
Abstract
Background
Young-onset type 2 diabetes mellitus is associated with prolonged disease duration and early development of complications such as diabetic retinopathy. Smoking is a modifiable risk factor, but longitudinal evidence in this population remains limited.
Objective
To evaluate the association between long-term smoking and the risk of diabetic retinopathy, including earlier-occurring cases, in young-onset type 2 diabetes mellitus.
Methods
This retrospective cohort study used electronic medical records and a diabetic complication database from Pu'er People's Hospital, this retrospective cohort study included 488 patients aged 18–39 with type 2 diabetes (2023–2025) and no DR at baseline. Patients were followed from diabetes diagnosis until DR, last fundus exam, death, or June 30, 2025. Smoking status and cumulative exposure were assessed, and patients were followed until incident diabetic retinopathy or censoring. Kaplan–Meier analysis, Cox regression, restricted cubic splines, and sensitivity analyses were performed.
Results
During follow-up, 92 patients developed diabetic retinopathy, including 61 earlier-occurring cases. Smokers had a significantly higher cumulative incidence of diabetic retinopathy. Adjusted analyses showed that smoking was associated with increased risk of diabetic retinopathy (hazard ratio 1.78, 95% confidence interval 1.18–2.69) and earlier-occurring diabetic retinopathy (hazard ratio 1.92, 95% confidence interval 1.21–3.05). A nonlinear dose–response relationship was observed, with greater cumulative exposure associated with earlier onset.
Conclusion
Long-term smoking is associated with higher risk and earlier occurrence of diabetic retinopathy in young-onset type 2 diabetes mellitus, supporting early screening and smoking cessation strategies in this high-risk population.
Keywords
Introduction
In recent years, diabetes has evolved from a chronic disease management issue into a core challenge of global public health and health economics. The latest International Diabetes Federation (IDF) Diabetes Atlas, 11th edition, indicates that in 2024 approximately 589 million adults aged 20–79 worldwide had diabetes (about 1 in 9 adults), a figure projected to rise to 853 million by 2050.1,2 Diabetes-related mortality and healthcare expenditures also continue to increase, with diabetes accounting for approximately 3.4 million deaths and global health spending of about US$1.015 trillion in 2024.3,4 Concurrently, the burden of diabetes is accumulating more rapidly among younger populations. Multi-country surveillance and international collaborative studies suggest an increasing incidence of diabetes with onset in youth and young adulthood, with distinct patterns of increase and population differences across diabetes types. 5 This trend signals an emerging crisis of complications arriving earlier in life, characterized by longer disease duration, earlier complication onset, and higher lifetime risks. 6
Among diabetic microvascular complications, diabetic retinopathy (DR) is a leading cause of vision impairment and avoidable blindness, 7 its public health impact and disease burden having been confirmed by multiple global studies. Recent systematic reviews and meta-analyses estimate a high overall prevalence of DR in diabetic populations, with significant regional variations. 8 Against the backdrop of a growing global diabetic population, DR screening and early prevention face mounting pressure. 9 More critically, the mere occurrence of DR does not fully capture the underlying risk structure. Earlier onset of DR often reflects greater microvascular vulnerability, a faster progression trajectory, and a higher cumulative risk of blindness. 10 Reducing DR to a binary outcome (present/absent) may underestimate its true risk profile. The progression of DR exhibits clear time-to-event characteristics and considerable interindividual heterogeneity; early-onset DR typically indicates heightened microvascular susceptibility and is associated with more rapid advancement to vision-threatening stages and poorer long-term visual outcomes. In this regard, youth- or young-onset type 2 diabetes (YOD/T2DM) populations offer a representative real-world example. For instance, long-term follow-up from the TODAY study demonstrated that DR can develop and progress within a relatively short diabetes duration among young-onset T2DM patients, highlighting the aggressive nature of complications in this group. 11 Similarly, contemporary real-world cohorts of adolescents with T2DM show that a notable proportion develop microvascular complications, including DR, even with relatively short diabetes duration and modern glucose-lowering therapies, suggesting that glycemic control alone may not fully offset early microvascular risk. 12 Therefore, research focusing on early-onset DR and identifying modifiable risk factors holds more direct clinical relevance for preventing long-term visual outcomes in young-onset T2DM. 13
Among numerous potentially modifiable exposures, smoking is characterized by long-term cumulative damage across multiple organ systems and has a biologically plausible role in metabolic and microvascular pathology. Recent reviews indicate that smoking may exacerbate insulin resistance, impair β-cell function through multiple pathways, and elevate the risk of diabetes-related vascular complications. 14 While the overall evidence supports adverse effects of smoking on diabetic microvascular outcomes, findings specifically regarding DR have been inconsistent. Some studies report a negative association or even an apparent protective effect of smoking on DR risk in certain subgroups, attributing such findings to confounding, selection bias, or methodological issues. 15 Others emphasize that variations in study design, DR grading criteria, diabetes types, and population characteristics may lead to unstable associations, underscoring the need for reassessment within more clearly defined populations and a more rigorous time-to-event framework. 16 Particularly in young-onset T2DM—a population with faster complication progression and a more critical follow-up window—smoking may not only influence whether DR develops but also affect how early it occurs and the rate of risk accumulation. However, evidence in this specific population remains limited. Recent literature has further emphasized that DR risk should be interpreted within a broader framework that includes modifiable systemic exposures, evolving treatment strategies, and earlier preventive intervention before vision-threatening stages develop.17–19 At the mechanistic level, contemporary reviews of diabetic retinal injury also highlight the importance of glycation-related stress, oxidative injury, inflammation, endothelial dysfunction, and neurovascular unit damage, which provide a relevant biological context for evaluating smoking-related retinal microvascular vulnerability. 20
Against this background, this study focuses on young-onset T2DM patients, employing a retrospective cohort design to systematically evaluate the association between long-term smoking history and the risk of diabetic retinopathy, with particular emphasis on earlier occurrence during the available follow-up period, based on clearly defined follow-up start points and outcome definitions. Furthermore, it explores the consistency and robustness of findings using different characterizations of smoking exposure (e.g., current/former/never, or cumulative exposure metrics). To mitigate the influence of baseline differences and confounding inherent in observational studies, this study incorporates multivariable modeling and propensity score weighting methods in sensitivity analyses. The aim is to provide more actionable evidence for early risk stratification, prioritization of behavioral interventions, and optimization of clinical follow-up strategies for young-onset T2DM patients.
Materials and methods
Study population
This was a retrospective cohort study. Using the electronic medical record system and diabetic complication follow-up database of Pu'er People's Hospital, we retrospectively screened and consecutively included patients first diagnosed with type 2 diabetes between January 1, 2023, and June 30, 2025. Because the study cut-off date was June 30, 2025, the available follow-up duration varied across participants according to the date of diabetes diagnosis.
During this period, 642 patients with an initial screening record of type 2 diabetes were identified. We then applied the prespecified eligibility criteria in a stepwise manner. After applying the criteria, 154 patients were excluded and the final analytic cohort consisted of 488 young-onset type 2 diabetes patients.
A time-to-event analysis design was employed. The date of the first documented diagnosis of type 2 diabetes in the electronic medical records served as the follow-up start point (time zero). Follow-up continued until the earliest of the following: first definite diagnosis of diabetic retinopathy, censoring at the date of the last valid fundus examination showing no DR, patient death, or the study cut-off date (June 30, 2025). In this study, ‘last valid fundus examination’ refers to the last ophthalmic assessment with interpretable documentation available for outcome ascertainment in a participant who had not yet developed DR. Accordingly, the present dataset supports analysis of DR occurrence during the available follow-up period rather than estimation of a true 5-year cumulative risk for all participants. The occurrence of DR was determined by retrospectively reviewing fundus examination records and related clinical documentation during follow-up.
To reduce population heterogeneity and enhance the interpretability of results, the study was restricted to young-onset type 2 diabetes patients. The detailed operational definitions for inclusion and exclusion, including the requirements for smoking history documentation, baseline DR-free status, follow-up fundus examination, and handling of missing or inconsistent records, are provided in Section 2.3. Focusing on this specific population allowed for a retrospective assessment of the association between long-term smoking—a modifiable behavioral factor—and the risk of early-onset diabetic retinopathy after diabetes diagnosis, thereby better reflecting the distinct disease progression characteristics potentially present in young-onset compared to later-onset T2DM.
Ethics and informed consent
The study protocol was reviewed and approved by the Ethics Committee of Pu'er People's Hospital. The research involved retrospective analysis of data from existing electronic medical records and follow-up databases, with no prospective interventions, treatment modifications, or additional tests performed.
All data used were routinely collected during prior clinical care. Before data extraction and analysis, all patient information was anonymized and de-identified, making it impossible to identify any individual during the study. Given the retrospective design, minimal risk, and non-traceable nature of the data, the ethics committee granted a waiver of written informed consent. No additional participant contact or consent procedures were required because all analyses were conducted on de-identified routinely collected clinical data.
The study was conducted in accordance with the Declaration of Helsinki and relevant medical ethics standards. All data handling, storage, and analysis complied with privacy protection and data security management requirements.
Inclusion and exclusion criteria
To ensure a clearly defined at-risk cohort for incident DR analysis, eligibility criteria were prespecified before data extraction and were applied uniformly to all screened patients. The criteria were designed to identify young-onset type 2 diabetes patients who were free of DR at baseline, had ascertainable smoking exposure, and had adequate ophthalmic follow-up for time-to-event outcome assessment.
Inclusion criteria
Patients were included only if they met all of the following criteria:
They had a first unequivocal diagnosis of type 2 diabetes recorded between January 1, 2023, and June 30, 2025, and the diagnosis date could be reliably identified from the medical record. They were aged 18–39 years at the time of diagnosis, consistent with the definition of young-onset type 2 diabetes used in this study. They had sufficiently documented smoking history to permit exposure classification, including smoking status and, where applicable, smoking duration and daily cigarette consumption for pack-year calculation. They underwent a baseline fundus examination at diagnosis or within 6 months thereafter, and this examination documented the absence of definite DR, thereby establishing that the participant was event-free at cohort entry. They had at least one valid follow-up fundus examination with interpretable findings after cohort entry, so that incident DR during follow-up could be ascertained. They had at least 6 months of traceable follow-up after diabetes diagnosis, unless DR was identified earlier during a valid follow-up examination. They had complete key covariate information required for the primary analysis, including age at diagnosis, sex, smoking exposure, and fundus examination results.
Exclusion criteria
Patients were excluded if any of the following applied:
The diabetes type was not type 2 diabetes, including type 1 diabetes, gestational diabetes, or other specific diabetes types, or if diabetes classification was unclear. Definite or suspected DR was already present before the recorded diagnosis of diabetes or was identified on the baseline fundus examination, because such patients were not eligible for incident DR analysis. They had major non-diabetic ocular diseases that could interfere with retinal evaluation or confound DR ascertainment, such as retinal vein occlusion, retinal detachment, advanced glaucoma, macular degeneration, or other clinically significant retinal disorders. They had severe systemic disease likely to compromise the completeness of follow-up or the validity of outcome ascertainment, such as active malignancy, end-stage renal disease, or severe hepatic failure. Key exposure, outcome, or covariate data were missing and could not be resolved through source-record review. No valid follow-up fundus examination was available after baseline, making incident DR ascertainment impossible. The medical record contained major temporal inconsistencies or implausible sequences that could not be reconciled, such as an outcome-related examination predating the documented diabetes diagnosis without a reasonable clinical explanation.
