
Abstract
Purpose
To evaluate adverse events (AEs) associated with teprotumumab in the reatment of thyroid eye disease (TED).
Methods
Reports involving teprotumumab were extracted from the U.S.FDA Adverse Event Reporting System (FAERS) from the first quarter of 2020 to the first quarter of 2025. After data standardization, disproportionality analyses were performed using multiple signal detection algorithms, including the Reporting Odds Ratio (ROR), Proportional Reporting Ratio (PRR), Bayesian Confidence Propagation Neural Network (BCPNN), and Empirical Bayesian Geometric Mean (EBGM).
Results
A total of 1,357 reports were identified. Detected signals at the system organ class (SOC) level included ear and labyrinth disorders, eye disorders, social circumstances and reproductive system and breast disorders. A total of 143 Preferred Terms (PTs) met the criteria of four algorithms. Among these, signals within the “Ear and labyrinth disorders” SOC were predominant (n = 598). Tinnitus was the most frequently reported PT (n = 146). The highest disproportionality signals, based on ROR values, were observed for permanent deafness (ROR 10,021.8; 95% CI 5,544.31–18,115.24), autophony (ROR 3,282.12; 95% CI 1,333.19–8,080.12), and patulous eustachian tube (ROR 1,401.68;95% CI 499.54–3,932.99).
Conclusion
These findings provide important real-world safety evidence and may support safer clinical use of teprotumumab.
Introduction
Thyroid eye disease (TED) is an autoimmune inflammatory orbital disorder closely associated with thyroid dysfunction and characterized by unilateral or bilateral eyelid edema, conjunctival injection, chemosis, proptosis, diplopia and strabismus.1,2 TED also imposes psychosocial distress and substantial socioeconomic burdens due to its disfiguring effects and chronic disease course.1,3 Epidemiological studies identify TED as the most common orbital disease in adults. 3 Notably, approximately 26% of newly diagnosed Graves’ disease patients develop TED, underscoring its clinical significance in endocrine-ophthalmic comorbidities. 4 Current management strategies emphasize a multidimensional evaluation that integrate disease activity, severity, and quality of life metrics to guide therapeutic decision-making.5,6
Emerging insights into TED pathogenesis have identified insulin-like growth factor 1 receptor (IGF-1R), a transmembrane tyrosine kinase receptor, as a key mediator of disease progression. Orbital fibroblasts (OFs) from TED patients exhibit IGF-1R overexpression, and receptor activation promotes interleukin-16 (IL-16) secretion, chemokine upregulation, and hyaluronan synthesis, thereby contributing to promotes adipogenesis and tissue expansion.7,8 Additionally, elevated orbital IGF-1 levels exacerbate hyaluronan deposition, which in turn increases tissue edema through osmotic water retention. 9 Concurrently, IGF-1R overexpression in T and B lymphocytes stimulates proinflammatory cytokine cascades (IL-6, IL-8, TNF-α), thereby perpetuating orbital inflammation and tissue remodeling. 7 Recent mechanistic studies also demonstrate functional crosstalk between IGF-1R and the thyroid-stimulating hormone receptor (TSHR) via signalosome formation, providing a molecular basis for therapeutic intervention.10–12
Therapeutic targeting of this pathway has been realized through teprotumumab, a 148 kDa recombinant human IgG1κ monoclonal antibody approved by the U.S. Food and Drug Administration (FDA) in January 2020 for active moderate-to-severe TED. This biologic agent exerts dual mechanisms: high-affinity binding to the cysteine-rich domain of IGF-1R α-subunit induces receptor internalization and degradation, while multimodal modulation of OFs downregulates surface IGF-1R/TSHR expression and suppresses TSH-dependent inflammatory mediator production.13,14 With teprotumumab approaching five years of post-marketing clinical use by 2025, systematic evaluation of its real-world safety profile becomes imperative. Despite its therapeutic promise, pharmacovigilance data remain limited, necessitating robust analysis of spontaneous adverse event reports.
The FDA Adverse Event Reporting System (FAERS) is a key global pharmacovigilance database that compiles drug safety reports, medication errors, and product quality complaints.This study uses FAERS data to conduct a systematic disproportionality analysis of teprotumumab to identify potential adverse drug reaction (ADR) signals and assess their clinical relevance and impact.
Methods
Data source
Using “teprotumumab” and its trade name “TEPEZZA” as search terms in the U.S. FAERS database, we extracted reports related to teprotumumab from the first quarter of 2020 to the first quarter of 2025. Seven data tables were obtained, including demographic and administrative information (DEMO), adverse reaction events (REAC), drug information (DRUG), patient outcomes (OUTC), reporting sources (RPSR), drug therapy timing (THER), and indications (INDI). Together, these tables provide essential information, including patient demographics, medication details, and specific adverse event manifestations. All seven tables were linked by a unique PRIMARYID. Ethical approval and informed consent were waived due to the anonymized nature of the publicly available data.
Data cleaning
Following FDA data management guidelines, duplicate records were systematically removed through a hierarchical selection process. For entries sharing identical CASEID, priority was assigned to records with the most recent FDA_DT timestamp. When both CASEID and FDA_DT were identical, the record with the highest PRIMARYID was retained.
The temporal relationship between treatment and adverse event onset was established through chronological validation of START_DT (treatment initiation) and EVENT_DT (adverse event onset). Temporal discordance cases (EVENT_DT ≤ START_DT) were rigorously excluded during data quality assessment, along with entries containing incomplete temporal markers or identifiable input inaccuracies.
