
Abstract
Purpose
To evaluate functional and anatomical outcomes after intravitreal dexamethasone implant (DEXI) in macular edema secondary to retinal vein occlusion (ME-RVO), comparing treatment-naïve eyes with early-switch (ES) and late-switch (LS) eyes previously treated with anti-VEGF, to explore the optimal therapeutic window for switching.
Methods
A retrospective real-world study including 71 eyes with ME-RVO treated with DEXI and followed for 12 months. Patients were classified as naïve (no prior intravitreal therapy), ES (≤3 anti-VEGF injections before switching), and LS (>3 anti-VEGF injections before switching). Functional outcomes were assessed by best-corrected visual acuity (BCVA), and anatomical outcomes by central macular thickness (CMT) using spectral-domain optical coherence tomography.
Results
BCVA improved significantly at month 2 in treatment-naïve and ES eyes (p < 0.05), whereas no significant change was observed in LS eyes. A ≥ 2-line gain occurred in 50% of naïve eyes, markedly higher than in previously treated eyes. Naïve patients maintained functional and anatomical improvement throughout follow-up. All groups demonstrated an early reduction in CMT at month 2 (p < 0.05). Multivariate analysis identified baseline BCVA, but not switching timing, as the main predictor of functional improvement.
Conclusions
While DEXI improved anatomical outcomes across all subgroups, functional recovery was more frequently observed in naïve and ES eyes. However, baseline BCVA emerged as the main independent determinant of functional response, suggesting that visual outcomes are primarily driven by initial visual status rather than switching timing. By including a naïve comparison group, this study provides novel insights into the management of ME-RVO in patients with suboptimal anti-VEGF response.
Keywords
Introduction
Cardiovascular disease is steadily increasing worldwide, and among its thrombotic manifestations, retinal vein occlusion (RVO) represents the second most common vascular retinal cause of vision loss after diabetic retinopathy. RVO prevalence varies by ethnicity and increases with age, regardless of gender.1–5 The main complication is visual loss secondary to macular edema (ME),3,4,6 resulting from blood-retinal barrier disruption and vascular inflammatory cascade. 6 Optical coherence tomography (OCT) enables an objective assessment of ME, with central macular thickness (CMT) closely correlated with the best-corrected visual acuity (BCVA).7–9
Over the past decade, intravitreal anti-VEGF agents have been established as first-line treatment for ME secondary to RVO (ME-RVO), providing significant anatomical and functional improvement.3,4,10,11 However, a substantial proportion of patients exhibit suboptimal responses, leading to growing interest in switching to alternative therapies. Intravitreal dexamethasone implants (DEXI) represent a validated therapeutic option, demonstrating both efficacy and safety in refractory cases and suboptimal responses.12–15 Although several real-world studies have assessed outcomes after switching from anti-VEGF agents to corticosteroids, only a limited number have clearly differentiated between early and late switching, and none have directly compared these approaches with a truly treatment-naïve cohort.16–18 Defining the optimal therapeutic window for transitioning to corticosteroids is essential to maximize functional recovery before irreversible structural retinal damage occurs.
In contrast to prior available research, the present study incorporates a treatment-naïve cohort and directly compares their outcomes with those of ES and LS patients. By evaluating both functional and structural responses across these three clinically relevant groups, our work aims to determine a more precise therapeutic window in which DEXI may achieve maximal visual and anatomical recovery.
Methods
Study design and ethics
This retrospective, real-world observational study of consecutive cases was conducted at a tertiary referral center. This study was approved by the local Ethics Committee and adhered to the tenets of the 1964 Declaration of Helsinki and its later amendments for research involving human subjects.
Inclusion and exclusion criteria
A total of 71 eyes from 71 patients diagnosed with ME-RVO and treated with a first DEXI between January 2013 and June 2024 at our institution were included.
Inclusion criteria were 1 : (1) age >18 years 2 ; (2) confirmed diagnosis of RVO with associated ME, defined as a CMT ≥315 µm measured using SD-OCT 19 ; 3 (3) either treatment- naïve or previously treated with anti-VEGF agents with suboptimal response 4 ; (4) having received at least one DEXI 5 ; (5) availability of a follow-up duration of 12 months after the first DEXI administration.
When both eyes were eligible or had received treatment, only one eye per patient was included in the analysis. In such cases, the first eye meeting the inclusion criteria was selected.
Exclusion criteria were as follows 1 : (1) significant media opacities interfering with OCT image acquisition (e.g., dense cataract, or vitreous haemorrhage) 2 ; (2) presence of any other ocular or systemic disease that could affect retinal morphology or visual function (e.g., uveitis, age-related macular degeneration) 3 ; (3) prior glaucoma (intraocular pressure (IOP) > 25 mmHg despite treatment) or history of glaucoma surgery 4 ; (4) ocular surgery within 6 months prior to DEXI administration 5 ; (5) baseline BCVA >1.7 in LogMAR.
