
Abstract
Purpose
To evaluate the association between systemic tocilizumab exposure and the development of age-related macular degeneration (AMD) in a large real-world cohort.
Methods
This was a retrospective, propensity-matched cohort study including patients aged ≥40 years in the TriNetX Research Network with or without exposure to tocilizumab between May 2008 and May 2025. Patients with documented tocilizumab use were matched 1:1 to controls based on demographic and clinical characteristics within the TriNetX platform. Individuals with prior AMD were excluded from incident analyses. Risk ratios (RRs) and 95% confidence intervals (CIs) were calculated for incident non-exudative and exudative AMD.
Results
After propensity score matching, 23,456 patients were included per group. Tocilizumab use was associated with a significantly lower risk of incident non-exudative AMD (RR, 0.282; 95% CI, 0.230–0.346; p < 0.001) and incident exudative AMD (RR, 0.234; 95% CI, 0.159–0.344; p < 0.001) compared with matched controls.
Conclusions
Systemic tocilizumab exposure was associated with a lower incidence of both non-exudative and exudative AMD in this real-world cohort. These findings should be considered hypothesis-generating and support further study of the relationship between IL-6 signaling and AMD.
Introduction
Age-related macular degeneration (AMD) is a leading cause of irreversible vision loss in older adults worldwide. 1 It is broadly classified into non-exudative (dry) and exudative (wet) forms. Dry AMD is characterized by drusen accumulation and geographic atrophy and typically progresses slowly, 2 whereas wet AMD is defined by choroidal neovascularization and can lead to rapid vision loss if untreated. 3
Current management strategies for non-exudative AMD involve lifestyle modifications, including smoking cessation, nutritional supplementation with antioxidants as demonstrated by the Age-Related Eye Disease Study (AREDS2), 4 and, recently, complement inhibitors such as Pegcetacoplan (C3 inhibitor) 5 and Avacincaptad pegol (C5 inhibitor) 6 which slow the progression of geographic atrophy when administered intravitreally . In contrast, the standard treatment for wet AMD primarily involves intravitreal injections of anti-vascular endothelial growth factor (anti-VEGF) agents, including bevacizumab, ranibizumab, aflibercept, brolucizumab, and faricimab, aimed at reducing vascular permeability and suppressing neovascular growth.7–10 Despite their efficacy, a significant proportion of patients exhibit incomplete responses or require frequent injections, underscoring the need for alternative therapeutic targets and strategies. 11
Recent research highlights inflammation, particularly the proinflammatory cytokine interleukin-6 (IL-6), as a critical contributor to AMD pathogenesis. Elevated IL-6 levels have been documented both systemically and intraocularly in AMD patients, correlating positively with macular edema and CNV severity.12–14
Tocilizumab, a monoclonal antibody targeting the IL-6 receptor (IL-6R), inhibits downstream inflammatory pathways and is FDA-approved for rheumatoid arthritis, giant cell arteritis, polyarticular juvenile idiopathic arthritis, systemic juvenile idiopathic arthritis, and cytokine release syndrome.15–18 Experimental models reveal that tocilizumab effectively suppresses corneal neovascularization following alkali injuries by downregulating VEGF expression. 19 Moreover, Tocilizumab has been reported to attenuate laser-induced CNV in murine models by inhibiting IL-6R signaling and modulating macrophage polarization through suppression of the STAT3/VEGF pathway. 20
This study aims to investigate the risk of developing non-exudative and exudative age-related macular degeneration (AMD) in patients receiving tocilizumab, using a large clinical database.
Methods
We conducted a retrospective cohort study using the TriNetX Research Network, a federated electronic health record system encompassing over 115 million patients from 56 U.S. healthcare organizations. All data were de-identified and HIPAA-compliant; Institutional Review Board approval was not required.