To ensure report reliability, only healthcare professional-submitted reports (including physicians, pharmacists, and other healthcare professionals) were retained.
Data standardization
Adverse event (AE) data were standardized using the Medical Dictionary for Regulatory Activities (MedDRA), version 26.1. MedDRA is a globally standardized medical terminology developed by the International Council for Harmonisation (ICH). Its structure comprises five hierarchical levels, from the most general to the most specific: System Organ Class (SOC), High-Level Group Term (HLGT), High-Level Term (HLT), Preferred Term (PT), and Lowest Level Term (LLT). 15
For the mining and analysis of AEs, this study employed PT—the most commonly used level for standardizing specific medical concepts, and SOC to identify the involved organ system.
Data mining
This study aimed to identify teprotumumabassociated AEs through disproportionality-based signal detection. Disproportionality analysis identifies potential drug-event associations by quantifying discrepancies between observed and expected reporting frequencies in the database. These analyses are based on 2 × 2 contingency tables used to determine whether reporting associations are disproportionately high. We applied four disproportionality algorithms: Reporting Odds Ratio (ROR), Proportional Reporting Ratio (PRR), Bayesian Confidence Propagation Neural Network (BCPNN), and Empirical Bayesian Geometric Mean (EBGM). 16 The calculation formulas and signal detection criteria were shown in Table 1.
Principle of dis-proportionality measure and standard of signal detection.
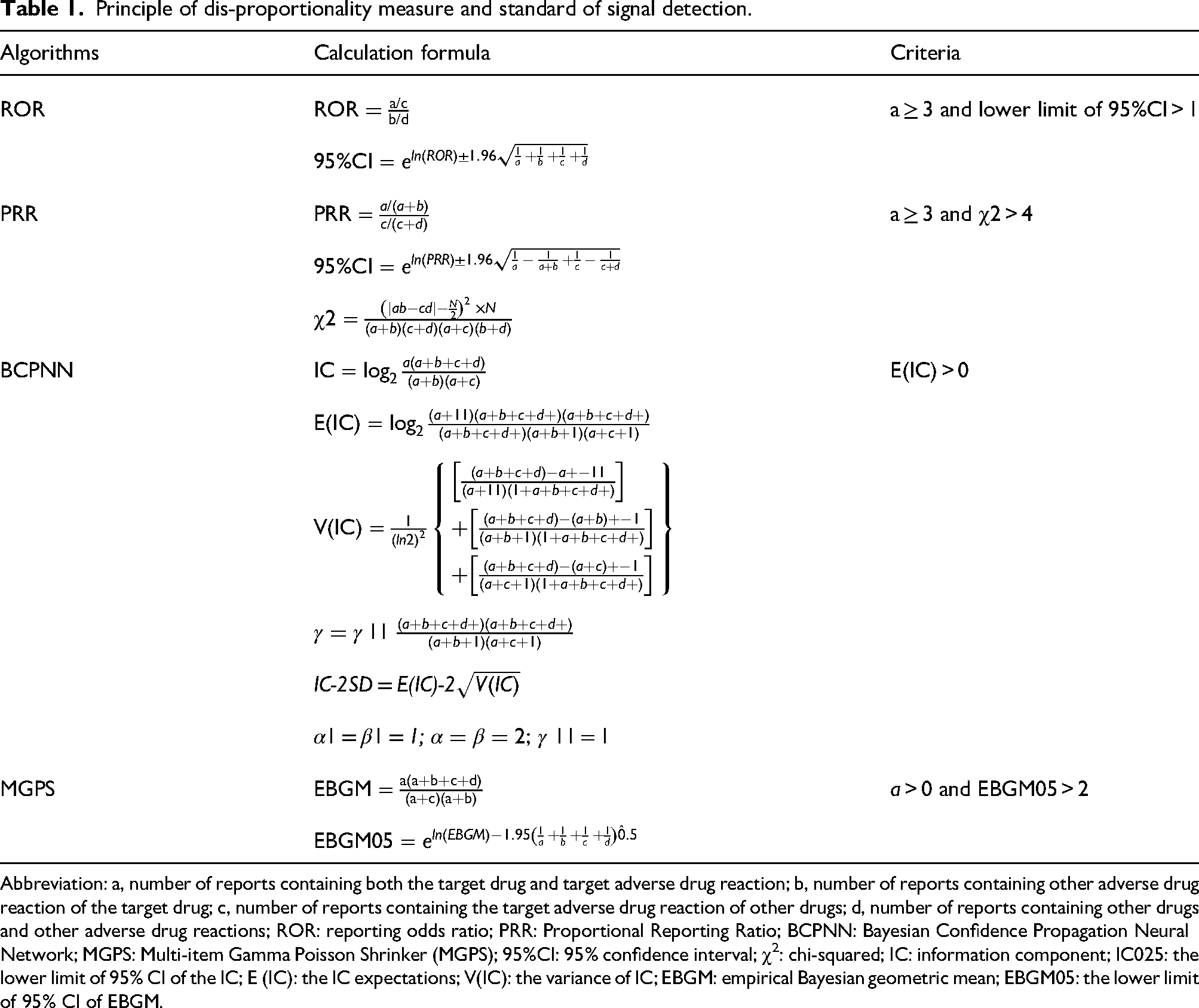
Abbreviation: a, number of reports containing both the target drug and target adverse drug reaction; b, number of reports containing other adverse drug reaction of the target drug; c, number of reports containing the target adverse drug reaction of other drugs; d, number of reports containing other drugs and other adverse drug reactions; ROR: reporting odds ratio; PRR: Proportional Reporting Ratio; BCPNN: Bayesian Confidence Propagation Neural Network; MGPS: Multi-item Gamma Poisson Shrinker (MGPS); 95%CI: 95% confidence interval; χ2: chi-squared; IC: information component; IC025: the lower limit of 95% CI of the IC; E (IC): the IC expectations; V(IC): the variance of IC; EBGM: empirical Bayesian geometric mean; EBGM05: the lower limit of 95% CI of EBGM.
