
Abstract
Purpose
To predict the development of traumatic angle recession glaucoma (TARG) and identify associated risk factors using Kaplan–Meier survival analysis.
Materials and Methods
This retrospective cohort study was conducted across three tertiary hospitals in Malaysia, involving patients treated for blunt ocular trauma and traumatic hyphaema between 1 January 2010 and 31 December 2020. Eligible patients had a minimum of one year of follow-up between 1 January and 31 December 2021. Data collected included demographics, medical and ocular history, injury mechanism, and initial ophthalmic assessment. Kaplan–Meier survival analysis and Cox proportional hazards regression were employed to evaluate glaucoma onset and prognostic indicators.
Results
Of 114 patients with angle recession, 30 (26.3%) developed TARG over a mean follow-up of 66.8 ± 52.1 months. Kaplan–Meier analysis estimated a mean survival time of 8.8 years, with most cases detected within nine months post-trauma. Age was a significant predictor, with a 1% increased risk per year (HR 1.02; 95% CI: 1.00–1.04; p = 0.022). Presence of peripheral anterior synechiae (PAS) conferred a 4.3-fold higher risk of developing TARG (HR 4.29; 95% CI: 2.02–9.13; p < 0.001).
Conclusion
Older patients with PAS following blunt ocular trauma are at significantly increased risk for TARG and warrant close surveillance. Further research is needed to establish optimal follow-up duration and develop predictive tools for early identification of high-risk individuals.
Keywords
Introduction
Ocular trauma is a significant global cause of visual impairment and blindness, particularly among children and young adults. 1 It was estimated 18 million people worldwide suffer from monocular blindness due to traumatic injury. 2 Following a closed-globe injury, regular and long-term ocular follow-up is crucial, as patients face an increased risk of secondary glaucoma. Two peak incidences of glaucoma following blunt ocular trauma have been reported: within the first-year post-trauma and at least ten years later. 2 The incidence of glaucoma following ocular contusion has been estimated at approximately 3.4% within the first six months of follow-up, rising to nearly 6–7% over a ten-year period.3,4 Among these cases, traumatic angle recession glaucoma (TARG) occurs in approximately 4–9% of patients. 6
TARG is defined as an intraocular pressure (IOP) elevation exceeding 21 mmHg following ocular trauma with evidence of structural and functional glaucomatous optic neuropathy. 4 It may present acutely or chronically and can result from both blunt and penetrating injuries. 4 Angle recession is the most common clinical marker of prior blunt ocular trauma. 2 It is thought to occur when the force of impact, acutely compresses the globe while simultaneously expanding it equatorially, resulting in disruption of the ciliary muscle architecture through tearing of its longitudinal and circular fibers. 2 This shearing force separates the longitudinal fibers of the ciliary muscle from the circular fibers, producing the characteristic widening of the ciliary body band seen on gonioscopy. 2 Hyphema may also occur due to shearing of small vessels within the anterior ciliary arteries. 2 Angle recession is widely recognized as a marker of past trauma rather than a direct cause of glaucoma. Concurrently, the trabecular meshwork and Schlemm's canal sustain damage, which progresses to fibrosis and fibrovascular membrane formation. Trauma-induced changes within the trabecular meshwork such as proliferative or degenerative remodeling are implicated in secondary glaucoma development. This may explain the second peak incidence of traumatic glaucoma. 7
Identifying the risk factors for TARG is vital to prevent its potentially devastating long-term consequences. However, establishing these risks remains challenging due to the long follow-up required, often resulting in limited sample sizes. To date, poor presenting visual acuity, hyphema, angle recession exceeding 180 degrees, traumatic cataract, lens displacement, and iris injuries have been identified as significant risk factors for TARG.1,4 Interestingly, the majority of patients with angle recession do not develop glaucoma. 8 Most available data are retrospective and lack standardized follow-up durations.
Clinically, the presence of two peak incidences raises ongoing debate about the ideal duration of long-term monitoring. Determining which patients require extended follow-up and the ideal duration is critical, given the cost and time burden on both patients and medical practitioners. Furthermore, cost-effectiveness considerations influence clinical decision-making, particularly if the yield of secondary glaucoma detection is low. Therefore, identifying high-risk patients for TARG is essential for optimized management and cost-effective care. This study aims to predict the development of traumatic angle recession glaucoma and its associated risk factors using Kaplan–Meier survival analysis.
Materials and method
This is a retrospective cohort record review, carried out at three tertiary hospitals in Malaysia: Hospital Raja Perempuan Zainab II and Hospital Universiti Sains Malaysia in Kelantan and Hospital Sultan Abdul Halim in Kedah. The study received ethical approval by the National Malaysia Research Review NMRR ID-23–00766-WFN and is conducted in accordance with the standards of the Declaration of Helsinki for human research. Medical records of all patients treated for blunt ocular trauma and traumatic hyphaema between 1 January 2010 and 31 December 2020 were retrieved. Patients were eligible only if they had completed at least one year of follow-up after the traumatic event with minimum of three visits. For individuals who presented with blunt ocular trauma on or before 31 December 2020, this required a documented follow-up visit between 1 January and 31 December 2021. A minimum one-year follow-up was necessary to assess the presence of TARG. Patients with open globe injury, previous ocular injuries, pre-existing glaucoma disease, associated brain injuries or no documentation of gonioscopy assessment were excluded from the study.