Patients aged 40 years or older with documented use of tocilizumab between May 1, 2008, and May 1, 2025, were included as the exposed group, with the index date defined as the first recorded administration. The comparator group comprised patients without any history of tocilizumab use but with a documented ophthalmic screening or examination (ICD-10: Z01.0 or Z13.5) during the same period. The index date for controls was the date of the first qualifying eye-related encounter. The control cohort was defined using documented ophthalmic screening or examination codes to ensure prior eye care contact, consistent with the general approach used in prior TriNetX-based AMD studies. 21
Propensity score matching (PSM) was performed within the TriNetX platform in a 1:1 ratio using greedy nearest-neighbor matching on the listed covariates. Matching variables included age, sex, race, ethnicity, nicotine dependence, alcohol-related disorders, diabetes mellitus, hypertensive disease, ischemic heart disease, cerebrovascular disease, rheumatoid arthritis with rheumatoid factor, other rheumatoid arthritis, giant cell arteritis, and polymyalgia rheumatica.
Two primary outcome analyses were conducted. For incident non-exudative AMD, patients with a diagnosis of dry AMD (ICD-10: H35.30 or H35.31) before the start of the analysis window were excluded, and the outcome was defined as a new diagnosis recorded beginning 365 days after the index date. For incident exudative AMD, patients with a diagnosis of neovascular AMD (ICD-10: H35.32) before the start of the analysis window were excluded, and the outcome was defined as a new diagnosis recorded beginning 365 days after the index date. Sensitivity analyses were performed by restricting the exposed cohort to patients with at least 3 documented tocilizumab administrations and, separately, by restricting both cohorts to patients aged 50 years or older. To better address confounding by