
Abstract
Purpose
To evaluate the clinical outcomes and safety of the Nishida muscle transposition procedure performed without tenotomy or muscle splitting in patients with severe paralytic horizontal or vertical strabismus.
Methods
This retrospective case series included 16 patients with complete paralytic strabismus who underwent Nishida transposition between January 2020 and September 2021. Eleven patients had abducens nerve palsy and five had vertical paralytic strabismus (elevation or infraduction deficiency). The procedure involved scleral fixation of adjacent rectus muscles closer to the paralyzed muscle without tendon disinsertion, preserving anterior ciliary circulation and allowing simultaneous antagonist recession when indicated. Outcomes included ocular alignment in primary position, ocular motility, binocular single vision, and postoperative complications over a follow-up period of 5–15 months.
Results
In abducens nerve palsy, combined transposition with medial rectus recession—performed using a standardized protocol based on preoperative deviation (6 mm for ≥80 prism diopters [PD] and 5 mm for <80 PD)—achieved a mean correction of 69.2 ± 12.8 PD, whereas isolated transposition resulted in a correction of 29 PD. In vertical paralytic strabismus, the mean correction was 38 ± 19.8 PD. All patients demonstrated improved duction beyond the midline postoperatively. Eight patients achieved binocular single vision in primary position and four with compensatory head posture. No anterior segment ischemia, induced secondary deviations, or other major complications were observed.
Conclusions
The Nishida procedure provides effective and safe correction of severe paralytic strabismus while preserving muscle insertions and anterior ciliary circulation. Its compatibility with simultaneous antagonist recession makes it a valuable single-stage approach for large-angle paralytic deviations.
Keywords
Introduction
Paralytic strabismus with absent ocular movement beyond the midline represents a profound loss of extraocular muscle function and is among the most challenging forms of ocular misalignment to manage clinically. 1 In such cases, conventional recession–resection procedures are often insufficient because they rely on residual muscle force that is functionally absent. As a result, various rectus muscle transposition techniques have been developed to redirect force from normally functioning muscles toward the paralyzed vector. 2
Classical procedures such as the Hummelsheim operation for abducens nerve palsy and the Knapp or reverse Knapp procedures for vertical paralytic strabismus can yield meaningful correction, but they require full rectus muscle tenotomy and tendon manipulation. These maneuvers disrupt anterior ciliary circulation, increase the risk of anterior segment ischemia (ASI), and may necessitate staged surgery when antagonist weakening is also required. 3 Jensen's 1964 procedure sought to preserve the anterior ciliary vessels by avoiding tenotomy and uniting adjacent rectus muscles without disinsertion. 4 Although safer, the technique involves three rectus muscles and remains relatively invasive, and cases of ASI have still been reported.5,6
In the early 2000s, Nishida and colleagues proposed a new muscle transposition concept in which the vertical rectus muscles were sutured to the sclera without tendon splitting or disinsertion, thereby preserving anterior segment circulation.7,8 Subsequent refinements demonstrated successful outcomes for abducens palsy and monocular elevation deficiency while minimizing ischemic risk. 9 However, the traditional Nishida approach places the scleral fixation point midway between adjacent rectus insertions, which may be insufficient for large deviations. Previous studies (e.g., Ref. 10) have also suggested that positioning the fixation closer to the paralyzed muscle may enhance transpositional force; however, this modification has not been consistently emphasized or systematically evaluated across different forms of paralytic strabismus. Moreover, its use in vertical paralytic strabismus has been limited.
Based on these limitations, in this study we applied the Nishida procedure with a modified scleral fixation position placed closer to the paralyzed rectus muscle to enhance transpositional force, while preserving the core principles of the original technique, including absence of tenotomy, no muscle splitting, and preservation of anterior ciliary circulation. Unlike classical approaches, this adaptation is designed to permit simultaneous antagonist recession in a single surgical session, making it particularly suited for large-angle deviations. The purpose of this study was to evaluate the clinical outcomes of this Nishida muscle transposition procedure in patients with severe paralytic horizontal or vertical strabismus, focusing on ocular alignment, motility recovery, binocular function, and safety.