Patient classification
Patients were classified according to their prior intravitreal treatment history as follows:
- Naïve (N): patients with no previous intravitreal therapy. - Early switch (ES): patients with suboptimal responses after ≤ 3 consecutive anti-VEGF injections before switching to DEXI. - Late switch (LS): patients with suboptimal responses after > 3 consecutive anti-VEGF injections administered within the 12 months prior to switching to DEXI.
Suboptimal response was defined as persistent CMT >300 µm and/or the absence of meaningful improvement in BCVA following anti-VEGF treatment. 19
The ≤3 anti-VEGF injection threshold was selected according to current clinical guidance and recent studies recommending reassessment of therapeutic benefit after the initial injections to determine whether continued anti-VEGF therapy is appropriate or whether alternative strategies should be considered.4,17–20,24,25
Study procedures
Follow-up visits were scheduled at baseline, month 2 (± 2 weeks), month 6 (± 2 weeks) and month 12 (± 4 weeks) after DEXI administration. For all groups, baseline corresponded to the visit at which the first DEXI injection was administered, and patients were followed for 12 months from this time point. Each participant underwent a comprehensive ophthalmic examination including BCVA (LogMAR), IOP measurement using Goldmann applanation tonometer, slit-lamp biomicroscopy, dilated fundus examination, and spectral-domain (SD) OCT imaging (SPECTRALIS, Heidelberg Engineering, Heidelberg, Germany). The decision to initiate DEXI, as well as any re-treatment during follow-up, was made at the discretion of the treating ophthalmologist in agreement with the patient.
Demographic data (age, gender, eye laterality, and type of occlusion) and medical history were collected from electronic medical records. Ischemic status was not systematically documented for all patients in this retrospective cohort and was therefore not included as a predefined stratification variable.
Outcome measures
The main functional outcome measured was the variation in BCVA at the different follow-up visits.
Anatomical outcomes were assessed as changes in CMT automatically quantified by the OCT software within the 500-μm radius ring centered on the foveola according to the ETDRS grid, reflecting the degree of foveal thickening.
Endpoints
Statistical analyses
Descriptive analyses included the mean and standard deviation (SD) for normally distributed variables, as well as frequencies and percentages where appropriate. The Shapiro–Wilk test was used to assess normality of distribution. For normally distributed variables, a paired t-test was used to compare pre- and post-treatment changes. For non-normally distributed variables, a paired Wilcoxon signed-rank test was used for intra-group comparison over time.
Inter-group differences were evaluated using ANOVA or the Kruskal–Wallis test, with the corresponding post hoc analyses. Specifically, BCVA comparisons between the three independent groups were performed using the Kruskal-Wallis test due to non-normal distribution. Categorical variables were compared using Pearson's chi-squared test or Fisher's exact test, as appropriate. This included the analysis of the proportions of eyes achieving a ≥ 2-line gain in visual acuity. For the analysis of changes in visual acuity (VA), BCVA values (Snellen chart) were converted and expressed in LogMAR. To account for repeated measurements over time, longitudinal changes in BCVA and CMT were evaluated using linear mixed-effects models, with time and treatment group as fixed effects and patient as a random effect, including age as a covariate. Pairwise post hoc comparisons were adjusted using the Bonferroni method to reduce the risk of type I error due to multiple testing. Multivariate logistic regression analysis was performed to identify independent predictors of functional (≥2-line BCVA gain) and anatomical (≥20% CMT reduction) outcomes at month 2. Variables included in the model were age, baseline BCVA, baseline CMT, prior anti-VEGF treatment, and lens status. Prior anti-VEGF exposure was modelled as a categorical variable dichotomized as ≤3 versus >3 injections, based on the predefined study groups, with ≤ 3 injections used as the reference category.
All data were analysed using R Studio version 4.0.3 software. The results of the statistical tests were considered significant when p < 0.05.
Results
Baseline demographic and clinical characteristics
A total of 71 eyes from 71 patients with ME-RVO were included in the study. The cohort comprised 33 males (46.48%) and 38 females (53.52%), with a mean age of 70.43 ± 10.76 years. Baseline demographic and clinical data are summarised in Table 1.
Baseline demographic and clinical data.