indication, we performed an active-comparator sensitivity analysis using patients treated with TNF inhibitors (adalimumab, infliximab, certolizumab pegol, etanercept, or golimumab) as the comparator cohort. As an additional sensitivity analysis, we restricted outcome ascertainment to a fixed interval from 1 year to 5 years after the index date.
Statistical analyses were conducted within the TriNetX platform. Risk ratios (RRs) and 95% confidence intervals (CIs) were calculated for all outcomes. A two-tailed p-value < 0.05 was considered statistically significant. Patients with the outcome prior to the analysis window were automatically excluded by the platform.
Results
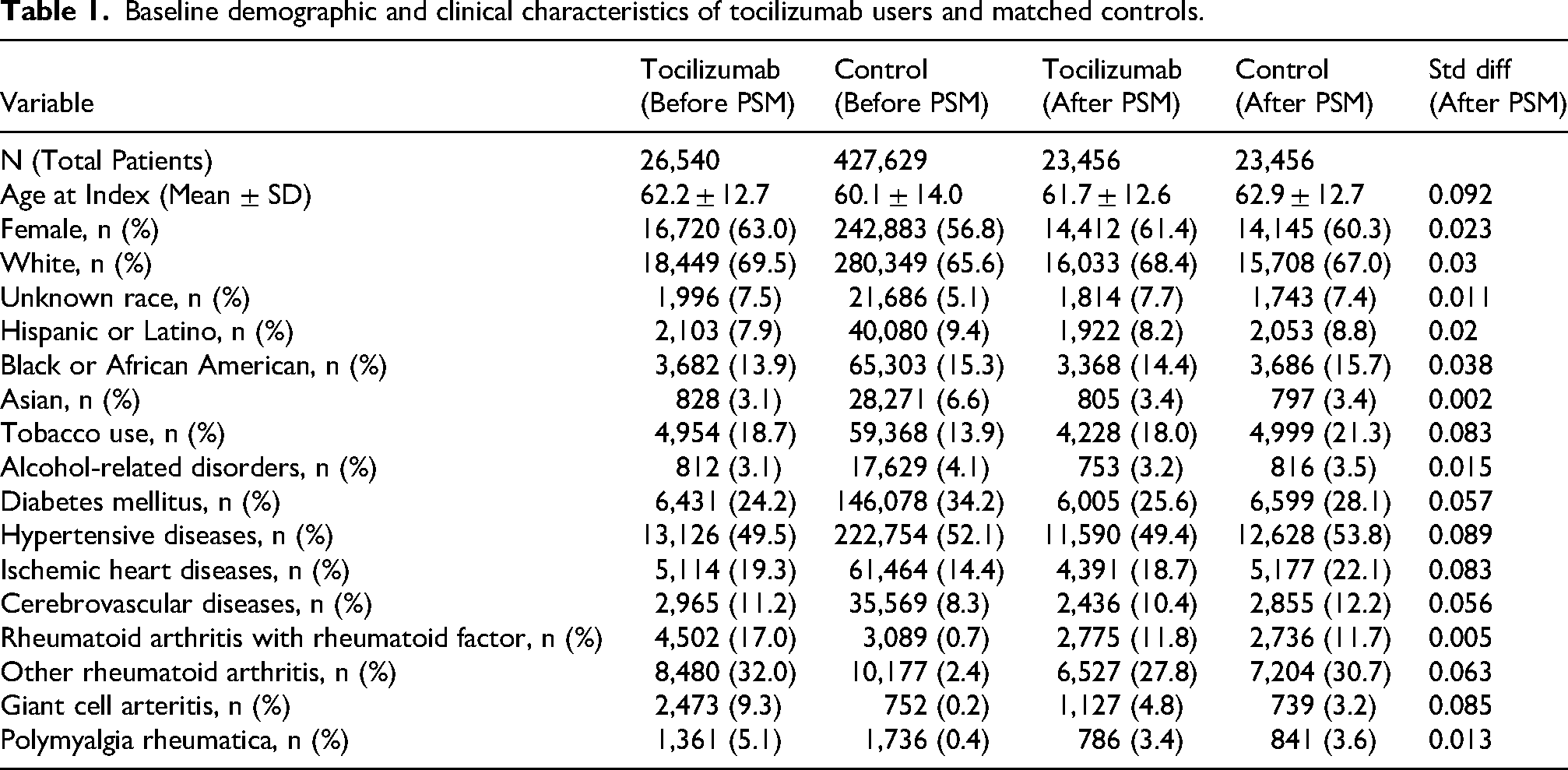
After propensity score matching, 23,456 patients were included in each of the tocilizumab and control cohorts. Baseline demographic and clinical characteristics were generally similar between groups after propensity score matching (Table 1). The mean age at index was 61.7 ± 12.6 years in the tocilizumab group and 62.9 ± 12.7 years in the control group, and 61.4% and 60.3% of patients were female, respectively. Most participants were White (68.4% in the tocilizumab group vs 67.0% in controls), followed by Black or African American (14.4% vs 15.7%). The prevalence of major systemic comorbidities was similar, including diabetes mellitus (25.6% vs 28.1%), hypertensive disease (49.4% vs 53.8%), ischemic heart disease (18.7% vs 22.1%), and cerebrovascular disease (10.4% vs 12.2%).
Baseline demographic and clinical characteristics of tocilizumab users and matched controls.
Incident dry AMD
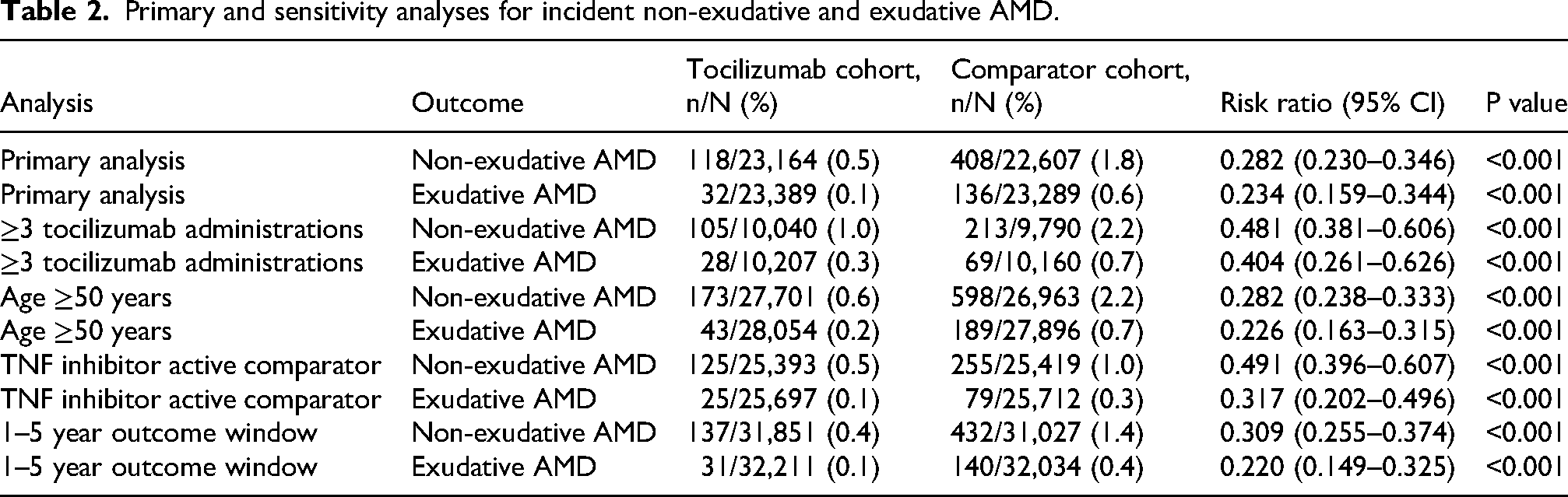
Among patients without pre-existing dry AMD, 118 individuals (0.5%) in the tocilizumab group developed new-onset dry AMD compared with 408 (1.8%) in the control group. Tocilizumab use was associated with a significantly lower risk of incident dry AMD (RR 0.282; 95% CI, 0.230–0.346; p < 0.001).
