
Abstract
Purpose
To compare laser refractive retreatment rates between patients with a clinically significant change in refraction (cycloplegic different) following cycloplegia versus those without (cycloplegic similar).
Settings
This retrospective study included consecutive patients who underwent laser in situ keratomileusis (LASIK) or photorefractive keratectomy (PRK) between January 2005 and December 2019 at the Care-Vision Laser Centers, Tel-Aviv, Israel.
Design
Myopic patients were divided into two groups according to whether or not they demonstrated preoperative cycloplegic difference (a hyperopic shift of 0.50D or more following cycloplegia).
Methods
Binary logistic regression analysis, was performed to account for potential confounders of retreatment.
Results
Overall, 14,679 eyes were included in the final analyses. The age of the participants was 27.4 ± 7.8 years and 53.2% were male. Of these, 1,458 (9.9%) were cycloplegic different. Overall, 0.62% (n = 91) of eyes underwent retreatment. The cycloplegic different group had a significantly greater retreatment rate (1.10% versus 0.57%, p = 0.01) and eyes which demonstrated cycloplegic difference were 1.94 times more likely (95% CI 1.13 to 3.35) to undergo retreatment. In stepwise binary logistic regression analysis, after accounting for potential confounders (gender, age, central corneal thickness, keratometry, best corrected visual acuity, cylinder, optic zone treatment, treatment type, laser model and ablation depth), cycloplegic difference remained a significant predictor of retreatment (OR = 1.80, 95% CI 1.01–3.18, p = 0.04).
Conclusion
A hyperopic shift of 0.50D or more in refraction following cycloplegia in myopic patients undergoing laser refractive surgery is associated with an increased risk for subsequent retreatment.
Key messages
WHAT IS KNOWN
Larger difference between dry and cycloplegic refraction may be more common among younger individuals and those with hyperopia, low-grade myopia and anisometropia.
WHAT IS NEW
A difference of 0.50D or more between cycloplegic and dry refraction is associated with increased risk for future retreatment. Cases with difference of 0.50D or more between cycloplegic and dry refraction require careful reevaluation and planning.
Introduction
Refractive errors are a leading cause of reversible visual impairment worldwide, thus making refractive surgery one of the most performed ocular procedures.1–3 Improving surgical refractive outcomes leads to improved quality of life and patient satisfaction. Enhancement rates, which reflect real-world surgical outcomes and patient satisfaction, have been used in numerous refractive surgery studies as a primary metric of success. In today's patient-centered environment, individuals are increasingly aware of the possibility of retreatment and may easily opt for retreatment if the initial surgical outcome does not meet their expectations.4–5
Factors associated with increased risk of enhancement have been the focus of studies aiming to predict cases that are more likely to require retreatment.5–9 The difference between dry (non-cycloplegic) and cycloplegic refraction is one such factor. Larger difference between dry and cycloplegic refraction may be more common among younger individuals and those with hyperopia, low-grade myopia and anisometropia. In published literature, up to 19% of young hyperopic patients may have a disparity of 1 diopter (D) or more between dry and cycloplegic refraction.10–11
Cycloplegic refraction is often mandatory in young and middle-aged patients, as significant accommodative spasm may persist even in the absence of symptoms. 11 Consequently, the use of both dry and cycloplegic refractions prior to refractive surgery has become more widespread, as it aids in improving surgical outcomes. In cases where there is a discrepancy between the two, a “pushing plus” technique is frequently employed to guide treatment.12–13 However, when a disparity persists, it may be unclear which refraction should be the basis for surgical planning. This uncertainty is particularly pronounced when the difference between dry and cycloplegic refractions exceeds 1D.11–12 Such cases often require reevaluation, and their management is controversial. 12
Based on clinical observations, we hypothesized that a clinically significant difference between dry and cycloplegic refraction may increase the likelihood of retreatment in myopic patients. Therefore, the aim of this study was to compare laser refractive retreatment rates between myopic patients who exhibited a significant cycloplegic refraction difference and those who did not.
Materials and methods
All data for the study were collected and analyzed in accordance with the policies and procedures of the Institutional Review Board of the E. Wolfson Medical Center (IRB no. 0188-19-WOMC) and the tenets set forth in the declaration of Helsinki.
Study participants
This retrospective study included consecutive patients who underwent LASIK or PRK between January 2005 and December 2019 at Care-Vision Laser Centers, Tel-Aviv, Israel. Inclusion criteria were ages 17 to 50 years; a stable refraction for at least 12 months; IOP less than 21 mm Hg; a period without wearing contact lenses (more than 2 weeks for rigid contact lenses and more than 4 days for soft contact lenses); and no history of autoimmune disease, diabetes or previous ocular surgery. Included in the analysis were patients with myopia (spherical equivalence <=-0.50D). Since the variance between eyes is usually less than that between subjects, the overall variance of a sample of measurements combined from both eyes is likely to underestimate the true variance. Therefore, if both eyes met the inclusion criteria, one eye was randomly selected. 14 Only patients targeted for emmetropia were included in this study, eyes that were treated for monovision were excluded.
