
Abstract
Purpose
To analyze the amplitude of accommodation and its changes at a 6-month follow-up in healthy subjects implanted with an anterior chamber pIOL, assessing whether accommodative function is affected. Additionally, changes in visual performance and other ocular parameters were evaluated.
Methods
Prospective study including 57 subjects (age range, 18–45 years) implanted with the Artiflex pIOL (Ophtec) were evaluated at one week and six months postoperatively. Changes in manifest refraction, uncorrected distance visual acuity (UDVA), corrected distance visual acuity (CDVA), and other clinical variables were analyzed. Amplitude of accommodation (AA) was measured under photopic conditions using the Sheard method. One randomly selected eye per subject was included for analysis.
Results
Statistically significant reduction in refraction was observed (p < 0.001), remaining stable throughout follow-up visits. Accordingly, both the 1-week and 6-month visits demonstrated significant improvements in UDVA compared to baseline (p < 0.001). CDVA also improved significantly following IOL implantation (p < 0.001). Longitudinal analysis revealed no clinically or statistically significant changes in AA from baseline to 1-week (p = 0.096) or 6-month postoperative visits (p = 0.317) ( Table 2). Mean change in AA in the whole sample was close to 0.10 ± 0.86 D. No significant differences were found in the accommodative changes found with spherical and toric models (p ≥ 0.092). Changes in AA at 1-week (ρ=0.378, p = 0.004) and 6 months (ρ=0.336, p = 0.011) were significantly correlated with age.
Conclusions
The implantation of Artiflex anterior chamber pIOL did not significantly affect the amplitude of accommodation in healthy subjects during the six-month follow-up period. Future comparative studies with posterior chamber pIOLs are needed.
Introduction
Myopia has become one of the most prevalent refractive errors worldwide, with its prevalence increasing dramatically in recent decades—ranging from 5% to 70%, depending on the country. 1 This rise is largely attributed to factors such as prolonged near work, limited time spent outdoors, and genetic predisposition. 2 As myopia progresses, it can cause significant visual impairment and is associated with an increased risk of ocular conditions such as glaucoma and retinal detachment, among others. 3
Over the years, various refractive surgical techniques have been developed to correct myopia and reduce dependence on glasses or contact lenses. While these techniques have proven effective and safe, they are not without complications. 4 Corneal refractive surgeries, such as LASIK and PRK, offer advantages like rapid recovery, minimal discomfort, and high success rates for mild to moderate myopia. However, they may not be suitable for individuals with thin corneas or severe myopia, 5 and they carry risks such as dry eye, undercorrection, or overcorrection, among others. 6 Alternatively, implantable phakic intraocular lenses (pIOLs) provide a permanent (but reversible) solution for patients with high myopia or thin corneas. 7 This procedure is more invasive, and poses different risks depending on the pIOL type. 8
These pIOLs can be implanted in either the anterior or posterior chamber, depending on the patient's ocular anatomy. Posterior chamber pIOLs, positioned behind the iris and in front of the natural lens, are the most widely used, with extensive studies supporting their safety and visual outcomes. 9 However, they are not without risks, including crystalline lens opacity, or elevated intraocular pressure, among others. 10 In recent years, research has also focused on their impact on accommodative function. 11 Studies indicate that improper sulcus placement can alter ciliary muscle dynamics, leading to postoperative accommodative dysfunction.12–17 In contrast, anterior chamber pIOLs are positioned entirely anterior to the iris, eliminating any interaction with the ciliary sulcus. This anatomical distinction suggests they should have minimal to no impact on accommodative function. However, these lenses remain associated with other potential complications.4,8
One of the most commonly used anterior chamber pIOLs is the Artiflex lens (Ophtec B.V., Groningen, The Netherlands). Its safety and efficacy have been extensively evaluated in long-term follow-up studies,18–20 and its visual performance has been well-documented, 21 including comparative studies with other pIOLs showing similar outcomes.22–27 However, unlike posterior chamber pIOLs, its potential impact on accommodative function remains unexplored. The present study aimed to analyze changes in accommodative amplitude at 6 months post-implantation in healthy subjects receiving the Artiflex pIOL, assessing whether accommodation is affected. Additionally, an evaluation of changes in visual performance and other ocular parameters was also performed.