A total of 156 patients were identified. However, 42 of them had more than 33% of missing data from medical record review. Missing data were defined as inadequate data on initial presentation, for example, no documentation of type of trauma, the absence of documented gonioscopic findings within 3 months post trauma, lack of fundus examination records, no structural or functional assessment of the optic nerve at minimum one year post-trauma, or fewer than three follow-up visits. For the purpose of analysis, only 114 patients were included. Demographic information, medical and ocular history, mechanism of injury, and results of initial ophthalmological assessment including Snellen visual acuity test, examination with slit-lamp biomicroscopy, IOP measurement by Goldman applanation tonometry and dilated fundoscopic examination were recorded for each patient. The vision is categorized following the International Classification of Diseases 11 for distance impairment; mild <6/12, moderate <6/18, severe <6/60 and blindness <3/60. 5 The presence and extent of angle recession assessed by Goldman gonioscopy examinations on subsequent examination or once the hyphaema level resolved were recorded. Angle recession is a gonioscopic finding characterized by a separation between the circular and longitudinal fibers of the ciliary muscle, typically presenting as a widened ciliary body band. 7 Peripheral anterior synechiae (PAS) was also identified but due to lack of proper documentation of the degree of PAS, only the binary data was included in the analysis.
Traumatic angle recession (TAR) refers to an eye with documented angle recession post blunt ocular trauma, with or without a transient rise in IOP, but without any evidence of glaucomatous optic neuropathy.4,6,9 The diagnosis of TAR was made no earlier than one week after the blunt ocular trauma, or once the hyphaema had resolved sufficiently to allow a reliable gonioscopic examination. Traumatic angle recession glaucoma (TARG) was defined as IOP >21 mmHg, sustained for minimum period of three months post trauma, in eyes with documented angle recession, associated optic nerve head changes or glaucomatous visual field defects.4,6,9 A transient rise in IOP is usually caused by the presence of hyphaema. This is typically managed with topical pressure-lowering medications and topical steroids to control inflammation, and it generally resolves within 1–4 weeks after blunt ocular trauma. If there was any suspicion of steroid-induced ocular hypertension or mixed causative factors, the eye was excluded from the analysis. The optic cup-disc ratio, Humphrey visual field analysis 24–2 Swedish Integrated Threshold Analysis (SITA), the IOP-lowering medications and any IOP-lowering procedures including anterior chamber washout, paracentesis, trabeculectomy, and glaucoma drainage implants were extracted from the medical records.
All data were entered into the Statistical Program for Social Science (SPSS) version 29.0 software and used for statistical analysis. Any wrong entry or double entry were checked. For all the numerical variables, the normality distribution was assessed. Kaplan-Meier survival analysis was performed to assess the development of glaucoma during the follow up period. Time to event was defined as the interval between the diagnosis of TAR in the eye with blunt ocular trauma and the subsequent development of TARG, measured in days, months, or years. Eyes that did not develop TARG by the end of the study period, or were lost to follow-up, were treated as censored observations. Cox proportional hazard regression analyses were performed to identify the prognostic factor for progression of glaucoma. All covariates with p values <0.25 or clinically important in univariable analysis were included in multivariate analysis. P < 0.05 is considered statistically significant in all analysis.
Result
A total of 114 patients with TAR following blunt trauma were included for analysis. Thirty patients (26.3%) developed TARG after the mean duration 66.8 ± 52.1 months of follow-up. Blunt ocular trauma is significantly more common in men: 93.3% in TARG and 91.7% in TAR (Table 1). Patients with TARG were significantly older than TAR (p = 0.020) (Table 1). This study included participants from the major ethnic groups in Malaysia residing in the states of Kedah and Kelantan. In both states, Malays constitute the predominant population. 8 Accordingly, a substantial proportion of the individuals who developed TARG were Malay (Table 1). Based on clinical parameters, patients with TARG had significantly higher median IOP at presentation, lens subluxation or dislocation, with gonioscopic findings of peripheral anterior synechiae (PAS) and angle recession >180°compared to those with TAR (Table 2). Majority had good vision, present of hyphaema and normal iris configuration at presentation following blunt trauma (Table 2).
Comparison of demographic characteristics of patients who developed TARG and TAR post blunt ocular trauma.
