
Abstract
Purpose
Restrictive strabismus is a major cause of diplopia and impaired quality of life in thyroid eye disease (TED), but its clinical and imaging characteristics remain incompletely understood. This study investigated the clinical and magnetic resonance imaging (MRI) characteristics of TED patients with restrictive strabismus at initial presentation.
Methods
Among 5,234 TED patients treated between 2009 and 2024, 339 patients (6.5%) with clinically confirmed restrictive strabismus and supportive MRI findings were retrospectively included. Restrictive strabismus was confirmed primarily by positive forced duction testing with limitation of ocular rotations. Clinical characteristics, thyroid function, Clinical Activity Score (CAS), NOSPECS classification, strabismus type, and orbital MRI findings were analyzed. Contrast-enhanced orbital MRI, including T1-weighted and fat-suppressed T2-weighted sequences, was used to evaluate extraocular muscle enlargement, inflammation, and edema.
Results
Patients with active extraocular muscles had higher CAS scores than those with stable muscles (P < 0.01). Monocular-onset patients showed higher CAS and NOSPECS scores (both P < 0.01). Hyperthyroid patients had higher NOSPECS scores than euthyroid patients (P < 0.01). Longer disease duration before presentation was associated with smaller muscle area, less inflammation, and reduced edema, whereas higher CAS scores correlated with larger muscle area and more severe edema.
Conclusions
TED patients with restrictive strabismus were predominantly male and commonly showed binocular involvement and hyperthyroidism. Inferior rectus involvement was the most common imaging finding, especially in vertical strabismus. Orbital MRI may help evaluate extraocular muscle activity and guide strabismus surgery timing.
Introduction
Thyroid eye disease (TED) is an autoimmune inflammatory orbital disorder associated with thyroid dysfunction and is the most common orbital disease encountered clinically.1,2 Clinical manifestations include eyelid retraction, proptosis, exposure keratopathy, diplopia, restrictive strabismus, and optic neuropathy. 3 Diplopia is one of the major symptoms affecting quality of life in TED patients and is usually caused by restrictive strabismus secondary to inflammation, enlargement, and fibrosis of the extraocular muscles.
TED patients with restrictive strabismus commonly present because of binocular diplopia rather than awareness of the restrictive process itself. Previous imaging studies have demonstrated that orbital magnetic resonance imaging (MRI) is valuable for evaluating extraocular muscle enlargement, inflammatory activity, edema, and fibrosis in TED. 4 MRI findings may also help determine disease activity and guide the timing of surgical intervention.
Previous studies have described the frequency of extraocular muscle involvement and the clinical course of TED.5–8 However, relatively few studies have specifically focused on TED patients presenting with restrictive strabismus, particularly regarding the relationship between strabismus type, MRI findings, disease activity, and extraocular muscle characteristics. Understanding these features is clinically important because patients with active extraocular muscle inflammation may experience unstable ocular deviation and poor surgical outcomes if strabismus surgery is performed prematurely. 9
Therefore, the present study aimed to investigate the clinical characteristics, MRI findings, and factors associated with extraocular muscle involvement in TED patients with restrictive strabismus at their initial presentation
Materials and methods
Population enrollment
Among 5,234 patients diagnosed with thyroid eye disease (TED) at the Department of Ophthalmology, West China Hospital, Sichuan University between 2009 and 2024, 367 patients with restrictive strabismus were initially identified. Restrictive strabismus was confirmed primarily by positive forced duction testing together with limitation of ocular rotations on clinical examination. Orbital MRI was used as an adjunctive structural evaluation. Therefore, the present study included patients with clinically confirmed restrictive strabismus rather than suspected restrictive disease.
Inclusion criteria were: (1) Diagnosis of TED based on Bartley diagnostic criteria 10 ; (2) Clinically confirmed restrictive strabismus; (3) Complete clinical and orbital MRI data at the first hospital visit. Exclusion criteria were: (1) Other orbital or neurological disorders causing restrictive strabismus; (2) Previous orbital or strabismus surgery; (3) Significantly incomplete medical records or imaging data.
After application of the inclusion and exclusion criteria, 339 patients were retrospectively included in the final analysis. Patients were subsequently classified into pure vertical strabismus, pure horizontal strabismus, or mixed vertical-horizontal strabismus groups. The patient enrollment process is summarized in Figure 1.
