
Abstract
Purpose
For young people, transition programmes between paediatric and adult services ensure continuity of care for young people while improving their confidence and autonomy in managing their health. Despite targeted support improving outcomes in other chronic conditions, the development of transition programmes in children's eye care remains limited. This scoping review aims to review published literature about transition programmes supporting young people in ophthalmic services.
Methods
Following guidance from the Joanna Briggs Institute, we carried out a scoping review, searching Ovid MEDLINE, Ovid Embase and Cochrane Library databases to identify articles on transition programmes for young people from paediatric to adult eye care services. Two reviewers independently screened the titles and abstracts before reviewing the full text. We extracted data into a pre-specified extraction tool.
Results
Of 339 identified publications, five met the inclusion criteria. No publications specifically addressed transition programmes in ophthalmology. The included studies reported ophthalmic care within the context of systemic conditions. Two studies reported a transition programme for young people with type 1 diabetes, two rheumatological conditions, and one explored young people's views on the transition process in an eye/vision context.
Conclusion
This review highlights the scarcity of reports about transition programmes relating to ophthalmology. Existing programmes in other specialities can provide a framework which could be adapted to ophthalmology. Further research is required to develop the use and impact of programmes in ophthalmology to ensure better outcomes for patients and healthcare providers.
Introduction
Growing up means gaining independence and autonomy, and also learning how to take responsibility for one's lifestyle and healthcare. For young people with chronic health conditions, learning about their condition and its management, how to interact with healthcare professionals, and how to advocate for themselves, is an essential part of growing up and is needed when moving from paediatric to adult healthcare services. For providers, transition is defined as the intentional and carefully planned process of transferring adolescents and young adults with chronic medical conditions from paediatric healthcare systems/ providers to those focused on adult care.1,2
Targeted support with the transition during adolescence and ensuring that young people are ready for transition are associated with better clinical and psychosocial outcomes in a range of chronic conditions with onset in childhood,2,3 such as inflammatory bowel disease,1,4 type-1 diabetes 5 and juvenile idiopathic arthritis (JIA),6–8 but clinical implementation is variable.8–10Chronic conditions affecting eyes can also present early in childhood and persist into adulthood, but there appears to be a lack of evidence regarding transition programmes in ophthalmology.
This scoping review aims to collate and evaluate existing literature about programmes supporting young people with their transition from paediatric to adult ophthalmic services and identify gaps to guide future programme development and evaluation.
Methods
We developed the protocol following Joanna Briggs Institute guidance 11 and published it on Open Science Framework. 12 This review follows the Preferred Reporting Items for Systematic Reviews and Meta-analysis Protocols/ Extension for Scoping reviews (PRISMA-ScR). 13
Eligibility criteria of reviewed studies
We included publications that included children and young people aged around 13–25 years. As transition programmes should consider the young person's maturity, an exact age limit cannot be set. We included publications that report the development, use and/ or evaluation of programmes to support young people with their transition from children's to adult eye care services. Transition programmes could be described as an intervention, and could include educational programmes including software, joint clinics staffed by paediatric and adult health care professionals, or any other activity that supports the transition from children's to adult eye care.
Outcomes included processes (e.g., developing and implementing a transition programme), patient – / condition – / service-specific outcomes (e.g., transition readiness, adherence, appointment attendance, and visual outcomes), and any unanticipated events.
We did not restrict the review to publications from specific geographic locations. We included studies conducted in all settings where eye/ vision care is provided for this age group, including community and hospital settings, child development centres, low-vision services (qualified teachers for sight-impaired students/ family support services) and local authorities. We included primary research articles with any study design other than single-case reports and secondary data analyses. We included peer-reviewed journal articles published until the last day of the search, written in English. We excluded articles in other languages that did not include an English translation within the publication, animal and cell/ tissue studies. We excluded interventions that are medicines, chronic conditions which do not affect eyes/ vision, and studies that did not describe a transition programme or process. We excluded meta-analyses, systematic and scoping reviews, commentaries and editorials. We also excluded grey literature to focus on peer-reviewed evidence and to ensure consistency in study quality and reporting.
Information sources
A specialist search expert (DB) carried out searches on Ovid Medline (1946-), Ovid Embase (1947-) and Cochrane Library.
Search
The key terms for conducting searches were ‘eye diseases’, ‘transition’‘paediatric’ and ‘adult’. We used Medical Subject Headings (MeSH) and free text terms with all relevant synonyms to develop the search strategies. We also used Boolean operators ‘OR’, ‘AND’ to combine search lines. A more detailed sample search strategy could be viewed in the protocol published on Open Science Framework (https://osf.io/93xcb/files/osfstorage). 12
Selection of sources of evidence
The search strategist (DB) conducted the search, and we imported the results to Covidence Systematic Review Software (Veritas Health Innovation, Melbourne, Australia) for de-duplication and screening. To ensure consistency among reviewers during title and abstract screening, we carried out a pilot: two reviewers (AK and SB) independently screened the same selection of 20 titles and abstracts from the search based on the eligibility criteria and discussed the results (include/exclude/unsure). They subsequently screened all remaining titles and abstracts, discussed and resolved disagreements within Covidence, with reviewer ADN as mediator when required.