Patients and methods
Patients
This retrospective case series included 16 consecutive patients with paralytic strabismus who presented to our hospital between January 2020 and September 2021. Of these, 11 patients had abducens nerve palsy, 3 had monocular elevation deficiency, and 2 had infraduction deficiency. All affected eyes demonstrated complete limitation of ocular movement that did not cross the midline, confirming the diagnosis of paralytic motility restriction. All procedures were conducted in accordance with the ethical standards of the Xiamen Eye Center Ethics Board and the 1964 Declaration of Helsinki and its later amendments. Because this investigation involved retrospective review of de-identified clinical data, the institutional review board waived the requirement for written informed consent. Written informed consent was obtained only for the publication of identifiable clinical photographs from the relevant patient(s).
Patient preparation
All patients underwent a comprehensive preoperative ophthalmic assessment, which included routine ocular examination, synoptophore evaluation, assessment of oculomotor function and diplopia, color fundus photography, prism cover testing, and retraction testing to exclude mechanical restriction. Surgeries were performed under general anesthesia with endotracheal intubation, and all procedures were conducted using an operating microscope. A forced-duction test was systematically performed after induction of anesthesia to differentiate paralytic from restrictive motility deficits. Ocular motility was graded on a standard −4 to 0 scale, where −4 indicated no movement beyond the midline, −3 limited movement toward the midline, −2 partial movement beyond the midline, −1 nearly full movement, and 0 full duction. The inclusion criteria were: patients with paralytic horizontal or vertical strabismus demonstrating absence of ocular movement beyond the midline on duction testing. The exclusion criteria were: restrictive strabismus, thyroid-associated ophthalmopathy, and any form of paralytic strabismus in which residual movement crossed the midline, indicating partial rather than complete paresis. The amount of medial rectus recession was determined based on preoperative deviation and was not modified intraoperatively based on forced-duction testing.
Surgical procedures
For cases with a paralyzed lateral rectus muscle requiring vertical rectus transposition, a standard trapezoidal conjunctival incision was created in the superotemporal or inferotemporal quadrant, depending on the planned approach. In patients with horizontal strabismus, after isolating each vertical rectus muscle, a 5-0 polyester nonabsorbable suture (Alcon Laboratories, Incorporated, USA) was passed through the temporal margin of the superior and inferior rectus muscles at approximately one-third of the muscle width from the lateral edge, positioned 8–10 mm posterior to their anatomical insertions. Two passes were placed at slightly offset positions to reduce the risk of suture slippage along the muscle fibers. The suture was then secured to the sclera 10–12 mm posterior to the limbus, immediately adjacent to the paralyzed lateral rectus muscle, while carefully avoiding the vortex veins during scleral placement.
In patients with vertical strabismus, the same technique was applied to the horizontal rectus muscles. A suture was placed through the superior margin of the medial and lateral rectus muscles for elevation deficits, or through the inferior margin for infraduction deficits, again positioned one-third of the muscle width from the edge and 8–10 mm posterior to the insertion. The suture was subsequently anchored 10–12 mm posterior to the limbus in the quadrant adjacent to the paralyzed vertical rectus muscle (Figure 1). Compared with the original Nishida procedure, the scleral fixation point in this study was positioned closer to the paralyzed rectus muscle to enhance transpositional force; however, the fundamental characteristics of the Nishida technique—namely, absence of tenotomy or muscle splitting and preservation of anterior ciliary circulation—were maintained. This modification is consistent with previously reported approaches (Ref. 10), which advocate positioning sutures closer to the paralyzed muscle to improve surgical effectiveness.