Methods
Subjects
This prospective study was conducted at the Madrid Ophthalmological Institute (Madrid, Spain) in accordance with the Declaration of Helsinki. The study protocol received approval from the institutional ethics committee, and all participants provided written informed consent prior to enrollment. Patients aged >18 years who underwent phakic Artiflex IOL implantation were included. Eligible subjects had central anterior chamber depth (ACD) ≥ 2.7 mm (from endothelium to anterior crystalline lens surface), endothelial cell density (ECD) ≥ 2200 cells/mm2, stable refraction (>1 year), and mesopic pupil diameter ≤6.0 mm. Exclusion criteria included active ocular or systemic disease contraindicating surgery, prior ocular surgery, aniridia/iris atrophy, pregnancy or diabetes, and intraocular pressure >21 mmHg.
Artiflex pIOL
The Artiflex lens is an iris-fixated anterior chamber phakic intraocular lens (pIOL) indicated for the correction of high myopia and astigmatism. The lens features an optical zone composed of polysiloxane (8.50 mm diameter; refractive index 1.43). Two models were implanted: Artiflex 401 for spherical corrections (−2.00 to −14.50 D in 0.50 D increments) and Artiflex Toric for astigmatic corrections (models 4A0 and 4C0). The power of this pIOL is available in spherical values from −1.00 to −13.50 D (0.50 D steps) and in cylinder values from −1.00 to −5.00 D (0.50 D steps).
Surgical protocol
All surgical procedures were performed by the same experienced surgeon (MR) using either peribulbar or retrobulbar anesthesia, selected according to the surgeon's clinical judgment. Prior to surgery, all patients received miosis-inducing drops to achieve optimal pupil constriction. The surgical technique began with creation of a 3.2-mm clear corneal incision at the superior (12 o'clock) position. Two additional paracentesis incisions were then made at the 10 and 2 o'clock positions to facilitate instrument access. Following anterior chamber inflation with viscoelastic material, the Artiflex pIOL was carefully introduced through the main incision. Under direct visualization, the lens was precisely positioned and securely fixated to the mid-peripheral iris using its specially designed haptic claws. A peripheral iridotomy was subsequently performed to prevent pupillary block and ensure normal aqueous humor dynamics. Finally, the viscoelastic material was thoroughly irrigated and aspirated, with the anterior chamber stabilized using balanced saline solution.
Clinical protocol
A comprehensive preoperative assessment included detailed anamnesis, manifest and cycloplegic refraction, along with measurement of uncorrected (UDVA) and corrected (CDVA) distance visual acuity. All subjects underwent complete ocular examination including slit-lamp biomicroscopy, corneal topography (Pentacam, Oculus Optikgeräte GmbH), optical biometry (IOL-Master, Carl Zeiss Meditec AG), endothelial cell count (EM-3000, Tomey), Goldmann applanation tonometry, and dilated fundus examination. Postoperative follow-up visits adhered to standard medical protocols, with study-specific variables analyzed at three key timepoints: preoperative baseline, 1-week postoperative, and 6-month postoperative. At each study visit, changes in refractive status (manifest refraction), visual acuity parameters (UDVA, CDVA), corneal metrics (mean keratometry [Km], central corneal thickness [CCT]), anterior segment dimensions (ACD, from endothelium to anterior crystalline lens surface, white-to-white distance [WTW]) and IOP were evaluated. Amplitude of accommodation (AA) was quantified using the Sheard method under photopic conditions. Measurements were obtained by presenting a near optotype at 40 cm and incrementally adding minus lenses until first sustained blur was reported. To maintain consistency, all accommodation measurements were performed on the same randomly selected eye for each subject throughout the study period. For statistical purposes, the accommodative change was evaluated as the change in the AA between two consecutive visits.
Statistical analysis
All analyses were performed using SPSS Statistics version 19.0 (IBM Corp., Chicago, IL). After assessing data distribution through normality tests, non-parametric methods for hypothesis testing were employed. The Friedman test served as our primary analysis to evaluate differences across the three study timepoints (preoperative, 1-week postoperative, and 6-month postoperative). For significant Friedman test results (p < 0.05), post hoc pairwise comparisons were conducted using the Wilcoxon signed-rank test with Bonferroni correction (α = 0.0167 for three comparisons). Relationships between baseline clinical parameters and accommodation changes were examined using Spearman's rank correlation coefficient. Throughout all analyses, a two-tailed p-value <0.05 indicated statistical significance.