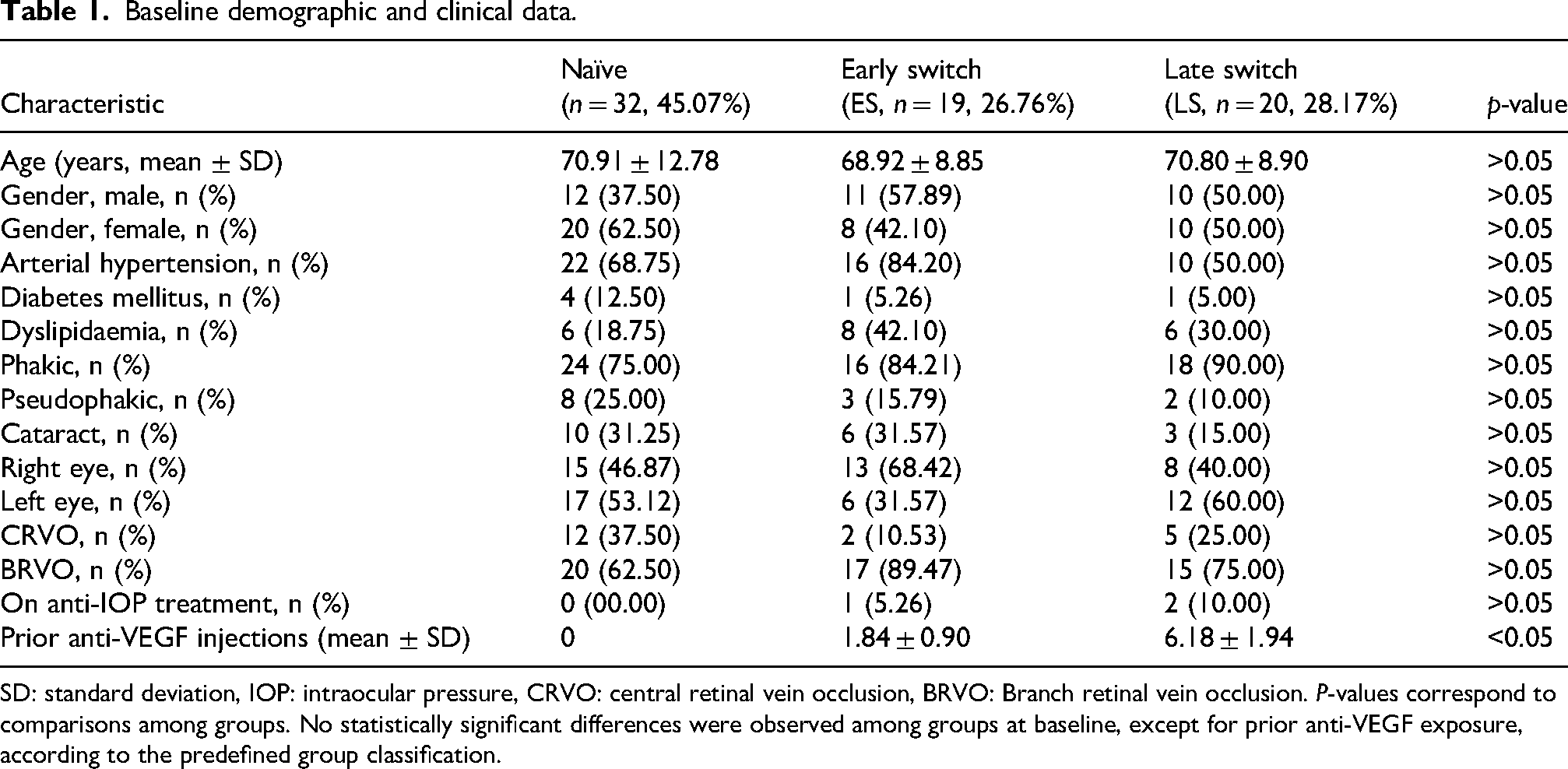
SD: standard deviation, IOP: intraocular pressure, CRVO: central retinal vein occlusion, BRVO: Branch retinal vein occlusion. P-values correspond to comparisons among groups. No statistically significant differences were observed among groups at baseline, except for prior anti-VEGF exposure, according to the predefined group classification.
Patients were classified into three groups: naïve (n = 32), ES (n = 19) and LS (n = 20). No statistically significant differences were observed among groups regarding baseline parameters. In the ES and LS groups, the mean time interval between the last anti-VEGF injection and DEXI administration was 6 ± 2 weeks. The duration of macular edema prior to DEXI administration showed a non-normal distribution and was therefore described using median and interquartile range (IQR). Median duration was 36 days (IQR 9–68.5) in the naïve group, 132 days (IQR 121.5–277.5) in the ES group, and 534 days (IQR 504.5–754.5) in the LS group. Mean duration was 102 ± 235 days, 351 ± 606 days, and 657 ± 416 days, respectively.
The mean baseline BCVA for the entire cohort was 0.78 ± 0.51 and the mean baseline CMT was 568.46 ± 176.57 μm. The mean baseline IOP from all the patients was 15.17 ± 2.56 mmHg, with only three patients requiring topical hypotensive treatment.
During the 12-month follow-up, the mean total number of DEXI injections in the overall cohort was 1.44. When stratified by group, the mean total number of injections was 1.44 in the naïve group, 1.37 in the ES group, and 1.50 in the LS group, with no statistically significant differences between groups (p > 0.05). Retreatment with DEXI was required in 14 naïve eyes, 7 ES eyes, and 10 LS eyes.