These four algorithms complement each other in the following aspects: the ROR helps mitigate bias in small samples, whereas the PRR demonstrates higher specificity. The BCPNN is well-suited for integrating multi-source data, and the EBGM is particularly effective in detecting signals from rare adverse events.17–20 To ensure high-confidence signal detection, a conservative approach was adopted in this study by using the consensus of all four algorithms, thereby focusing only on the most robust adverse reaction signals. Higher signal values indicate stronger statistical associations with teprotumumab.
Time-to-onset analysis
Time-to-onset (TTO) was calculated as the interval between EVENT_DT (adverse event date) and START_DT (treatment initiation). A Weibull distribution model was applied to assess the temporal risk pattern of teprotumumab-associated AE. This model is defined by two parameters: the scale parameter (α) and the shape parameter (β). The scale parameter (α) defines the time scale for event occurrence, where higher values are associated with a later onset of adverse events. The shape parameter (β) describes the hazard rate: β<1 indicates a decreasing hazard (earlyfailure pattern), β=1 indicates a constant hazard, and β>1 indicates an increasing hazard (wear-out pattern). 21
Statistics analysis
In this study, all data mining and statistical analyses were conducted using R statistical software (version 4.3.0). Descriptive analysis were used to characterize patients treated with teprotumumab. The chi-square test was used to compare the AEs between groups. The Kruskal-Wallis test was applied to compare the onset time of AEs across sex-stratified subgroup. A P value < 0.05 was considered statistically significant.
Results
Descriptive analysis of teprotumumab associated reports in FAERS from 2020 to 2025
From the FAERS database, a total of 22,775,812 reports submitted between the first quarter of 2020 to the first quarter of 2025 were screened. Following the extracting and analysis procedure, 1,357 reports teprotumumab-related reports were identified, involving 1,092 PTs. Most reports originated from the United States (98.01%), with France, Italy, Japan, and other countries comprising the remaining submissions. The year of marketing (2020) demonstrated the lowest reporting frequency (139 cases). Subsequent annual reports remained stable at approximately 200 cases during the following three-year period, followed by a notable surge to 458 cases in 2024. Individuals aged 18–65 years constituted the predominant population (67.23%). Females accounted for 75% of cases, showing a clear predominance over males.. Physicians submitted 87.55% of reports, with pharmacists contributing the remainder (12.45%). Regarding clinical outcomes in documented cases, disability (6.12%) and hospitalization (5.45%) represented the most frequent consequence, serious adverse constituted a minority of reports (35.52%). Clinical characteristics are shown in Figure 1. Detailed information of indications and accompanying drugs is presented in Supplementary Materials Tables S1 and S2. The most prevalent diagnostic categories comprised endocrine ophthalmopathy, Graves’ disease, and toxic goitre (Table S1). The top three concomitant drugs were methimazole, synthroid and prednisone (Table S2).

Characteristics of reports with teprotumumab from the FAERS database. Notes Figure 1A presents a pie chart by country. Figure 1B presents a histogram of the distribution of reported adverse events by report year. Figure 1C presents a pie chart by age. Figure 1D presents a pie chart by gender. Figure 1E presents a pie chart by reporter. Figure 1F presents a pie chart by outcome. Figure 1G presents a pie chart by serious condition.
Disproportionality analysis at SOC level
Adverse reactions associated with teprotumumab were distributed across 27 SOCs. The most frequently reported SOCs were general disorders and administration site conditions (n = 727), investigations (n = 669), and ear and labyrinth disorders (n = 633). Table 2 presents SOC-level signal values across the four disproportionality algorithms.
The signals of teprotumumab at SOC level.