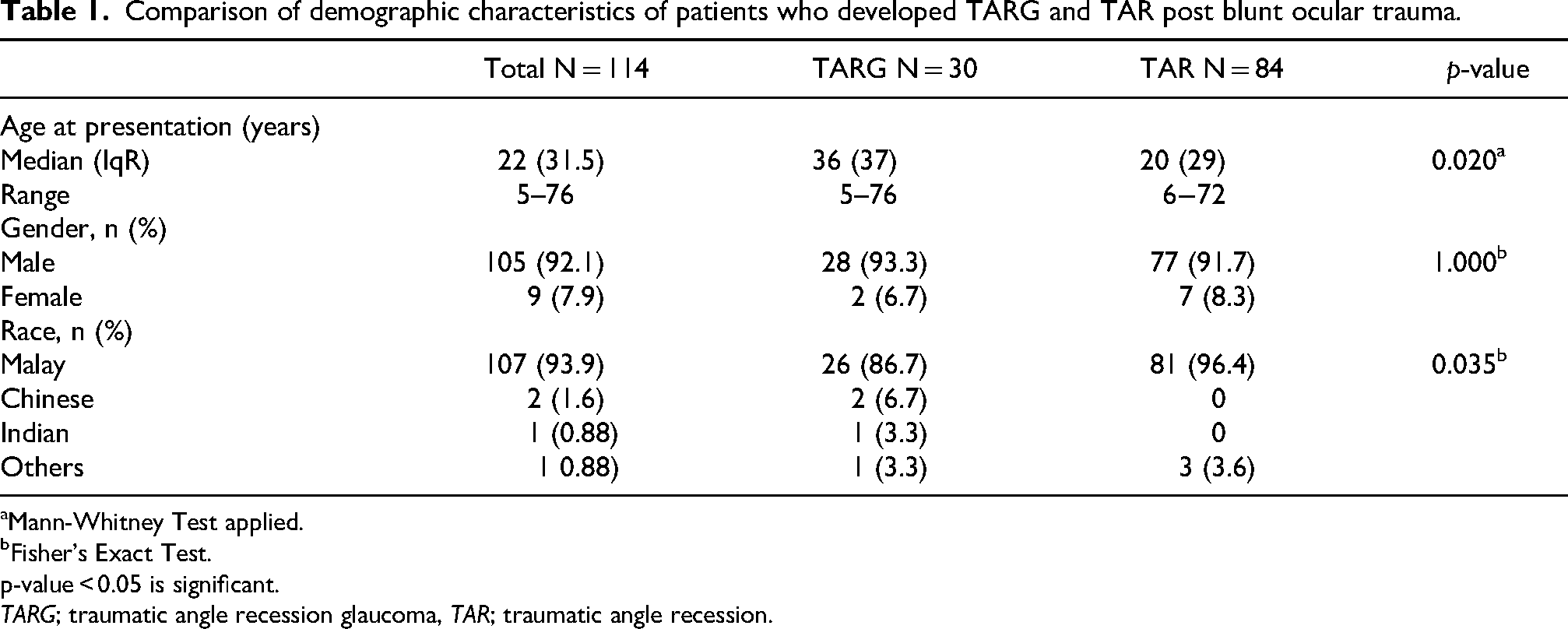
Mann-Whitney Test applied.
Fisher's Exact Test.
p-value < 0.05 is significant.
TARG; traumatic angle recession glaucoma, TAR; traumatic angle recession.
Clinical characteristics of patients with blunt ocular trauma between those with traumatic angle recession glaucoma and traumatic angle recession.
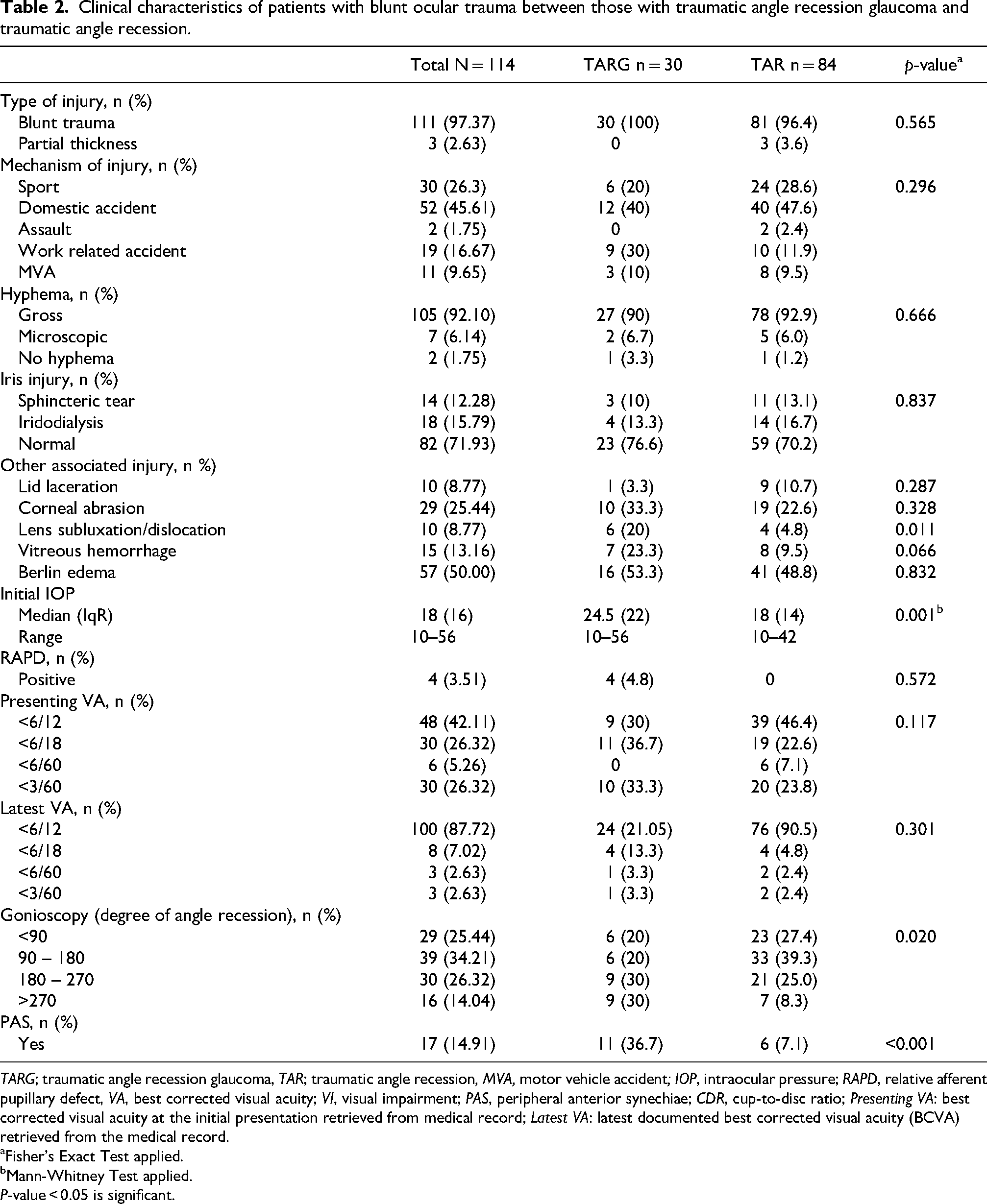
TARG; traumatic angle recession glaucoma, TAR; traumatic angle recession, MVA, motor vehicle accident; IOP, intraocular pressure; RAPD, relative afferent pupillary defect, VA, best corrected visual acuity; VI, visual impairment; PAS, peripheral anterior synechiae; CDR, cup-to-disc ratio; Presenting VA: best corrected visual acuity at the initial presentation retrieved from medical record; Latest VA: latest documented best corrected visual acuity (BCVA) retrieved from the medical record.
Fisher's Exact Test applied.
Mann-Whitney Test applied.
