
Abstract
Purpose
To compare the visual and refractive outcomes of breastfeeding versus non-breastfeeding women who underwent photorefractive keratectomy (PRK) surgery.
Methods
In this retrospective study, medical files of women who underwent PRK surgery between January 2013 and December 2023 were reviewed. The patients were divided into two groups: women who reported breastfeeding during their screening examination and women who did not. Pre-, intra-, and post-operative parameters were compared between the groups.
Results
The study included 12,843 eyes from 6,567 women, with 550 eyes from breastfeeding women. Time from screening to surgery was similar between groups (159.5 ± 412.5 vs. 142.8 ± 390.6 days, P = 0.331). Breastfeeding women were older (28.7 ± 4.8 vs. 25.6 ± 6.7 years, P < 0.001), had shorter follow-up (61.0 ± 72.9 vs. 70.6 ± 84.0 days, P = 0.008), higher keratometry (44.78 ± 1.49 vs. 44.55 ± 1.54 D, P < 0.001), worse myopia (SEQ −5.31 ± 2.54 vs. −4.65 ± 2.45 D, P < 0.001), and worse uncorrected visual acuity (UCVA: 1.3 ± 1.1 vs. 1.22 ± 1.05, P = 0.006) and best corrected visual acuity (BCVA: 0.04 ± 1.0 vs. 0.03 ± 1.0, P = 0.02). Postoperative UCVA (0.03 ± 0.85 vs. 0.04 ± 0.8) and BCVA (0.03 ± 0.89 vs. 0.03 ± 0.85) were similar. Breastfeeding was not linked to higher retreatment rates (P = 0.79). Multivariate analysis found no significant differences.
Conclusion
Women who reported breastfeeding on average 5 months prior to surgery achieved visual and refractive outcomes comparable to non-breastfeeding women. PRK appears to deliver satisfactory results within the early postoperative period assessed in this study. Nevertheless, these exploratory findings do not establish long-term refractive stability and should not be interpreted as supporting a change in standard clinical counseling during lactation.
Introduction
Photorefractive keratectomy (PRK) is one of the most performed procedures for the correction of refractive errors. The refractive outcomes of PRK surgery can be influenced by several factors, including the patient's age, baseline refractive error, corneal thickness, and other ocular parameters. One group that has gained interest for potential variability in refractive outcomes is women who are breastfeeding. Hormonal changes during pregnancy and lactation, particularly fluctuations in progesterone, estrogen, and prolactin are assumed to impact corneal parameters such as corneal thickness and curvature, 1 yet this area remains underexplored and debatable.2–4
Refractive instability, especially the occurrence of myopic shifts 5 in lactating patients, remains a subject of ongoing debate, as not all pregnant or lactating women experience noticeable changes in their vision. 6 Additionally, pregnancy reduces tear production, and when coupled with PRK's potential to worsen dry eye symptoms, ensuring sufficient tear quality is essential before contemplating surgery during the post-partum period. 1
Many of the changes observed during pregnancy tend to persist through lactation and may influence visual and refractive outcomes following PRK. For this reason, PRK refractive surgery is typically not recommended for breastfeeding patients. It is generally advised to delay the procedure until lactation has fully ceased and refraction has stabilized to pre-pregnancy levels, ensuring optimal outcomes, and minimizing the risk of complications linked to hormonal fluctuations. However, as most of the current research focuses on the pregnancy phase rather than the post-partum period, particularly during lactation, this remains an area requiring further study.7,8
The aim of this study was to conduct a comprehensive comparison of visual and refractive results by analyzing data from a large-scale database of breastfeeding and non-breastfeeding women who underwent PRK surgery.
Materials and methods
All data for the study were collected and analyzed in accordance with the policies and procedures of the Institutional Review Board of the Barzilai Medical Center (Ashkelon, Israel) and the tenets of the Declaration of Helsinki (Ethics committee approval number: 0154–20-BRZ, originally received on 14.09.2021, and renewed on 01.01.2024).
Study participants
This retrospective study included patients who underwent their first PRK surgery between January 2013 and December 2023 at Care-Vision Laser Centers, Tel-Aviv, Israel. Inclusion criteria were females aged 18 to 50, a stable refraction (≤0.50 D change in spherical equivalent) for at least 12 months, as determined by patient interview regarding changes in spectacle prescription and, when available, review of prior refraction records, intraocular pressure lower than 21 mmHg, and a contact lenses-free period of more than two weeks for rigid lenses and over three days for soft lenses.
