table S4.
Eye selection technique
Upon analyzing the studies, it was shown that regardless of whether they used a single-eye or both-eyes selection approach, there was a notable and statistically significant rise in the thickness of the foveal retinal layer across all datasets. The information is available in Table S4.
Location
The analysis showed that the increase in foveal retinal thickness was significant in studies conducted in Asia (p = 0.003), but not in Europe. The information is available in Table S4.
Sensitivity analysis
We conducted a sensitivity analysis on all factors. We systematically excluded each article individually to examine whether a particular study was responsible for the significant variation in results. The heterogeneity and effect sizes exhibited considerable alterations compared to the primary study across many parameters. The studies yielded diverse causes of heterogeneity in different variables, as shown in Table S5.
Publication bias
Publication bias assessments were exploratory given the small number of studies per outcome. Funnel plot asymmetry and Egger's test suggested small-study effects for several outcomes; however, trim-and-fill analyses did not materially change pooled estimates for foveal RT, GCIPL, or perifoveal RT, and these findings should be interpreted cautiously.
Quality assessment
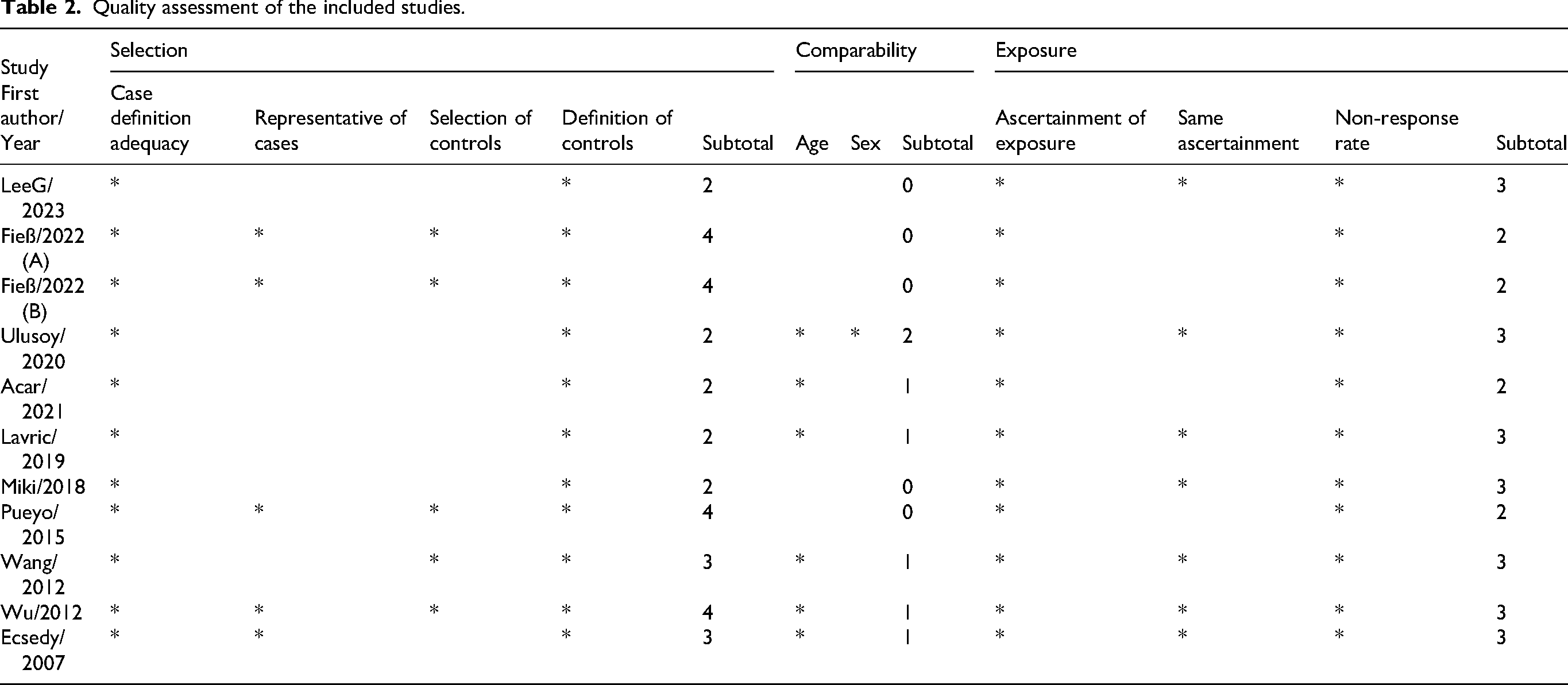
We assessed the quality of the studies included by using the NOS for both case-control and cohort studies. Table 2 illustrates that most case-control studies achieved satisfactory to excellent grades (ranging from 5 - 8 out of 9) when assessed in terms of selection, comparability, and exposure. All case-control studies achieved the highest level of quality in the domain of exposure. The studies utilizing the cohort design obtained specific information regarding their selection, comparability, and outcome scores.
Quality assessment of the included studies.