Results
The study cohort comprised 57 patients (30 women, 52.6%; 27 men, 47.4%) with a mean age of 28.4 years (SD ±6.3, range 18–45 years). The sample included 31 right eyes (54.4%) and 26 left eyes (45.6%), reflecting a balanced distribution between eyes. Patients presented with characteristic biometric parameters of high myopia, including an average axial length of 26.61 mm (SD ±1.74, range 22.15–31.82 mm). Anterior segment measurements revealed a mean white-to-white distance of 12.31 mm (SD ±0.40) and central corneal thickness of 542.14 μm (SD ±37.45). Endothelial cell density averaged 2828 cells/mm2 (SD ±222), with all values remaining above the safety threshold for surgery. Surgeons implanted spherical Artiflex IOLs in 39 eyes (68.4%) and toric models in 18 eyes (31.6%). The lenses addressed a wide refractive range, with spherical corrections averaging −8.37 D (SD ±3.08, up to −14.50 D) and cylindrical corrections averaging −0.68 D (SD ±1.15) in toric cases.
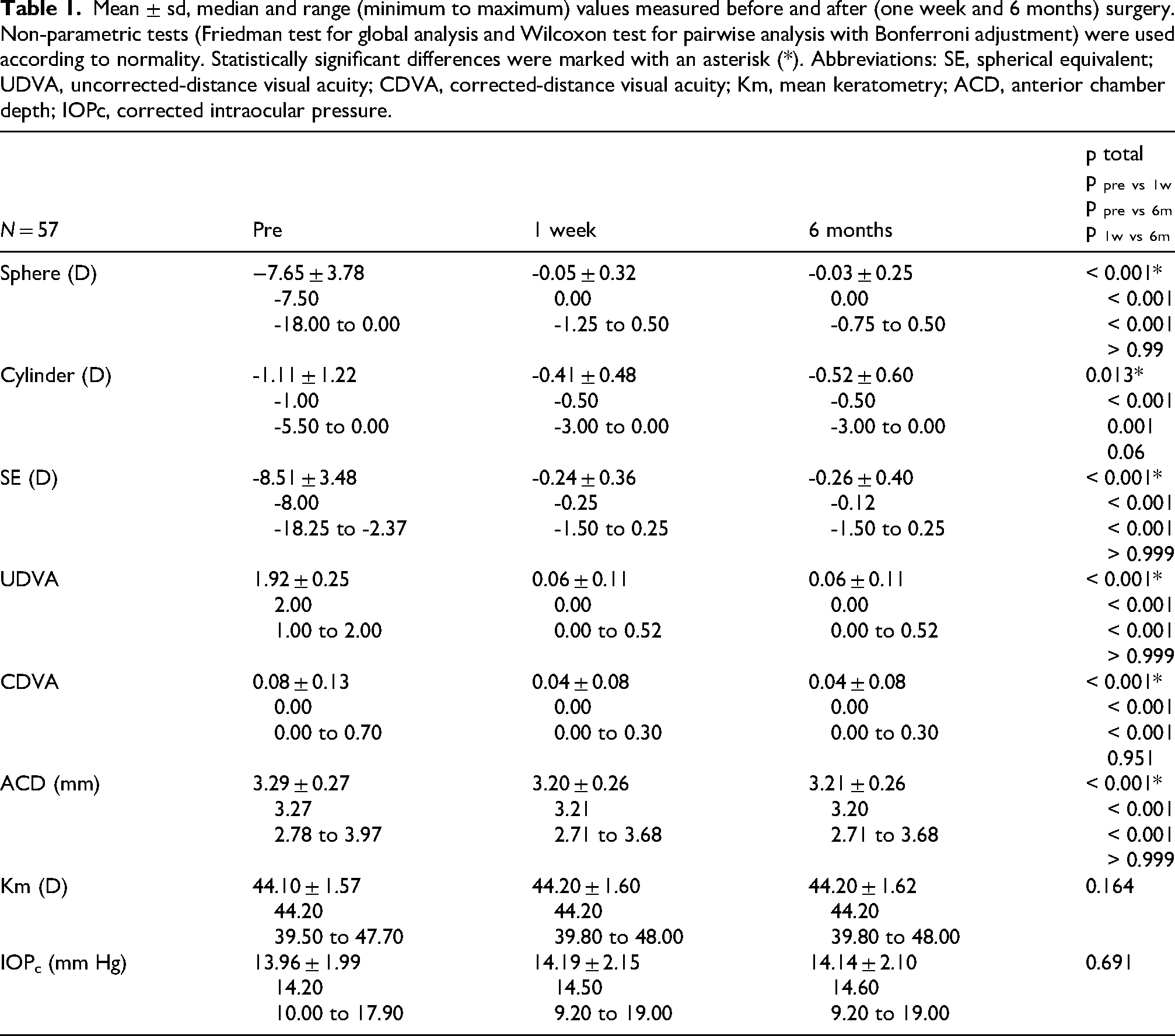
All baseline characteristics and their changes across the study timepoints (preoperative, 1-week postoperative, and 6-month postoperative) are comprehensively detailed in Table 1. As shown, there was a significant reduction of the refractive error combined with a significant improvement in both UDVA and CDVA (p < 0.001). This change was observed at the first postoperative period and maintained throughout the rest of the follow-up (p ≥ 0.06). A small but statistically significant reduction of ACD (p < 0.001) was found when comparing baseline with 1-week or baseline with 6 months visit. No significant changes were observed in IOP during the postoperative follow-up (p = 0.691).
Mean ± sd, median and range (minimum to maximum) values measured before and after (one week and 6 months) surgery. Non-parametric tests (Friedman test for global analysis and Wilcoxon test for pairwise analysis with Bonferroni adjustment) were used according to normality. Statistically significant differences were marked with an asterisk (*). Abbreviations: SE, spherical equivalent; UDVA, uncorrected-distance visual acuity; CDVA, corrected-distance visual acuity; Km, mean keratometry; ACD, anterior chamber depth; IOPc, corrected intraocular pressure.
Changes in amplitude of accommodation
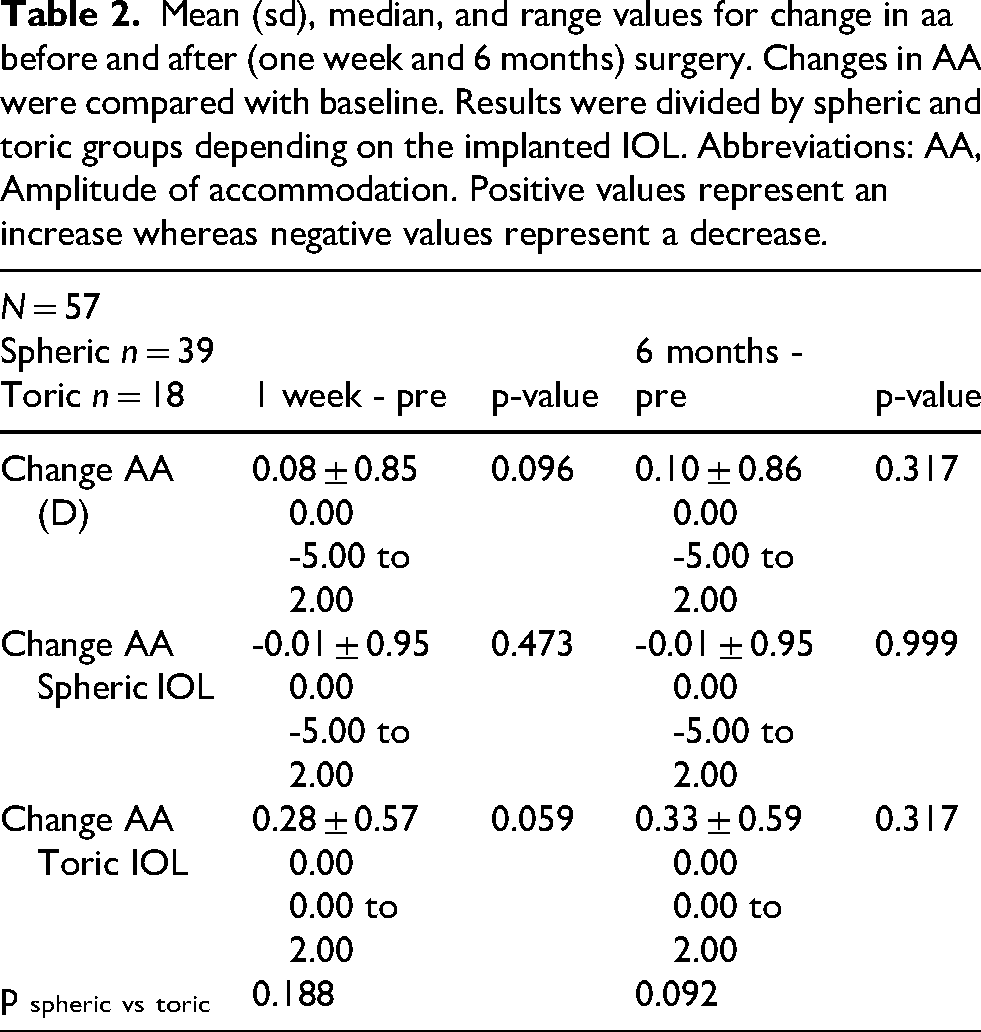
Longitudinal analysis revealed no clinically or statistically significant changes in AA from baseline to 1-week (p = 0.096) or 6-month postoperative visits (p = 0.317) (Table 2). Indeed, the mean change in AA in the whole sample was close to 0.10 D. While both spherical and toric IOL groups maintained stable accommodation (p ≥ 0.059), a nonsignificant trend toward improved AA was observed in the toric group. In addition, no significant differences were found in the accommodative changes found with spherical and toric models (p ≥ 0.092).
Mean (sd), median, and range values for change in aa before and after (one week and 6 months) surgery. Changes in AA were compared with baseline. Results were divided by spheric and toric groups depending on the implanted IOL. Abbreviations: AA, Amplitude of accommodation. Positive values represent an increase whereas negative values represent a decrease.
Changes in AA at 1-week (ρ=0.378, p = 0.004) and 6 months (ρ=0.336, p = 0.011) were significantly correlated with age (Figure 1). No statistically significant correlations were found with other parameters at any visit: SE (ρ=0.106, p = 0.433 and ρ=0.134, p = 0.320); AA (ρ=0.108, p = 0.422 and ρ=0.166, p = 0.216); AXL (ρ=-0.170, p = 0.205 and ρ=-0.217, p = 0.105); WTE (ρ=-0.001, p = 0.992 and ρ=-0.052, p = 0.702); ACD (ρ=-0.119, p = 0.377 and ρ=-0.155, p = 0.250); Km (ρ=-0.018, p = 0.893 and ρ=0.027, p = 0.844); CCT (ρ=0.080, p = 0.552 and ρ=0.038, p = 0.778); IOP (ρ=-0.189, p = 0.160 and ρ=-0.197, p = 0.142); spherical IOL power (ρ=0.103, p = 0.444 and ρ=0.148, p = 0.273); and cylinder IOL power (ρ=-0.178, p = 0.185 and ρ=-0.245, p = 0.067).