Incident exudative AMD
Among patients without prior exudative AMD, 32 tocilizumab-treated patients (0.1%) developed the condition compared with 136 patients (0.6%) in the control group. Tocilizumab use was associated with a significantly reduced risk of incident exudative AMD (RR 0.234; 95% CI, 0.159–0.344; p < 0.001).
In a sensitivity analysis restricted to patients with at least 3 documented tocilizumab administrations, the inverse association remained significant for both outcomes. Incident non-exudative AMD occurred in 105 of 10,040 patients (1.0%) in the tocilizumab group and 213 of 9,790 matched controls (2.2%) (RR 0.481, 95% CI 0.381–0.606; p < 0.001). Incident exudative AMD occurred in 28 of 10,207 patients (0.3%) and 69 of 10,160 patients (0.7%), respectively (RR 0.404, 95% CI 0.261–0.626; p < 0.001).
In a sensitivity analysis restricted to patients aged 50 years or older, the inverse association also remained significant for both outcomes. Incident non-exudative AMD occurred in 173 of 27,701 patients (0.6%) in the tocilizumab group and 598 of 26,963 matched controls (2.2%) (RR 0.282, 95% CI 0.238–0.333; p < 0.001). Incident exudative AMD occurred in 43 of 28,054 patients (0.2%) and 189 of 27,896 patients (0.7%), respectively (RR 0.226, 95% CI 0.163–0.315; p < 0.001).
In an active-comparator sensitivity analysis using TNF inhibitor users as the comparator cohort, the inverse association remained significant for both outcomes. Incident non-exudative AMD occurred in 125 of 25,393 patients (0.5%) in the tocilizumab group and 255 of 25,419 patients (1.0%) in the TNF inhibitor comparator group (RR 0.491, 95% CI 0.396–0.607; p < 0.001). Incident exudative AMD occurred in 25 of 25,697 patients (0.1%) and 79 of 25,712 patients (0.3%), respectively (RR 0.317, 95% CI 0.202–0.496; p < 0.001).
In an additional sensitivity analysis restricting outcome ascertainment to 1 to 5 years after the index date, the inverse association remained significant for both outcomes. Incident non-exudative AMD occurred in 137 of 31,851 patients (0.4%) in the tocilizumab group and 432 of 31,027 matched controls (1.4%) (RR 0.309, 95% CI 0.255–0.374; p < 0.001). Incident exudative AMD occurred in 31 of 32,211 patients (0.1%) and 140 of 32,034 patients (0.4%), respectively (RR 0.220, 95% CI 0.149–0.325; p < 0.001). Primary and sensitivity analyses for incident non-exudative and exudative AMD are summarized in Table 2.
Primary and sensitivity analyses for incident non-exudative and exudative AMD.
Discussion
In this large, real-world cohort, tocilizumab exposure was associated with a lower incidence of both non-exudative and exudative AMD. These findings are consistent with prior evidence implicating inflammatory pathways, including IL-6 signaling, in AMD pathogenesis, but should be interpreted as associative and hypothesis-generating.