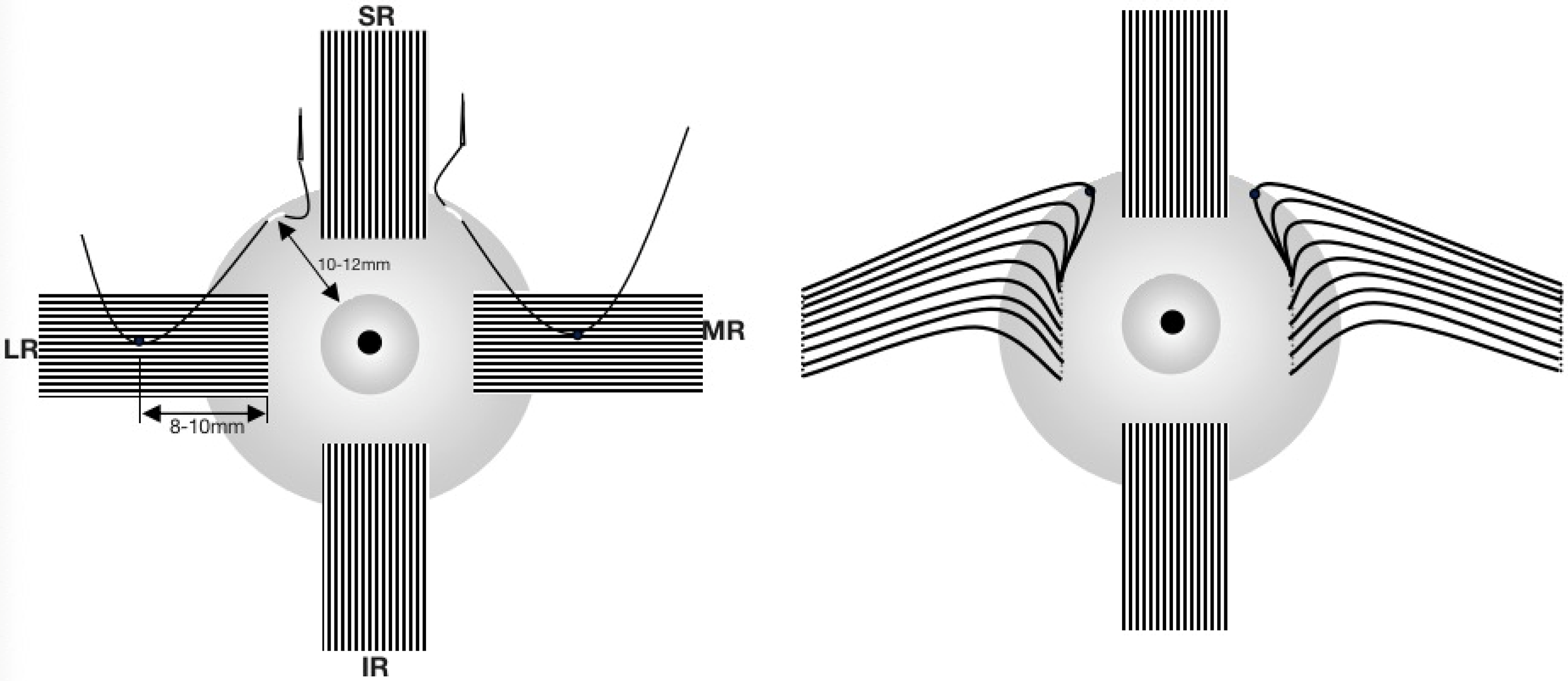
Muscle transposition procedure of the right eye.
Statistical analyses
All statistical analyses were performed using SPSS software, version 21.0 (IBM Corp., Armonk, NY, USA). Continuous variables are presented as mean ± standard deviation (SD), median, and range, as appropriate. Because this was a retrospective descriptive case series with a small sample size and no comparison groups, no inferential statistical tests were applied. The analysis focused on descriptive outcomes, including preoperative and postoperative deviations, the amount of strabismus correction achieved, and follow-up stability over time. A two-tailed significance threshold of P < 0.05 was defined for completeness, although no hypothesis-testing was undertaken due to the descriptive nature of the study.
Results
Horizontal strabismus (abducens nerve palsy)
Table 1 summarizes the patients’ clinical and demographic characteristics. Among the 11 patients with abducens nerve palsy, the underlying causes included trauma in five, nasopharyngeal carcinoma in two, brain tumor in two, and unknown etiology in two. The mean age (± standard deviation [SD]) was 51.4 ± 12.5 years (range: 28–69 years), the mean disease duration was 15.9 ± 11.4 months (range: 6–42 months), and the mean follow-up period was 9.2 ± 2.7 months (range: 6–15 months). The mean preoperative horizontal deviation was 66.1 ± 21.6 prism diopters (PD; range: 25–100 PD), and the mean postoperative deviation was 1.27 ± 5.7 PD (range: −8 to +12 PD). Case 5 had previously undergone medial rectus recession (5 mm) and lateral rectus resection (8 mm) at another institution but remained with 25 PD esotropia and marked limitation of abduction. After undergoing the present procedure, oculomotor function and alignment improved substantially. All other patients with abducens palsy underwent simultaneous medial rectus recession according to a standardized protocol based on preoperative deviation (6 mm for ≥80 PD and 5 mm for <80 PD).