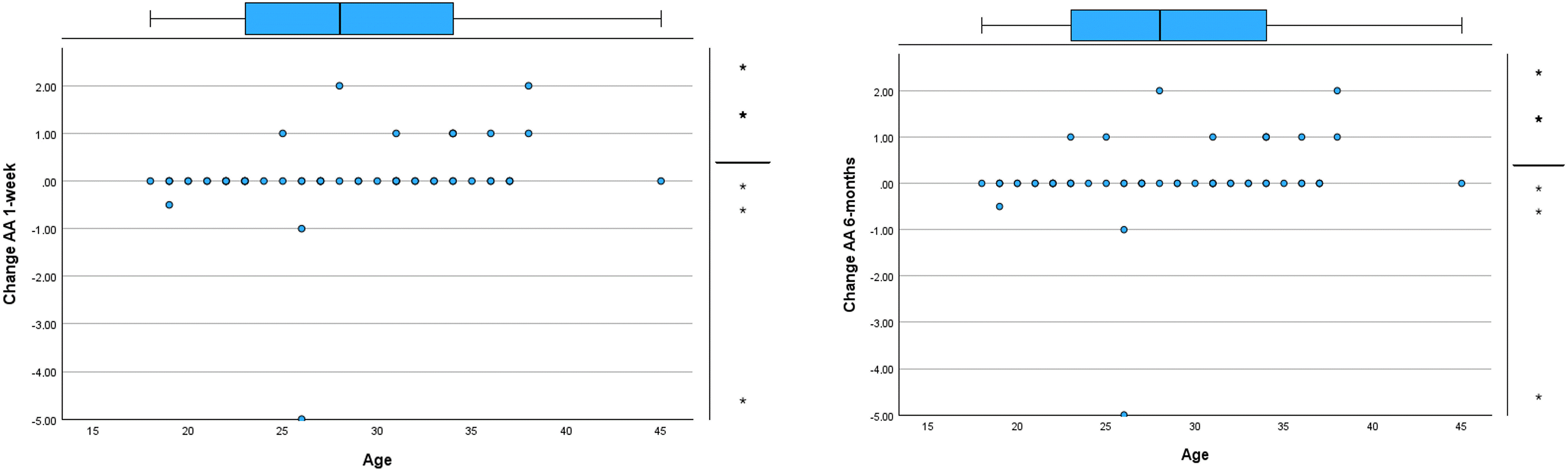
Scatterplot showing the relationship between age and change in amplitude of accommodation (aa) at 1 week and 6 months after surgery. Likewise, a box plot showing the distribution of the AA is provided. The boxes represent the interquartile range (IQR) (difference between the upper 75% and lower quartile 25%); the thick black lines, the median; the whiskers, the highest and lowest values that were not outliers or extreme values; the circle, an outlier (value between 1.5 and 3.0 times the IQR); and the asterisks, extreme values (values more than 3 times the IQR).
Discussion
The implantation of pIOLs has emerged as a safe and effective approach for myopia correction, despite the inherent risks associated with any surgical intervention. 4 Both anterior and posterior chamber pIOL designs offer distinct advantages and limitations,7–10 with the ultimate treatment choice depending on a careful consideration of patient-specific factors, surgeon expertise, and overall ocular health. While the refractive outcomes and safety profiles of pIOLs are well-established, recent research has increasingly focused on their impact on broader visual functions, particularly accommodative performance.12–17 Posterior chamber pIOLs have been extensively studied in this regard, with consistent reports demonstrating reduced accommodative amplitude and altered ciliary muscle function.12–14,16,17 However, the accommodative effects of anterior chamber pIOLs remain largely unexplored - a significant knowledge gap given their different anatomical position and fixation mechanism. The current study specifically addresses this gap by evaluating accommodative changes following implantation of the iris-fixed Artiflex pIOL. Unlike posterior chamber designs that interact with the ciliary sulcus, the anterior chamber placement of Artiflex lenses theoretically preserves normal ciliary muscle anatomy and function. Our investigation provides the first comprehensive analysis of whether this theoretical advantage translates to maintained accommodative performance in clinical practice.
Our analysis revealed minimal fluctuations in AA following Artiflex pIOL implantation, with a slight non-significant increase that remained stable throughout postoperative visits. This stability contrasts markedly with published reports on posterior chamber ICLs, which consistently demonstrate substantial accommodative changes.12,13,14,16,17 The observed preservation of accommodative function in our cohort differs particularly from the findings of Tang et al. (2016) with a posterior chamber pIOL, 12 who reported >3.00 D reductions in AA using identical minus-lens methodology. While some ICL studies describe partial recovery of accommodation during follow-up,14,16,17 many note persistent deficits compared to preoperative baselines.14,17 Our results suggest the anatomical position of anterior chamber pIOLs may better preserve ciliary muscle dynamics compared to sulcus-placed ICLs. Future studies should evaluate other accommodative parameters such as accommodative facility or the magnitude of accommodative LAG with the Artiflex pIOL.