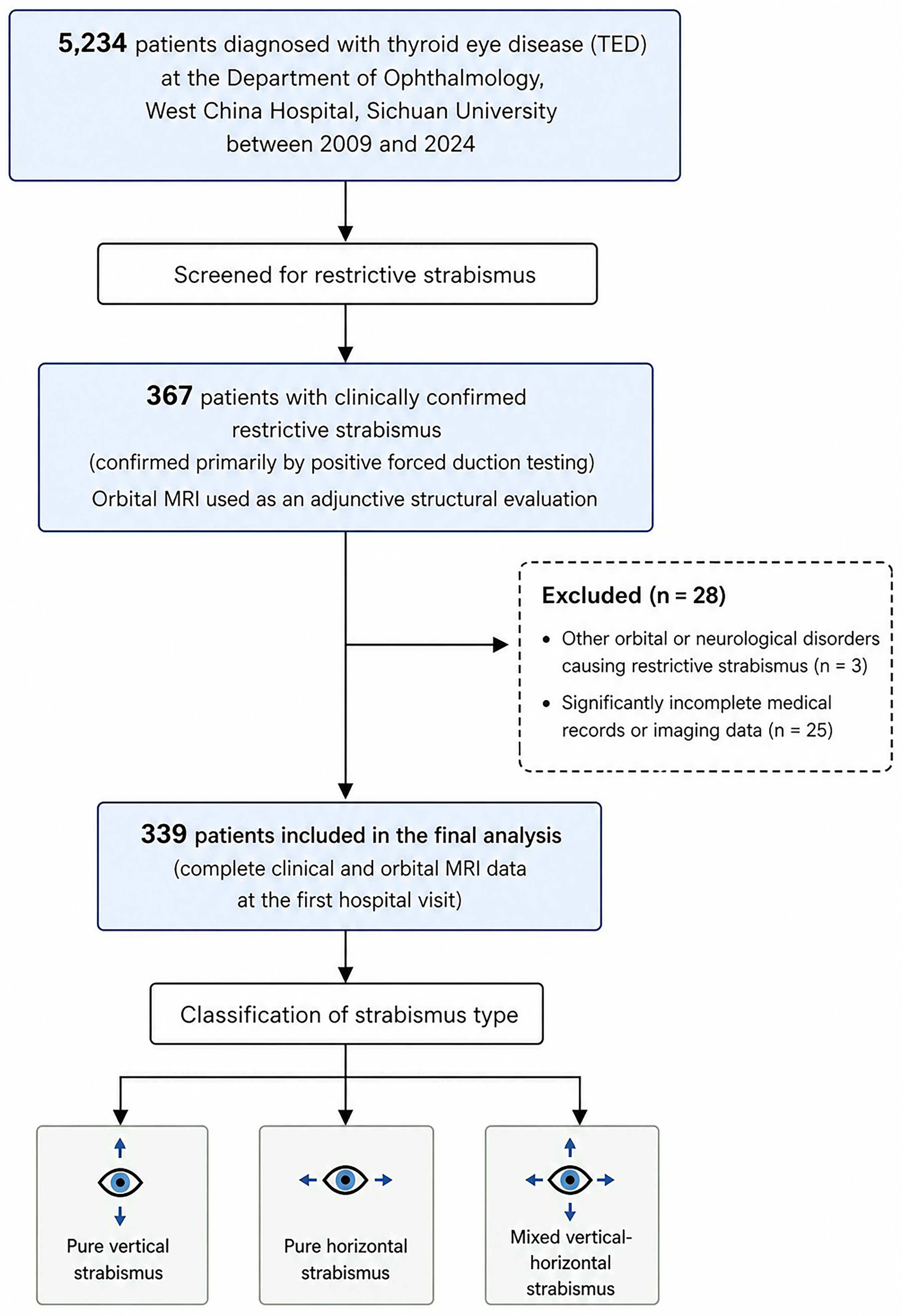
Flow diagram of patient enrollment and study population selection.
Patient evaluation
Patient data were collected, including sex, age at disease onset, affected eye(s), time interval between symptom onset and first hospital visit, condition of the extraocular muscles, smoking history, type of strabismus, Clinical Activity Score (CAS),5,11 NOSPECS, 12 and thyroid function.