Patients’ clinicodemographic characteristics.
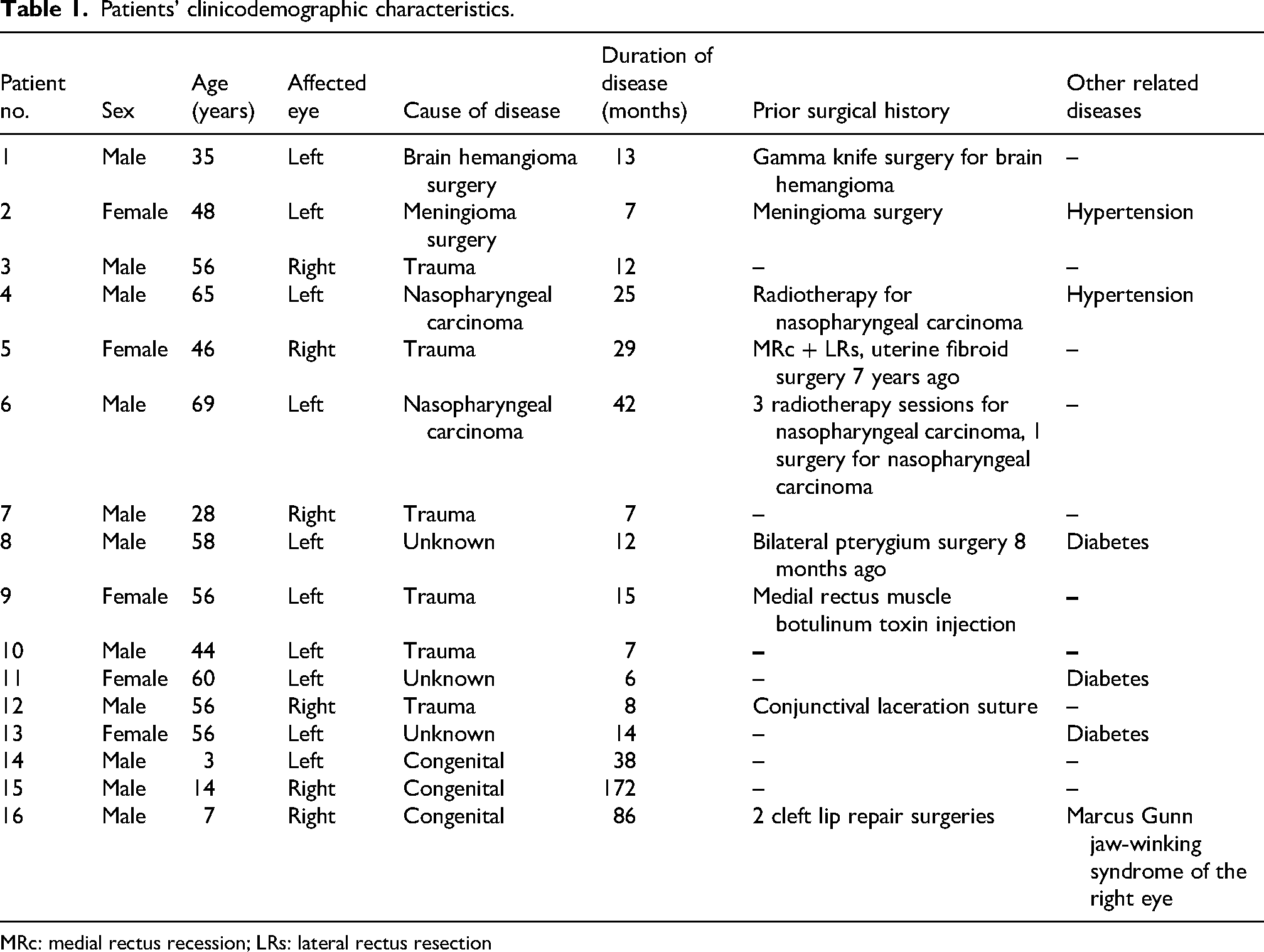
MRc: medial rectus recession; LRs: lateral rectus resection
Vertical strabismus (elevation and infraduction deficiency)
Five patients exhibited vertical paralytic strabismus, including three with congenital causes and two of unknown origin. Their mean age (± SD) was 27.2 ± 26.6 years (range: 3–56 years), the mean disease duration was 63.6 ± 67.9 months (range: 8–172 months), and the mean follow-up duration was 6.8 ± 1.9 months (range: 5–10 months). Preoperatively, although the primary presentation was vertical motility limitation, mild associated horizontal deviations were observed in some patients (e.g., esotropia in Case 15). In such cases, additional horizontal muscle procedures, including medial rectus recession, were performed based on the magnitude of horizontal deviation to achieve optimal ocular alignment, as detailed in Table 2. Case 16 had congenital Marcus Gunn jaw-winking syndrome associated with elevation deficiency, with a stable deviation that did not vary with eyelid movement. Both antagonist and yoke muscle recession (4 mm) were performed simultaneously in this patient. The mean preoperative vertical deviation in the vertical-strabismus group was 39.4 ± 23.9 PD (range: 20–80 PD), and the mean postoperative deviation was 1.4 ± 4.2 PD (range: −8 to +3 PD). A representative vertical-strabismus case (Patient 15), demonstrating preoperative limitation of elevation with right-eye esotropia and postoperative improvement in alignment and elevation, is illustrated in Figures 2 and 3.