Inflammation is increasingly recognized as a key driver of AMD. Interleukin-6 (IL-6), a pleiotropic cytokine, is elevated both in the aqueous humor and systemically in patients with exudative AMD. In eyes with choroidal neovascularization, higher aqueous IL-6 correlates with VEGF levels and greater central macular thickness, supporting a mechanistic link between IL-6 signaling and neovascular activity. 22 Experimental studies further support IL-6's role in CNV formation. In murine models, IL-6 blockade has been shown to suppress CNV development via downregulation of STAT3 and VEGF signaling pathways and by modulating macrophage polarization in the RPE–choroid complex.20,23
Beyond angiogenesis, IL-6 has also been implicated in promoting oxidative stress and geographic atrophy. Elevated systemic IL-6 levels have been shown to correlate with geographic atrophy progression, and in vitro models demonstrate IL-6-induced oxidative damage to RPE cells and impairment of antioxidant defenses.24,25 These findings support the broader relevance of IL-6 inhibition across both dry and wet forms of AMD.
Clinically, IL-6 receptor blockade has shown benefits in ophthalmic disease outside AMD: tocilizumab improves vision and reduces macular edema in refractory non-infectious uveitis, and has been used in uveitic macular edema that is unresponsive to standard therapy.26,27 Intravitreal IL-6–targeted therapies are also under clinical investigation in other ocular inflammatory conditions.28,29 Recent evidence also highlights tocilizumab's utility in thyroid eye disease; in a randomized clinical trial, tocilizumab significantly improved clinical activity scores in corticosteroid-resistant TED compared with placebo, and a systematic review reinforced its efficacy in reducing inflammation and proptosis.30,31 Given IL-6's established role in promoting angiogenesis, oxidative stress, and retinal degeneration—key processes implicated in AMD pathogenesis—IL-6 signaling remains a biologically plausible pathway of interest in AMD, although our findings do not establish a therapeutic effect in AMD.
Our findings extend the existing literature by demonstrating an inverse association between tocilizumab exposure and incident AMD. In matched cohorts, patients receiving tocilizumab had lower rates of incident non-exudative and exudative AMD than matched controls. Although these associations persisted after propensity score matching, causality cannot be inferred, and residual confounding, including confounding by indication, remains a major consideration. The association also remained significant in an active-comparator sensitivity analysis using TNF inhibitor users, although residual confounding by indication and treatment selection remains possible.
Several limitations should be noted. First, this was a retrospective observational study using electronic health record data and is therefore susceptible to coding errors, outcome misclassification, and surveillance bias. Second, although propensity score matching was performed, substantial residual confounding remains possible, particularly confounding by indication, because patients treated with tocilizumab may differ from controls in inflammatory disease severity, treatment history, concomitant immunosuppressive therapy, underlying treatment indication, and AMD-related factors such as AREDS vitamin use. Third, medication dose, duration, persistence, and adherence were not available, limiting assessment of exposure intensity and temporality. In addition, AMD outcomes were identified using coded diagnoses within the TriNetX platform, without access to imaging confirmation, visual acuity data, or detailed ophthalmic follow-up intensity. Accordingly, outcome misclassification and detection bias remain possible, particularly for non-exudative AMD. Finally, the present analysis relied on risk-based measures of association within a prespecified post-index time window and did not incorporate formal time-to-event modeling. As a result, differences in follow-up duration, censoring, and competing risks such as death were not fully accounted for.
Despite these limitations, to our knowledge, this is the first large-scale study to examine the association between tocilizumab exposure and incident AMD. These findings should be considered hypothesis-generating. Further studies with stronger control of confounding, clearer exposure definitions, and time-to-event modeling are needed to clarify whether the observed association reflects a true relationship between tocilizumab exposure and AMD risk.
Footnotes
Abbreviations/acronyms
Ethical considerations
This study did not require IRB approval because all data were de-identified and HIPAA-compliant.
Consent to participate
This study did not require consent because all data were de-identified and HIPAA-compliant.
Consent for publication
Not Applicable
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Meeting presentation
Podium presentation at The Association for Research in Vision and Ophthalmology (ARVO) 2025, Salt Lake City, Utah