MRI evaluation of extraocular muscle activity
Measurements were performed on coronal orbital MRI sections routinely acquired in the institutional orbital imaging protocol. The maximum cross-sectional area of the affected extraocular muscle at the level of maximal enlargement, as well as the enhancement ratio on contrast-enhanced T1-weighted imaging and fat-suppressed T2-weighted imaging (T2WI-FS), were measured using the YINGLIAN imaging system's built-in software. Orbital contrast-enhanced T1-weighted imaging was used to evaluate extraocular muscle inflammation, while T2WI-FS was used to evaluate extraocular muscle edema. The signal intensity of the affected extraocular muscle was compared with that of the ipsilateral temporalis muscle. Extraocular muscles were considered active when the signal intensity ratio on either contrast-enhanced T1-weighted imaging or T2WI-FS exceeded that of the ipsilateral temporalis muscle. For contrast-enhanced T1-weighted imaging, a signal intensity ratio increase of >0% and <30% was defined as mild inflammation, 30%–60% as moderate inflammation, and >60% as severe inflammation. For T2WI-FS, a signal intensity ratio increase of >0% and <30% was defined as mild edema, 30%–60% as moderate edema, and >60% as severe edema. Stable extraocular muscles were defined as enlarged extraocular muscles without increased signal intensity on either contrast-enhanced T1-weighted imaging or T2WI-FS. Active extraocular muscles were defined as enlargement of one or more extraocular muscles with increased signal intensity on either sequence. 4