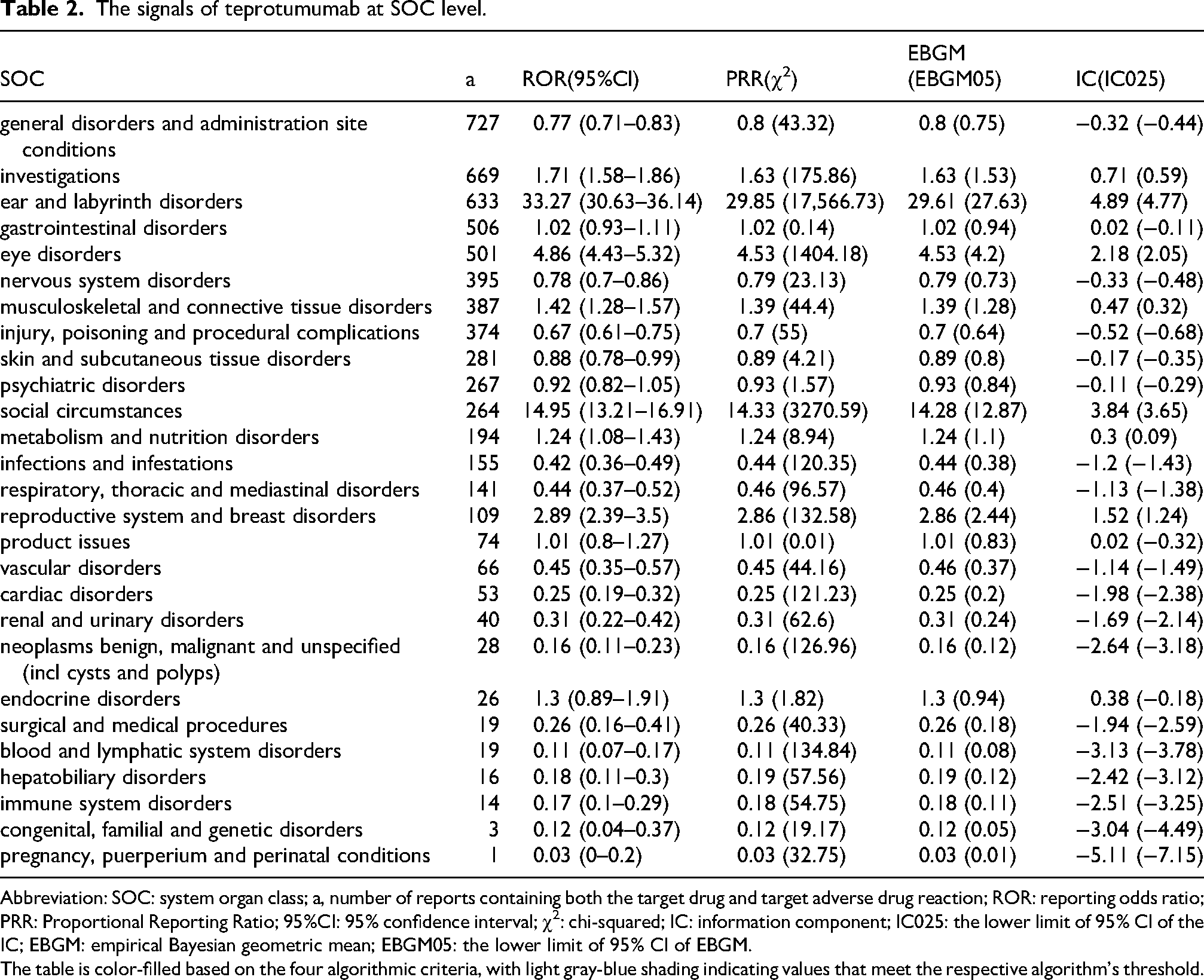
Abbreviation: SOC: system organ class; a, number of reports containing both the target drug and target adverse drug reaction; ROR: reporting odds ratio; PRR: Proportional Reporting Ratio; 95%CI: 95% confidence interval; χ2: chi-squared; IC: information component; IC025: the lower limit of 95% CI of the IC; EBGM: empirical Bayesian geometric mean; EBGM05: the lower limit of 95% CI of EBGM.
The table is color-filled based on the four algorithmic criteria, with light gray-blue shading indicating values that meet the respective algorithm's threshold.
The following SOCs met the criteria of all four statistical algorithms and were confirmed as validated SOC signals for teprotumumab: ear and labyrinth disorders, eye disorders, social circumstances and reproductive system and breast disorders (Table 2). When ranked by decreasing ROR Disproportionality analysis at SOC level ROR values, the strongest SOC-level signals were observed for ear and labyrinth disorders (ROR 33.27; 95% CI 30.63–36.14), social circumstances (ROR14.95; 95% CI 13.21–16.91), and eye disorders (ROR 4.86; 95% CI 4.43–5.32). Notably, ear and labyrinth disorders demonstrated both the highest ROR values and ranked among the three most frequently reported SOCs, indicating a significant pharmacovigilance signal association with teprotumumab.
Disproportionality analysis at PT level
Within the FAERS database, the five most frequently reported PTs were: muscle spasms (n = 183), tinnitus (n = 146), hypoacusis (n = 143), fatigue (n = 130), and diarrhoea (n = 96). Signal detection results for the top 30 PTs are visualized in a clustered heatmap (Figure 2).