P-value < 0.05 is significant.
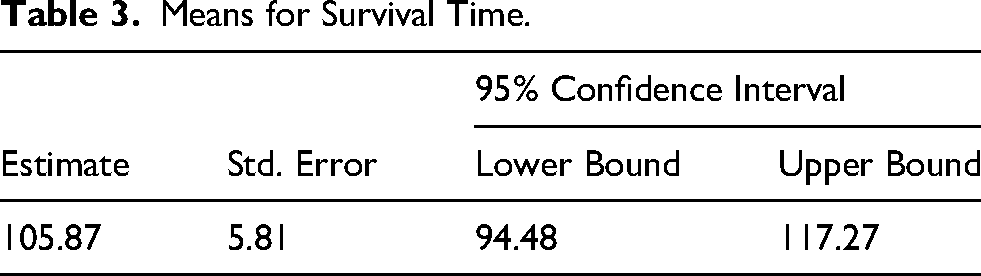
The Kaplan–Meier analysis estimated the mean survival time to be 105.9 (SE = 5.81) (95% CI 94.48, 117.27) months: 8.8years (Table 3). A total of 30 TARG events out of 114 cases occurred in 9 years. The median survival time could not be estimated, as fewer than 50% of participants had developed traumatic angle recession glaucoma by the end of the follow-up period. The trend based on Kaplan–Meier survival analysis demonstrated a progressive decline in the cumulative probability of remaining TARG-free over time (Figure 1). At 1 month, the survival rate was 90.4%, dropping to 80.7% at 3 months, and further to 69.9% at the end of 113 months. Majority developed TARG within 9 months post blunt ocular trauma. At 5 years (60 months), 29 eyes developed TARG, which interpreted as survival analysis of 74.6%. At 113 months, another 1 eye fulfilled the criteria for TARG (Figure 1).