Statistical analysis
Data from both eyes were analyzed using SAS software (version 9.4). For quantitative data, the mean ± standard deviation was used, and categorical variables were expressed as frequencies and percentages. The Kolmogorov ‒ Smirnov test was used to test the normality of variables. A linear mixed model or generalized estimating equations (GEE) approach were used to explore the influencing factors of CAS, NOSPECS, the maximum area of the coronal position of the affected extraocular muscle, the edema and inflammation of the affected extraocular muscle, etc. A P value < 0.05 was considered statistically significant.
Results
The basic characteristics of the research subjects
Among 5,234 TED patients screened during the study period, 339 patients (6.5%) with restrictive strabismus met the inclusion criteria and were analyzed.
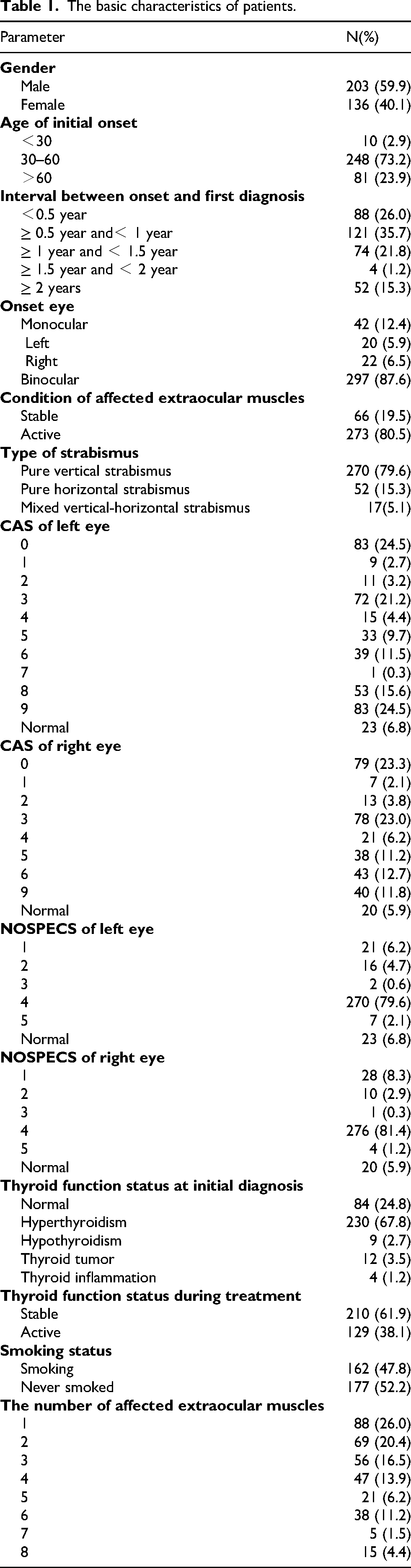
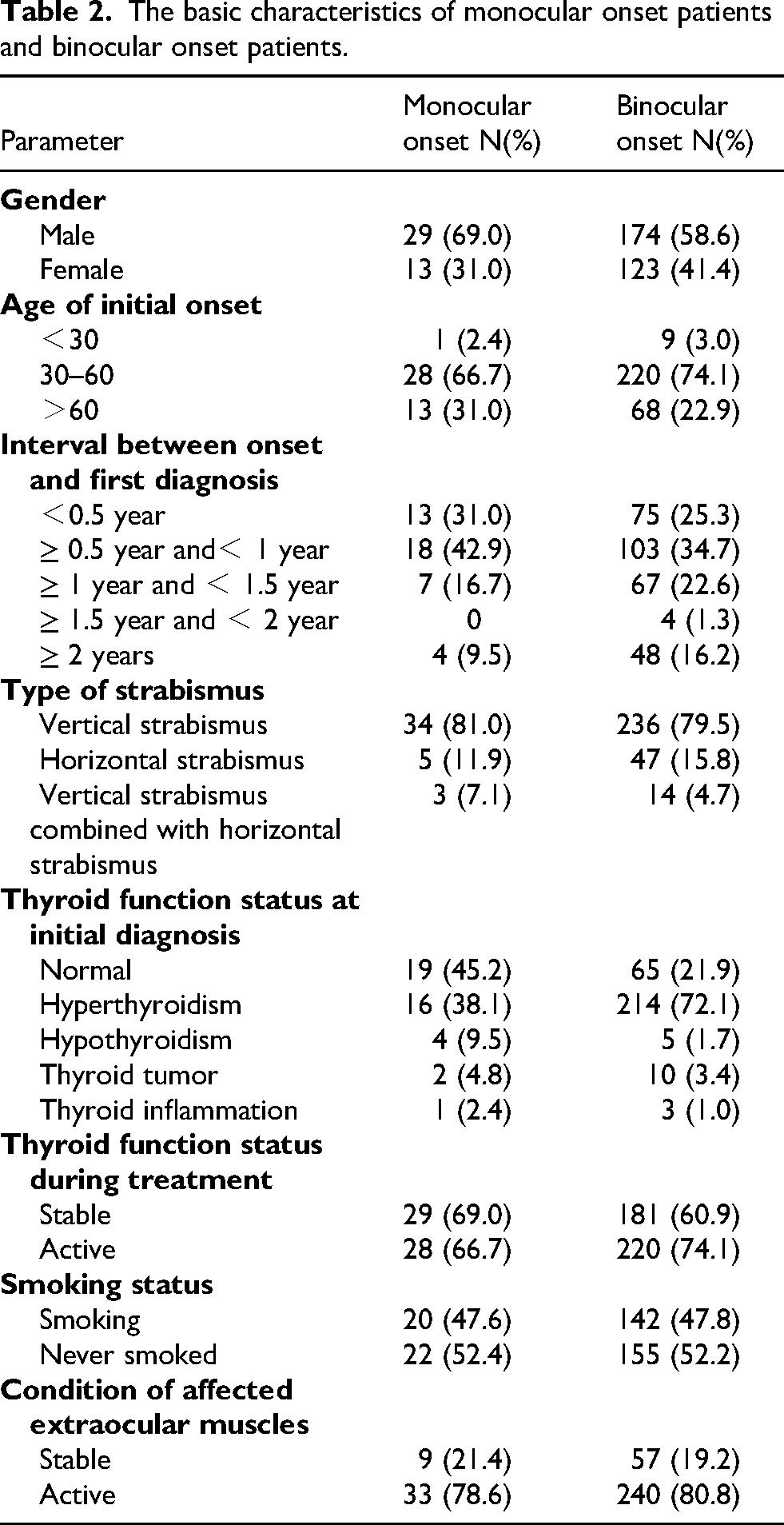
A total of 203 patients (59.9%) were male and 136 (40.1%) were female, with a mean age of 52.17 ± 10.88 years. The characteristics of the participants are summarized in Table 1. Binocular onset was more common than monocular onset (Table 2).
The basic characteristics of patients.
The basic characteristics of monocular onset patients and binocular onset patients.