Best corrected visual acuity
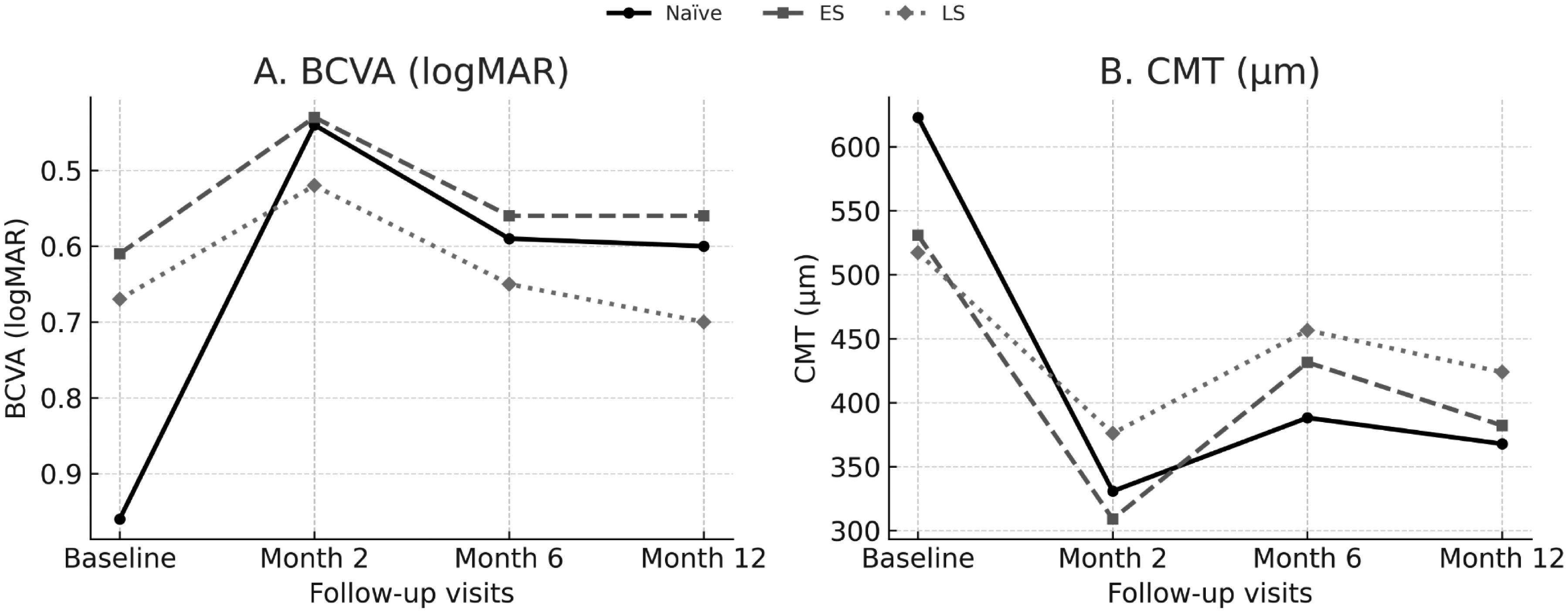
The analysis of BCVA revealed significant differences during the follow-up (Table 2, Figure 1).
Changes in BCVA and CMT after DEXI treatment during follow-up.
Changes in BCVA (LogMAR) during follow-up after DEXI treatment
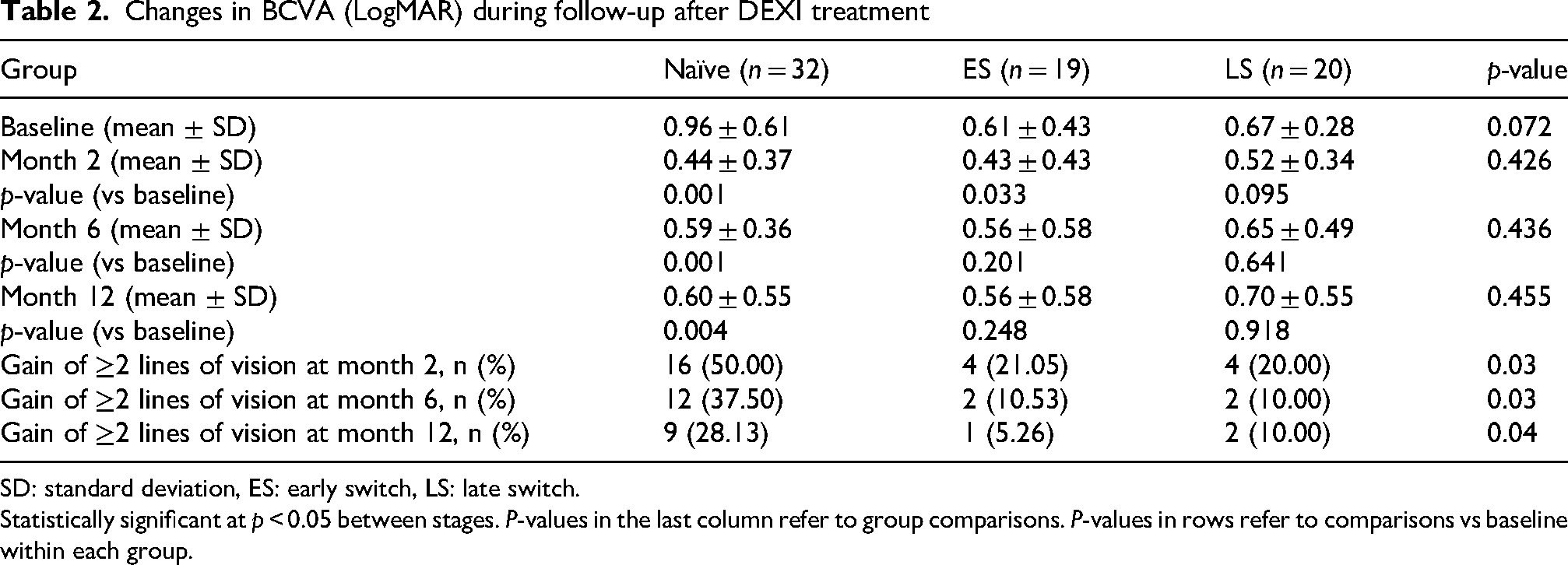
SD: standard deviation, ES: early switch, LS: late switch.