The exclusion criteria included patients whose worst-seeing eye had a best-corrected visual acuity (BCVA) of worse than (i.e., greater than) 0.4 logMAR, patients not targeted for emmetropia, eyes treated for monovision, and patients without postoperative data within a one-year range. For analysis purposes, patients were divided into two groups based on their responses to the medical questionnaire, which was part of the screening process for refractive surgery. The groups were categorized based on their self-reported breastfeeding status at the time of the preoperative screening. The screening questionnaire did not distinguish between exclusive and partial breastfeeding; patients were classified as either actively breastfeeding or not. It is acknowledged that due to the time interval between screening and surgery, the lactation status at the exact moment of surgery could not be definitively confirmed for every patient.
Data collection
The medical files of all eligible patients were reviewed, and the following demographic and preoperative information was extracted: age, operated eye, pachymetry, mean, minimal, and maximal keratometry power (based on keratometry [K] of the Sirius [Scheimpflug tomographer; CSO, Firenze, Italy]), decimal uncorrected visual acuity (UCVA), decimal best corrected visual acuity (BCVA), spherical equivalent (SEQ), sphere, cylinder power and axis. The following intraoperative data were extracted: treatment parameters - sphere and cylinder, optical zone diameter, and maximum ablation depth. Decimal scores were converted to logMAR using the formula logMAR = -log(decimal acuity).
Main outcome measures
The main outcome measures were recorded at the last available follow-up visit. While the protocol encouraged long-term follow-up, the analyzed data reflects the last actual visit, which ranged from 1 month to 1 year post-operatively. These measures included UCVA, BCVA, subjective SEQ, subjective sphere, subjective cylinder, mean, minimal, and maximal keratometry power, safety index (postoperative BCVA/preoperative BCVA), and efficacy index (postoperative UCVA/preoperative BCVA). If post-operative data on subjective refraction was available, we used that. In cases where subjective refraction was not available, we used autorefraction.
Surgical technique
During surgery one drop of a topical anesthetic (benoxinate hydrochloride 0.4%) was instilled in the conjunctival fornix, after which a lid speculum was inserted. Epithelial removal was performed via alcohol assisted PRK (20% ethyl alcohol placed on the cornea for 15 s). Following epithelial removal, the WaveLight Allegretto 200 Hz excimer laser (Alcon Laboratories, Fort Worth, Texas, USA) was used for wave front optimized stromal ablation under constant eye tracking. The ablation zone was composed of an optic zone of 6.0–7.0 mm and a transition zone of 2.0–3.0 mm. Following excimer ablation, all PRK cases were treated with a 0.02% mitomycin C-soaked sponge placed on the stroma for 30–40, 50–60 or 60–70 s (<6, 6–8, or >8 D of SEQ, respectively). After rinsing the mitomycin a contact lens was placed. Following surgery, patients were prescribed moxifloxacin 0.5% (4 times a day), dexamethasone 0.1% (4 times a day) and artificial tears without preservatives (4 times a day). Surgery was performed by multiple surgeons using a standard protocol at one surgical center. Patients were routinely examined on 1 day; 1 week; and 1, 3 months postoperatively and later if necessary. Patients were encouraged to return for examination if vision deteriorated at any time after surgery, and laser enhancement procedures were offered free of charge after surgery whenever needed and after a 6-month period of stable refraction.
Statistical analysis
The data were analyzed using IBM® SPSS® Statistics software (version 27). An independent samples t-test was used to compare the means of the variables. To compare the outcomes between the groups while controlling for potential confounders, a multivariate regression analysis was conducted. The model was adjusted for any preoperative and intraoperative factors that showed statistically significant differences between the parameters. Accordingly, adjustment accounted for differences in baseline (follow-up time, age, pachymetry, average, minimal, and maximal keratometry, UCVA, subjective SEQ, sphere, and cylinder, and BCVA) and intraoperative parameters (treated sphere and maximum ablation depth) (P < 0.05 for all). We investigated the association between breastfeeding status and the number of retreatments using a Chi-square test for independence. Standardized graphs illustrating the refractive outcomes were generated using the mEYEstro Software (version 2.4). 9 In all analyses, a two-sided P-value of less than 0.05 was considered statistically significant. All means were reported with their corresponding standard deviations (SDs).
Results
Overall, 12,843 eyes of 6,567 women were included. The mean age was 25.7 ± 6.7 years, and 550 eyes (4.2%) were in the breastfeeding group.