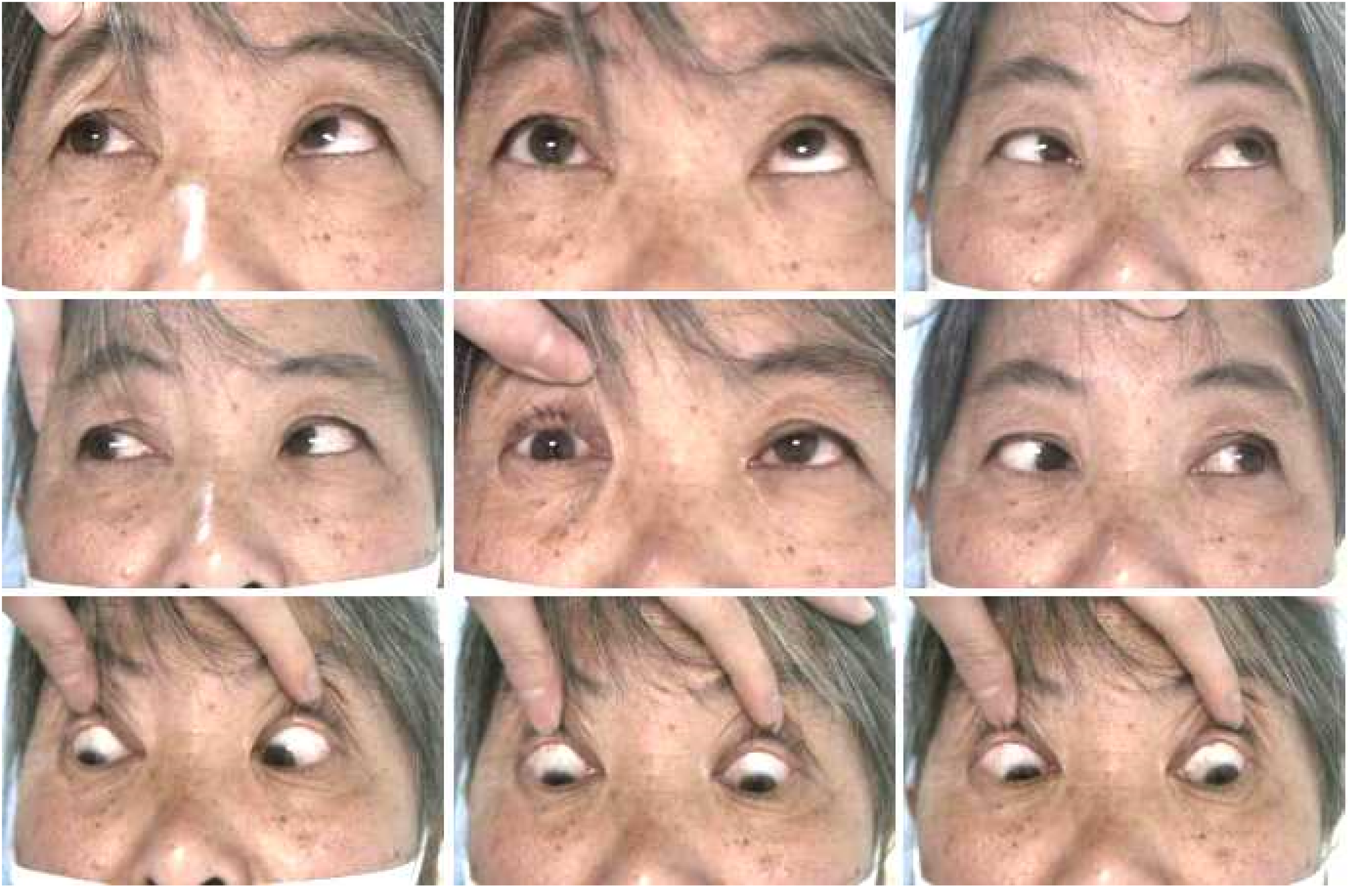
Preoperative photographs of patient 15 showing double elevator palsy with right-eye esotropia. Vertical strabismus is evident, and ocular elevation does not cross the midline. Written informed consent for publication of these clinical images was obtained.