Discussion
To the best of our knowledge, this is the first systematic review and meta-analysis assessing the structural differences between individuals with a history of ROP and healthy controls. The results of the current meta-analysis revealed that cases with ROP had significantly thinner macular GCIPL and superior and temporal perifoveal retina, but thicker foveal retina compared to healthy controls. Moreover, additional analysis showed that variables like the mean age of patients with ROP, type of OCT model, and study location had significant confounding influences on estimated differences detected in foveal retinal thickness.
Mechanistically, the OCT phenotype in ROP should be interpreted as the structural footprint of a disrupted neurovascular developmental program. ROP is classically described as a biphasic disease: an early hyperoxia-driven phase characterized by vaso-attenuation and delayed physiologic vascular growth, followed by a later relative-hypoxia phase that induces VEGF- and IGF-1–modulated pathologic angiogenesis. 9 Beyond vasculature, these oxygen and growth-factor perturbations occur during a critical window of macular maturation when the fovea normally undergoes centrifugal displacement of inner retinal layers and centripetal packing/elongation of cone photoreceptors.12–14 Premature birth and ROP-associated dysregulation can therefore plausibly produce persistent inner retinal tissue at the foveal center (reduced excavation) and altered layer-specific trajectories that remain detectable years later on OCT.28,31,36,37 Our pooled results, greater foveal retinal thickness with concurrent thinning of macular GCIPL and selective superior/temporal perifoveal thinning, are consistent with this developmental-disruption model. Increased foveal thickness in ROP is often interpreted as foveal hypoplasia or incomplete inner retinal migration, yielding a “thicker” central fovea driven by persistence of inner retinal elements rather than true hypertrophy. In parallel, reduced GCIPL thickness may reflect either (i) neurodevelopmental vulnerability of retinal ganglion cells/inner plexiform circuitry in the context of early-life oxygenation stress and neurovascular uncoupling, and/or (ii) downstream effects of treatment exposure (e.g., laser) and disease severity, which may differ substantially across cohorts. The regional perifoveal findings (superior/temporal thinning) may represent differential susceptibility of macular subregions to developmental vascular insufficiency and/or later-life remodeling, but these quadrant effects should be interpreted conservatively given the small number of studies and the sensitivity of regional thickness to segmentation conventions and ocular biometry.
Although our meta-analysis did not identify a consistent difference in SFCT, this should not be interpreted as excluding choroidal involvement in ROP. The choroid is the principal oxygen supply to the outer retina, and early-life oxygen dysregulation may alter choroidal development; however, SFCT is highly variable and strongly confounded by age, axial length, refractive error, imaging protocol, and diurnal/systemic factors, sources of variability that differed substantially across included studies. Therefore, the null pooled result likely reflects biologic and measurement heterogeneity rather than absence of a choroidal contribution. Future work integrating structural OCT with OCTA-derived choroidal and retinal perfusion measures may yield more mechanistically informative biomarkers than thickness alone.33–35
Concomitant with our pooled estimate, most included studies reported thinner GCIPL in individuals with ROP compared with controls. GCIPL thinning may reflect inner retinal neurodevelopmental vulnerability in the setting of early-life oxygen dysregulation and altered neurovascular signaling, but it may also be influenced by disease severity and treatment exposure (e.g., laser), which were inconsistently reported across cohorts. 23 Notably, GCIPL alterations are not specific to ROP; prematurity and impaired fetal growth alone have been associated with thinner GCIPL and smaller intracranial volumes, suggesting that some of the inner retinal signal may reflect broader neurodevelopmental context rather than ROP-specific injury. 24 The conflicting directionality reported in some cohorts, particularly those comparing treated ROP to preterm controls, highlights that the observed GCIPL phenotype likely integrates prematurity, ROP severity, and treatment effects, underscoring the need for stratified analyses in standardized prospective datasets. 32
In individuals born preterm, the central foveal retinal thickness increases as gestational age decreases. Foveal hypoplasia, a condition characterized by underdevelopment of the fovea, is associated with prematurity and advanced stages of ROP requiring treatment. 31 Foveal microvascular anomalies are identified in children with ROP, regardless of the treatment option or spontaneous regression. Extreme prematurity without ROP is associated with increased foveal retinal thickness at the foveal center and reduced foveal depth compared to full-term controls.36,37 In line with the results of our analysis revealing a significant thickening in the foveal retina of ROP cases, one of the included studies examining macular volume in preterm children found an increase in the central retinal region, while the foveal depression decreased compared to full-term children. 30 This suggests that the preservation of the inner retina may play a role in the unusual foveal morphology observed in individuals with a history of ROP. In practical terms, the most biologically coherent interpretation is that increased foveal thickness in ROP reflects incomplete inner retinal centrifugal migration (a foveal hypoplasia spectrum), rather than a generalized increase in retinal tissue. Additionally, retinal laser photocoagulation has the potential to cause axonal injury, which may initially appear as a short-term increase in the thickness of the RNFL, but over time, can lead to gradual thinning of the RNFL. 38 Furthermore, the only significant alterations found in our conducted analyses of parafoveal and perifoveal regions were the thinning of the superior and temporal perifoveal retina in the patients with ROP compared to healthy controls. Several mechanisms could contribute to quadrant-specific perifoveal differences, including regional variation in developmental vascular supply and later-life remodeling.39,40 However, given the small number of studies and substantial dependence of quadrant thickness on segmentation algorithms, scan centration, ocular magnification (axial length/refractive status), and ring-definition conventions across devices, these regional findings should be treated as hypothesis-generating until replicated using harmonized acquisition and analysis pipelines. 41
Exploring possible confounders, meta-regression indicated that the effect sizes of differences observed in foveal retinal thickness were inversely associated with the mean age of ROP patients. Previous evidence also suggests that foveal retinal thickness is subject to age-related influences as differences are observed across various age groups. In younger individuals, specifically those between the ages of 6 and 17, foveal retinal thickness demonstrates an increase as age progresses. 42 However, in the case of adults, the connection between foveal retinal thickness and age becomes more intricate. Certain studies have documented a decline in inner retinal layer thickness with advancing age while the thickness of the outer retinal layer remains relatively stable. 43 Additionally, other studies have uncovered a reduction in total retinal thickness concerning age that shows that the most significant decline occurs after the age of 52. 44 Moreover, it has been reported that in the case of children who are born very preterm, there is a positive correlation between decreasing gestational age and an increase in foveal minimum thickness. 45 These findings underscore the significance of accounting for age-related changes when comparing foveal retinal thickness in patients with ROP vs. healthy controls.