Statistically significant at p < 0.05 between stages. P-values in the last column refer to group comparisons. P-values in rows refer to comparisons vs baseline within each group.
The Naïve group improved from 0.96 ± 0.61 at baseline to 0.44 ± 0.37 at month 2 (p < 0.05 vs baseline), and this functional gain remained significant at months 6 and 12 (both p < 0.05 vs baseline).
The ES group showed baseline mean BCVA of 0.61 ± 0.43 and experienced a significant improvement to 0.43 ± 0.43 at month 2 (p < 0.05 vs baseline). However, this early gain was not maintained at months 6 and 12 (both p > 0.05 vs baseline).
In the LS group the mean BCVA at baseline was 0.67 ± 0.28, which did not exhibit significant improvement in BCVA at any follow-up visit (p > 0.05 vs baseline).
Although inter-group differences did not reach statistical significance when BCVA was analysed in LogMAR, the use of ETDRS letter equivalents revealed a clinically relevant functional gain. Notably, the naïve group exhibited a markedly higher proportion of eyes achieving a ≥ 2-line improvement at month 2 (50%) compared with ES (21.05%) and LS (20%) eyes (p = 0.03).
Central macular thickness
Regarding CMT, all groups showed a consistent improvement at all follow-up visits, with reductions most pronounced at month 2 (Table 3, Figure 1).
Changes in CMT (µm) during follow-up after DEXI treatment
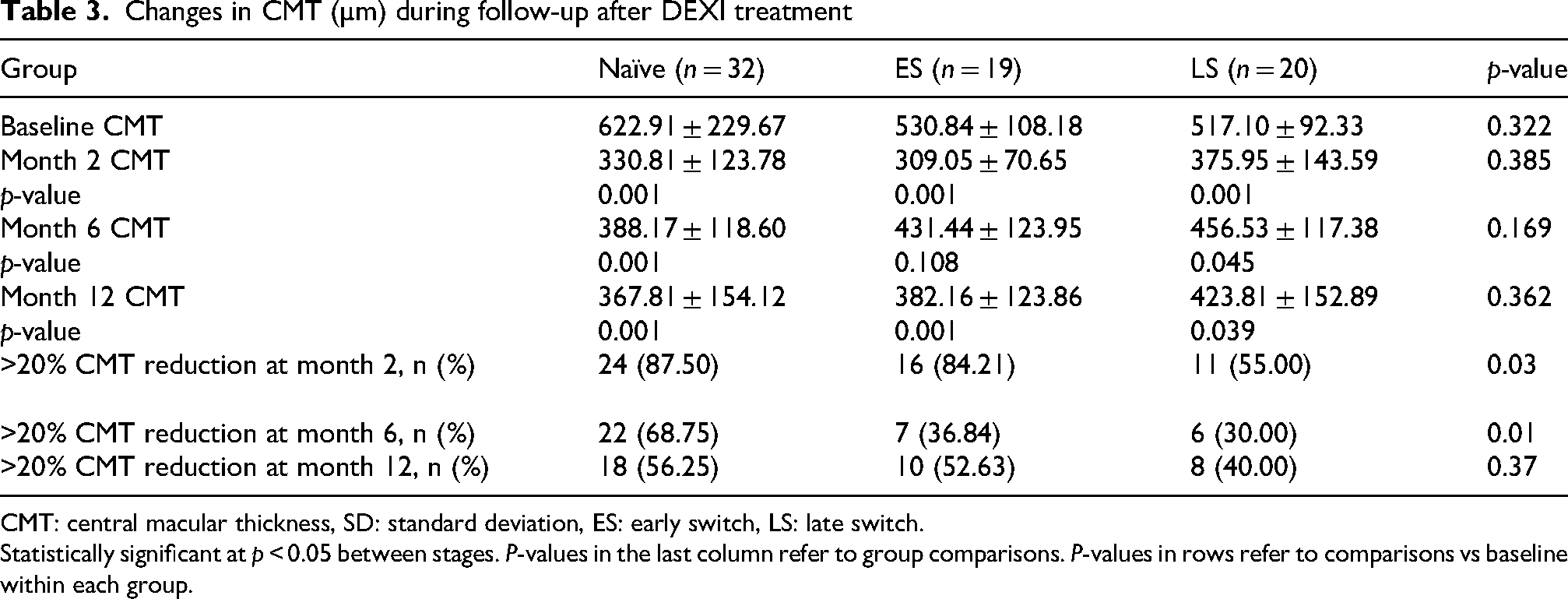
CMT: central macular thickness, SD: standard deviation, ES: early switch, LS: late switch.