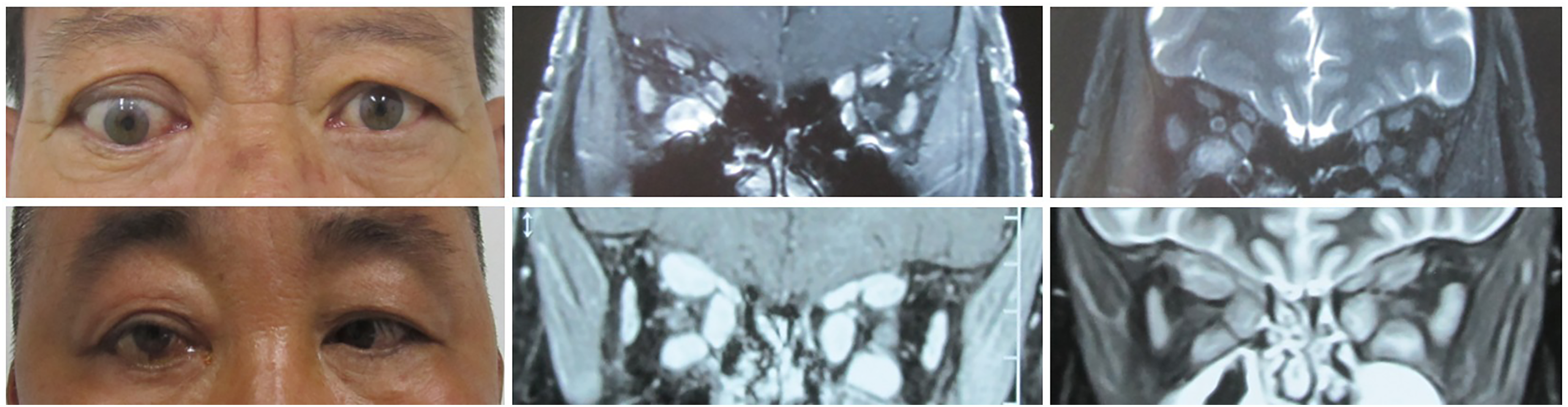
At the initial visit, extraocular muscles were active in 80.5% of patients and stable in 19.5%. All patients showed varying degrees of extraocular muscle thickening; 79.9% had inflammation, and 46.3% had edema. Additionally, 30.38% of patients had a CAS ≤ 3 despite having active extraocular muscles. Figure 2 presents the ocular appearance and orbital contrast-enhanced MRI images of patients with active extraocular muscles and either low or high CAS. Among patients with multiple muscle involvement, 88.4% exhibited varying degrees of inflammation and edema across different affected muscles. Details of the affected extraocular muscles are shown in Table 3.
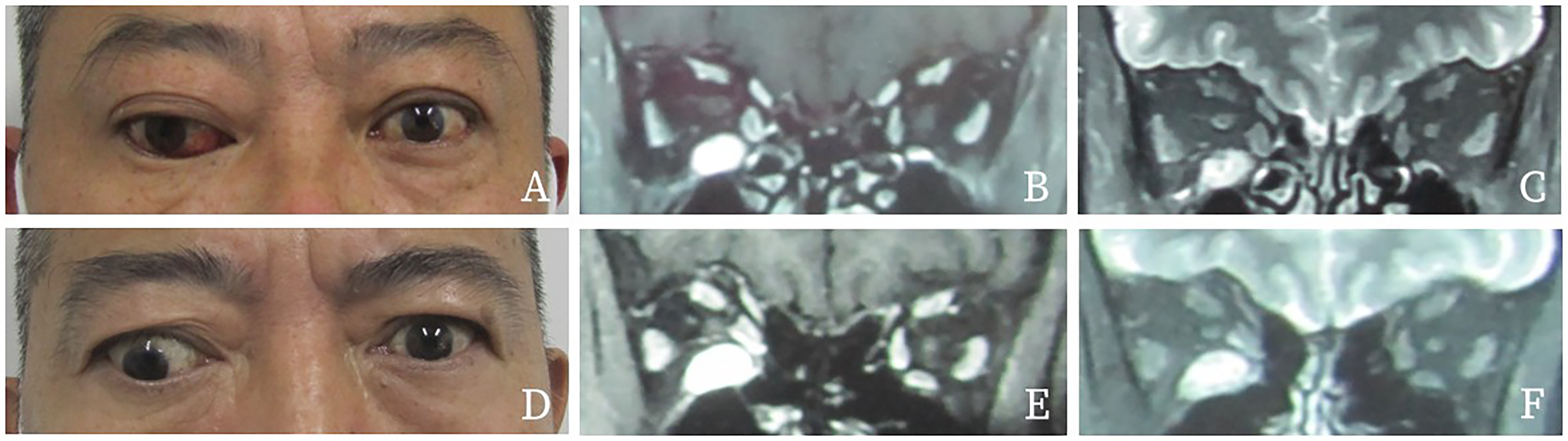
Legends, (A, B, C): A patient with high CAS. A shows the image of ocular appearance. B shows T1-weighted images and C shows the T2-weighted images of orbital enhanced MRI, indicating that the patient had inflammation and edema in the right inferior rectus muscle; (D, E, F): A patient with low CAS. D shows the image of ocular appearance. E shows T1-weighted images and F shows the T2-weighted images of orbital enhanced MRI, indicating that the patient had inflammation and edema in the right inferior rectus muscle.