1 week post-operative photographs of patient 15 demonstrating marked improvement in ocular alignment and elevation, with eye movement extending beyond the midline following surgery. Written informed consent for publication of these clinical images was obtained.
Preoperative and postoperative strabismus at far distance in the original position.
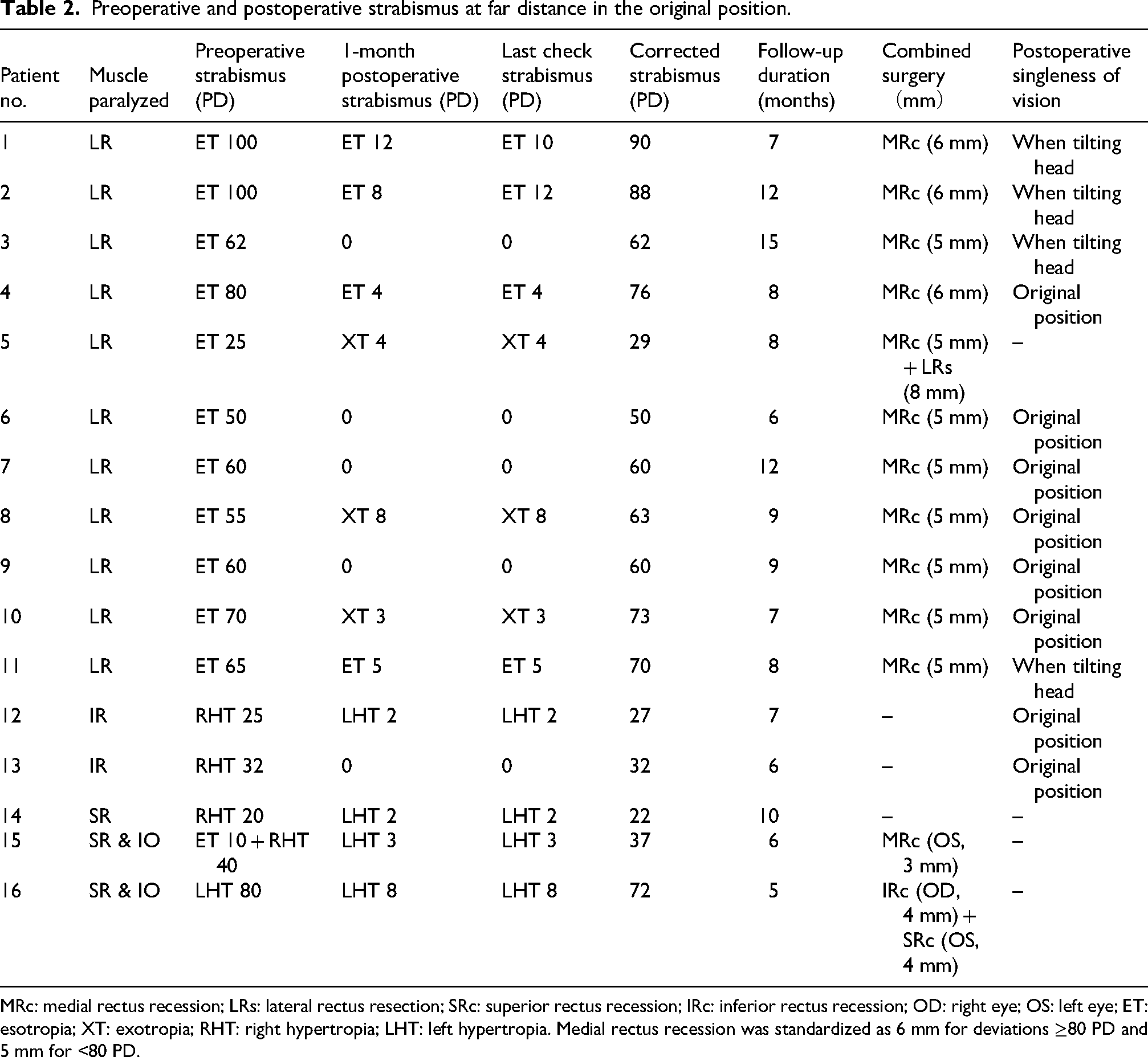
MRc: medial rectus recession; LRs: lateral rectus resection; SRc: superior rectus recession; IRc: inferior rectus recession; OD: right eye; OS: left eye; ET: esotropia; XT: exotropia; RHT: right hypertropia; LHT: left hypertropia. Medial rectus recession was standardized as 6 mm for deviations ≥80 PD and 5 mm for <80 PD.