Statistically significant at p < 0.05 between stages. P-values in the last column refer to group comparisons. P-values in rows refer to comparisons vs baseline within each group.
Naïve group presented a baseline CMT of 622.91 ± 229.67 µm, which decreased to 330.81 ± 123.78 µm at month 2 (p < 0.05 vs baseline); 87.5% of naïve patients achieved a CMT reduction greater than 20%. This anatomical improvement remained significant at months 6 and 12 (both p < 0.05 vs baseline).
ES group improved from a CMT of 530.84 ± 108.18 µm at baseline to 309.05 ± 70.65 µm at month 2 (p < 0.05 vs baseline) with 84.21% of eyes showing a reduction greater than 20%. Although this improvement was not maintained at month 6 (p > 0.05 vs baseline), it became significant again at month 12 (p < 0.05 vs baseline).
LS patients also achieved significant reductions in CMT at every follow-up visit (all p < 0.05 vs baseline), with an initial decrease from 517.10 ± 92.33 at baseline to 375.95 ± 143.59 µm at month 2; 55% of LS patients experienced a reduction greater than 20%.
Safety profile
The most frequent adverse event observed was IOP elevation (17 eyes). Mean IOP values at baseline and during follow-up are represented in Figure 2.
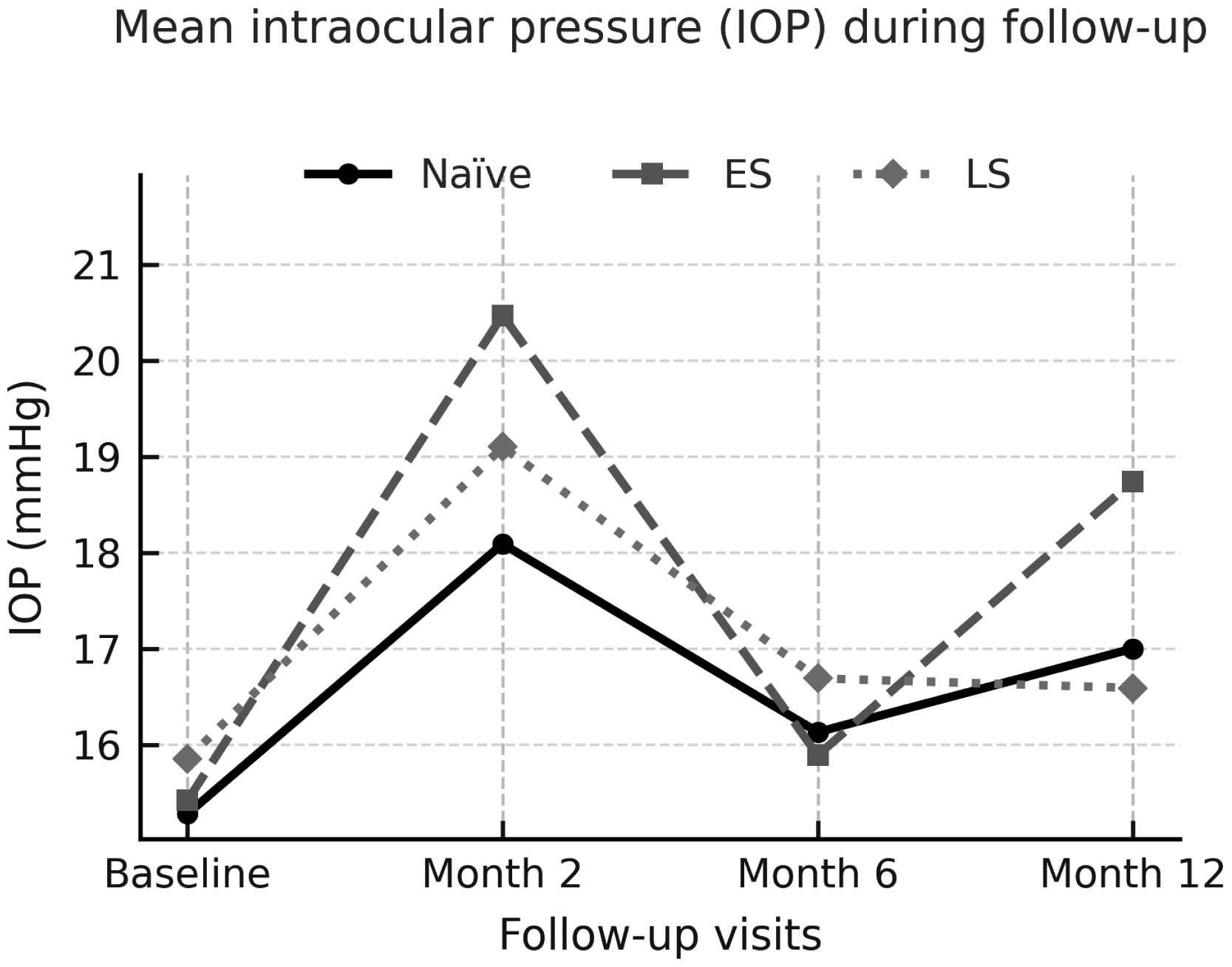
Changes in IOP during the 12 months of follow-up.