The condition of the involved extraocular muscle of patients.
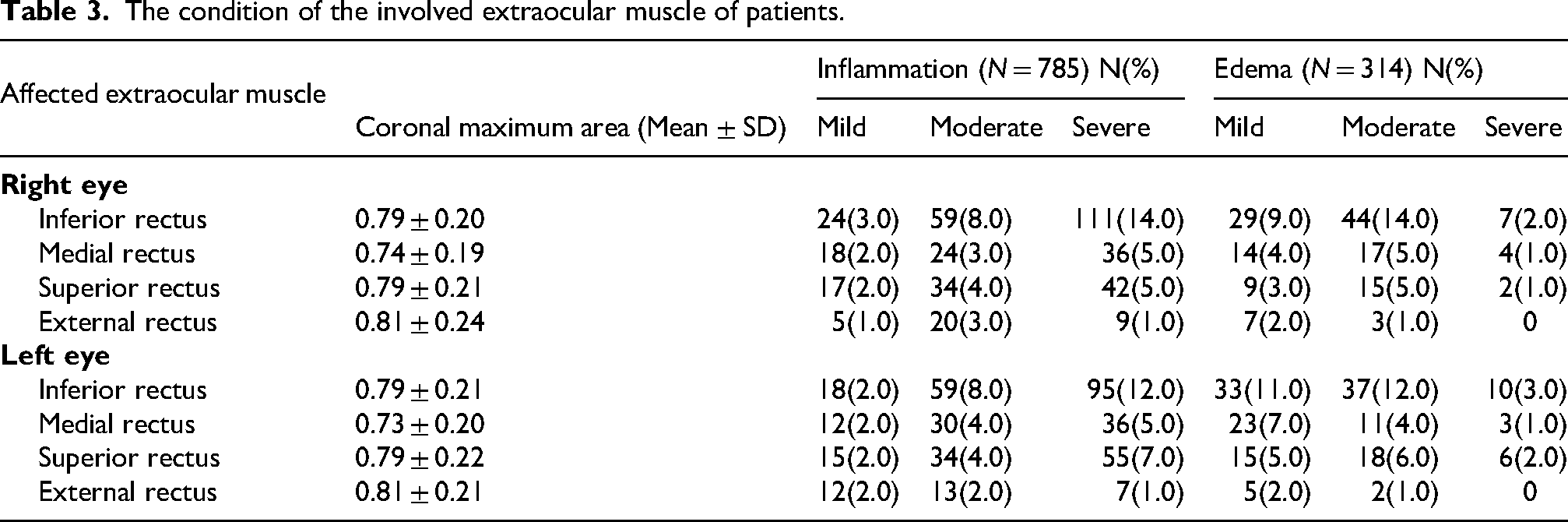
In patients with vertical strabismus, the most frequently involved muscles were, in descending order, the inferior rectus (49.6%), superior rectus (26.3%), medial rectus (15.9%), and lateral rectus (8.2%). In horizontal strabismus, involvement rates were highest for the inferior rectus (34.2%), followed by the medial rectus (30.9%), superior rectus (23.6%), and lateral rectus (11.3%).
For vertical strabismus, the top three patterns of muscle involvement were: right inferior rectus (13.5%), left inferior rectus (11.3%), and bilateral inferior rectus (9.6%). For horizontal strabismus, the top three patterns were: bilateral involvement of the inferior, medial, and superior rectus muscles (22.8%); all four rectus muscles bilaterally (12.3%); and bilateral inferior and medial rectus involvement (10.5%).
Figure 3 illustrates the ocular appearance and orbital contrast-enhanced MRI findings in patients with vertical and horizontal strabismus.
Legends, (A, B, C): A patient with vertical strabismus. A shows the image of ocular appearance. B shows T1-weighted images and C shows the T2-weighted images of orbital enhanced MRI, indicating that the patient had inflammation and edema in the right inferior rectus muscle; (D, E, F): A patient with horizontal strabismus. D shows the image of ocular appearance. E shows T1-weighted images and F shows the T2-weighted images of orbital enhanced MRI, indicating that the patient had inflammation and edema in the inferior rectus, medial rectus and superior rectus of both eyes.