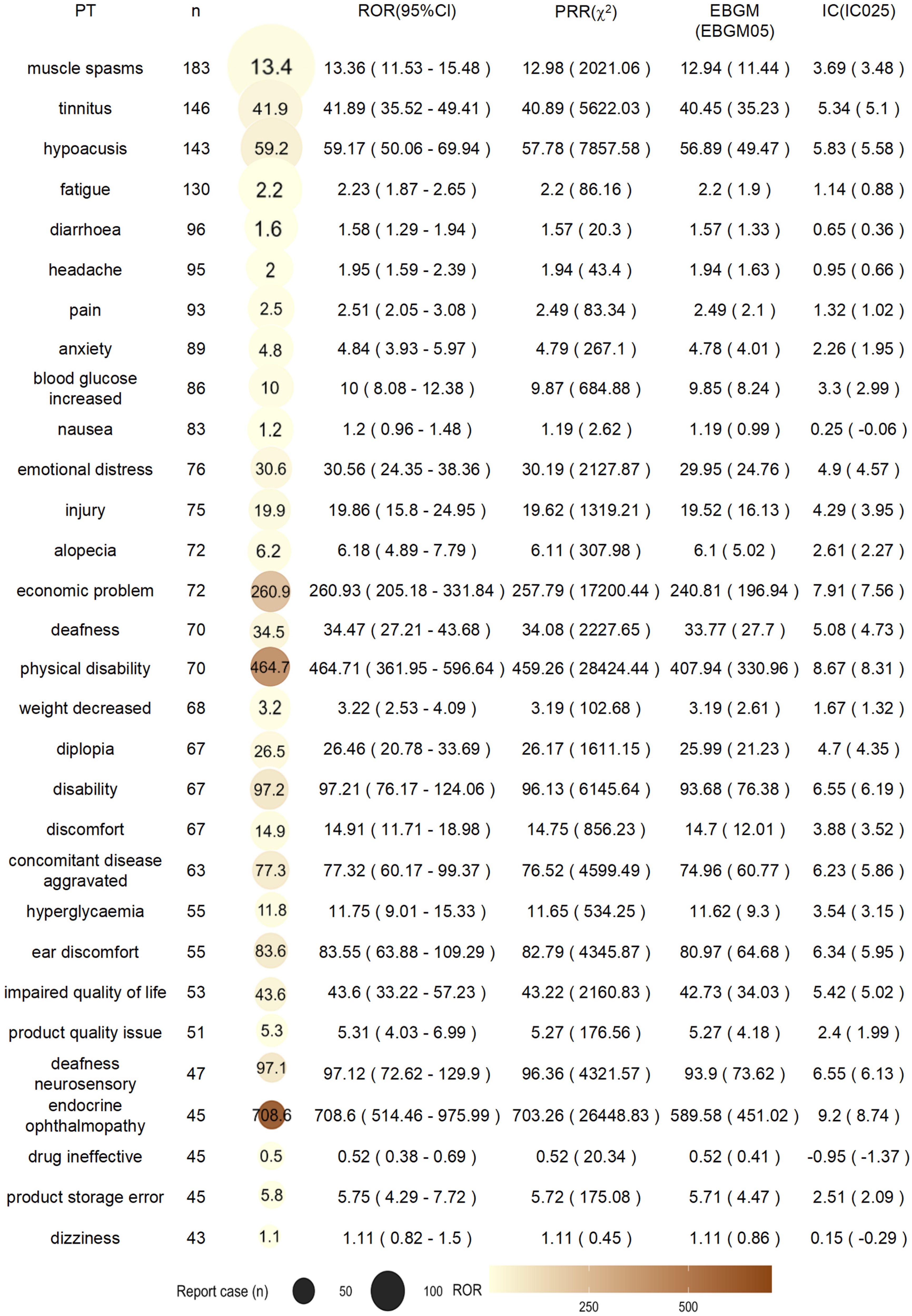
ROR heatmap of the top 30 PTs. Abbreviations: PT, preferred terms; n, total number of adverse drug events; ROR, reporting odds ratio; PRR, Proportional Reporting Ratio; BCPNN, Bayesian Confidence Propagation Neural Network; IC, information component; IC025, the lower limit of 95% CI of the IC.
The PTs with the strongest ROR-based signals were endocrine ophthalmopathy (ROR 708.60; 95% CI514.46–975.99), physical disability (ROR 464.71; 95%CI 361.95–596.64), economic problem (ROR 260.93;95% CI 205.19–331.84), disability (ROR 97.21; 95% CI76.17–124.06), and neurosensory deafness (ROR97.12; 95% CI 72.64–129.90). Each PT was evaluated using all four algorithms. A total of 143 PTs met the criteria across all methods and were therefore considered validated signals (Figure 3B). Stratification of validated PTs showed highest counts in “ear and labyrinth disorders” (n = 598), followed by “investigations” (n = 391) and “eye disorders” (n = 369). Figure 3A illustrates the SOC level distribution of validated PTs through a treemap.
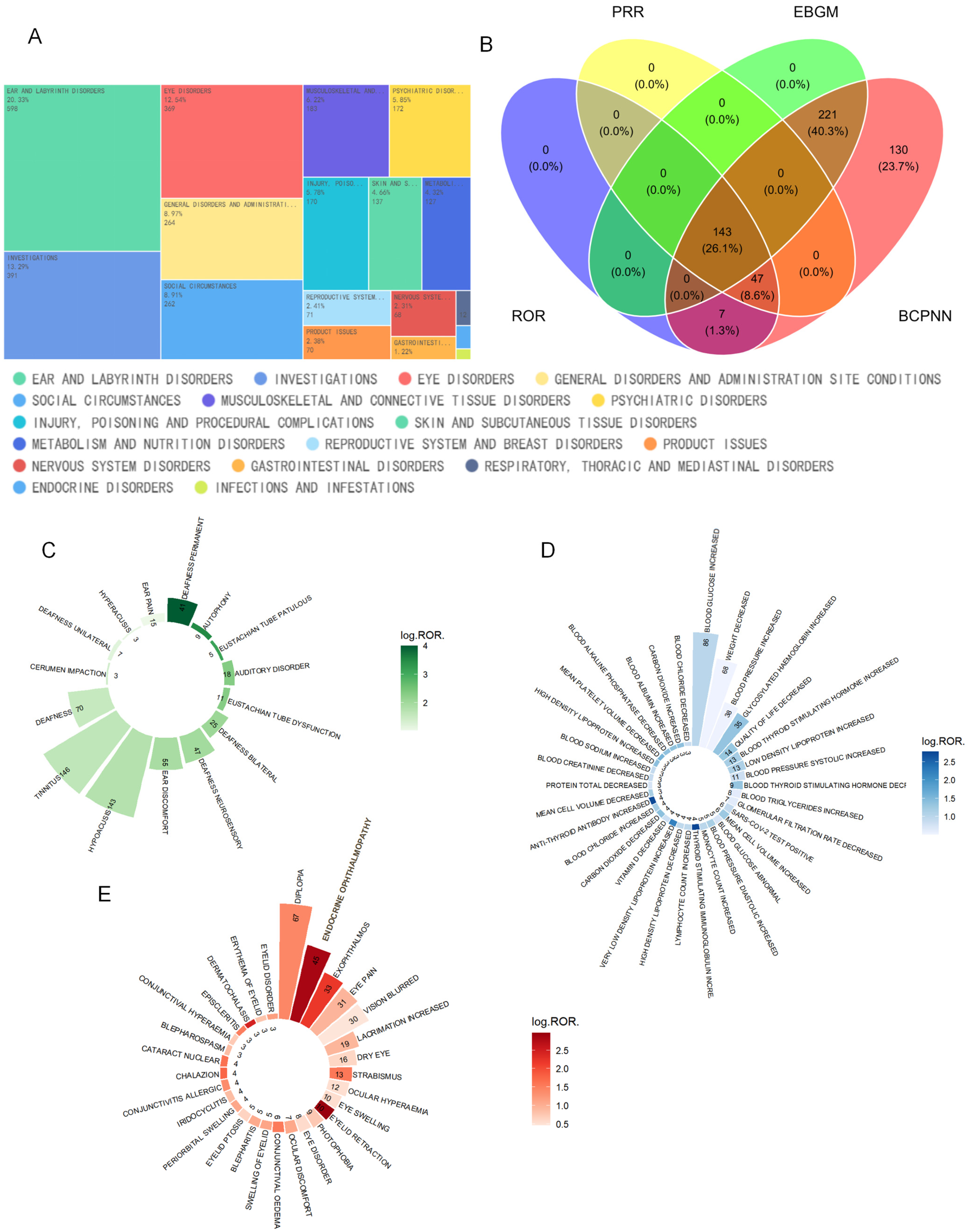
PTs validated by four signal detection algorithms criteria. Notes Figure 3A presents a treemap of the validated PTs in SOC level. Figure 3B presents a venn diagram of PTs by four signal detection algorithms criteria. Figure 3C presents a integrates of bar chart and heatmap of PTs in ear and labyrinth disorders. Figure 3D presents a integrates of bar chart and heatmap of PTs in investigations. Figure 3E presents a integrates of bar chart and heatmap of PTs in eye disorders.