Binocular function and complications
Across the entire cohort, eight patients achieved binocular single vision (Titmus Stereo Test) in primary position, and four achieved binocular single vision with compensatory head posture. The remaining four did not attain binocular single vision. Alignment was maintained during the available short- to mid-term follow-up (5–15 months), although this duration is insufficient to assess long-term stability. Two patients with abducens palsy exhibited small residual deviations (+10 PD and +12 PD), which were managed with press-on prism lenses to correct compensatory head posture. Importantly, no postoperative complications, including anterior segment ischemia, were observed. No patient with horizontal strabismus developed a new vertical deviation, and no patient with vertical strabismus developed a new horizontal deviation. The function of all transposed muscles remained intact throughout the follow-up period.
Discussion
The present study evaluated the clinical effectiveness of a Nishida muscle transposition procedure performed without tenotomy or muscle splitting in two distinct groups of paralytic strabismus: horizontal (abducens nerve palsy) and vertical (elevation or infraduction deficiency). Across all 16 patients, the procedure produced substantial alignment improvements with preservation of muscle function and without postoperative complications. To ensure accurate interpretation, the outcomes of horizontal and vertical paralytic strabismus are discussed separately below, as these conditions differ fundamentally in pathophysiology, clinical presentation, and expected surgical response.
Outcomes in horizontal strabismus (abducens nerve palsy)
Patients with complete abducens palsy demonstrated marked improvement following the Nishida procedure, particularly when combined with medial rectus recession. The mean correction achieved in our horizontal strabismus group (69.2 ± 12.8 PD for combined procedures and 29 PD for isolated transposition) aligns with or exceeds previously reported outcomes for the Hummelsheim, Jensen, and superior rectus transposition techniques,9–14 including recent large-cohort studies evaluating the Nishida procedure in abducens nerve palsy. 10
Traditional vertical rectus transposition procedures require complete tenotomy of two rectus muscles and may disrupt the anterior ciliary vessels (ACVs), increasing the risk of anterior segment ischemia (ASI) and limiting the ability to perform simultaneous medial rectus recession. In contrast, the Nishida approach used in this study avoided tenotomy entirely, preserved ACV integrity, and still allowed combined medial rectus surgery when indicated. Importantly, medial rectus recession in our cohort was applied using a standardized dosing protocol based on preoperative deviation, which enhances the reproducibility of this combined surgical approach. This likely contributed to the substantial corrections observed in larger-angle esotropia, enabling improved abduction and primary-position alignment without inducing vertical imbalance.
Outcomes in vertical strabismus (elevation and infraduction deficiency)
Vertical paralytic strabismus has a different biomechanical and clinical profile from sixth-nerve palsy; therefore, its surgical outcomes must be interpreted independently. In our vertical group, the Nishida procedure produced a mean correction of 38 ± 19.8 PD, with postoperative mobility extending beyond the midline in all patients. This performance is comparable to historical outcomes of the Knapp and reverse Knapp procedures, which require complete tenotomy of both horizontal rectus muscles.