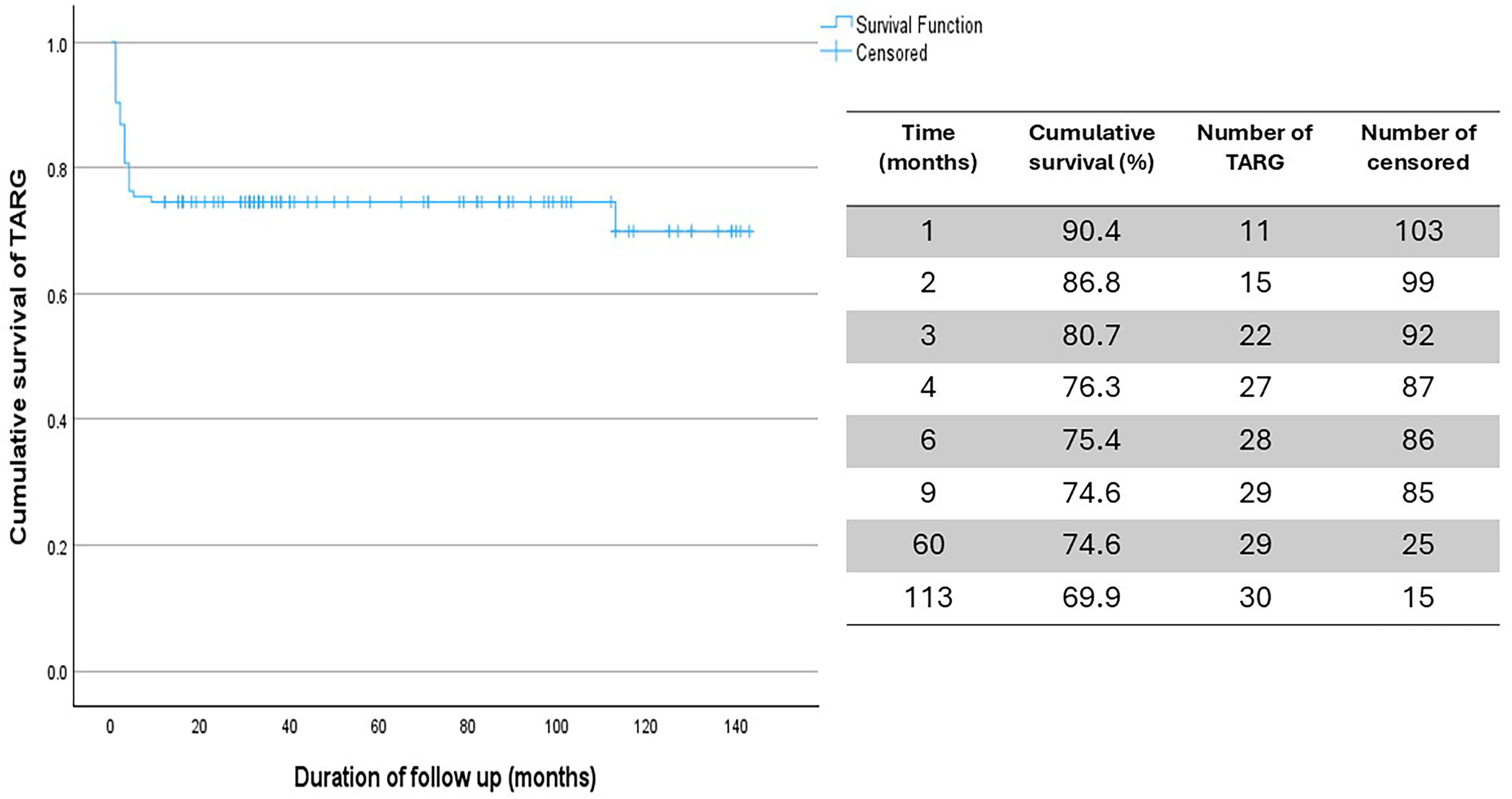
Kaplan Meier analysis on cumulative development of TARG post blunt trauma.
Means for Survival Time.
In the simple Cox regression analysis, age, work related accident, angle recession >270°, PAS, and lens subluxation or dislocation were significant predictors of TARG (Table 4). However, only age and the presence PAS remained significant in the multiple Cox regression analysis (Table 5). Age was a significant predictor for TARG, with a hazard ratio (HR) of 1.02 (95% CI: 1.00,1.04; p = 0.022). For each additional year, the risk of developing TARG increases by approximately 1%. Patients with PAS had over a fourfold increased risk of developing TARG (HR = 4.29; 95% CI: 2.02, 9.13; p < 0.001) compared to those without PAS.