Preoperative comparison of breastfeeding and non-breastfeeding groups
Table 1 compares preoperative baseline variables between the breastfeeding and non-breastfeeding groups. In summary, the breastfeeding group was notably older, averaging 28.7 ± 4.8 years versus 25.6 ± 6.7 years in the non-breastfeeding group (P < 0.001). Corneal pachymetry measurements were thinner in the breastfeeding group (521.68 ± 32.57 μm) compared to the non-breastfeeding group (526.72 ± 33.31 μm), a difference that was statistically significant (P < 0.001). Keratometry readings revealed higher values in the breastfeeding group: average keratometry was 44.78 ± 1.49 D versus 44.55 ± 1.54 D (P < 0.001), minimal keratometry was 44.21 ± 1.50 D compared to 44.01 ± 1.55 D (P = 0.003), and maximal keratometry was 45.35 ± 1.59 D against 45.09 ± 1.60 D (P < 0.001). Visual acuity assessments showed that the breastfeeding group had slightly worse UCVA at LogMAR 1.3 ± 1.1 compared to 1.22 ± 1.05 in the non-breastfeeding group (P = 0.006), and a worse BCVA of LogMAR 0.04 ± 1.0 versus 0.03 ± 1.0 (P = 0.020). Refractive measurements indicated greater myopia in the breastfeeding group, with a subjective SEQ of −5.31 ± 2.54 D compared to −4.65 ± 2.45 D (P < 0.001), and a more myopic sphere of −4.82 ± 2.57 D versus −4.20 ± 2.44 D (P < 0.001). Astigmatism was also worse at −0.99 ± 0.90 D compared to −0.89 ± 0.85 D in the breastfeeding group (P = 0.008). No significant differences were observed in the side of the eye operated (%right eyes, P = 0.643) or in the subjective axis (P = 0.199) between the two groups.
Comparison of preoperative parameters.
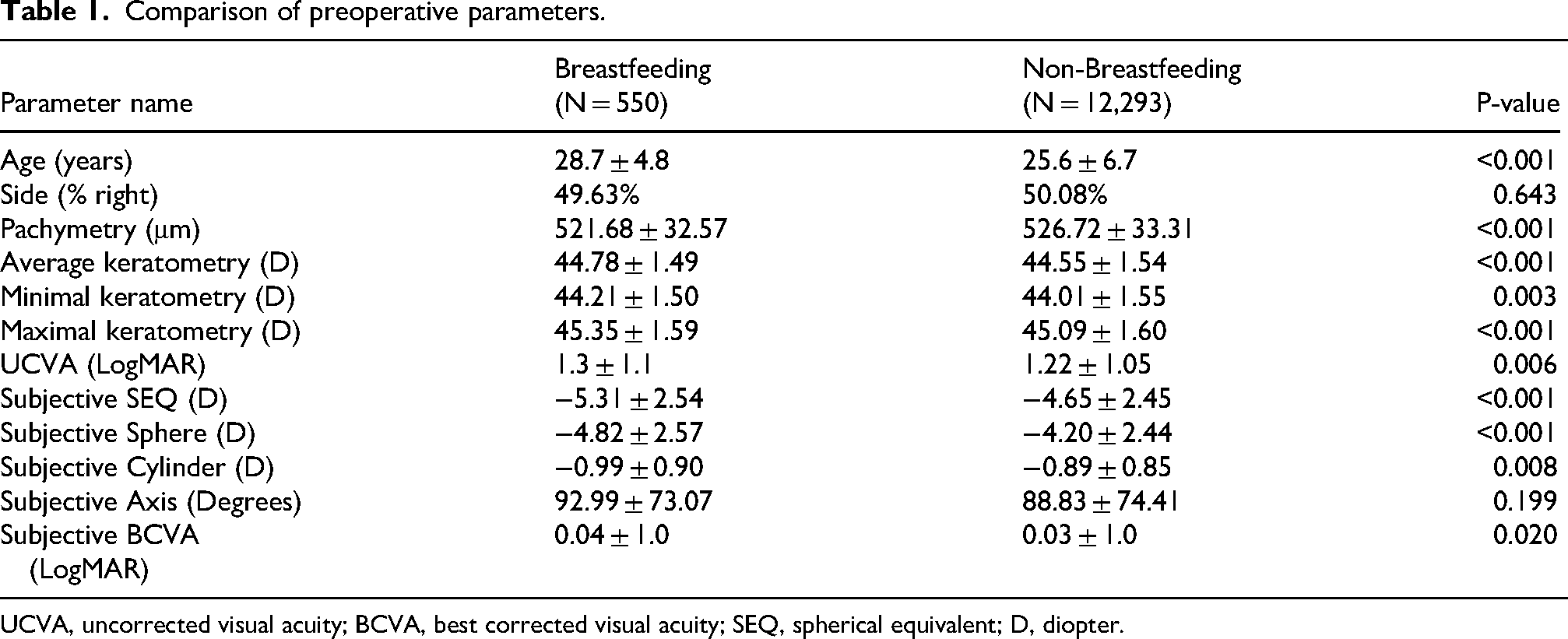
UCVA, uncorrected visual acuity; BCVA, best corrected visual acuity; SEQ, spherical equivalent; D, diopter.