Study procedures
Data sources and medical record retrieval
All data were obtained from the electronic medical record system and diabetic complication follow-up database of Pu'er People's Hospital. After ethics approval, medical records generated within the study window (January 1, 2023 – June 30, 2025) were retrospectively retrieved. Case screening was based on existing diagnostic information, examination records, and follow-up data in the electronic records, with no prospective data collection or additional surveys. All potentially eligible patients were consecutively screened in order of diagnosis date. A standardized data extraction template was used to systematically collate structured data and key unstructured text information from the medical records, ensuring consistency across cases.
Review of diabetes diagnosis and determination of onset time
Diabetes classification was confirmed by retrospectively reviewing diagnosis records, laboratory results, and discharge summaries in the electronic medical records. Only cases explicitly documented as type 2 diabetes with a clear time stamp were used for analysis. The date of the first unequivocal recording of a type 2 diabetes diagnosis was defined as the diabetes onset date. If multiple relevant diagnostic records existed for a patient, the earliest date with a clear diagnostic statement was selected as the diagnosis date. This date served as the uniform follow-up start point (time zero) to ensure accuracy of temporal sequence in the retrospective time-to-event analysis.
Extraction of smoking history and exposure grouping
Smoking history information was obtained by retrospectively extracting data from outpatient and inpatient medical histories, as well as history-taking forms completed during follow-up. Researchers reviewed records regarding smoking status, lifetime cigarette consumption, daily cigarette consumption, smoking duration, and—when available—the timing of smoking in relation to the diabetes course. During data extraction, smoking exposure was first categorized according to medical record documentation. Participants with lifetime consumption of fewer than 100 cigarettes were classified as the ‘<100 cigarettes ever’ group; when the records explicitly stated that the participant had never smoked, they were additionally identifiable as ‘never smokers’ in descriptive analyses. Participants with a history of past or current regular smoking for at least 6 months were classified as regular smokers. For individuals with documented regular smoking, daily consumption and duration were extracted. Pack-years of smoking were calculated retrospectively as the product of packs smoked per day and years of smoking. In case of discrepancies across different records for the same patient, the record closest in time to the diabetes diagnosis date with the most complete information was prioritized. If uncertainty remained, the variable was marked as missing and handled according to prespecified rules. Operationally, smoking variables were used both categorically and continuously in subsequent analyses. Because the timing of smoking initiation or cessation relative to diabetes diagnosis was not uniformly or reliably recorded for all participants, the primary exposure definition captured long-term smoking history rather than a strictly time-updated smoking status during follow-up.
Review of Fundus examination data and determination of follow-up time
Fundus examination data were obtained by retrospectively retrieving ophthalmology examination reports and related diagnostic records. All fundus examination records for each participant during follow-up were systematically reviewed to extract examination dates and corresponding diagnostic conclusions. Fundus examinations were performed using non-mydriatic or mydriatic fundus photography, with interpretation and standardized diagnostic reporting conducted by qualified ophthalmologists. For each patient, the first fundus examination record showing a definitive DR diagnosis during follow-up was treated as the event date. For participants without DR during observation, follow-up was right-censored at the date of the last valid fundus examination, defined as the last ophthalmic assessment with interpretable results sufficient to determine the absence of DR. This process established the follow-up time interval for each participant for subsequent time-to-event analysis.
Data consistency verification and temporal logic check
To minimize potential information bias and temporal misalignment in this retrospective study, key time points—including diabetes diagnosis date, smoking history recording date, and fundus examination dates—were checked for consistency during data preparation. Cases with implausible temporal sequences (e.g., a fundus examination date preceding the diabetes diagnosis date without logical clinical explanation) underwent further review of original records. Cases that could not be reasonably reconciled were excluded. All data cleaning and verification procedures were completed prior to analysis, with relevant rules predefined before study initiation.
Outcomes and exposures
Primary outcome: occurrence and timing of diabetic retinopathy
The primary outcome was the incidence of diabetic retinopathy (DR) after diabetes diagnosis. An outcome event was defined as the first unequivocal diagnosis of DR during follow-up. The time to event was defined as the interval (in months) from the date of type 2 diabetes diagnosis to the date of first definite DR diagnosis, used in time-to-event analyses. DR ascertainment was based on prior clinical fundus examination reports and diagnostic records. Only cases where an ophthalmologist explicitly documented “diabetic retinopathy” in a formal examination report or diagnostic conclusion were considered an outcome event. Descriptions such as “suspected,” “to be ruled out,” or unspecified diagnoses were not treated as events.
Secondary outcome: early-onset diabetic retinopathy
Building on the primary outcome, an earlier-occurring DR phenotype was defined as a secondary outcome. Because follow-up duration was not uniform and did not extend to a common fixed 5-year horizon for all participants, this outcome was operationalized within the observed follow-up window rather than as a conventional fixed-time cumulative incidence endpoint. Specifically, among participants who developed incident DR, event times (defined as months from diabetes diagnosis to the first definite DR diagnosis) were ranked, and DR events occurring at or before the prespecified cohort-specific cutoff for the earlier event-time distribution were classified as ‘earlier-occurring DR during follow-up’, whereas later events were classified as later-occurring DR. Participants without DR remained censored and did not contribute an event to this secondary endpoint. Thus, this secondary outcome was analyzed in a time-to-event framework as a relatively earlier event subtype within the available observation window, intended to distinguish faster- from slower-occurring DR phenotypes under the constraints of retrospective follow-up.
Outcome grading: severity of diabetic retinopathy
For participants with complete fundus grading information, the severity of DR was further assessed. Grading followed internationally recognized classification standards or the hospital's unified DR grading protocol adopted in clinical practice. Categories included: no diabetic retinopathy, non-proliferative diabetic retinopathy (NPDR), and proliferative diabetic retinopathy (PDR). When more detailed NPDR gradings (e.g., mild, moderate, severe) were recorded in the medical chart, the original grading information was retained for supplementary analysis. If multiple fundus grading records existed for a patient, the grade at the time of first DR diagnosis was considered the initial grade. In cases of inconsistent grading across records, original fundus examination reports were reviewed for clarification; if ambiguity persisted, the case was excluded from grading analyses.
Outcome progression: phenotype of diabetic retinopathy progression
For patients who developed DR during follow-up, disease progression was further documented. DR progression was defined as a worsening of retinopathy severity after the initial DR diagnosis, such as progression from NPDR to PDR or to a more advanced documented grade within NPDR when such grading detail was available. For the progression analysis, the analytic population was restricted to participants with incident DR and at least one ophthalmic assessment after the initial DR diagnosis. Time zero for this post-onset analysis was defined as the date of the first definite DR diagnosis. Progression time was calculated in months from the first DR diagnosis to the first subsequent examination documenting worsening of grade. Participants without documented progression were right-censored at the last ophthalmic assessment available after DR onset, death, or the study cut-off date, whichever occurred first. The association between smoking exposure and progression risk was then estimated using Cox proportional hazards models, with hazard ratios interpreted as the relative rate of grade worsening after DR onset.
Primary exposure: smoking Status and cumulative exposure level
The primary exposure was smoking history. For the primary binary analysis, smoking exposure was classified based on medical record documentation as ‘<100 cigarettes ever’ versus ‘regular smokers’. The ‘<100 cigarettes ever’ group referred to participants with lifetime consumption of fewer than 100 cigarettes; when the records explicitly indicated no smoking at all, these participants were considered true ‘never smokers’ in descriptive reporting where appropriate. Regular smokers were defined as participants with a history of past or current regular smoking lasting at least 6 months. To quantify the long-term cumulative effect of smoking, smoking exposure level was further assessed using pack-years. Pack-years were calculated as the product of packs smoked per day and years of smoking and used as a continuous variable in dose-response analyses. Based on prior literature and the sample distribution, cumulative smoking exposure was also categorized as 0 pack-years, ≤10 pack-years, and >10 pack-years for stratified analyses assessing outcome risk across different exposure levels. Because smoking timing relative to diabetes diagnosis was not consistently available in the retrospective records, the exposure variable should be interpreted as reflecting accumulated smoking history that may have occurred before diagnosis, after diagnosis, or across both periods.
Structured exposure–outcome metric: smoking exposure and disease aggressiveness features
To comprehensively evaluate the relationship between smoking exposure and the aggressiveness of diabetic retinopathy, a structured metric integrating cumulative smoking exposure level, timing of DR onset, and severity grade was constructed. By jointly considering pack-years, time to DR onset, and grading results, this metric captured the association between smoking exposure and early disease progression characteristics, used in subsequent multivariable modeling.
Statistical analysis
All statistical analyses were performed according to a prespecified analysis plan. Data cleaning, statistical modeling, and visualization were primarily conducted in the R software environment (version 4.3.2; R Foundation for Statistical Computing, Vienna, Austria). Some descriptive statistics and consistency checks were performed using Stata software (version 17.0; StataCorp LLC, College Station, TX, USA). Time-to-event analyses relied mainly on the survival package in R, restricted cubic spline modeling used the rms package, and propensity score-related analyses used the WeightIt, cobalt, and MatchIt packages where applicable. For all time-to-event analyses, time was measured in months because the underlying clinical records documented diagnosis and ophthalmic examination dates at calendar-date resolution and because months provided a clinically interpretable unit for diabetes complication follow-up. Event times were calculated from the diagnosis date to the corresponding event or censoring date and converted to elapsed months using the actual calendar interval.
Baseline characteristics of the study population were described according to the primary smoking exposure grouping (<100 cigarettes ever vs regular smokers) and cumulative smoking exposure level. Continuous variables were presented as mean ± standard deviation or median (interquartile range) based on their distribution; categorical variables were summarized as frequencies and percentages. Differences in baseline characteristics between smoking groups were primarily assessed using standardized mean differences (SMD), rather than relying solely on hypothesis testing. In the unweighted baseline comparison, SMD values were used descriptively to identify imbalance between exposure groups, with values ≥0.10 indicating potentially meaningful between-group differences. Covariate balance after propensity score weighting was evaluated separately, and SMD values <0.10 in the weighted sample were considered indicative of adequate balance. Baseline glucose-lowering therapy was coded as a three-level categorical variable: oral antidiabetic agents only, insulin only, and insulin plus oral antidiabetic agents. Covariates considered for adjustment were selected a priori based on clinical relevance, prior literature on DR risk, and their potential role as confounders of the smoking–DR association. The core adjustment set included age, sex, body mass index, HbA1c, hypertension, dyslipidemia, and chronic kidney disease. These variables were chosen because they could plausibly be associated with both smoking exposure and retinopathy risk and were measured with acceptable completeness in the medical records.