The subgroup analysis revealed interesting trends in accommodative response between spherical and toric Artiflex implants. While no statistically significant differences emerged between groups, a consistent pattern of marginally better accommodative performance in the toric cohort was observed. Notably, the spherical IOL group demonstrated greater variability, with one outlier showing a 5.00 D reduction in AA. When excluding this outlier, the spherical group's mean AA change increased to +0.11 ± 0.49 D (median: 0.00 D; range: −1.00 to +2.00 D), reflecting a minimal change in accommodative function, reduced variability compared to the full dataset, and maintenance of the performance gap relative to toric implants. Despite these trends, the intergroup differences failed to reach either clinical or statistical significance (p > 0.05). This suggests that both spherical and toric designs generally preserve preoperative accommodative capacity.
When interpreting our AA findings, several methodological factors warrant careful consideration. The Sheard technique, while clinically useful, carries inherent limitations due to its subjective nature.28–30 This psychophysical method relies on patients’ blur perception thresholds, which may introduce variability from both individual response differences and testing conditions, potentially overestimating true accommodative capacity compared to objective measures. 28 Objective measures of the crystalline anterior and posterior surface movement by means of OCT technology have been also used to evaluate the cryistaline lens during accomodation after an iris-claw implantation. 31 Our study design incorporated important safeguards to address these limitations: longitudinal changes (pre- vs post-operative values) rather than absolute measurements were analyzed, all testing was performed under standardized photopic conditions, and the same examiner conducted all measurements using consistent methodology. However, certain constraints should be acknowledged, such as the psychophysical nature of the test that precludes definitive conclusions about physiological accommodative capacity and the limitation of our analysis to monocular assessment of a randomly selected eye. These considerations suggest our findings should be interpreted as demonstrating relative stability of subjective accommodative response rather than absolute preservation of accommodative function.
Our correlation analysis revealed a poor but significant positive relationship between age and changes in AA after surgery (r = 0.336–0.378, p < 0.05). This finding aligns with established literature demonstrating age-related declines in accommodative function. 32 The observed correlation likely reflects the natural progression of presbyopia during the study period, particularly given that older subjects showed more pronounced AA reduction, the longitudinal design encompassed the presbyopic transition period for some patients and that age remains the strongest predictor of accommodative capacity in phakic adults.
Regarding the primary refractive objectives of the surgical intervention, they were successfully achieved. There was a significant reduction in spherical error, cylinder, and spherical equivalent (all p < 0.05), stable refractive outcomes maintained through 6-month follow-up, clinically meaningful improvement in UDVA, and modest but statistically significant gains in CDVA. The CDVA improvement (mean +0.04 to +0.08 logMAR), while statistically significant, represents a subtle clinical change consistent with previous Artiflex studies.18,19,21,25 This effect may be attributable to elimination of spectacle magnification effects, reduced retinal image minification compared to high-minus spectacles, and improved optical quality through elimination of spectacle aberrations.18,19,21,25 In addition, postoperative anatomical assessment revealed a small, but significant ACD reduction (mean −0.10 mm) that may be attributed to changes in the magnification of anterior segment image due to the introduction of the pIOL, leading to some level of bias of ACD measures. 33 Stable corneal curvature (Km) and IOP measurements confirm minimal corneal impact and an appropriate IOL sizing and positioning.
This study has some limitations that should be acknowledged. First, there was no control group for comparison. In any case, the follow-up period was only 6 months and minimal changes are expected to occur in a non-operated group as this follow-up period is short to detect age-related accommodative changes. Second, this is a retrospective study, but it should be considered that the clinical protocol followed in our clinical practice is very strict in terms of measures and follow-up visits. Finally, other accommodative measures such as accommodative facility (with flipper lenses) may have been included to provide an integral analysis of the accommodative function. This should be considered for future studies.
In conclusion, our study demonstrates that Artiflex anterior chamber pIOL implantation preserves accommodative function, with no clinically significant changes in amplitude of accommodation observed postoperatively. This stability occurs regardless of lens type (spherical or toric), suggesting the iris-fixated design maintains normal ciliary muscle dynamics. These results underscore the need for direct comparative studies evaluating accommodative changes between anterior and posterior chamber pIOLs using standardized protocols. Future research should incorporate both subjective (e.g., Sheard method) and objective accommodation assessments to fully characterize these functional differences.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article. No funding was received for the performance of this research
Disclosure
The authors have no proprietary or commercial interest in the medical devices that are involved in this manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.