The main contribution of this meta-analysis is not only the directionality of individual OCT metrics, but the demonstration that structural signals in ROP are layer-specific (GCIPL) and region-specific (perifoveal quadrants) while foveal thickness shows large context dependence. The meta-regression and subgroup findings indicate that age at imaging, device platform, and geography explain a meaningful portion of between-study variability, implying that unadjusted thickness comparisons across cohorts are likely to produce apparently contradictory conclusions. This provides a concrete roadmap for the field: (i) adopt age-aware reporting and analysis windows; (ii) prespecify device-specific segmentation and ring definitions or perform cross-device harmonization; and (iii) stratify by prematurity metrics, ROP severity, and treatment modality. Without these steps, thickness-based OCT biomarkers risk being non-transportable across NICUs and follow-up clinics. An additional source of heterogeneity is variation in population characteristics across studies, including prematurity profiles, ROP severity, and treatment history (treated vs. spontaneously regressed). These factors likely have distinct effects on retinal development and OCT metrics. In particular, treatment exposure and disease severity may differentially impact inner retinal layers and foveal morphology. The lack of stratified analyses due to inconsistent reporting limits causal interpretability and may confound pooled estimates, especially for foveal thickness and GCIPL. Therefore, findings should be interpreted as aggregate signals across heterogeneous phenotypes rather than effects of a specific ROP subtype.
Despite efforts made in this systematic review and meta-analysis to address interstudy heterogeneity and potential confounders, several limitations must be acknowledged. A central limitation is the substantial between-study heterogeneity observed across most outcomes, which constrains the interpretability and generalizability of pooled estimates. This heterogeneity is likely driven by differences in OCT devices, segmentation algorithms, and measurement protocols, as well as variability in age at imaging and underlying clinical characteristics. In particular, included studies varied in terms of prematurity profiles, ROP severity, and treatment status, and the lack of stratified analyses based on these factors may confound the interpretation of structural outcomes. Additionally, variability in control group matching (e.g., age and sex) and differences in eye selection methods (single-eye vs. both-eyes inclusion), with limited reporting of adjustments for inter-eye correlation, may introduce bias and affect variance estimates. Subgroup analyses suggested that OCT model and study location significantly influenced foveal thickness estimates, further underscoring the need for standardized methodologies across diverse populations. Moreover, the measured thickness of ocular layers such as the choroid is dynamically influenced by multiple factors, making it highly susceptible to variability. 46 The potential impact of wearing glasses during follow-up visits may also affect the outcomes. 47 Additionally, patients with poor vision could not be reliably imaged with OCT, and those with developmental delays might not be able to undergo OCT, introducing a selection bias as the results are based on cases where OCT was feasible. The lack of OCTA-based vascular assessment also limits mechanistic interpretation and should be addressed in future studies. Although some studies matched for age and sex, other confounders such as timing of OCT acquisition were inconsistently reported. 48 Finally, insufficiently detailed reporting of treatment modalities prevented stratified analyses, and future longitudinal studies incorporating well-defined subgroups (e.g., spontaneously regressed, anti-VEGF–treated, laser-treated) are warranted. 48
Conclusion
Available OCT studies suggest altered macular development in individuals with a history of ROP, characterized by relative foveal thickening and selective inner retinal thinning. However, substantial heterogeneity and methodological variability limit the interpretability and generalizability of pooled estimates, and findings should be interpreted as directional rather than definitive. Future prospective studies using standardized imaging protocols and age-stratified designs are needed before OCT metrics can be adopted as reliable biomarkers in ROP.
Footnotes
Ethical considerations
This study was a systematic review and meta-analysis of published data and did not require institutional review board approval.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
All data analyzed in this study are derived from previously published articles cited in the manuscript.