Prognostic factors of time to traumatic angle recession glaucoma diagnosis by simple cox proportional hazards model (n = 114).
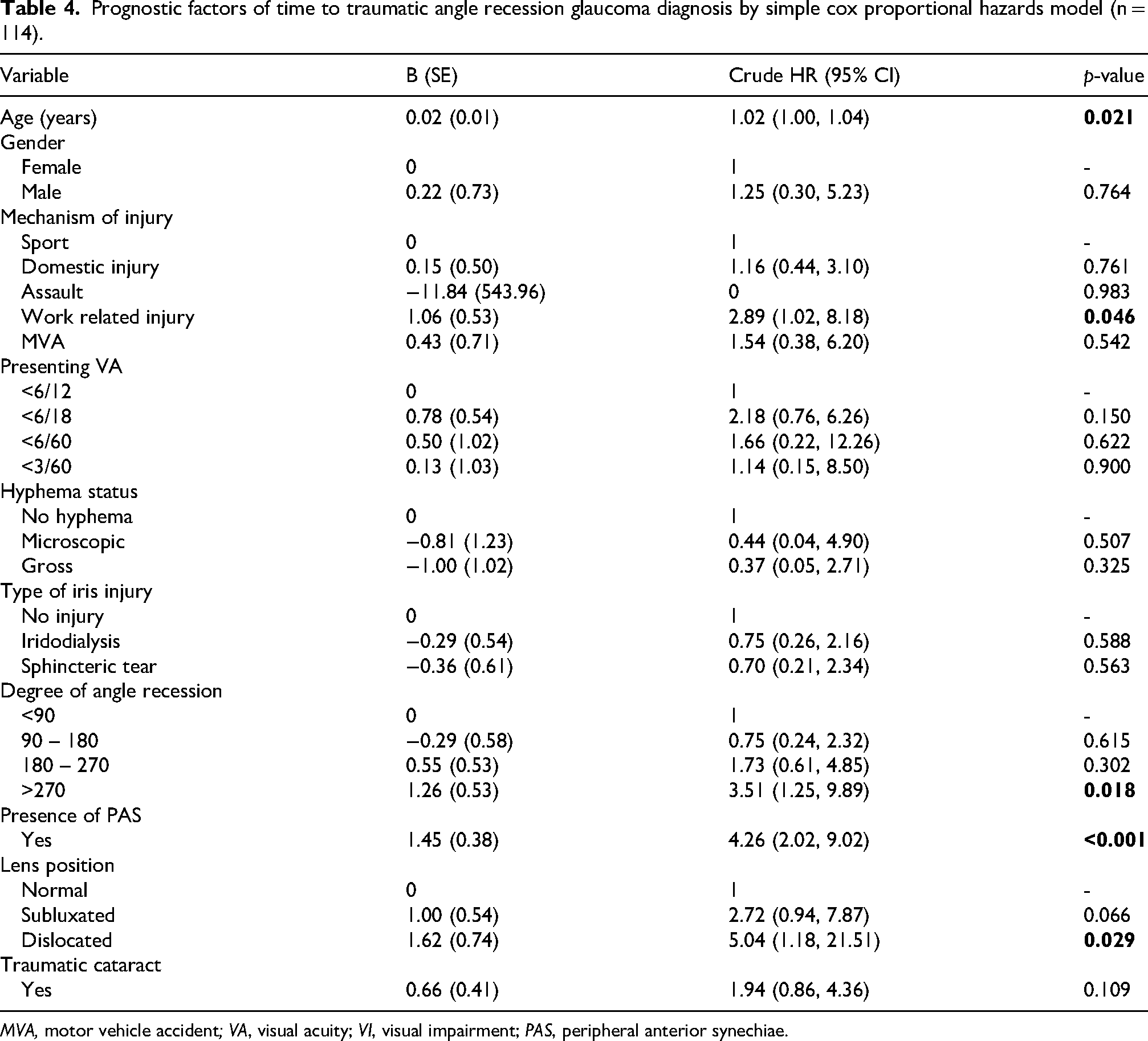
MVA, motor vehicle accident; VA, visual acuity; VI, visual impairment; PAS, peripheral anterior synechiae.
Prognostic factors of time to traumatic angle recession glaucoma diagnosis using multiple cox proportional hazards model.
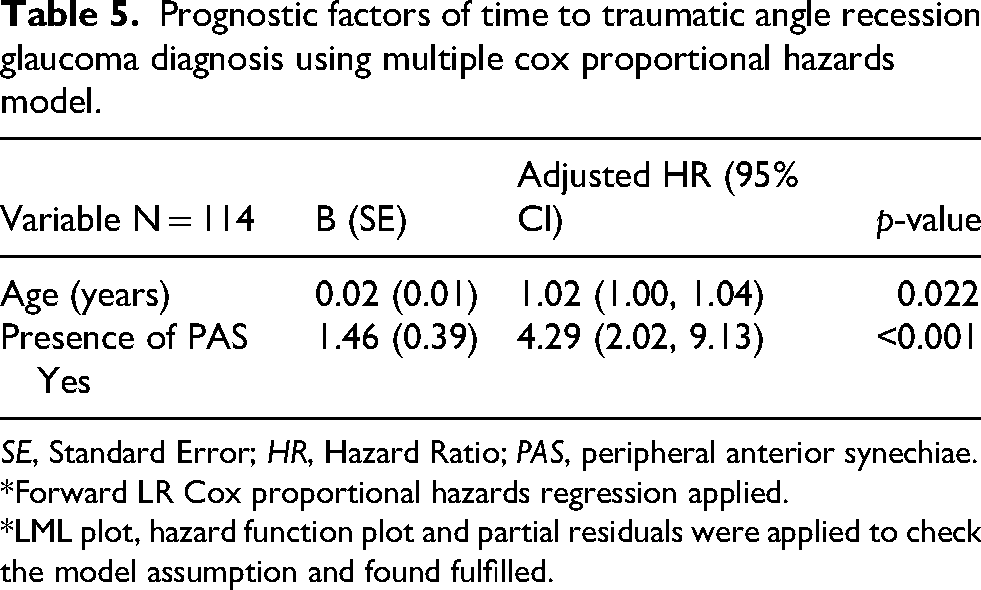
SE, Standard Error; HR, Hazard Ratio; PAS, peripheral anterior synechiae.
*Forward LR Cox proportional hazards regression applied.
*LML plot, hazard function plot and partial residuals were applied to check the model assumption and found fulfilled.