At the 2-month follow-up, all groups demonstrated a statistically significant rise in IOP compared with baseline (p < 0.05). The mean increase from baseline was of +2.81 mmHg in naïve eyes, +5.05 mmHg in ES eyes, and +3.25 mmHg in LS eyes. At this visit, 17 out of 71 eyes (24%) exceeded the threshold of 21 mmHg, distributed as follows: 8 naïve eyes, 6 ES eyes, and 3 LS eyes. All cases were subsequently controlled with topical medication or resolved spontaneously during follow-up, and none required glaucoma surgery.
Additional adverse events included cataract progression in one patient and reactivation of herpes keratitis in another.
Multivariate and longitudinal analysis
A multivariate logistic regression analysis was performed to evaluate factors associated with functional and anatomical outcomes at month 2. Baseline BCVA was the only variable significantly associated with ≥2-line visual gain (OR = 161.7, 95% CI: 14.95–3587.76, p = 0.0002), whereas switching timing and other covariates were not independently associated with functional gain. For anatomical response (≥20% CMT reduction), prior anti-VEGF treatment was modelled as a categorical variable (>3 vs ≤ 3 injections, with ≤ 3 as the reference category). Eyes with > 3 prior injections were significantly less likely to achieve anatomical response (OR = 0.17, 95% CI: 0.03–0.74, p = 0.025), corresponding to an approximately 83% reduction in the odds of achieving ≥ 20% CMT reduction compared to those with ≤ 3 injections, while other variables did not reach statistical significance.
In addition, longitudinal analysis using linear mixed-effects models confirmed a significant effect of time on both BCVA and CMT (both p < 0.001), indicating a significant improvement in BCVA and reduction in CMT over follow-up. Age was significantly associated with BCVA evolution (p < 0.001), suggesting an influence of age on visual outcomes. The interaction between time and treatment group showed a borderline effect for BCVA (p = 0.051), indicating a trend toward differential visual evolution between groups, although not reaching statistical significance. A significant statistical interaction between time and treatment group was observed for CMT (p = 0.046), suggesting differences in anatomical response over time according to prior treatment status.
Discussion
ME-RVO remains a major cause of vision loss, and its optimal management continues to represent a therapeutic challenge in real-world practice. Although the efficacy of DEXI has been well established, evidence differentiating outcomes between treatment-naïve, ES, and LS patients remains limited.12,21,22 The present study provides clinical insights by directly comparing anatomical and functional outcomes across these three subgroups and exploring the optimal window for switching to DEXI, thereby addressing a relevant gap in current evidence.15–18,23–30
In ME-RVO with suboptimal response to anti-VEGF therapy, switching to DEXI has been associated with favourable anatomical responses and, in selected cases, meaningful functional recovery. Chiquet et al. and Lee et al. both reported meaningful improvements following DEXI in eyes previously exposed to multiple anti-VEGF injections, supporting corticosteroid use when anti-VEGF response is insufficient.16,25 Notably, Chiquet et al. observed that a higher proportion of patients initially treated with anti-VEGF required switching to DEXI than vice versa (31% vs 13%). 25 In our cohort, DEXI produced consistent anatomical improvement across all subgroups. Although a higher proportion of naïve and ES eyes achieved a clinically meaningful ≥2-line improvement, inter-group comparisons in mean LogMAR BCVA did not reach statistical significance. Furthermore, multivariate analysis identified baseline BCVA, rather than switching timing, as the main independent predictor of functional improvement, suggesting that the observed differences between groups should be interpreted with caution. Longitudinal analysis also suggested that age may influence visual outcomes over follow-up. It also confirmed a significant effect of time on CMT, with modest differences in anatomical evolution across groups. Differences in macular edema chronicity between groups may also have contributed to the observed functional outcomes, as longer duration prior to DEXI administration has been associated with reduced potential for visual recovery.