Intraoperative parameters of breastfeeding and non-breastfeeding groups
As seen in Table 2, the treated sphere value was significantly higher in the breastfeeding group than in the non-breastfeeding group (−5.03 ± 2.21 D vs. −4.57 ± 2.13 D, P < 0.001). Additionally, the maximal ablation depth was greater in the breastfeeding group (87.46 ± 37.18 µm) compared to the non-breastfeeding group (79.70 ± 32.62 µm), also showing statistical significance (P < 0.001). Although marginal, there were no significant differences in the treated cylinder (−1.24 ± 0.81 vs. −1.17 ± 0.80 D; P = 0.063), and optical zone size (6.56 ± 0.26 mm vs. 6.57 ± 0.27 mm; P = 0.293) between the two groups.
Comparison of intraoperative parameters.

D, diopter.
Postoperative visual and refractive results of the breastfeeding and non-breastfeeding groups
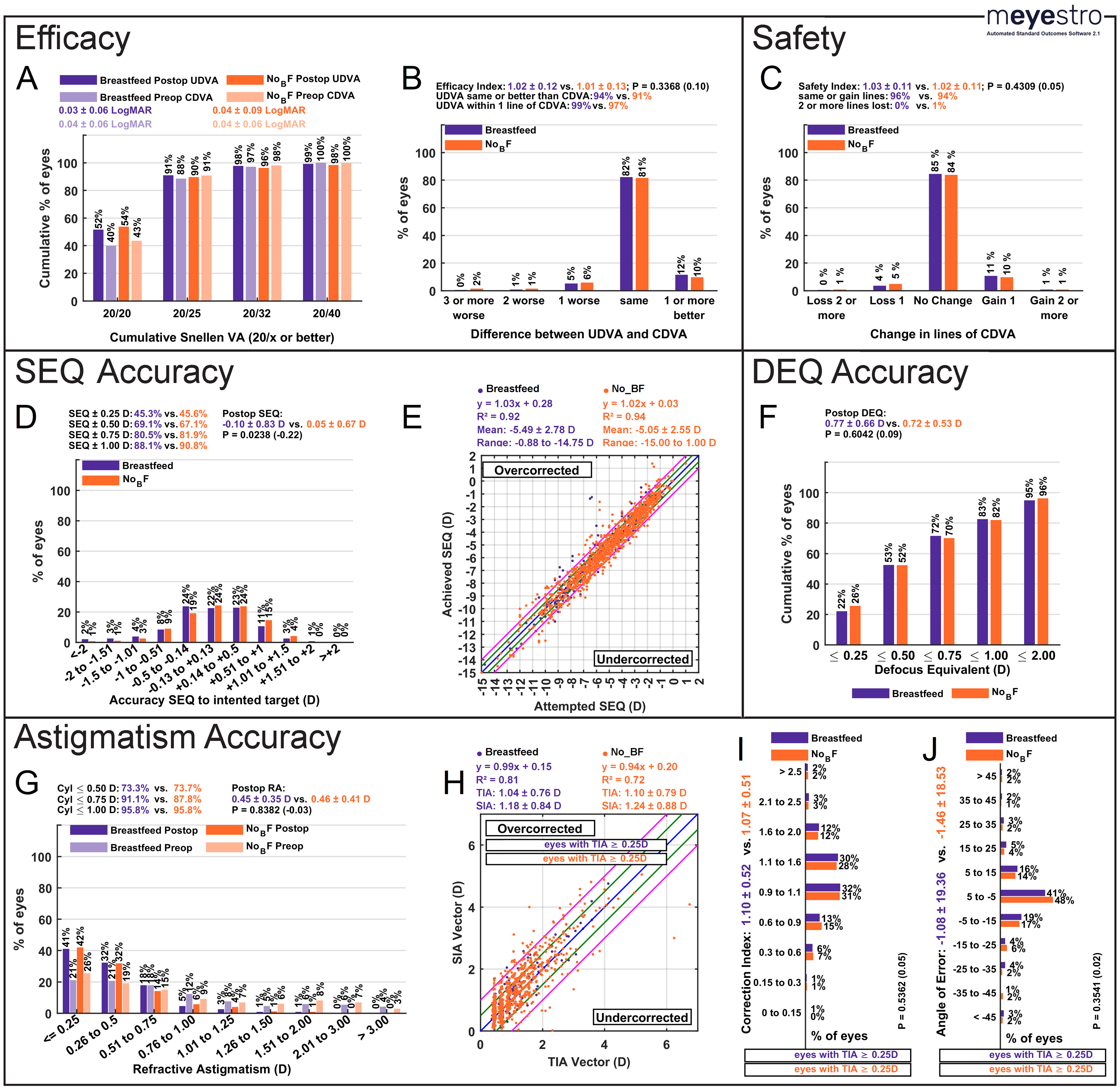
Table 3 presents a comparison of visual and refractive outcomes between breastfeeding and non-breastfeeding women. The time elapsed between completing the screening questionnaire and undergoing the surgery was not significantly different between the breastfeeding and the non-breastfeeding groups (159.5 ± 412.5 vs. 142.8 ± 390.6 days, P = 0.331). The follow-up time was significantly shorter for the breastfeeding group (61.0 ± 72.9 days) compared to the non-breastfeeding group (70.6 ± 84.0 days), with a P-value of 0.008. UCVA was similar between the groups, with