The “ear and labyrinth disorders”SOC included 15 validated PTs, with tinnitus exhibiting the highest report frequency (n = 146). Figure 3C integrates a bar chart and heatmap to visualize case counts and logarithmic ROR values across these PTs. The three PTs with maximal ROR value were: deafness permanent (ROR 10,021.8; 95% CI 5,544.31–18,115.24), autophony (ROR 3,282.12; 95% CI 1,333.19–8,080.12), and patulous eustachian tube (ROR 1,401.68; 95% CI499.54–3,932.99).
The SOC of “Investigations” encompassed 34 validated PTs, dominated by blood glucose increased (n = 86, ROR:10(8.08–12.38)), thyroid stimulating immunoglobulin increased (ROR: 607.29(210.65–1750.81)), anti-thyroid antibody increased (ROR: 560.58(195.58–1606.73)) and very low density lipoprotein increased (ROR:169.48(62.17–462)) displayed the strongest ROR signals in this category (Figure 3D).
In the SOC of “Eye disorders” showed diplopia (n = 67, ROR:26.46(20.78–33.69)) as the most frequently reported event, with eyelid retraction (ROR:935.23 (466.66–1874.32)), endocrine ophthalmopathy (ROR:708.6(514.46–975.99)) and dermatochalasis (ROR:280.24(86.58–907.09)) demonstrating the highest ROR values (Figure 3E).
TTO analysis
Time-to-onset data were available for 128 cases. The median onset time was 59 days (quartile range [IQR] 24–113). As shown in Figure 4A, the onset time differed, ranging from 1 to 823 days, with most cases occurred within 69 days after the start of teprotumumab (n = 66, 51.6%). The onset time showed no differences among different gender groups (Figure 4B and C). The shape parameter (β) of Weibull distribution is 0.77, and its 95% confidence interval (CI) is 0.68–0.87 (Figure 4D). When β<1, it indicates that the risk of AE decreases over time, which is characteristic of an early-failure distribution.