Cox proportional hazards models were used to evaluate the association between smoking exposure and the risk of developing DR after diabetes diagnosis. The primary time scale was elapsed time in months from the date of type 2 diabetes diagnosis to the first definite DR diagnosis, end of follow-up, or study cut-off date, whichever occurred first. Results were expressed as hazard ratios (HR) with 95% confidence intervals. Sequential multivariable models were prespecified to show the stability of the exposure effect under increasing confounder control: Model 1 was unadjusted; Model 2 adjusted for age and sex; Model 3 additionally adjusted for body mass index and HbA1c; and Model 4 further adjusted for hypertension, dyslipidemia, and chronic kidney disease. This staged approach was used to distinguish crude association, demographic adjustment, metabolic-risk adjustment, and fuller clinical confounder adjustment. The proportional hazards assumption was tested using Schoenfeld residuals. If violation was detected, time-dependent interaction terms or stratified Cox models were to be considered.
For the secondary outcome of earlier-occurring DR during follow-up, a time-to-event analytical framework was applied within the available observation window using the same underlying time scale in months from diabetes diagnosis. Kaplan–Meier methods were used to compare the accumulation of earlier-occurring DR events across smoking exposure groups, and differences between curves were assessed using the log-rank test. Cox proportional hazards models were then fitted to estimate the association between smoking exposure and the hazard of earlier-occurring DR during follow-up, with censoring handled as in the primary analysis. The same sequential covariate-adjustment strategy used for the primary DR outcome was applied to this secondary endpoint so that estimates would remain comparable across models.
To assess the dose-response relationship between cumulative smoking exposure and DR risk during the observed follow-up period, pack-years were included as a continuous variable in Cox proportional hazards models, with potential nonlinear effects modeled using restricted cubic spline (RCS) functions. Knot placement was prespecified at the 5th, 35th, and 65th percentiles of the pack-year distribution, with 0 pack-years as the reference value. The nonlinear component was evaluated using a Wald-type test of nonlinearity. This approach was chosen to allow flexible modeling of cumulative smoking burden without imposing a strictly linear exposure–response assumption.
Among participants with DR grading information, further analyses focused on severity. The cross-sectional distribution of DR severity grades at first DR diagnosis across smoking exposure levels was compared using ordinal or multinomial outcome regression, depending on the granularity of the available grading categories. For patients who developed DR, a separate post-onset progression analysis was performed. In this progression analysis, time zero was defined as the date of the first definite DR diagnosis, and follow-up continued until the first record of grade worsening, the last ophthalmic assessment available after DR onset, death, or the study cut-off date, whichever occurred first. Cox proportional hazards models were used to estimate the hazard of progression after DR onset, with smoking exposure as the primary explanatory variable and adjustment performed using the same core confounder set as in the main models. Results were reported as HR and 95% CI.
Given the non-random assignment of exposure groups in retrospective cohort studies, propensity score methods were introduced as a supplementary confounding control strategy alongside the primary multivariable models. The propensity score for being classified as a regular smoker was estimated using logistic regression including age, sex, body mass index, HbA1c, hypertension, dyslipidemia, chronic kidney disease, family history of diabetes, current alcohol consumption, and baseline glucose-lowering treatment. The primary weighting approach was inverse probability of treatment weighting (IPTW) using stabilized weights. Balance before and after weighting was assessed by SMDs, with values <0.10 considered indicative of adequate balance in the weighted sample. Weighted Cox proportional hazards models with robust variance estimation were then fitted for the primary outcome. In addition, prespecified subgroup or stratified analyses were conducted for selected clinically relevant characteristics, including age category, baseline HbA1c level, hypertension, and chronic kidney disease status, to examine whether the association was directionally consistent across strata; these analyses were considered exploratory and were not used to redefine the main effect estimate.
To examine the robustness of primary findings, several prespecified sensitivity analyses were conducted. These included repeating the main models using a stricter exposure definition (current smokers only), excluding patients who developed DR within 12 months after diabetes diagnosis to reduce potential reverse-causation or diagnostic-timing bias, and restricting analyses to participants with more intensive ophthalmic follow-up (≥3 fundus examinations). Results of each sensitivity analysis were compared with those of the primary analysis in terms of direction, magnitude, and statistical precision of the smoking effect estimate.
All statistical tests were two-sided, with a P-value <0.05 considered statistically significant. Effect estimates are reported alongside their 95% confidence intervals to convey both statistical significance and the uncertainty of the estimates.
Because residual confounding remains a key concern in observational studies, we additionally calculated E-values for the fully adjusted hazard ratios of the primary outcome and the secondary earlier-occurring DR outcome. The E-value quantifies the minimum strength of association that an unmeasured confounder would need to have with both the exposure and the outcome, on the risk-ratio scale, conditional on the measured covariates, to fully explain away the observed association. E-values were calculated for both the point estimate and the lower bound of the 95% confidence interval closest to the null. Larger E-values indicate that stronger unmeasured confounding would be required to negate the observed association.
Results
Study population and baseline characteristics
During the study period (January 1, 2023, to June 30, 2025), a retrospective search of the hospital electronic medical record system identified 642 patients with a first-time recorded diagnosis of type 2 diabetes. After applying the prespecified inclusion and exclusion criteria, 488 young-onset type 2 diabetes patients remained in the final analytic cohort. All included patients had a baseline DR-free fundus examination and at least one valid follow-up fundus examination during follow-up.
The median follow-up time was 32.4 months (interquartile range [IQR]: 21.6–44.8 months), indicating that follow-up duration was sufficient for incident-event analysis during the available observation period but did not uniformly permit formal estimation of a 5-year event risk for all participants. Of the included patients, 208 (42.6%) were classified as regular smokers and 280 (57.4%) belonged to the <100 cigarettes ever group. When explicitly identifiable from the records, true never smokers were nested within the latter category. Compared with the <100 cigarettes ever group, regular smokers had a higher proportion of males and higher levels of several metabolic and cardiovascular risk indicators, including body mass index, waist circumference, HbA1c, fasting plasma glucose, blood pressure, triglycerides, and current alcohol consumption.
Overall, the unweighted baseline characteristics were not fully balanced between the smoking groups. Several variables showed meaningful between-group differences, including sex (SMD 0.46), body mass index (SMD 0.31), waist circumference (SMD 0.41), HbA1c (SMD 0.46), fasting plasma glucose (SMD 0.38), systolic blood pressure (SMD 0.35), diastolic blood pressure (SMD 0.33), LDL cholesterol (SMD 0.36), HDL cholesterol (SMD 0.41), triglycerides (SMD 0.32), and current alcohol consumption (SMD 0.37), indicating appreciable confounding by baseline characteristics before weighting. The unweighted baseline characteristics were not fully balanced between groups, as shown in Table 1. Baseline glucose-lowering treatment patterns also differed modestly between groups (overall treatment-category SMD 0.18), with regular smokers more frequently receiving insulin-only therapy at baseline. The cohort derivation and the primary analytic framework are summarized in the revised Figure 1.
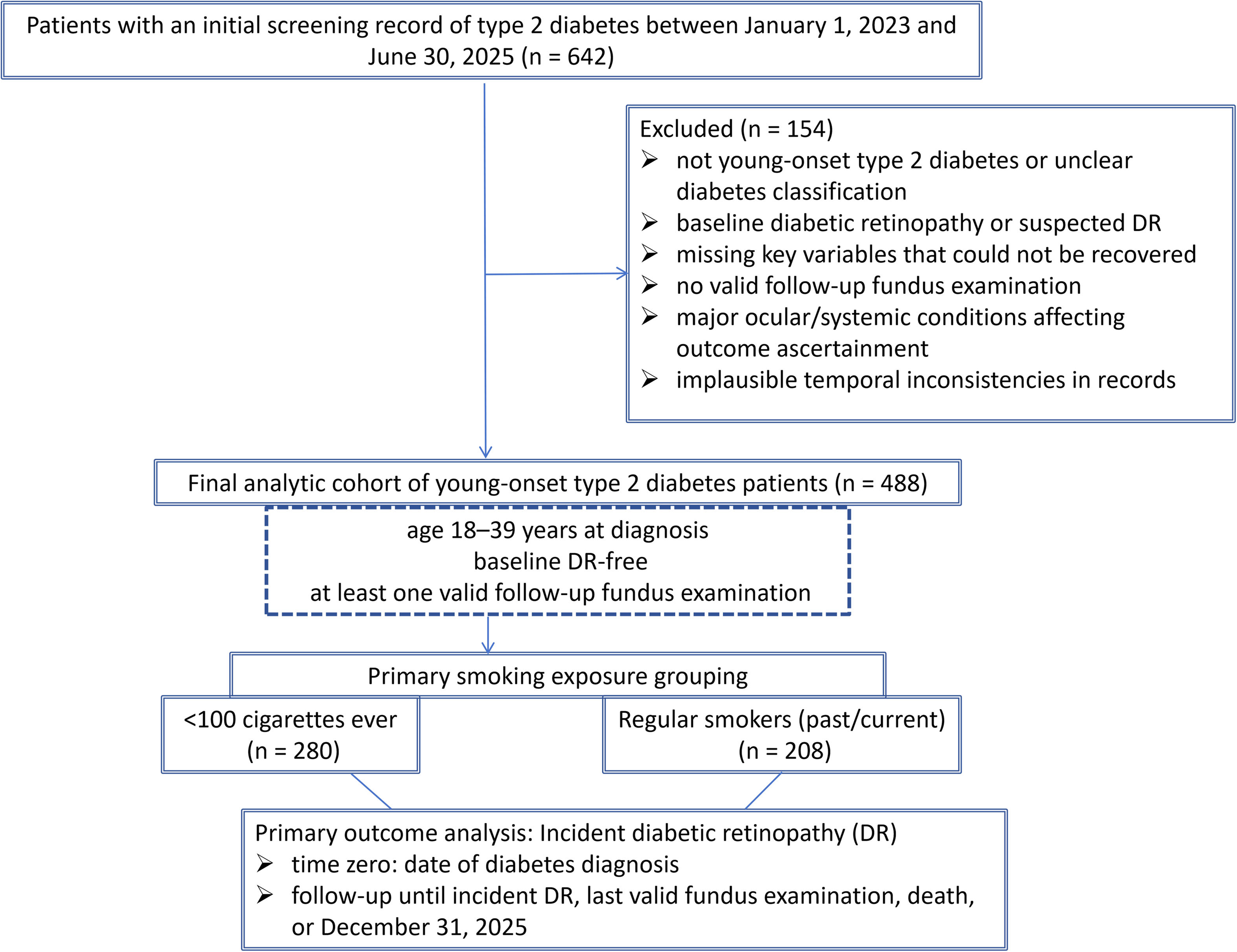
Cohort selection and primary analytical framework. The figure shows screening from 642 initially identified patients to the final analytic cohort of 488 young-onset type 2 diabetes patients, followed by the primary smoking exposure grouping used in the main analyses (<100 cigarettes ever vs regular smokers). Secondary dose-stratified and post-onset analyses are not displayed in the flowchart.