the breastfeeding group having a mean UCVA of LogMAR 0.03 ± 0.85 and the non-breastfeeding group 0.04 ± 0.85 (P = 0.597). Subjective SEQ and sphere showed marginally non-significant differences. The breastfeeding group had a mean SEQ of −0.09 ± 0.82 D and a subjective sphere of 0.12 ± 0.83 D, while the non-breastfeeding group had a mean SEQ of −0.008 ± 0.68 D and a subjective sphere of 0.21 ± 0.70 D, with P-values of 0.051 and 0.065, respectively. Subjective cylinder values were nearly identical between the groups, with the breastfeeding group at −0.45 ± 0.35 D and the non-breastfeeding group at −0.44 ± 0.40 D (P = 0.825). BCVA was the same for both groups, each with a mean of 0.03 ± 0.9 for the breastfeeding group and 0.03 ± 0.85 for the non-breastfeeding group (P = 0.902). Safety and efficacy indices were also comparable. The safety index was 1.02 ± 0.14 for the breastfeeding group and 1.02 ± 0.15 for the non-breastfeeding group (P = 0.711). The efficacy index was 1.01 ± 0.15 for the breastfeeding group and 1.00 ± 0.17 for the non-breastfeeding group (P = 0.297). Standardized graphs comparing breastfeeding and non-breastfeeding are provided in Figure 1.
Outcome comparison of breastfeeding and non-breastfeeding patients.
Comparison of visual and refractive outcomes.
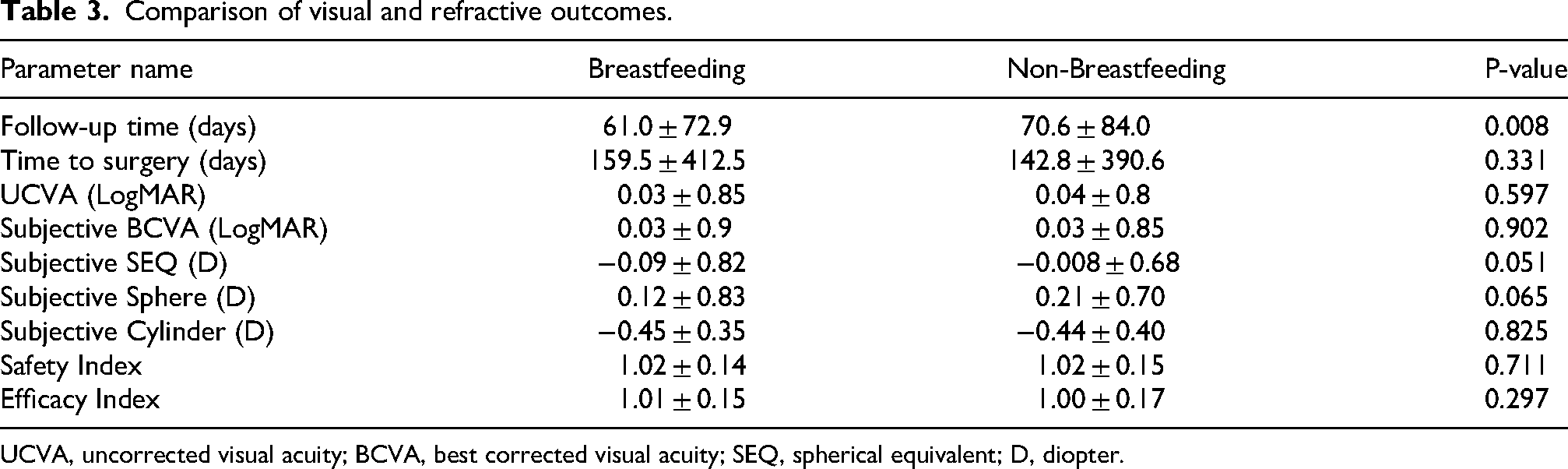
UCVA, uncorrected visual acuity; BCVA, best corrected visual acuity; SEQ, spherical equivalent; D, diopter.