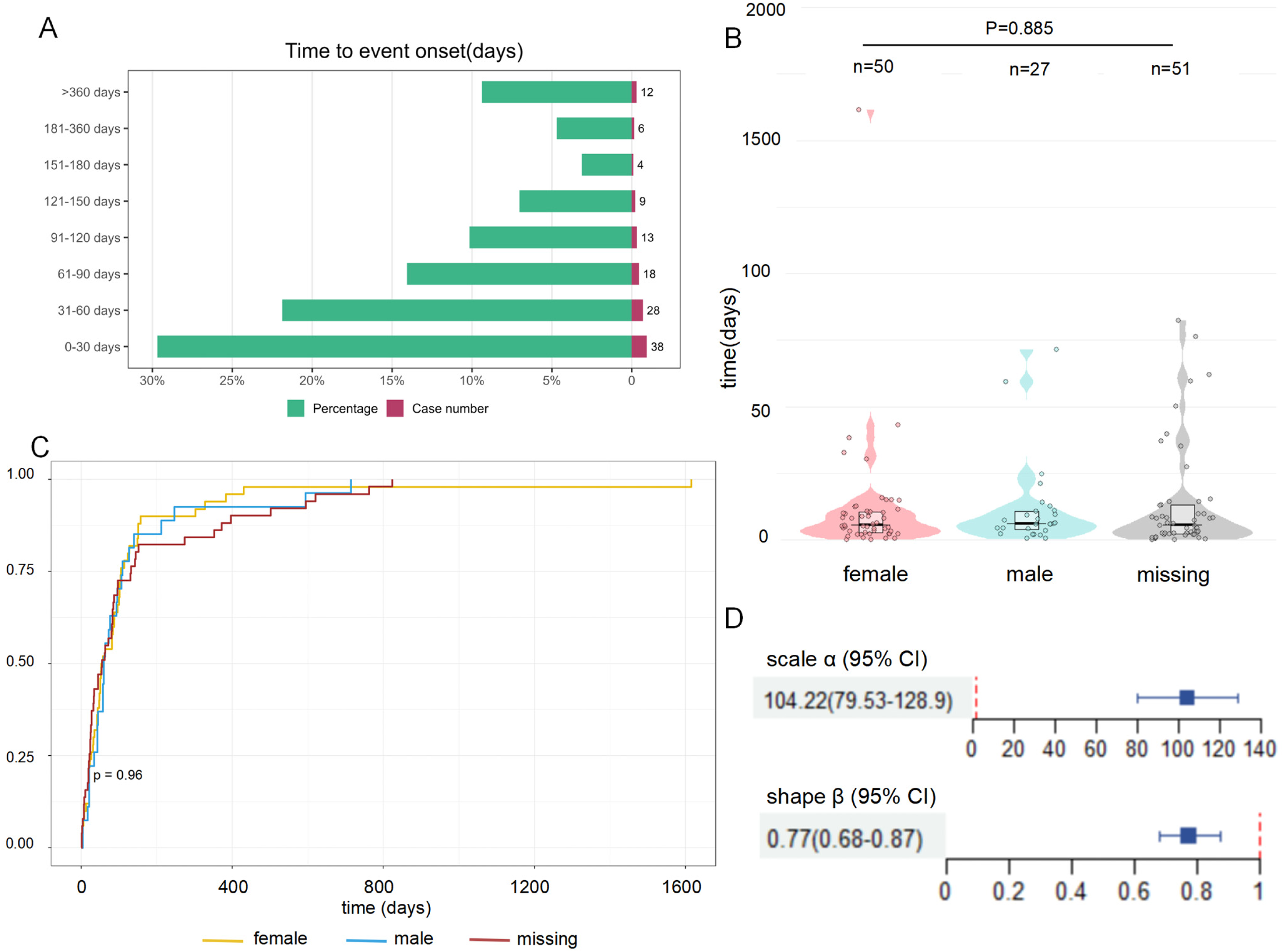
Time to event onset of adverse events. Notes Figure 4A presents a bi-direction Bar Chart of time to event onset. Figure 4B presents a violin plot of the time to event onset by gender. Figure 4C presents a survival curve of time to event onset by gender. Figure 4D presents a Weibull distribution of time to event onset.
Discussion
Phase II clinical trials conducted by Smith et al. 1 and Phase III trials by Douglas et al. 22 demonstrated the significant efficacy of teprotumumab in treating moderate-to-severe active TED. Based on this evidence, teprotumumab became the first FDA-approved treatment for TED in January 2020. Subsequently, the 2021 EUGOGO Clinical Practice Guidelines listed teprotumumab as a second-line therapy for moderate-to-severe TED. 6 In 2022, the European Thyroid Association and the American Thyroid Association issued consensus recommendations stating that teprotumumab may be considered a first-line treatment for patients with moderate-to-severe TED presenting with active inflammation, marked proptosis, and/or diplopia. 23 A 2023 Phase IV clinical trial enrolled patients diagnosed with stable, chronic (inactive) TED. Results indicated that teprotumumab reduced proptosis by 2.4 mm in patients with long-standing disease/low disease activity. 24 Furthermore, a multicenter observational case series by Sears et al. reported significant therapeutic outcomes in 10 patients with acute/chronic active TED complicated by dysthyroid optic neuropathy (DON) following intravenous teprotumumab infusion. 25 As accumulating evidence highlights the substantial improvement in ocular manifestations achieved with teprotumumab across diverse TED patient types and its expanding clinical applications, the associated adverse effects have also garnered increasing clinical attention.
This pharmacovigilance study represents the first comprehensive analysis leveraging the latest real-world data from the FAERS database to systematically identify AEs associated with teprotumumab. More than 22 million FAERS reports from a global population were screened. Utilizing multiple disproportionality analysis methods enhanced both the sensitivity and specificity of AE signal detection. 16 The analysis revealed the validated signals for teprotumumab at SOCs level were: ear and labyrinth disorders, social circumstances, and eye disorders. At the PT level, the strongest signals were observed for endocrine ophthalmopathy, physical disability, economic problem, disability, and neurosensory deafness.
Our findings align with previous clinical studies. The most frequently reported adverse reactions in clinical trials included muscle spasms, nausea, alopecia, diarrhea, fatigue, hyperglycemia, and hearing impairment. Other common adverse reactions comprised dysgeusia, headache, and dry skin (adverse reactions occurring in 5% or more of patients treated with TEPEZZA and greater incidence than placebo).1,22 Our study results indicate that muscle spasms (n = 183, ROR13.36; 95% CI 11.53–15.48) were the most frequently validated PT, aligning with the highest proportion of adverse reactions documented in the product label. Alopecia (n = 72; ROR 6.18;95% CI 4.89–7.79), hyperglycaemia (hyperglycaemia: n = 55; ROR 11.75; 95% CI 9.01–15.33; blood glucose increased: n = 85; ROR 10.00; 95% CI 8.08–12.38), hearing impairment (captured by multiple related PTs; see below), dysgeusia (n = 20; ROR 3.77; 95% CI 2.43–5.84), and dry skin (n = 33;ROR 4.33; 95% CI 3.08–6.10) also showed high case numbers and strong disproportionality signals. However, no significant signal strength in nausea, diarrhea, fatigue, or headache was detected in our study.