Unweighted baseline characteristics of the study population according to smoking exposure group.
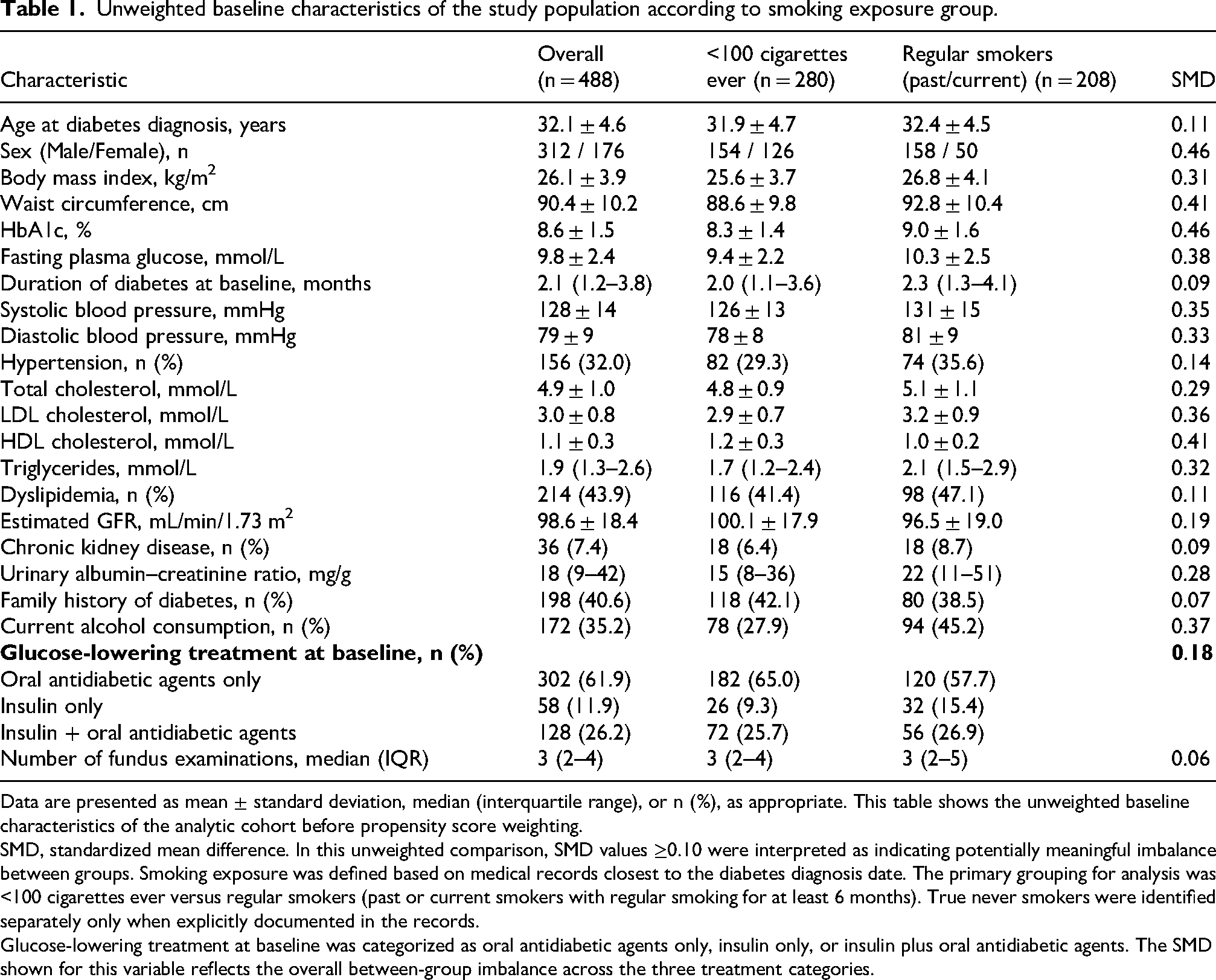
Data are presented as mean ± standard deviation, median (interquartile range), or n (%), as appropriate. This table shows the unweighted baseline characteristics of the analytic cohort before propensity score weighting.
SMD, standardized mean difference. In this unweighted comparison, SMD values ≥0.10 were interpreted as indicating potentially meaningful imbalance between groups. Smoking exposure was defined based on medical records closest to the diabetes diagnosis date. The primary grouping for analysis was <100 cigarettes ever versus regular smokers (past or current smokers with regular smoking for at least 6 months). True never smokers were identified separately only when explicitly documented in the records.
Glucose-lowering treatment at baseline was categorized as oral antidiabetic agents only, insulin only, or insulin plus oral antidiabetic agents. The SMD shown for this variable reflects the overall between-group imbalance across the three treatment categories.
Association between smoking exposure and risk of diabetic retinopathy.
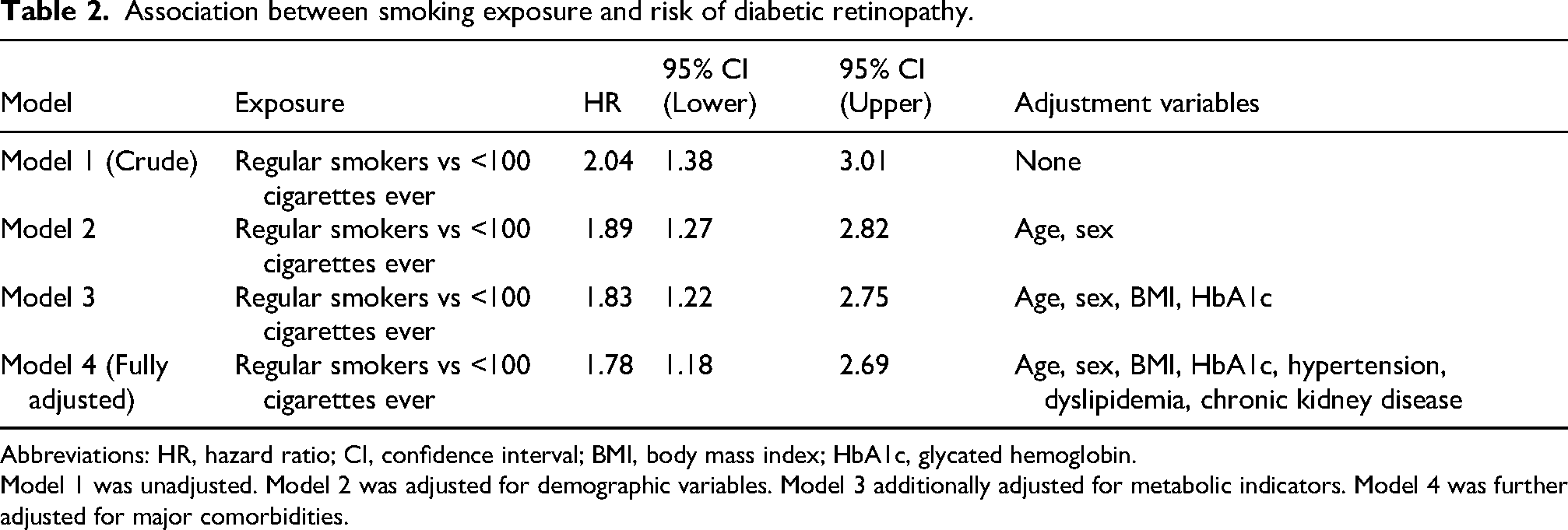
Abbreviations: HR, hazard ratio; CI, confidence interval; BMI, body mass index; HbA1c, glycated hemoglobin.
Model 1 was unadjusted. Model 2 was adjusted for demographic variables. Model 3 additionally adjusted for metabolic indicators. Model 4 was further adjusted for major comorbidities.
Smoking and the incidence/temporal pattern of diabetic retinopathy
During the median follow-up of 32.4 months (IQR: 21.6–44.8 months), 92 patients were newly diagnosed with diabetic retinopathy, representing an overall incidence of 18.9%. Among these, DR occurred in 41 (14.6%) participants in the <100 cigarettes ever group and 51 (24.5%) regular smokers. The median time to DR onset was 28.7 months after the diabetes diagnosis.
Kaplan–Meier analysis revealed significant differences in the cumulative incidence of DR between smoking exposure groups (Figure 2). Throughout follow-up, regular smokers consistently exhibited a higher cumulative risk of DR than participants in the <100 cigarettes ever group, with the survival curves separating relatively early after cohort entry. The log-rank test indicated a statistically significant between-group difference (χ2 = 10.34, P = 0.0013; Figure 2).
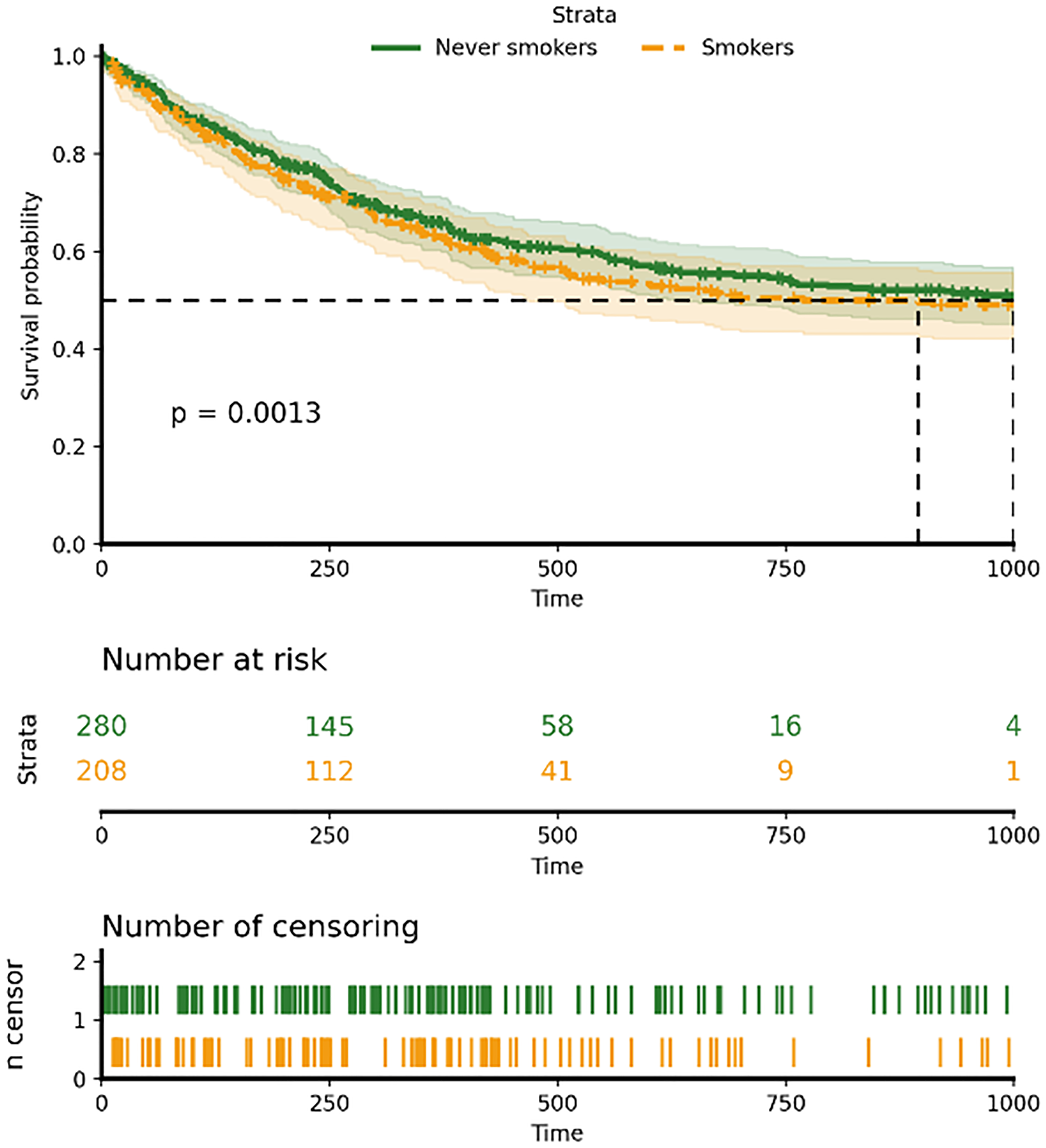
Kaplan–Meier curves for the primary outcome of incident diabetic retinopathy in the full analytic cohort according to the primary smoking exposure grouping (<100 cigarettes ever vs regular smokers). The event of interest was the first definite DR diagnosis after diabetes diagnosis, and time was measured in months from cohort entry.