Comparison of breastfeeding and non-breastfeeding groups after adjustment for potential confounders
As can be seen in Table 4, after adjusting for differences in baseline (follow-up time, age, pachymetry, average, minimal, and maximal keratometry, UCVA, subjective SEQ, sphere, and cylinder, and BCVA) and intraoperative parameters (treated sphere and maximum ablation depth) (P < 0.05 for all), no statistically significant differences across all parameters were observed. UCVA averaged LogMAR 0.05 ± 0.85 in the breastfeeding group and 0.06 ± 0.74 in the non-breastfeeding group (P = 0.364). Subjective SEQ measurements were 0.13 ± 0.50 D for breastfeeding women versus 0.003 ± 0.62 D for non-breastfeeding women (P = 0.104). Subjective sphere values were 0.31 ± 0.54 D and 0.22 ± 0.67 D (P = 0.319), while subjective cylinder measurements were −0.35 ± 0.34 D and −0.44 ± 0.48 D (P = 0.149) for the breastfeeding and non-breastfeeding groups, respectively. Both groups shared a similar BCVA of 0.04 ± 0.95 and 0.04 ± 0.92 (P = 0.941). The safety index was 0.99 ± 0.08 for breastfeeding women compared to 1.02 ± 0.13 for non-breastfeeding women (P = 0.086), and the efficacy index was 0.96 ± 0.12 versus 0.97 ± 0.19 (P = 0.879), respectively.
Comparison of visual and refractive outcomes after adjustment of pre- and intra-operative variables.
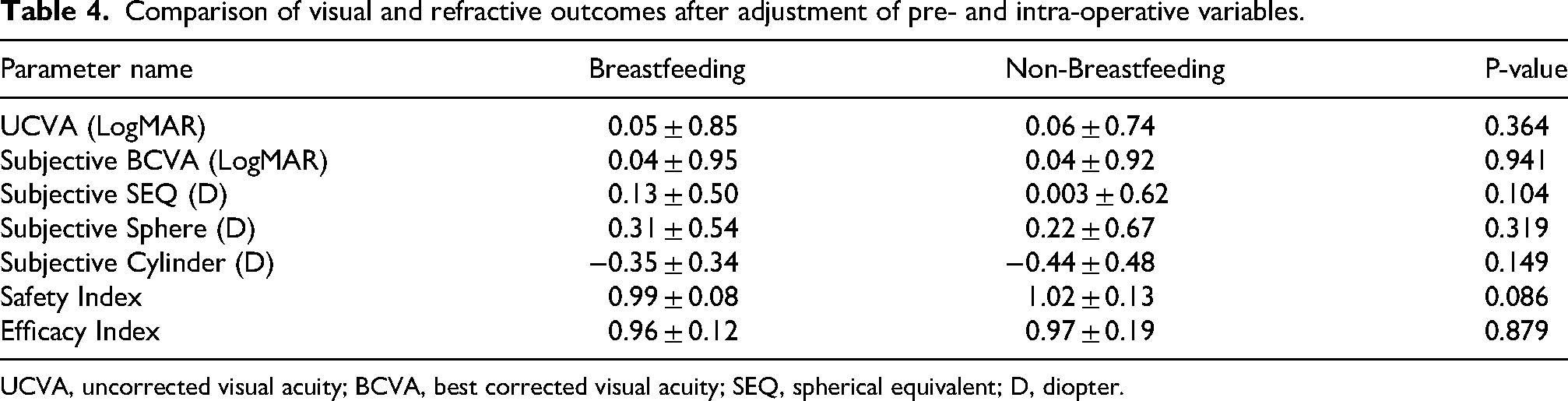
UCVA, uncorrected visual acuity; BCVA, best corrected visual acuity; SEQ, spherical equivalent; D, diopter.
Retreatment rates
The analysis revealed that there was no significant association between breastfeeding and undergoing retreatment (χ2 (2, N = 12,741) = 0.45, P = 0.796).