Notably, our data mining findings indicate a strong association between teprotumumab and ear and labyrinth disorders, primarily hearing impairment. Several PTs reflecting hearing dysfunction showed marked signal strength: hypoacusis (n = 143; ROR 59.17; 95% CI50.06–69.94), deafness (n = 70; ROR 34.47; 95% CI27.21–43.68), neurosensory deafness (n = 47; ROR 97.12;95% CI 72.62–129.90), permanent deafness (n = 41;ROR 10,021.8; 95% CI 5,544.31–18,115.24), bilateral deafness (n = 25; ROR117.20; 95% CI 78.63–174.67), auditory disorder (n = 18; ROR 221.35; 95% CI137.46–356.45), and unilateral deafness (n = 7; ROR 15.86; 95% CI 7.54–33.33). Other hearing-related adverse reactions should not be overlooked: tinnitus (n = 146; ROR 41.89; 95% CI 35.52–49.41) and autophony (n = 9; ROR 3,282.12; 95% CI 1,333.19–8,080.12). An observational study involving 22 patients (total of 44 ears) with TED found that 17 ears (38.6%) met the criteria for ototoxicity-related hearing loss following teprotumumab treatment for TED, with 11 patients (50%) experiencing hearing impairment in at least one ear. 26 Prospective research revealed that patients developing teprotumumab-associated hearing changes, compared to those without such changes, were more likely to have pre-existing baseline hearing abnormalities, be older, and have higher baseline Clinical Activity Scores (CAS). 27 Insulin-like growth factor 1 (IGF-1) is recognized as crucial for inner ear development and the maintenance of cochlear hair cell proliferation and survival. Studies have identified a link between genetic IGF-1 deficiency and severe hearing impairment.28,29 Given the association between teprotumumab and auditory adverse events, clinicians are advised to assess relevant risk factors for hearing impairment prior to initiating treatment, carefully weigh the potential therapeutic benefits against the risks, and monitor hearing function during the course of therapy.
Certain adverse reactions not documented in the product label, but identified as associated with teprotumumab in our data mining study, warrant particular clinical attention. For instance, psychiatric disorders were reported, including anxiety n = 89; ROR4.84; 95% CI 3.93–5.97) and emotional distress (n = 76;ROR 30.56; 95% CI 24.35–38.36). Given that this study was restricted to adverse reaction reports submitted by healthcare professionals—whose recognition and diagnosis of psychiatric symptoms carry relative objectivity—these findings merit closer scrutiny. Yee et al. 30 also reported a case of a 62-year-old female TED patient who developed intermittent altered mental status lasting one week following her third intravenous infusion of teprotumumab; her neurocognitive symptoms resolved after plasmapheresis. Previous studies have indicated that loss of IGF-1/IGF-1R signaling in the brain is associated with an increased risk of cognitive decline, Alzheimer's disease, early-onset dementia, depression, and anxiety.31,32 However, it remains unclear whether teprotumumab selectively affects IGF-1R on OFs, or if it also impacts IGF-1/IGF-1R signaling within the brain.
This study has several limitations. First, the data originated from the FAERS database, which carries inherent limitations: FAERS reports are unverified and may contain inaccuracies, including misreporting and underreporting. To mitigate reporting bias, we restricted our analysis to reports submitted exclusively by healthcare professionals. However, this approach itself may have excluded some relevant reports. Second, our findings can only identify signals of association between teprotumumab and AEs and cannot establish causality. Nevertheless, the results offer the valuable insights for future research. Subsequent studies, such as cohort studies or randomized controlled trials (RCTs), are needed to further evaluate potential causal relationships. Additionally, prospective studies should be conducted to elucidate the drug's mechanisms of action on ear and labyrinth function, thereby furnishing a more detailed scientific basis for pharmacovigilance. Third, due to teprotumumab's relatively recent market approval, its long-term adverse effect profile cannot yet be accurately assessed. Additionally, teprotumumab requires repeated administrations. Considering that some patients discontinue treatment upon experiencing adverse reactions, the potential cumulative effects following multiple injections remain unassessable.
In this study, we conducted a comprehensive analysis using five years of post-marketing real-world data for teprotumumab, applying multiple disproportionality analysis methodologies to assess associated adverse reactions. The results indicate that adverse reactions linked to teprotumumab are generally aligned with those documented in the product label. However, adverse reactions related to hearing impairment and psychiatric disorders warrant heightened clinical vigilance.
Supplemental Material
sj-docx-1-ejo-10.1177_11206721261446011 - Supplemental material for Five year of post-marketing safety of teprotumumab: A disproportionality analysis of the FDA adverse event reporting system
Supplemental material, sj-docx-1-ejo-10.1177_11206721261446011 for Five year of post-marketing safety of teprotumumab: A disproportionality analysis of the FDA adverse event reporting system by Jiantong Du, Chen Xing, Zhiyue Zhang and Zonghui Ma in European Journal of Ophthalmology
Footnotes
Acknowledgements
We are grateful to Yijia Jiang for her assistant in study design.
Ethics declarations
Ethical approval and informed consent were waived due to the anonymized nature of the publicly available data.
Author contributions
Du: designed the study, analyzed the data, wrote and revised the manuscript. Xing: conceived and designed the study, analyzed the data and wrote the manuscript. Zhang: analyzed the data and wrote the manuscript. Ma: conceived the study and contributed to the design of the study. All authors read and approved the final manuscript.
Declaration of conflicting interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Data availability
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.