In Cox proportional hazards models, smoking exposure was significantly associated with an increased risk of DR. The unadjusted model showed that regular smokers had a significantly higher risk of developing DR compared with the <100 cigarettes ever group (hazard ratio [HR] = 2.04, 95% confidence interval [CI]: 1.38–3.01), indicating a strong association in the crude analysis (Table 2).
This association remained materially unchanged after adjusting for potential confounders. Sequential adjustments for demographic characteristics (age, sex), metabolic indicators (body mass index, HbA1c), and major comorbidities yielded stable results, with only a slight attenuation of the effect size, suggesting that the association was not fully explained by these factors (Table 2).
In the fully adjusted model, after controlling for demographic features, metabolic status, and major comorbidities, regular smokers had a 78% higher risk of developing DR compared with the <100 cigarettes ever group (HR = 1.78, 95% CI: 1.18–2.69). These results indicate that smoking exposure is independently associated with DR incidence in young-onset type 2 diabetes patients, and this association remained statistically significant after multivariable adjustment. The proportional hazards assumption was not violated, as assessed by Schoenfeld residuals (global test P = 0.64) (Table 2).
Smoking and earlier-occurring diabetic retinopathy during follow-up
Among the 92 patients who developed DR during follow-up, 61 (66.3%) were classified as having earlier-occurring DR according to the revised outcome definition based on the available observation window. The proportion of participants classified as having earlier-occurring DR in the entire cohort was 12.5% (61/488). Earlier-occurring DR during follow-up was more common among regular smokers. Among patients who developed DR, the proportion classified as having earlier-occurring disease during follow-up was 73.8% in regular smokers versus 58.2% in the <100 cigarettes ever group, suggesting an association between smoking exposure and earlier disease occurrence (χ2 = 6.84, P = 0.009).
In the time-to-event analysis of earlier-occurring DR during the available follow-up period, regular smokers consistently showed a higher event accumulation than participants in the <100 cigarettes ever group. The between-group difference was statistically significant in the log-rank comparison (P = 0.006).
In multivariable Cox models, smoking exposure was significantly associated with an increased risk of earlier-occurring DR during follow-up. In the unadjusted model, regular smokers had a significantly higher risk than participants in the <100 cigarettes ever group (Table 3). This association remained stable after sequential adjustment for age, sex, body mass index, HbA1c, and major comorbidities (Table 3). In the fully adjusted model, regular smokers had a 92% higher risk of earlier-occurring DR during follow-up compared with the <100 cigarettes ever group (HR = 1.92, 95% CI: 1.21–3.05, Table 3), indicating that smoking exposure is associated not only with overall DR risk but also with earlier disease occurrence after diabetes diagnosis.
Multivariable cox proportional hazards models for the association between smoking exposure and earlier-occurring diabetic retinopathy during follow-up in the full analytic cohort.
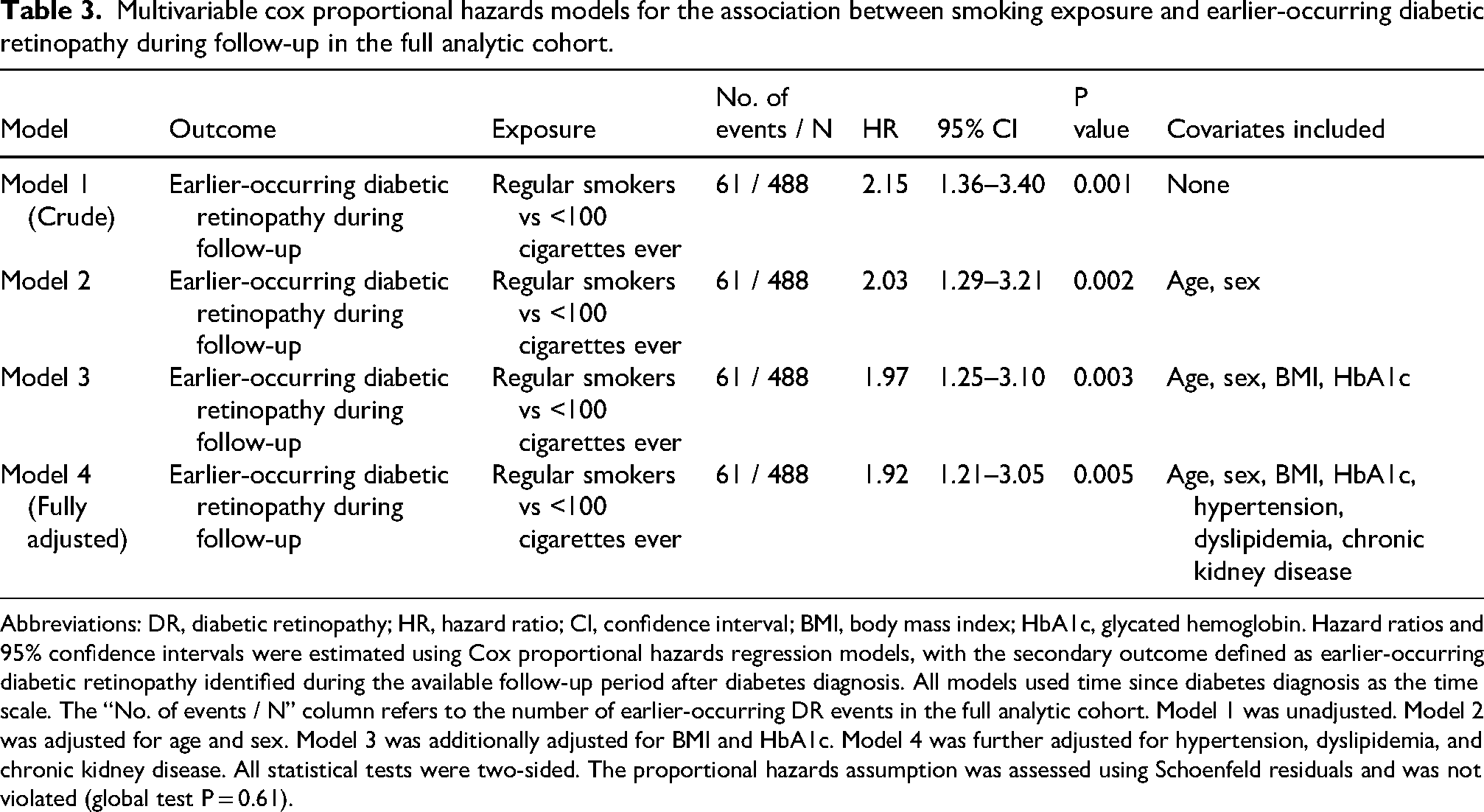
Abbreviations: DR, diabetic retinopathy; HR, hazard ratio; CI, confidence interval; BMI, body mass index; HbA1c, glycated hemoglobin. Hazard ratios and 95% confidence intervals were estimated using Cox proportional hazards regression models, with the secondary outcome defined as earlier-occurring diabetic retinopathy identified during the available follow-up period after diabetes diagnosis. All models used time since diabetes diagnosis as the time scale. The “No. of events / N” column refers to the number of earlier-occurring DR events in the full analytic cohort. Model 1 was unadjusted. Model 2 was adjusted for age and sex. Model 3 was additionally adjusted for BMI and HbA1c. Model 4 was further adjusted for hypertension, dyslipidemia, and chronic kidney disease. All statistical tests were two-sided. The proportional hazards assumption was assessed using Schoenfeld residuals and was not violated (global test P = 0.61).
Dose–response relationship between cumulative smoking exposure and DR risk
To further examine whether cumulative smoking burden provided information beyond the binary smoking grouping, dose–response analyses were performed using pack-years as both a categorized and continuous exposure metric. Stratified results according to cumulative smoking exposure are summarized in Table 4, and the continuous nonlinear association between pack-years and DR risk is shown in Figure 3.