Risk factors affecting CAS and NOSPECS in patients
Univariate generalized linear regression analysis was performed, and variables with P < 0.10 were considered to have a statistically significant impact on the outcome. Variables found to be significant in the univariate analysis were included in the multivariate analysis. Subsequently, multivariate generalized linear regression analysis was conducted. Variables with P < 0.05 were considered independent risk factors.
Multivariate analysis demonstrated that CAS scores were significantly higher in patients with active extraocular muscles than in those with stable extraocular muscles (P < 0.01). Patients with monocular onset had significantly higher CAS scores than those with binocular onset (P < 0.01) (see Table 1). NOSPECS scores were significantly higher in patients with hyperthyroidism compared to those with normal thyroid function (P < 0.01). Patients with monocular onset also had significantly higher NOSPECS scores than those with binocular onset (P < 0.01) (Supplementary Table 1).
Risk factors affecting the condition of affected extraocular muscles
Univariate generalized linear regression analysis was performed, and variables with P < 0.10 were considered to have a statistically significant impact on the outcome. Significant variables from the univariate analysis were included in the multivariate analysis. Multivariate generalized linear regression analysis was subsequently performed. Variables with P < 0.05 were considered independent risk factors.
Multivariate analysis further demonstrated that a longer interval between disease onset and the first hospital visit was associated with a smaller maximum cross-sectional area of the affected extraocular muscle in the coronal plane (P < 0.05). Higher CAS scores in the left eye were associated with a larger maximum cross-sectional area of the affected extraocular muscle in the left eye (P < 0.01), and similarly, higher CAS scores in the right eye were associated with a larger maximum area of the affected muscle in the right eye (P < 0.01) (Supplementary Table 2). A longer interval between disease onset and the first hospital visit was also associated with a lower degree of edema in the affected extraocular muscle (P < 0.05). Higher CAS scores in the left and right eyes were both associated with more severe edema in the corresponding affected muscles (P < 0.01) (see Table 2). In addition, a longer interval between onset and the first visit was also associated with a lower degree of inflammation in the affected extraocular muscle (P < 0.01) (Supplementary Table 2).
Discussion
In this retrospective study of 339 TED patients with restrictive strabismus, we found that most patients were male, had binocular involvement, and demonstrated MRI evidence of active extraocular muscle disease at presentation. Inferior rectus involvement was the predominant imaging finding, particularly in patients with vertical strabismus. In addition, higher CAS scores were associated with greater extraocular muscle enlargement and edema, whereas delayed presentation was associated with reduced inflammatory activity and smaller extraocular muscle size.
Restrictive strabismus represents a clinically important subgroup of TED because ocular motility limitation and diplopia significantly impair daily activities and quality of life. Unlike diplopia, which is a patient-reported symptom, restrictive strabismus is a clinician-confirmed diagnosis resulting from inflammatory enlargement and fibrosis of the extraocular muscles. In the present study, the mean age of patients was approximately 52 years, and male patients accounted for the majority of the cohort. Among all included patients, 12.4% had monocular onset, which is consistent with the findings of Kashkouli et al.. 13 In addition, patients with monocular onset showed significantly higher CAS and NOSPECS scores than those with binocular onset, suggesting greater disease severity at presentation.
Thyroid dysfunction is closely associated with the onset and severity of TED. Previous studies involving European and Asian TED populations have reported that approximately 80%–90% of TED patients have abnormal thyroid function. 14 In our study, 75.2% of TED patients with restrictive strabismus had thyroid dysfunction, with hyperthyroidism being the predominant subtype (67.8%). Furthermore, hyperthyroid patients demonstrated significantly higher NOSPECS scores than euthyroid patients, indicating more severe orbital involvement. Although previous studies suggested that smoking and male sex may influence disease activity and severity in TED,15,16 we did not observe significant associations between smoking, sex, and CAS or NOSPECS scores in this restrictive strabismus subgroup. One possible explanation is that patients with restrictive strabismus already exhibited relatively severe extraocular muscle involvement at presentation.
Previous MRI studies of TED have consistently reported that the inferior rectus muscle is the most frequently involved extraocular muscle,5–8 which is consistent with our findings. In our study, among patients with pure vertical strabismus, the inferior rectus muscle was the most commonly affected muscle, followed by the superior rectus, medial rectus, and lateral rectus muscles. This finding is consistent with the known relationship between inferior rectus involvement and vertical ocular deviation in TED. In contrast, among patients with pure horizontal strabismus, medial rectus involvement was relatively more frequent, although inferior rectus involvement remained the most common overall finding. These imaging patterns may partly explain the different forms of ocular deviation observed in TED patients.