The two reviewers AK and SB then independently scrutinised the full texts for inclusion using a custom-designed inclusion/ exclusion criteria list within Covidence. We included publications for full-text review where the abstract review indicated ‘unsure’ after discussion. We discussed and resolved disagreements, with ADN as mediator.
Data charting process
We developed a data extraction tool within Covidence. Two reviewers independently extracted data, then discussed and resolved disagreements.
Data items
We extracted publication-identifying information (first author and author contact details, year, title, country), study aims, design, start/ end date, funding sources, conflicts of interest, target population, inclusion/ exclusion criteria, recruitment methods, number of participants and duration of study participation, population demographics (mean age, gender, diagnosis), intervention(s), parameters studied, technology used, summary statistics of intervention parameters outcomes at baseline and follow-up timepoints.
Critical appraisal of individual sources of evidence
In line with guidance for scoping 13 reviews, we did not carry out a critical appraisal of individual sources.
Synthesis of results
We tabulated the characteristics of included studies (number, geographic distribution, populations, study designs). We then analysed the content and summarised the findings of included studies according to interventions (if any) and outcomes. We did not carry out a quality assessment of included studies, because the objective of this scoping review is to provide a map and overview of the research conducted to date.
Results
Selection of sources of evidence
The search was performed in October 2024 and generated 339 publications (Figure 1). Five duplicates were removed. Screening of titles and abstracts excluded 295 papers; of 39 full texts reviewed, 5 met the inclusion criteria (Table 1).
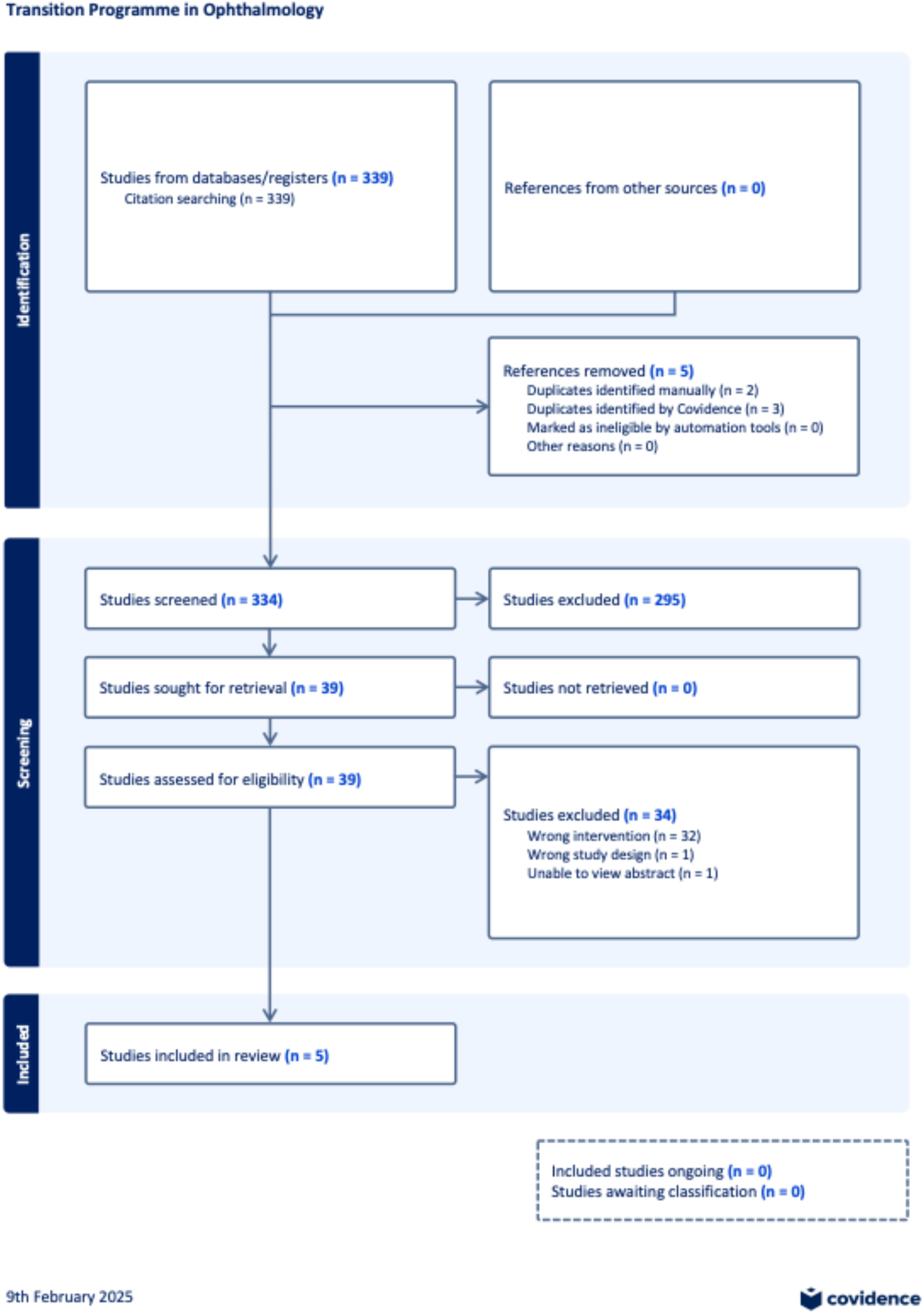
PRISMA flowchart of process identification of publications included in this scoping review.