Our technique allowed effective elevation or depression improvement while maintaining muscle integrity and minimizing surgical trauma, similar to outcomes recently reported using Nishida-based approaches in monocular elevation deficiency and postoperative vertical rectus injuries.15–18 Notably, no patient developed a new horizontal deviation, supporting the stability of the procedure in vertical cases.
Advantages of the Nishida approach
The present approach represents an adaptation of the Nishida procedure in which the scleral fixation point is positioned closer to the paralyzed rectus muscle, rather than at the midpoint between adjacent recti, thereby allowing greater transpositional force. This concept has been previously reported (Ref. 10); however, our study further emphasizes its clinical applicability by systematically implementing this modification across both horizontal and vertical paralytic strabismus and combining it with a standardized antagonist recession protocol. Importantly, this adjustment does not alter the fundamental principles of the Nishida technique, as no tenotomy or muscle splitting is performed and anterior ciliary circulation is preserved. Preservation of all muscle insertions reduces the risk of slippage, ischemic complications, and postoperative motility loss. Because the procedure does not disturb the ACVs, combined antagonist or yoke-muscle recession can be safely performed in a single stage, an important advantage for large-angle deviations. This may partially explain the larger corrections observed in our horizontal group compared with earlier reports. Thus, rather than introducing a completely novel technique, our study provides a structured and clinically validated application of this previously described modification. Unlike previous reports, this study specifically evaluates a modified scleral fixation strategy positioned closer to the paralyzed rectus muscle, along with a standardized protocol for antagonist recession, thereby providing additional practical guidance for surgical decision-making in cases of complete paralytic strabismus.
Stability of alignment and binocular function
The improvements in ocular alignment were maintained over the available short- to mid-term follow-up (5–15 months); however, this interval is too limited to draw firm conclusions about long-term stability. Binocular function outcomes were heterogeneous but generally favorable, with approximately half of the patients achieving fusion in primary position and an additional quarter achieving fusion with compensatory head posture. These findings indicate that motor realignment was consistently obtained, but sensory outcomes appear to depend on individual patient characteristics, duration of disease, and preexisting binocular status.
Limitations
This study has several limitations. First, the small sample size and retrospective design limit generalizability. Second, follow-up was relatively short, making long-term stability and sensory outcomes uncertain. Third, direct comparison with classical procedures such as the Hummelsheim, Knapp, or Jensen techniques is limited and should be interpreted with caution, as the larger horizontal corrections observed in our cohort likely reflect, in part, the use of simultaneous medial rectus recession rather than the transposition alone. Nevertheless, the present study provides additional clinical insight by focusing on severe cases with complete motility limitation and by applying a standardized and reproducible combined surgical approach, aspects that are not consistently detailed in prior literature. Future studies with larger cohorts, control groups, and long-term follow-up are needed to validate and refine these findings.
Conclusion
The Nishida muscle transposition procedure evaluated in this study provided substantial correction of both horizontal and vertical paralytic strabismus while preserving rectus muscle insertions and avoiding tenotomy or muscle splitting. By anchoring adjacent rectus muscles to the sclera near the paralyzed muscle and maintaining anterior ciliary circulation, the technique improved large-angle deviations and restored ocular motility beyond the midline with a favorable short- to mid-term safety profile and no observed anterior segment ischemia. Functional outcomes were also encouraging, with many patients achieving binocular single vision in primary position or with compensatory head posture. These findings build upon previously described modifications of suture positioning (Ref. 10) and further support their clinical applicability. However, the retrospective design, small sample size, heterogeneity of etiologies, and limited follow-up duration restrict the strength of the conclusions and preclude firm statements about long-term stability or superiority over classical transposition procedures. Larger prospective, controlled studies with longer follow-up are needed to better define the indications, comparative efficacy, and durability of this approach.
Footnotes
Competing interests
The authors declare that they have no competing interests.
Funding
This work was supported by the Natural Science Foundation of Xiamen, China (Grant No. 3502Z202374102); the Science and Technology Project of Fujian Province (Grant No. 2024D006); the Guiding Project of Medical and Health of Xiamen, China (Grant No. 3502Z20244ZD1194); and the Guiding Project of Combination of Medicine and Engineering of Xiamen, China (Grant No. 3502Z20244ZD2041).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of data and materials
The datasets generated and/or analyzed during the current study are not publicly available due to patient privacy considerations but are available from the corresponding author on reasonable request.