Discussion
This study aimed to evaluate the visual and refractive outcomes of PRK surgery in breastfeeding versus non-breastfeeding women. Our study found that both groups achieved satisfactory results and there were no statistically significant differences between the groups in post-operative findings. The results demonstrated that, over an average follow-up period of approximately two months, ranging up to one-year, breastfeeding status was not associated with a statistically significant reduction in the short-term safety or effectiveness of myopic PRK surgery when performed, on average, about five months after reporting active breastfeeding. This finding offers preliminary observational data for breastfeeding patients who are considering the procedure in that time frame, although these results should not be interpreted as evidence supporting a change in current clinical recommendations. Our findings highlight significant preoperative differences between these two groups, particularly in terms of preoperative myopia severity, keratometry, visual acuity, and related intraoperative parameters. Our data demonstrate that breastfeeding women were, on average, older and exhibited significantly worse preoperative UCVA and BCVA compared to non-breastfeeding women. Furthermore, breastfeeding women had slightly steeper corneas, and higher degree of preoperative myopia and astigmatism, as evidenced by their worse SEQ, sphere, and cylinder values. These findings suggest that breastfeeding women may present for refractive surgery at a later age and with higher levels of myopia, potentially due to older age and perhaps due to hormonal changes associated with pregnancy and lactation, which have been shown to impact ocular physiology. Previous studies have suggested that the hormonal fluctuations during in pregnancy and postpartum can cause temporary changes in corneal curvature, hydration, and refractive error, which may explain the worse SEQ, sphere, and cylinder values observed in this group.1,10 As a reflection of that, the maximum ablation depth was greater in the breastfeeding group, likely corresponding to the higher myopic correction required. The greater ablation depth in breastfeeding women may present potential additional risks, such as increased corneal thinning or ectasia after laser-assisted in situ keratomileusis (LASIK) surgery, particularly if corneal biomechanical properties are temporarily altered during lactation.11–14 Future studies are warranted to investigate the long-term effects of such changes on corneal stability in breastfeeding women following PRK. We found that breastfeeding women underwent surgery an average of 159 days after reporting active breastfeeding in the preoperative screening questionnaire. The exact timing of childbirth and the duration of breastfeeding were not recorded, but it is well known that hormonal changes during lactation can vary widely among individuals. Achieving full hormonal balance may take several months after breastfeeding ends. Lactation causes significant long-term hormonal changes, including reduced estrogen levels and increased prolactin production, which can influence the body's physiology long after breastfeeding ceases. For example, some studies indicate that it may take six months or more for certain hormone levels to fully stabilize after extended periods of breastfeeding. 15
Postoperatively, average follow-up time was shorter in the breastfeeding group. Nevertheless, breastfeeding women showed no statistically significant differences in refractive or visual outcomes, including safety and efficacy indices, suggesting that the surgical correction was effective in both groups, despite the unfavorable starting conditions in the breastfeeding group. However, SEQ values were slightly worse in the breastfeeding group, though this difference was only marginally insignificant. Importantly, these borderline differences are of negligible clinical significance, as the absolute magnitude of the observed differences in SEQ and sphere between groups was minimal and well within the accepted clinical threshold of ±0.50 D. After adjusting for pre- and intra-operative parameters, all parameters remained without any significant differences. These outcomes may be since both groups were of a similar age, as better visual and refractive results are often associated with younger patients, and younger age typically correlates with faster healing and improved visual recovery following refractive surgery.16,17
Since the average follow-up period for both groups was around two months, with a standard deviation of an additional two and half months, it is unlikely that the women stopped breastfeeding during this time. Therefore, in the short term, postoperative outcomes appear to be similar between breastfeeding and non-breastfeeding women, despite the hormonal changes that can affect corneal morphology and function during breastfeeding. It seems that, despite these changes, breastfeeding women are able to achieve good and satisfactory results. This area warrants further investigation into future studies. With an average follow-up period of approximately two months and a standard deviation of an additional two months, our conclusions are limited to this time frame. In that short term, postoperative outcomes appear to be similar for both breastfeeding and non-breastfeeding women, despite the potential hormonal changes during breastfeeding that can affect corneal morphology and function. Notably, breastfeeding women still achieve good and satisfactory results, indicating that these hormonal changes do not negatively impact the effectiveness of the procedure within this period. This topic warrants further investigation through future long-term studies. It is important to emphasize that our study evaluates early postoperative outcomes and does not establish long-term refractive stability; hormonal effects may continue to fluctuate during lactation and after cessation, and refractive parameters may stabilize only after complete normalization of hormonal status. A similar, smaller-scale study by Zarei-Ghanavati et al. did not indicate any adverse effects of breastfeeding on the results of PRK surgery. 18 Similarly, in their study, Alonso-Santander et al. reported results comparable to ours, showing no significant differences between breastfeeding women and those who had stopped breastfeeding at least 3 months before undergoing LASIK or PRK. This finding applied to postoperative SEQ, efficacy index, visual acuity, predictability, and safety index. 19