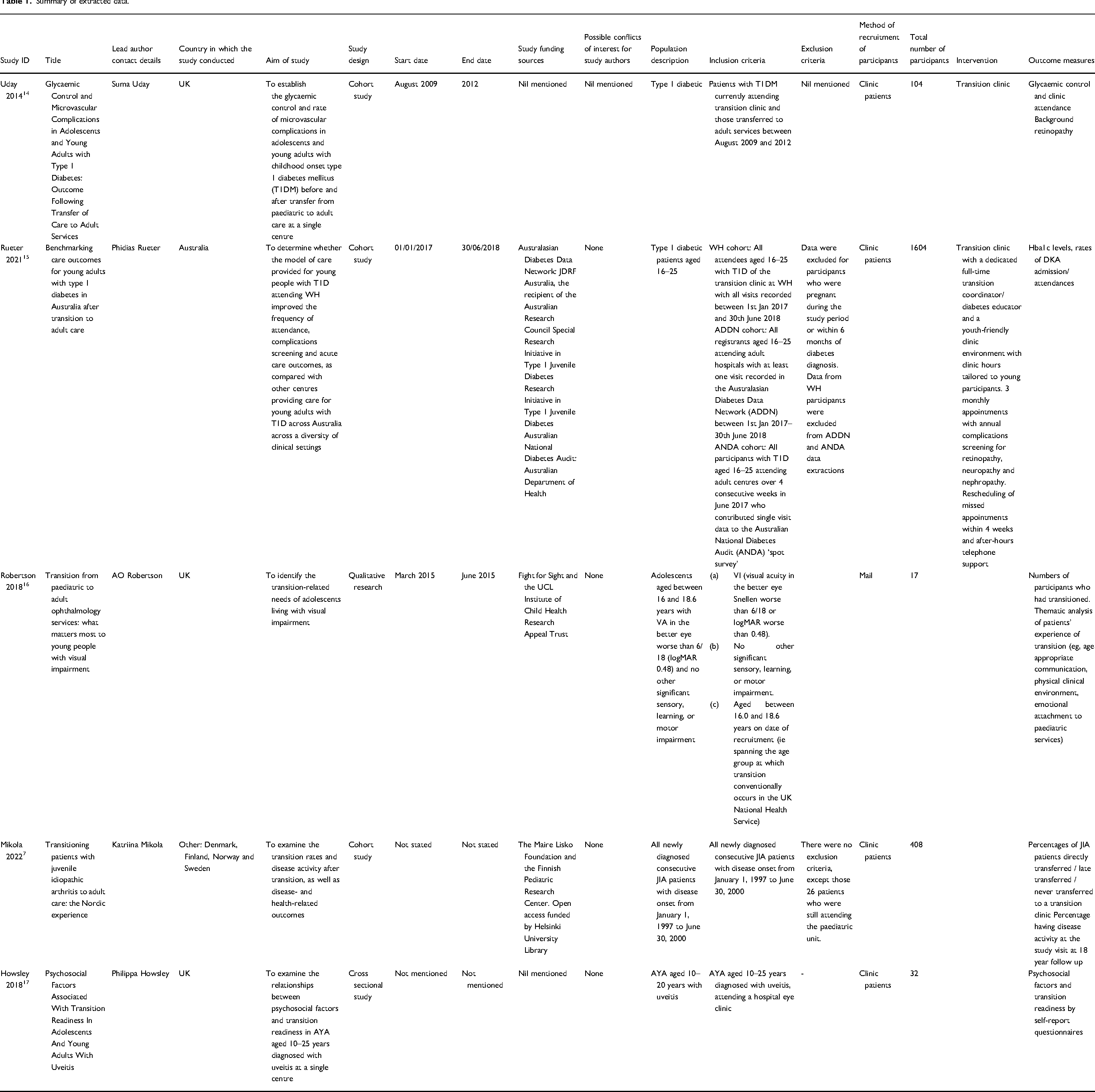
Summary of extracted data.