Discussion
Predicting the onset of TARG as a consequence of blunt ocular trauma is inherently complex. One major challenge lies in determining the optimal follow-up duration, further complicated by the reported double-peaked incidence of TARG.11,12 Another critical issue is the lack of a standardized definition where previous studies have diagnosed TARG based solely on intraocular pressure (IOP) without confirming structural or functional glaucomatous changes.6,12 Additionally, gonioscopic findings were often excluded from the diagnostic criteria for both TAR and TARG. 12 Accordingly, in the present study, TARG was defined not solely on persistent elevation of IOP but also on demonstrable structural and/or functional glaucomatous optic neuropathy. The event-to-time analysis was initiated at the onset of documented TAR, rather than from the moment of the blunt ocular injury, as this approach offers a clearer reference point for subsequent follow-up scheduling and facilitates more individualised clinical management.
Given the predominantly retrospective nature of existing studies, considerable variability in findings has been reported.11,13 Ng et al. performed a Kaplan-Meier survival analysis comparing the likelihood of TARG development in patients with microscopic versus gross hyphaema. Their findings indicated that TARG onset following blunt trauma ranged between six months and ten years, with an average onset at approximately 6.2 years. 15 However, in the present study, which included 114 patients, the mean time to TARG development was longer 105.9 months (95% CI 94.5,117.3), approximately 8.8 years. Of the cases analyzed, 30 eyes met the criteria for TARG, demonstrating a progressive decline in the cumulative probability of remaining TARG-free over time. On average, this suggests that patients remained glaucoma-free for approximately nine years post detection of TAR.
A striking observation in this study was the early onset of TARG with 22 out of 30 cases (73.3%) were diagnosed within the first three months following detection of TAR. This finding aligns with previous retrospective studies, which have reported peak prevalence within three to six months post-injury.1,3,6,9,13 Interestingly, the overall prevalence of TARG as a sequela of blunt trauma was lower than anticipated, preventing the calculation of median survival time. Median survival time is defined as the time at which half of the study cohort is still being followed without censoring or occurrence of the event. 14 Because it is less sensitive to outliers, it offers a more stable and clinically representative summary of patient follow-up. Mean survival time, on the other hand, represents the average duration of observation and is calculated as the area under the survival curve. 14 Prior research indicates that, irrespective of injury timing, the lifetime incidence of secondary glaucoma following trauma ranges between 7% and 9%. 16 Kaplan-Meier analysis in the present study revealed a cumulative probability of 75% for remaining TARG-free at five years, reinforcing the notion that while TARG can develop insidiously, a substantial proportion of patients maintain stability over extended periods. Notably, no double-peaked incidence was observed, as only one eye met the criteria for TARG after 8.8 years of follow-up.
The identification of high-risk cases is crucial for optimizing follow-up strategies and improving long-term outcomes. Despite various attempts to define predictive markers for TARG, no specific algorithm has been established. The Ocular Trauma Score (OTS) has been utilized to estimate secondary glaucoma risk in both open and closed globe injuries. 17 However, while OTS provides reasonable predictive value, it has demonstrated lower accuracy in closed globe injuries due to the disproportionate influence of initial visual acuity (VA) in scoring.18–20 Another potential bias stems from follow-up patterns associated with injury severity. Severe blunt ocular trauma generally necessitates closer surveillance, increasing the probability of earlier event detection, while mild injuries are more likely to result in missed or defaulted appointments, potentially leading to under-ascertainment or delayed identification of outcomes.
Hyphaema, whether gross or microscopic, is a common clinical presentation following blunt ocular trauma, contributing to ocular hypertension through trabecular meshwork obstruction and inflammation-related haemostatic processes. While the presence of hyphaema and lens-related pupillary block are known to influence early-stage IOP elevation the findings of this study contradict prior reports, as hyphaema did not emerge as a strong predictor of TARG. 15 Notably, one case of TARG developed without preceding hyphaema, and no significant difference in survival time was observed between patients with gross versus microscopic hyphaema. 15
Late-onset IOP elevation beyond six months is more frequently associated with traumatic angle recession or secondary fibrosis within the angle, leading to progressive outflow resistance. 1 Angle recession exceeding 180° has been identified as a significant risk factor for TARG, independent of hyphaema.9,15,21–23 Epidemiological studies indicate that only 5.5% of eyes with angle recession develop glaucoma, while this proportion rises to 8.0% in cases involving 360° angle recession. 24 These findings suggest that angle recession alone may not be a strong predictor of TARG, in agreement with the present study's conclusions. Similarly, subluxated lenses have been proposed as potential contributors to secondary glaucoma due to zonular instability and altered aqueous dynamics, yet in this cohort, lens subluxation did not demonstrate a significant association with TARG development. 25
In interpreting these findings, it is important to acknowledge methodological considerations related to multivariate modelling. Variables were selected for inclusion in the Cox regression analysis based on their univariate significance and established clinical relevance. While this approach is commonly used to minimise overfitting particularly in studies with a limited number of events (as in the present study), it may inadvertently exclude factors that exhibit only weak individual associations but could exert meaningful effects when considered jointly. This potential omission bias may influence the detection of subtle or synergistic predictors such as the degree of angle recession or lens subluxation.