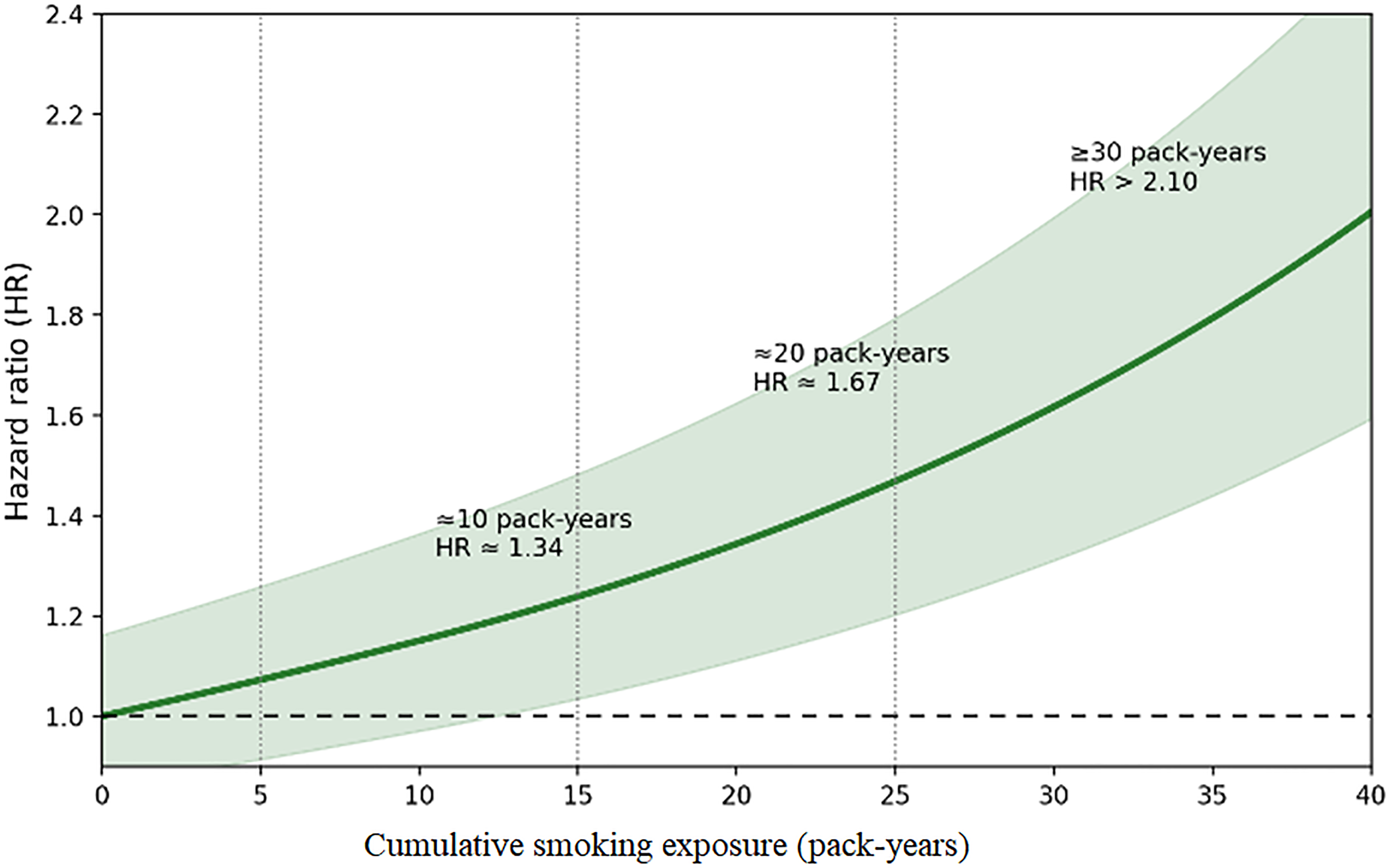
Restricted cubic spline analysis of cumulative smoking exposure and the risk of incident diabetic retinopathy. Pack-years were modeled as a continuous exposure in the multivariable Cox model, with 0 pack-years as the reference. Time was measured in months from diabetes diagnosis.
Diabetic retinopathy severity distribution and categorized cumulative smoking exposure among participants who developed incident diabetic retinopathy.
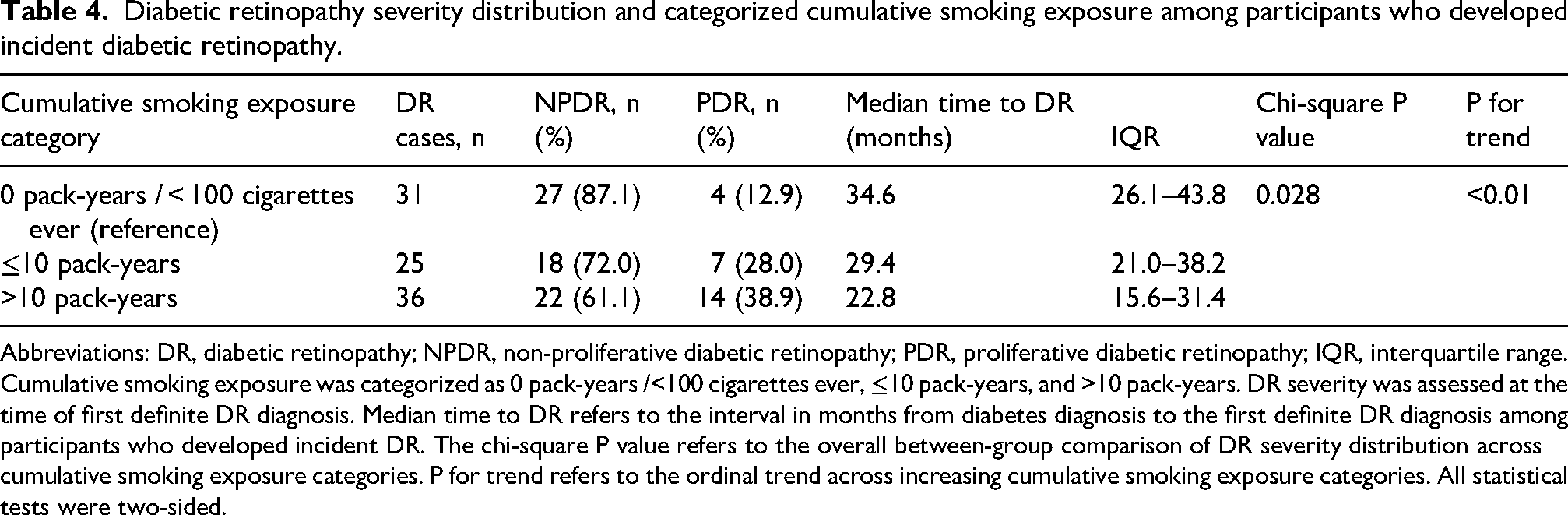
Abbreviations: DR, diabetic retinopathy; NPDR, non-proliferative diabetic retinopathy; PDR, proliferative diabetic retinopathy; IQR, interquartile range. Cumulative smoking exposure was categorized as 0 pack-years /<100 cigarettes ever, ≤10 pack-years, and >10 pack-years. DR severity was assessed at the time of first definite DR diagnosis. Median time to DR refers to the interval in months from diabetes diagnosis to the first definite DR diagnosis among participants who developed incident DR. The chi-square P value refers to the overall between-group comparison of DR severity distribution across cumulative smoking exposure categories. P for trend refers to the ordinal trend across increasing cumulative smoking exposure categories. All statistical tests were two-sided.
To systematically evaluate the dose–response relationship, smoking pack-years were included as a continuous variable in a RCS model based on the multivariable Cox framework. Knots were placed at the 5th, 35th, and 65th percentiles of pack-year distribution, with the 0 pack-year group as the reference. The analysis revealed a significant nonlinear relationship between pack-years and DR risk (nonlinear trend test P = 0.018, Figure 3). At lower exposure levels (≤5 pack-years), the increase in DR risk was modest and not significantly different from the reference. The risk curve began to rise noticeably around 10 pack-years. Compared with the 0 pack-year reference group, the hazard ratio was approximately 1.34 at 10 pack-years, further increased at 20 pack-years (HR ≈ 1.67), and exhibited a steeper rise at 30 pack-years and above, with HRs exceeding 2.10. These findings were directionally consistent with the categorized comparisons shown in Table 4.
After adjustment for age, sex, body mass index, HbA1c, and major comorbidities, this dose-response relationship persisted, indicating that the effect of cumulative smoking exposure on DR risk is dose-dependent and not fully explained by demographic or metabolic factors.
Severity grading and progression of diabetic retinopathy
Among the 92 patients who developed DR, 67 (72.8%) were diagnosed with non-proliferative DR (NPDR) and 25 (27.2%) with proliferative DR (PDR) (Table 4). The distribution of DR severity differed markedly between smoking exposure groups. Among regular smokers, the proportion of PDR was 34.4% (21/61), significantly higher than the 12.9% (4/31) observed in the 0 pack-year /<100 cigarettes ever reference group (P = 0.028, Table 4). In an ordinal trend analysis, smoking exposure was significantly positively associated with DR severity. The probability of being diagnosed with a higher severity grade increased with greater smoking exposure (P for trend < 0.01, Table 4).
After the initial diagnosis of DR, progression analyses were performed in the post-onset risk set consisting of participants with incident DR and at least one ophthalmic assessment after DR diagnosis. Within this risk set, 29 patients experienced subsequent DR grade progression, including 22 in regular smokers and 7 in the <100 cigarettes ever group. Using the first record of grade worsening after DR onset as the progression event, time-to-event analysis assessed the risk of progression. Results showed that regular smokers had a significantly increased risk of progressing from a lower to a higher DR grade compared with the <100 cigarettes ever group. This association remained stable after adjusting for age, sex, body mass index, HbA1c, and major comorbidities. In the fully adjusted Cox model, regular smokers had an 87% higher risk of DR grade progression after initial DR diagnosis (HR = 1.87, 95% CI: 1.02–3.41).
Robustness analyses
To further assess the robustness of the primary findings, inverse probability of treatment weighting (IPTW) was used to address the baseline imbalances observed in the unweighted cohort. After weighting, the SMDs for all included covariates were substantially reduced to <0.10, indicating good balance between the weighted groups (Table 5).
IPTW-weighted and sensitivity analyses for the association between smoking exposure and incident diabetic retinopathy.