Importantly, patients with mixed vertical-horizontal strabismus were also present in our cohort and accounted for 5.1% of all patients. However, because the sample size of this subgroup was relatively small, further subgroup analysis was not statistically feasible. Therefore, conclusions regarding muscle involvement patterns were primarily based on the pure vertical and pure horizontal strabismus groups.
Orbital MRI played an important role in evaluating disease activity in this cohort. At the initial visit, 80.5% of patients demonstrated MRI-defined active extraocular muscles, 79.9% showed inflammation, and 46.3% showed edema. Notably, more than 30% of patients with active extraocular muscles had CAS scores ≤3. These findings suggest that CAS alone may not fully reflect MRI-defined extraocular muscle activity in some TED patients with restrictive strabismus. In the present study, extraocular muscle activity was evaluated using contrast-enhanced T1-weighted imaging for inflammation assessment and fat-suppressed T2-weighted imaging for edema assessment. The signal intensity of the affected muscle was compared with that of the ipsilateral temporalis muscle using the YINGLIAN imaging system. These findings indicate that orbital MRI may provide complementary information regarding disease activity in TED patients with restrictive strabismus.
Our statistical analyses further demonstrated that shorter disease duration and higher CAS scores were associated with larger extraocular muscle cross-sectional area and more severe edema. In contrast, longer disease duration was associated with lower inflammatory activity. These findings may reflect the pathological progression of TED-associated extraocular muscle changes. During the early active phase, lymphocytic infiltration, vasodilation, and glycosaminoglycan accumulation produce edema and muscle enlargement, whereas later stages are characterized by progressive fibrosis and gradual resolution of inflammation and edema. 3 Our findings are consistent with this pathological progression model.
These findings may have clinical implications regarding the timing of strabismus surgery. Surgical correction is usually considered after the extraocular muscle condition becomes clinically and radiologically stable. Therefore, patients with restrictive strabismus, particularly those with persistent MRI evidence of inflammation or edema despite low CAS scores, should undergo careful orbital MRI evaluation before surgical intervention to confirm extraocular muscle stability.
This study has several limitations. First, because of its retrospective single-center design, referral and selection bias may exist. Second, some subgroup analyses could not be further performed because several subgroups contained relatively small sample sizes, resulting in insufficient statistical power. Third, MRI acquisition spanned a 15-year study period, which may have introduced some variability in imaging quality and measurement methods despite the use of standardized institutional protocols. Finally, this study included only a Chinese population, which may limit the generalizability of the findings to other populations.
Conclusion
Among patients with thyroid eye disease and restrictive strabismus, males, binocular involvement, and hyperthyroidism were predominant clinical features. Inferior rectus involvement was the most common imaging finding, particularly in vertical strabismus. MRI evidence of inflammation and edema was strongly associated with higher disease activity, whereas delayed presentation was associated with reduced inflammatory changes and smaller extraocular muscle size. Orbital MRI may therefore provide important information for evaluating extraocular muscle activity and determining the optimal timing of strabismus surgery in TED patients with restrictive strabismus.
Supplemental Material
sj-docx-1-ejo-10.1177_11206721261461917 - Supplemental material for Clinical characteristics of thyroid eye disease with restrictive strabismus
Supplemental material, sj-docx-1-ejo-10.1177_11206721261461917 for Clinical characteristics of thyroid eye disease with restrictive strabismus by Hao Zhang and Weimin He in European Journal of Ophthalmology
Supplemental Material
sj-docx-2-ejo-10.1177_11206721261461917 - Supplemental material for Clinical characteristics of thyroid eye disease with restrictive strabismus
Supplemental material, sj-docx-2-ejo-10.1177_11206721261461917 for Clinical characteristics of thyroid eye disease with restrictive strabismus by Hao Zhang and Weimin He in European Journal of Ophthalmology
Footnotes
Informed consent
Not applicable.
Authors’ contributions
HZ collected the data and wrote the first draft of the manuscript. WH helped to provide the clinical advice and interpreted clinical data and provided supplemented, perfected and revised the first draft of the manuscript. All authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Since the original data belong to West China Hospital of Sichuan University, data sets generated during the current study are available from the corresponding author on reasonable request.
Institutional review board statement
All procedures performed in studies involving human participants were in accordance with the ethical standards of the Biomedical Ethics Sub-Committee of the West China Hospital of Sichuan University and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.