Among the predictive markers assessed, peripheral anterior synechiae (PAS) emerged as a strong independent risk factor for TARG. Regardless of its extent, PAS increased the likelihood of TARG by 4.3-fold (95% CI: 2.02–9.13; p < 0.001). Fibrotic PAS formations at the boundaries of angle recession further compromised trabecular meshwork function, contributing to persistent IOP elevation. 7 Tumbocon et al. observed that PAS frequently forms at the lateral margins of angle recession, strongly correlating with post-concussion glaucoma, particularly in cases involving traumatic cataracts. 26 Major limitation in the present study relates to the incomplete documentation of gonioscopic findings, particularly the extent of PAS. Owing to the retrospective design of this study and variability in clinical record-keeping, detailed information on PAS extension was unavailable for a substantial proportion of patients. This is noteworthy because the degree of PAS involvement rather than its mere presence has been shown to influence aqueous outflow compromise and may carry important prognostic value in traumatic glaucoma.9,10,13,21 The inability to quantify PAS extension in this cohort limits the precision of risk stratification and may underestimate the true predictive contribution of extensive synechial closure. Additionally, some individuals were lost to follow-up after one year, often due to retained good vision or the absence of gonioscopy evaluations.
Age plays a complex and multifactorial role in TARG development. While advanced age is a widely recognized risk factor for glaucoma progression, 27 the initial susceptibility to angle recession is more strongly associated with trauma exposure, which tends to be higher among younger individuals.9,21 However, as patients age, the likelihood of developing TARG increases. 16 In this study, older age at presentation significantly heightened susceptibility. Younger individuals generally exhibit more elastic ocular tissues, facilitating faster recovery and reducing the probability of permanent angle recession following trauma.11,28 Conversely, older adults particularly those over 50 often show diminished trabecular meshwork resilience due to fibrotic changes, leading to progressive outflow resistance and delayed-onset glaucoma. 29
The necessity for glaucoma surgery rises with age among patients with secondary glaucoma following ocular trauma. 22 Established risk factors such as lens injury, poor initial visual acuity, hyphaema, extensive angle recession (>180°), and elevated baseline IOP are more frequently observed in older individuals or those with severe ocular trauma. 9 This highlights an important distinction: while younger patients experience higher trauma exposure, older individuals face an elevated risk of disease progression and surgical intervention due to age-related trabecular dysfunction and optic nerve vulnerability. 22
Despite the valuable insights provided by this study's Kaplan-Meier survival analysis, limitations such as its retrospective design, small sample size, and high censoring rate must be acknowledged. The lack of standardized follow-up protocols further constrains the interpretation of risk factors. Moving forward, prospective studies with larger cohorts, structured clinical protocols, and extended follow-up durations are necessary to enhance the reliability of findings and improve clinical applicability. In conclusion, older patients presenting with PAS following blunt ocular trauma warrant vigilant monitoring, given the significant clinical implications for the development of TARG. These findings underscore the importance of early identification and sustained follow-up in high-risk individuals. While the optimal duration of surveillance and a robust predictive algorithm remain to be established, this study lays a valuable foundation for future research aimed at refining risk stratification and enhancing long-term care strategies.
Footnotes
What is known
Traumatic angle recession glaucoma (TARG) typically manifests within 3 to 6 months or around 10 years following blunt ocular trauma. Extensive angle recession and the presence of hyphaema are established risk factors for TARG development after blunt ocular injury.
What is new
At five years post-trauma, only 25% of patients progressed to TARG, underscoring the importance of long-term surveillance in at-risk individuals. Advancing age at presentation was significantly associated with TARG onset, likely reflecting cumulative age-related ocular changes compounded by trauma-induced structural disruption. The presence of peripheral anterior synechiae independently conferred a fourfold increased risk of TARG, underscoring its prognostic significance in post-traumatic glaucoma assessment.
Acknowledgements
We would like to express our sincere gratitude to Associate Professor Dr Siti Azrin Abd Hamid for her invaluable guidance in the Kaplan–Meier survival analysis. We also extend our appreciation to the dedicated staff of the Eye Clinics at Hospital Pakar Universiti Sains Malaysia, Hospital Raja Perempuan Zainab II, and Hospital Sultan Abdul Halim for their support and assistance, both directly and indirectly, throughout the course of this study.
Ethical approval
The study received ethical approved by the National Malaysia Research Review NMRR ID-23–00766-WFN and is conducted in accordance with the standards of the Declaration of Helsinki for human research.
Author contributions
Concept and design: Liza Sharmini Ahmad Tajudin, Izyani Hussin, Rahimie Hanafi
Data acquisition: Izyani Hussin, Saranya Pulanisamy, Siti Hajar Abu, Nurhamiza Buang, Norhalwani Husain, Azhany Yaakub
Data analysis and interpretation: Liza Sharmini Ahmad Tajudin, Izyani Hussin, Rahimie Hanafi
Manuscript drafting: Liza Sharmini Ahmad Tajudin, Izyani Hussin
Critical revision: Liza Sharmini Ahmad Tajudin
Approval of final manuscript: Liza Sharmini Ahmad Tajudin, Izyani Hussin, Rahimie Hanafi
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Presentation
Part of this study was presented as e-poster during the 6th Asia-Pacific Glaucoma Congress 2022 (APGC 2022), Kuala Lumpur on 4 −7 August 2022.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.