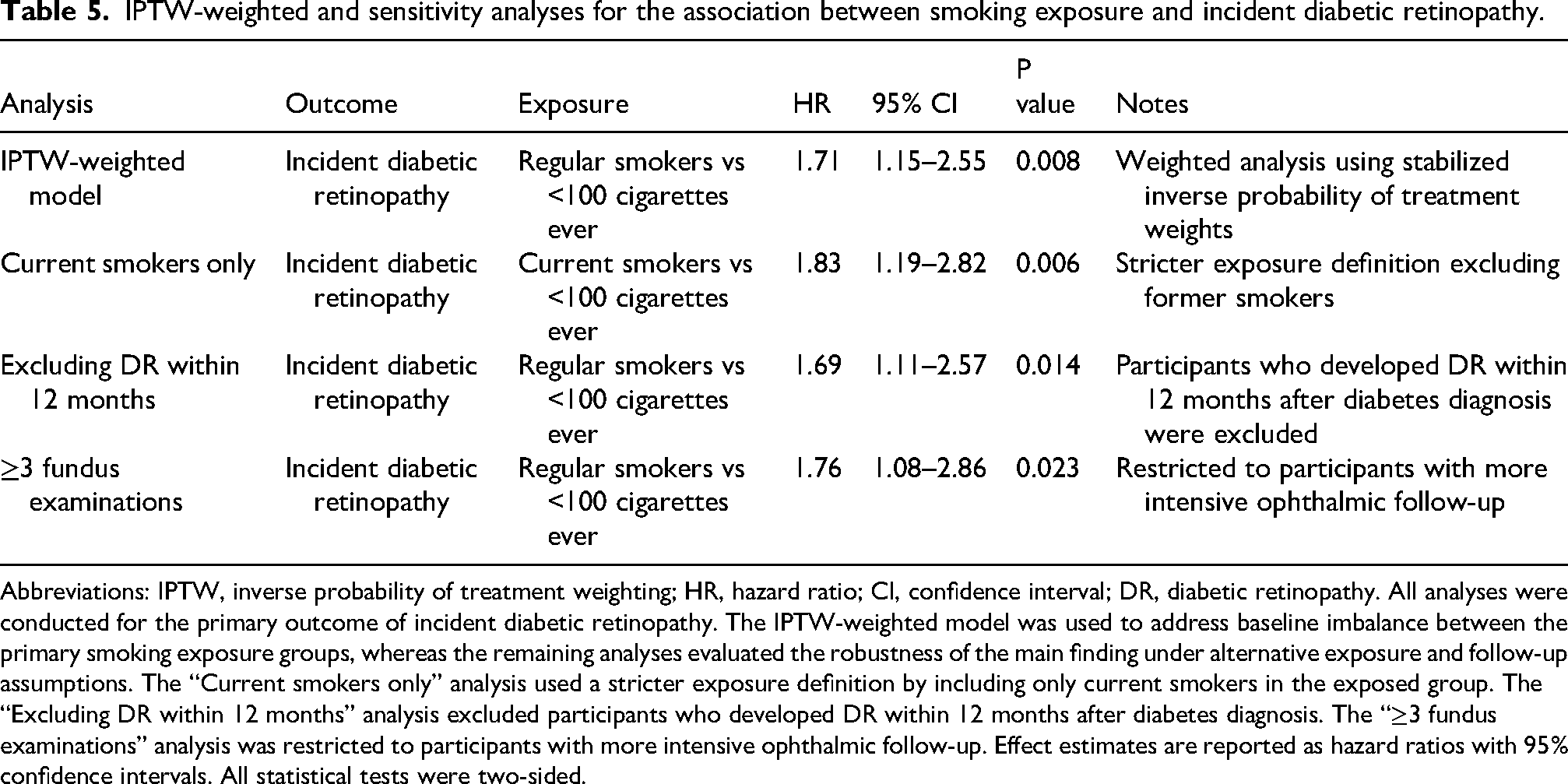
Abbreviations: IPTW, inverse probability of treatment weighting; HR, hazard ratio; CI, confidence interval; DR, diabetic retinopathy. All analyses were conducted for the primary outcome of incident diabetic retinopathy. The IPTW-weighted model was used to address baseline imbalance between the primary smoking exposure groups, whereas the remaining analyses evaluated the robustness of the main finding under alternative exposure and follow-up assumptions. The “Current smokers only” analysis used a stricter exposure definition by including only current smokers in the exposed group. The “Excluding DR within 12 months” analysis excluded participants who developed DR within 12 months after diabetes diagnosis. The “≥3 fundus examinations” analysis was restricted to participants with more intensive ophthalmic follow-up. Effect estimates are reported as hazard ratios with 95% confidence intervals. All statistical tests were two-sided.
In the IPTW-weighted Cox model, the association between smoking exposure and DR risk remained significant. Compared with the <100 cigarettes ever group, regular smokers had an approximately 70% higher risk of DR (HR = 1.71, 95% CI: 1.15–2.55, Figure 4, Table 5), an effect size highly consistent in direction and magnitude with the primary multivariable model. Figure 4 summarizes the primary and sensitivity-effect estimates to facilitate direct comparison of robustness across analytic scenarios.
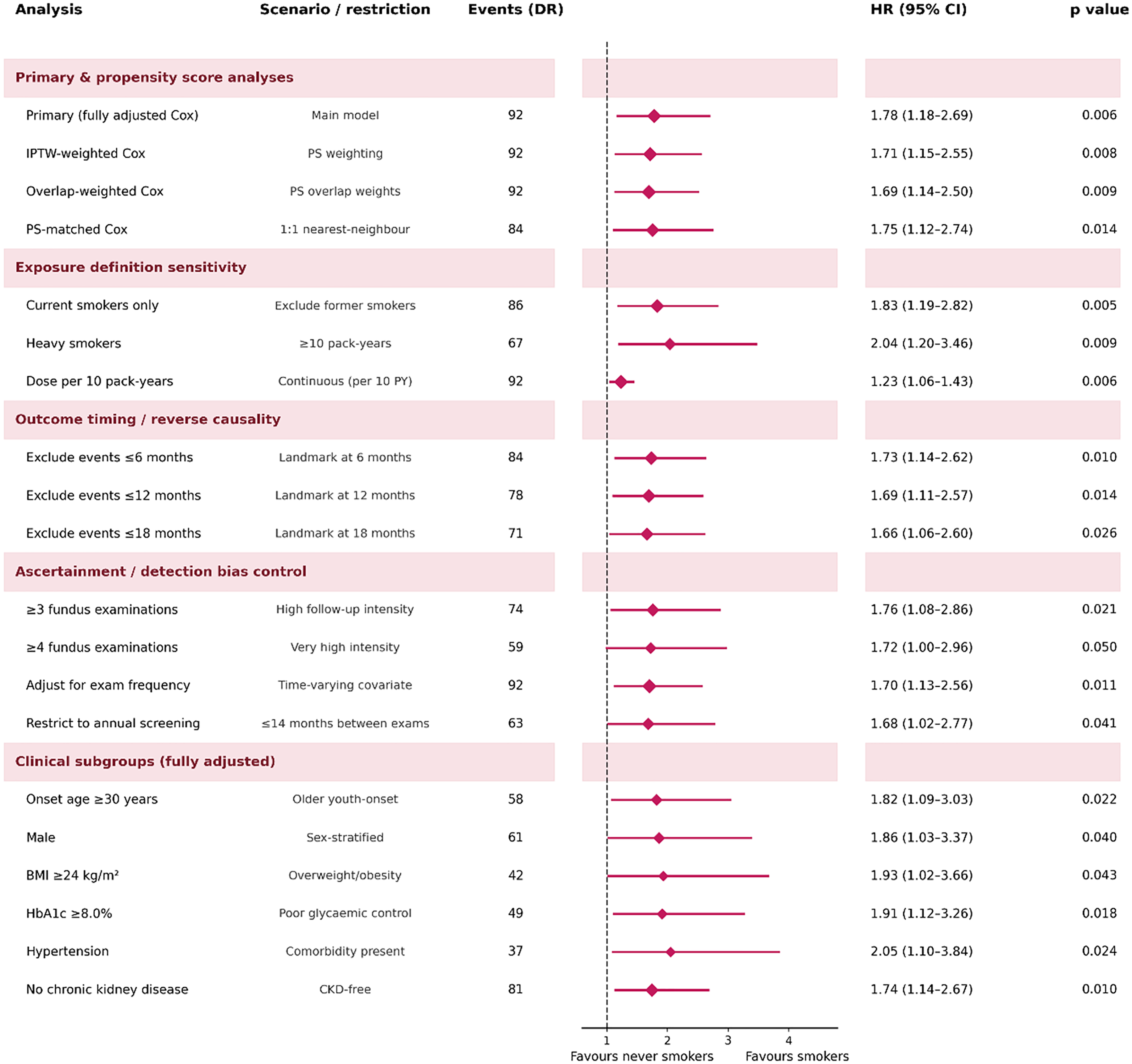
Forest plot summarizing the association between smoking exposure and incident diabetic retinopathy across the primary multivariable model, IPTW-weighted model, and prespecified sensitivity analyses. Effect estimates are shown as hazard ratios with 95% confidence intervals.
Several sensitivity analyses evaluated the dependence of conclusions on different assumptions. First, using a stricter exposure definition (including only current smokers, excluding former smokers) still yielded a significant association (HR = 1.83, 95% CI: 1.19–2.82, Table 5). Second, excluding patients who developed DR within 12 months of diabetes diagnosis did not materially alter the results (HR = 1.69, 95% CI: 1.11–2.57, Table 5). Third, restricting the analysis to patients with ≥3 fundus examinations during follow-up also showed a stable association (HR = 1.76, 95% CI: 1.08–2.86, Table 5).
Overall, the association between smoking exposure and DR risk remained consistent in direction and statistically significant across propensity score-weighted analyses and various sensitivity scenarios, suggesting good robustness of the study findings. In addition, E-value analysis was performed to assess the potential impact of unmeasured confounding. For the fully adjusted primary DR model (HR 1.78, 95% CI 1.18–2.69), the E-value for the point estimate was 2.95 and the E-value for the lower confidence bound was 1.64. For the fully adjusted earlier-occurring DR model (HR 1.92, 95% CI 1.21–3.05), the corresponding E-values were 3.25 and 1.71, respectively. These values indicate that an unmeasured confounder would need to be associated with both smoking exposure and the DR outcomes by risk ratios of at least approximately 2.95 and 3.25, respectively, above and beyond the measured covariates, to fully explain away the observed point estimates.
Discussion
YOD is characterized by a long disease duration and significant metabolic abnormalities, often leading to multiple complications, among which DR is one of the most common and serious microvascular sequelae. Smoking can damage vascular endothelium, induce oxidative stress and inflammation, thereby exacerbating the progression of diabetic microvascular complications.21,22 Although smoking is recognized as an important risk factor for cardiovascular and renal complications, evidence regarding its role in early-onset DR within the YOD population has been lacking. This retrospective cohort study aimed to evaluate the association between long-term smoking history and the risk of DR, particularly earlier-occurring DR during follow-up, in young-onset type 2 diabetes patients, providing new observational evidence regarding a potentially modifiable exposure associated with complications in this specific group. In the present retrospective dataset, smoking exposure reflected accumulated smoking history documented around and during clinical care, which may have occurred before diabetes diagnosis, after diagnosis, or across both periods.
Our findings suggest that long-term smoking is associated with a higher hazard of earlier-occurring DR during the available follow-up period among young-onset type 2 diabetes patients compared with the reference group. This pattern suggests that smoking exposure may be related not only to DR occurrence but also to an earlier observed manifestation of microvascular disease in this population. This observation is biologically plausible. Smoking has been shown to impair the microvascular system through multiple pathways, including inducing sustained endothelial dysfunction, enhancing oxidative stress, promoting chronic low-grade inflammation, and accelerating capillary basement membrane thickening and microvascular occlusion. These processes reduce the compensatory capacity of the retinal microcirculation and trigger pathological changes earlier.23–26 In young-onset diabetes, due to an earlier onset and longer duration of metabolic disturbances, smoking-related damage may synergize with hyperglycemia and insulin resistance, pushing the microvascular system past its decompensation threshold sooner, manifesting as an earlier onset of DR. 27 This interpretation is also consistent with recent literature emphasizing that DR should be framed not only as an ophthalmic endpoint but also as a complication shaped by modifiable systemic exposures and by the opportunity for earlier identification of high-risk individuals before progression to vision-threatening stages.17–19
However, our results differ from some prior reports. For example, an analysis by Wang et al. (2019) using NHANES data found a negative association, even an apparent protective effect, between smoking and DR risk. 19 This discrepancy may be explained by methodological and population factors. Their cross-sectional design could not establish temporal sequence between smoking exposure and DR onset, and their findings might reflect survivor bias or behavioral changes (e.g., patients with existing retinopathy being more likely to quit, artificially inflating DR prevalence among non-smokers in a cross-sectional snapshot). While Mendelian randomization can reduce confounding, its assumptions are not always fully met for complex behavioral exposures like smoking, and the genetic instruments often reflect smoking initiation rather than cumulative exposure intensity—the focus of our study. Furthermore, earlier large prospective cohorts like WESDR and UKPDS did not observe a significant positive association between smoking and DR incidence in type 2 diabetes populations,28,29 but these studies primarily involved middle-aged or older-onset patients and focused on DR occurrence rather than its timing or early-onset phenotype. Our study, by focusing on young-onset patients and emphasizing the timing of DR occurrence within the available follow-up period, reframes the assessment of smoking's impact from both risk-structure and temporal perspectives. Collectively, inconsistencies in the literature regarding smoking and DR likely reflect differences in study populations, outcome definitions, and analytical frameworks rather than contradictory biological effects. Our findings suggest that in young-onset type 2 diabetes—a population with heightened microvascular vulnerability—long-term smoking may exert a more pronounced adverse effect on the timing of DR onset, offering new evidence for early risk stratification and behavioral intervention in this group.