Characteristics of sources of evidence
The five included studies were published between 2014 and 2022 and were conducted in high-income countries, with three from the United Kingdom. Study designs included three cohort studies, one cross-sectional study, and one qualitative study. The number of participants ranged between 17 and 1604. All but one study was conducted in hospital settings, with three recruiting patients through clinics and two by postal mail.
The studies explored the transition process for children and young people with a range of long-term conditions. Two studies were focused on individuals with type 1 diabetes,14,15 two were related to rheumatology patients,7,16 and one on adolescents with visual impairment. 17 The study populations were heterogeneous, with a wide age group of 10 to 25 years.
Transition programmes
Transition programmes varied significantly across studies. Some studies described the use of a structured transition clinic, dedicated coordinators, email support and involvement of a wider multidisciplinary team. In others, the transition process was not clearly outlined. There was also variability among participating centres within studies. In the Nordic study, there were geographical differences in the delivery of transition services and the transition rate.
Clinical and service outcomes
The impact of transition programmes on healthcare outcomes appears to be variable. Patient engagement metrics, such as screening rates and loss to follow-up, appear to be better for individuals in transition programmes. There appears to be limited evidence of improvement in clinical outcomes, such as disease activity and glycaemic control. In Mikola's cohort study, the prevalence of JIA-related uveitis was lowest in the ‘not transferred’ group; only 9% (n = 18) had a history of uveitis, compared to twenty-five percent (n = 41) of the directly transferred patients, and 30% (n = 15) of those who were referred later. It was suggested that the patients undergoing transition were more likely to have more active or advanced disease, but further work is needed to explore this association.
Psychosocial factors
Psychosocial factors were explored to assess correlation with readiness and experience with the transition process. Greater transition readiness was found to be associated with better psychosocial quality of life, physical quality of life and social support, and lower anxiety/ depression levels, highlighting the need for psychosocial needs to be managed alongside medical needs. Qualitative data revealed that age-appropriate communication and the clinic environment were associated with greater confidence in managing health care as an adult.
Discussion
Despite increasing recognition of the importance of transition programmes for young people, this review did not identify any publications describing a transition programme for young people moving from children's to adult eye care services. This signifies an unmet research need, especially given that many chronic conditions affect vision from childhood and can result in considerable visual morbidity going into adulthood.
The studies we identified presented transition programmes for young people with chronic systemic medical conditions with ophthalmic manifestations such as type 1 diabetes and JIA. Studies reported both clinical outcomes, such as disease control and rate of complications, as well as psychosocial needs and transition readiness. Three studies included an intervention, typically a specialist clinic with multi-disciplinary input. There was heterogeneity in the age of the population included, highlighting the wide classification of the timing of the transitionary period in children. This limits comparability between studies and presents a challenge for standardisation of the transition process. As transition readiness is likely to vary between individuals, there may be a need for formalised assessment protocols to ascertain the timing of transition.
The lack of ophthalmology-specific transition programmes suggests that other specialities, such as diabetes and endocrinology, are more advanced in developing and establishing these programmes. However, the core elements of transition programmes are not unique to particular specialities, as the main goal is to enable young people to understand their condition and its management, engage with healthcare providers, and take control of medication adherence and hospital visits. 18 A transition programme for children and young people attending eye care services could therefore draw on existing models. This could include specialist transition clinics, with allocated coordinators and multidisciplinary staff.
Future research should focus on the development of ophthalmology-specific programmes, with particular evaluation of their impact on service delivery, patient and staff experience and clinical outcomes. 19 There should also be an emphasis on meeting individual psychosocial needs to optimise transition readiness and improve their self-efficacy and knowledge. A greater consensus is required to standardise the transition process, including optimal timing and core components of transition care.
As this is a scoping review, no quality assessment or evaluation of the risk of bias in the literature was performed. Additionally, only a small number of studies were identified, all in high-income settings with varying outcomes, which may limit the generalisability of the findings. However, this review has provided useful insight by identifying gaps in the current literature to guide further research and clinical reports.
Conclusion
Transition programmes play a key role in providing development-appropriate care for young people with chronic ocular conditions and have the potential to improve long-term outcomes. However, ophthalmology-specific evidence to inform best practice is lacking. Further research is needed to support the implementation and evaluation of transition programmes with chronic eye conditions.
Footnotes
Ethical considerations
Not applicable.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study did not receive specific funding. ADN is supported by the NIHR Moorfields Biomedical Research Centre. The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.