Several limitations should be considered when interpreting the results of our study. First, the retrospective nature of this study made it impossible to assess the cohort for additional factors affecting postoperative visual outcomes, mainly pre-existing ocular surface conditions. Second, although ranging up to a year, the relatively short mean follow-up period may not capture long-term visual and refractive outcomes, particularly in breastfeeding women whose hormonal levels and corneal properties may continue to fluctuate during lactation and after breastfeeding ends. In addition, as mentioned above, the average time among breastfeeding women between completing the preoperative suitability questionnaire and undergoing the surgery itself was approximately five months in the breastfeeding groups. We did not have information about the exact date of childbirth or the duration of breastfeeding prior to completing the questionnaire. Instead, we only know whether the patient reported actively breastfeeding at the time of filling out the questionnaire. Furthermore, we lack information on whether the patient was still breastfeeding at the time of the surgery or had recently stopped. This creates a potential overlap: women in the non-breastfeeding group may have become pregnant or initiated breastfeeding, while women in the breastfeeding group may have ceased lactation. However, given the established physiology that hormonal normalization can take 6 months or more post-weaning14,20,21 the ‘breastfeeding group’ represents a cohort with recent or active significant hormonal fluctuations distinct from the general population. Even if lactation had ceased shortly before surgery, the corneal biomechanics may still be under hormonal influence. Additionally, the relatively small number of breastfeeding women compared to non-breastfeeding women (4.2% of the cohort) may limit the generalizability of our findings. This proportion may also reflect selection bias, as breastfeeding women who sought refractive surgery despite conventional recommendations to defer may represent a self-selected subgroup, potentially differing from the broader population of lactating women in motivation, symptom burden, or clinical profile. Accordingly, these results should be regarded as exploratory observational data rather than as evidence supporting a change in current clinical recommendations. Larger prospective studies are needed to confirm these results and explore the long-term impact of breastfeeding on refractive surgery outcomes, particularly as hormonal levels return to baseline postpartum over time. Moreover, tear film parameters, tear dysfunction metrics, and formal dry eye assessments were not routinely performed as part of the preoperative screening protocol at our center; however, patients with clinically suspected preoperative dry eye were excluded from surgery. The absence of standardized tear film evaluation represents a limitation, particularly given that dry eye may fluctuate during the postpartum period. Additionally, our screening questionnaire did not distinguish between exclusive and partial breastfeeding, and therefore the degree of lactational hormonal exposure may have varied among participants in the breastfeeding group. Furthermore, postoperative refractive data were based on subjective refraction when available, and autorefraction when subjective refraction was unavailable; this methodological heterogeneity may have introduced some variability in refractive outcome assessment. Finally, preoperative refractive stability was assessed primarily through patient interview regarding changes in spectacle prescription rather than through serial refraction measurements, which represents a less rigorous verification method compared to longitudinal objective documentation.
Conclusion
In conclusion, our retrospective, exploratory study found that short-term visual and refractive outcomes were comparable between women who reported breastfeeding during preoperative screening and non-breastfeeding women following PRK surgery. Importantly, these findings represent early postoperative observations and do not establish long-term refractive stability. Given the retrospective design, the absence of longitudinal preoperative refraction data, and the inability to confirm lactation status at the exact time of surgery, these results should be interpreted with appropriate caution. This study does not provide sufficient evidence to recommend a change in current clinical practice. The traditional recommendation to defer refractive surgery until hormonal stability has been achieved and refraction has returned to pre-pregnancy levels remains valid and clinically prudent. Standard preoperative counseling regarding the potential risks of surgery during or shortly after lactation should continue to be offered. Nevertheless, these exploratory data may offer preliminary reassurance when counseling breastfeeding patients who are unable or unwilling to delay surgery, provided that refractive stability has been verified. Prospective, long-term studies with confirmed breastfeeding status at the time of surgery and serial refractive assessments are warranted to further clarify the safety and stability of PRK outcomes in this population.
Footnotes
ORCID iDs
Ethical considerations
All data for the study were collected and analyzed in accordance with the policies and procedures of the Institutional Review Board of the Barzilai Medical Center (Ashkelon, Israel) and the tenets of the Declaration of Helsinki (Ethics committee approval number: 0154–20-BRZ, originally received on 14.09.2021, and renewed on 01.01.2024).
Consent to participate
Not applicable
Consent for publication
Not applicable
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
Due to commercial retrictions, supporting data is not available.