Beyond establishing the association, our study systematically evaluated the dose-response relationship between cumulative smoking exposure and DR risk, moving beyond a simple binary exposure framework. The risk of DR showed a continuous upward trend with increasing pack-years, with a more pronounced rise at higher exposure levels. This pattern suggests that smoking may be better interpreted not merely as a present/absent exposure, but as a cumulative behavioral exposure associated with progressively greater microvascular risk. Epidemiologically, this supports the notion that smoking-induced damage to the retinal microcirculation is a long-term, progressive process, where repeated tobacco exposure gradually undermines vascular endothelial homeostasis through additive effects, eventually crossing a pathological threshold to manifest as clinically detectable retinopathy.21,30–33 Notably, this dose-response pattern aligns with prior evidence for other diabetic microvascular complications. For instance, research in type 2 diabetes has shown that individuals with 15–30 and >30 pack-years of smoking have significantly elevated risks of diabetic nephropathy-related proteinuria compared to non-smokers, with risk increasing in a graded manner with cumulative exposure. 34 That study underscores the importance of tobacco dose-response in diabetic microvascular injury. Integrating this evidence with our findings suggests that smoking's impact on the diabetic microvascular system is consistent across organs; its harm is not confined to a single complication but operates via cumulative mechanisms affecting high-perfusion microvascular beds like the kidneys and retina simultaneously. In young-onset type 2 diabetes, where the disease starts earlier, the prolonged exposure duration from long-term smoking may further amplify this dose-dependent effect, explaining why higher cumulative smoking is linked to earlier DR onset and greater risk. This result emphasizes that assessing diabetic complication risk based solely on smoking status may underestimate its true impact. Incorporating cumulative smoking exposure into risk stratification frameworks is crucial for identifying high-risk individuals and formulating more precise early intervention strategies.
In subgroup analyses, the association between long-term smoking and earlier DR occurrence during follow-up demonstrated high consistency across various population characteristics. Stratification by sex, hypertension status, or diabetes duration yielded risk estimates that were stable in direction and magnitude, with no statistically or clinically significant effect modification observed. This consistency carries important methodological and pathological implications. On one hand, it suggests that smoking's effect on early-onset DR is not merely amplified in a specific high-risk subgroup but likely represents a pervasive, cumulative hazardous exposure with a stable influence on microvascular outcomes in young-onset type 2 diabetes patients across populations. 35 On the other hand, such consistency reduces the likelihood that the results are driven by a single covariate or specific subgroup structural bias. 36 Statistically, we further employed propensity score weighting to construct a doubly robust model. After substantially improving the imbalance in baseline characteristics observed in the unweighted cohort, the association between smoking and early-onset DR risk remained materially unchanged 37 This finding indicates that the observed risk elevation persists even under an analytical framework approximating quasi-random assignment, supporting the notion that the association is not fully explained by measured confounders. Additionally, the observed E-values indicated that a relatively strong unmeasured confounder would be required to fully explain away the observed associations, especially for the point estimates of both the primary DR outcome and the earlier-occurring DR outcome. Given current clinical and epidemiological understanding, such strong confounders are unlikely to exist in reality. Considering the subgroup consistency, propensity score analysis, and E-value results together, the primary conclusion of this study—that long-term smoking increases the risk of earlier-occurring DR during follow-up in young-onset type 2 diabetes patients—appears robust and credible.
From a mechanistic perspective, the observed association between smoking and elevated earlier-occurring DR risk, together with the dose-response relationship with cumulative exposure, is biologically plausible and is broadly compatible with current concepts of diabetic retinal injury. 2 °Chronic smoking continuously exposes the body to abundant free radicals and toxic chemicals, markedly increasing systemic oxidative stress and activating chronic low-grade inflammation. This directly impairs retinal microvascular endothelial cell function, disrupts endothelial integrity, and increases capillary permeability—key early events in DR pathogenesis. 25 In young-onset type 2 diabetes, where hyperglycemia exposure starts earlier and lasts longer, smoking-induced oxidative stress and inflammation may synergize with metabolic abnormalities, accelerating the accumulation of microvascular damage. This could explain the earlier appearance of retinopathy among smokers in our study. Furthermore, smoking can upregulate vasoconstrictors like endothelin, reducing retinal microcirculatory perfusion and exacerbating local ischemia and hypoxia. 38 Retinal tissue is highly sensitive to hypoxia. Chronic hypoperfusion not only promotes endothelial dysfunction but can also trigger hypoxia-inducible factor-related signaling pathways, further driving aberrant angiogenesis and disease progression—consistent with our findings of higher proportions of severe grades and progression events among smokers. Simultaneously, nicotine and other harmful components in cigarettes can act directly on retinal pigment epithelial cells and capillary walls, inducing apoptosis, basement membrane thickening, and breakdown of the blood-retinal barrier, 39 thereby diminishing the retina's tolerance to metabolic and hemodynamic fluctuations. In this context, smoking is not merely a risk factor influencing whether DR occurs, but more likely a factor that persistently amplifies microvascular vulnerability, driving earlier disease onset and a faster progression trajectory. Although our retrospective design cannot directly validate these molecular pathways, the observed elevation in early-onset risk, clear dose-response relationship, and increased progression risk align logically with established mechanisms of smoking-related inflammation, oxidative stress, and microvascular injury from prior experimental and epidemiological studies, providing indirect support for the plausibility of an adverse association between smoking exposure and the development and progression of DR in young-onset type 2 diabetes, while not establishing causality.
As a retrospective cohort study, our conclusions must be interpreted within the inherent limitations of observational research and should not be read as establishing a causal effect of smoking on DR. The non-random allocation of exposure means the results are susceptible to selection bias, residual confounding, and incomplete capture of clinically relevant behavioral and socioeconomic variables. Although we systematically controlled for numerous known confounders through multivariable regression and propensity score weighting, and verified the directional consistency of results across multiple sensitivity scenarios, we cannot entirely rule out the influence of unmeasured or difficult-to-quantify factors. For example, socioeconomic status, health behavior patterns, healthcare access, and medication adherence may jointly influence smoking behavior and DR risk but are often inadequately captured in routine electronic medical records. Additionally, because fundus examinations were performed in routine clinical practice rather than according to a fixed study protocol, examination frequency differed across patients. Although we adjusted for follow-up intensity in sensitivity analyses, differential surveillance may still have influenced the timing of DR detection. The available observation window was also limited and heterogeneous across participants, which constrained the ability to estimate longer-term risk uniformly. Furthermore, smoking exposure assessment relied primarily on historical medical records and self-reported information, which may have introduced exposure misclassification and measurement error. In particular, although smoking duration and cumulative exposure could be reconstructed for many participants, the temporal sequence of smoking initiation, cessation, or change in intensity relative to diabetes diagnosis was not uniformly available. Therefore, we could not consistently determine whether smoking occurred predominantly before diagnosis, after diagnosis, or overlapped both periods. Recall bias or social desirability bias regarding smoking amount and duration could lead to underestimation of exposure. The study also did not dynamically capture changes in smoking behavior or quitting during follow-up, nor did it allow time-updated modeling of smoking exposure across different stages of the diabetes course. Such non-differential misclassification typically biases estimates toward the null, suggesting our risk estimates for the smoking–early-onset DR relationship may be conservative. Moreover, we did not systematically assess exposure to secondhand smoke or the use of novel tobacco products, which are increasing among younger populations. Their potential impact on microvascular outcomes remains unclear and could lead to an underestimation of overall tobacco-related risk. Our study drew participants from a single medical center; thus, the demographic structure, healthcare delivery model, and retinopathy screening practices may reflect specific regional and institutional characteristics. Caution is therefore warranted when generalizing the findings to young-onset type 2 diabetes populations in different regions, ethnic backgrounds, or healthcare systems. Finally, although we focused on the early post-diagnosis phase and employed a time-to-event framework, the follow-up duration remains relatively limited and insufficient to fully assess the long-term impact of smoking exposure on DR progression trajectories and vision-threatening outcomes. Importantly, because the available follow-up window did not uniformly extend to 5 years for all participants, the present study should not be interpreted as providing a formal estimate of 5-year DR risk. In addition, analyses of DR grade progression were conducted only among participants who had already developed DR, with time zero defined at the first definite DR diagnosis; therefore, these estimates should be interpreted as post-onset progression analyses rather than progression from diabetes diagnosis. Taken together, these limitations mean that the present findings should be interpreted as evidence of association rather than proof that smoking independently causes or accelerates DR onset or progression.
Conclusion
This retrospective cohort study systematically evaluated the association between long-term smoking history and the risk of diabetic retinopathy, particularly earlier-occurring DR during follow-up, in patients with young-onset type 2 diabetes. The findings indicate that smoking is significantly associated with an increased risk of DR and with earlier DR occurrence during the available follow-up period after diabetes diagnosis. This association remained stable after multivariable adjustment, propensity score weighting, and multiple sensitivity analyses, suggesting that smoking is related not only to the overall occurrence of complications but also to differences in the observed timing of disease onset. Further analysis revealed a clear dose-dependent relationship between cumulative smoking exposure and earlier DR occurrence during follow-up. With increasing cumulative smoking exposure, the observed hazard of DR rose progressively, and individuals with high exposure tended to show earlier occurrence of retinopathy during follow-up and more severe DR phenotypes. These findings support viewing smoking as a modifiable risk factor with time-cumulative effects, impacting not just whether complications occur but also how early they emerge and how aggressive their phenotype may be. In the high-risk population of young-onset type 2 diabetes, this study supplements existing evidence from a time-to-event perspective, emphasizing that using DR occurrence alone as an outcome may underestimate the true impact of smoking on microvascular injury. Incorporating early-onset DR into risk assessment frameworks could aid in more accurately identifying high-risk individuals and inform the personalization of clinical follow-up strategies.
In summary, this study suggests that in patients with young-onset type 2 diabetes, long-term smoking is associated with a higher risk of diabetic retinopathy, while higher cumulative smoking exposure is associated with earlier disease occurrence during follow-up and with more severe clinical phenotypes. These findings underscore the importance of enhancing early, targeted smoking cessation efforts, refining retinopathy screening schedules, and implementing more individualized, risk-stratified complication management in this population. Furthermore, this work establishes a foundation for future prospective studies and intervention trials aimed at mitigating microvascular complications in young-onset diabetes.