Previous studies have highlighted the importance of switch timing. Wolfe et al. demonstrated that limited early CMT reduction predicts poor response to continued anti-VEGF treatment, supporting earlier consideration of corticosteroids. 26 Similarly, Yozgat et al. reported better visual outcomes in ES CRVO eyes, consistent with our results. 17 Omar et al. and Pielen et al., both of whom included patients with multiple prior anti-VEGF injections, reported significant anatomical improvement without functional gain after corticosteroid switch, potentially reflecting chronic or irreversible photoreceptor damage.23,24 Our findings extend these observations by providing long-term real-world comparisons across naïve, ES and LS groups, showing that DEXI effectively reduces CMT in all subgroups, whereas functional recovery was mainly observed in naïve and, to a lesser extent, ES eyes. Collectively, these discrepancies reinforce the hypothesis that earlier corticosteroid intervention may preserve retinal integrity and optimise anatomical recovery, although functional recovery appears to be strongly influenced by baseline BCVA.
The differential functional response observed between naïve, ES, and LS patients may be explained by the progressive structural and biochemical alterations occurring in chronic ME. Persistent exposure to elevated VEGF levels and inflammatory cytokines promotes irreversible photoreceptor and retinal pigment epithelium damage, as well as gliosis, which reduce the potential for functional recovery despite subsequent anatomical improvement.31–34 Early corticosteroid intervention may therefore modulate inflammation, stabilise the blood–retinal barrier, and prevent permanent retinal disorganisation, potentially contributing to improve structural outcomes and supporting visual recovery when baseline retinal integrity is preserved.12,26 In addition, retinal ischemia may further contribute to disease severity and is a recognised prognostic factor in RVO, being associated with worse BCVA and greater CMT.35–37 However, ischemic status was not systematically documented in our retrospective cohort and therefore could not be included as an analytical variable.
The safety profile observed in our cohort aligns with previous reports. Transient IOP elevations above 21 mmHg occurred in 24% of eyes, affecting all groups, all of which were subsequently controlled with topical hypotensive therapy or resolved spontaneously. Similar rates (15–30%) and timing—peaking at 1–2 months and resolving with medical treatment—have been reported.12,18,21,22
These findings have clinical relevance for guiding therapeutic decisions in ME-RVO. Functional recovery occurred mainly in naïve eyes, and to a lesser extent, in ES eyes, suggesting that earlier consideration of DEXI may be associated with a higher likelihood of visual benefit in patients with suboptimal anti-VEGF response, although functional outcomes remain primarily influenced by baseline BCVA. Conversely, the lack of functional gains in LS eyes despite anatomical reductions may indicate reduced potential after prolonged edema. Integrating early anatomical response and prior treatment exposure into routine assessment may therefore help identify candidates who could benefit from an earlier switch.
This study has limitations that should be acknowledged. Its retrospective design may introduce selection bias and limits causal inference. Ischemic status was not systematically documented and therefore was not included in the analysis. Consequently, its potential influence on treatment response cannot be excluded and should be considered when interpreting the results. The sample size, while comparable to similar real-world reports, may be insufficient to detect subtle subgroup differences, and it did not allow separate analyses of BRVO and CRVO. However, the distribution of occlusion types was comparable across naïve, ES, and LS groups, helping to maintain subgroup homogeneity. Despite these limitations, this study has notable strengths. The sample was well balanced across subgroups, reducing potential confounding in the comparison between groups. To our knowledge, this is the first study to directly stratify outcomes by timing of switch, including comparisons with a naïve cohort, thereby providing novel insights into the optimal therapeutic window for DEXI monotherapy. Finally, the real-world design enhances the external validity and clinical applicability. Further studies are warranted to validate these findings, address the limitations of the present analysis, and refine treatment algorithms for patients with ME-RVO.
Conclusion
Overall, functional and anatomical responses to DEXI in ME-RVO appear to be influenced by prior treatment history and baseline visual status. By directly comparing naïve, ES, and LS eyes, this study provides new insights into the treatment patterns and clinical evolution in patients with suboptimal anti-VEGF response. Although naïve and ES eyes showed a higher proportion of clinically meaningful visual improvement, multivariate analysis identified baseline BCVA, rather than switching timing, as the main independent predictor of functional recovery. Anatomical benefits were observed across all groups. Together, these findings may assist clinicians in refining treatment decisions for patients insufficiently responsive to anti-VEGF agents.
Footnotes
Ethical approval and informed consent statements
This study was approved by the local Ethics Committee in accordance with the tenets of the 1964 Declaration of Helsinki and its later amendments for research involving human subjects. Due to the retrospective nature of the study, individual informed consent was waived by the ethics committee.
Consent to participate
Not applicable (retrospective study with waived consent)
Consent for publication
Not applicable (the manuscript contains no identifiable personal data, images, or videos from individual participants).
Author contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Due to patient confidentiality and ethical restrictions, the dataset generated for this study is not publicly available. Data may be obtained from the corresponding author on reasonable request and subject to institutional approval.
No additional identifying information related to the authors, institutions, funders, or approval committees is included that might compromise anonymity during the review process.
New affiliation
Olga Diego Navarro has moved to University Hospital of Ciudad Real since completing the research.