Data collection
The medical files of all eligible patients were reviewed and the following demographic and preoperative information were extracted: age, gender, date of surgery, central corneal thickness (CCT) measured by ultrasonic pachymetry (Sonomed Escalon, NY, USA), preoperative manifest sphere, preoperative manifest cylinder, preoperative cycloplegic sphere, preoperative cycloplegic cylinder, mean keratometric power, minimum keratometric power (Kmin), maximum keratometric power (Kmax), Kaxis (against, oblique or with the rule), uncorrected visual acuity (UCVA) and best corrected visual acuity (BCVA). The following intraoperative information was extracted: optical zone, treatment type (LASIK or PRK), laser model (WaveLight EX200 or EX500, Alcon, Fort Worth, TX), maximum ablation depth and the involved eye (right or left).
Cycloplegic different and similar groups
Cycloplegic refraction measurements for both eyes were attained 30 min after instillation of one drop of 1% tropicamide (Mydramide) into each eye of participants. The cycloplegic effect of tropicamide has been shown to be similar to cyclopentolate with minimal difference in the magnitude of residual accommodation when measured by objective methods.15–16 Eyes which had a hyperopic shift of 0.50D or more (e.g., went from a spherical equivalence of −3.00D to −2.50D following cycloplegia) were categorized as “Cycloplegic Different” whereas all other eyes were categorized as “Cycloplegic Similar”.
Surgical technique
All patients underwent either LASIK or PRK in a similar manner as previously described by our group with the common practice of performing PRK when CCT was below 500 µm.7,17–18 Patients were encouraged to return for examination if vision deteriorated at any time after surgery, and laser enhancement procedures were offered free of charge at any time point after surgery. Criteria for retreatment were stable refraction for a period of at least 6 months and UCVA that was at least 1 line worse than BCVA. Briefly, topical anesthetic (benoxinate hydrochloride 0.4%) was instilled prior to surgery, after which a lid speculum was inserted. In LASIK cases, a Moria microkeratome with a thickness plate of 90 microns was used to create the flap and in PRK cases, epithelial removal was performed either manually, using alcohol delamination or with transepithelial PRK. 19 Following flap creation (LASIK) or epithelial removal (PRK), either the WaveLight® EX200 or EX500 excimer laser system was used. In all PRK cases, following ablation, a sponge soaked with 0.02% mitomycin C was placed on the stroma for 20–60 s (depending on the amount of ablation), and a contact lens was placed after rinsing the mitomycin C. Following surgery, patients were prescribed moxifloxacin 0.5% four times daily, dexamethasone 0.1% either twice or four times daily, and artificial tears four times daily. Patients were examined at the 1 day, 1 week, 1-, 3- and 6-months post operatively and thereafter as needed.
Statistical analysis
Data were analyzed using Minitab Software, version 17 (Minitab Inc, State College, PA). For the analysis of continuous data, Student's t-test was used for normally distributed variables and Kruskal-Wallis for non-parametric variables. For the analysis of categorical variables, Chi-Square or Fishers’ exact test were used and when applicable, odds ratio values were calculated. Finally, a stepwise binary logistic regression analysis was performed to account for potential confounders of retreatment. For this purpose, independent variables that reached a significance level of <0.05 in univariate analysis were included. In all analyses, a two-sided P value <0.05 was considered statistically significant. All presented means are accompanied by their respective standard deviations.
Results
Throughout the study period, 103,730 primary laser refractive procedures were performed, of which 28,780 eyes met the inclusion criteria. After randomly selecting one eye per patient, 14,679 eyes were included in the final analyses. The age of the participants was 27.4 ± 7.8 years and 53.2% were male.
Preoperative comparison between groups
Of the 14,679 eyes included 1,458 (9.9%) were cycloplegic different (difference ≥ 0.50D) and 13,221 eyes (90.1%) were cycloplegic similar. Table 1 depicts a comparison of preoperative parameters between both groups. Briefly, the cycloplegic different group had a higher proportion of males (p = 0.03), was of older age (p < 0.001), had a thinner central corneal thickness (p = 0.004), steeper corneas (p < 0.001), worse BCVA (p < 0.001), higher SEQ (p < 0.001) and a higher proportion of patients with an astigmatism larger than 1.00D (p < 0.001).
Comparison of preoperative variables between groups**.
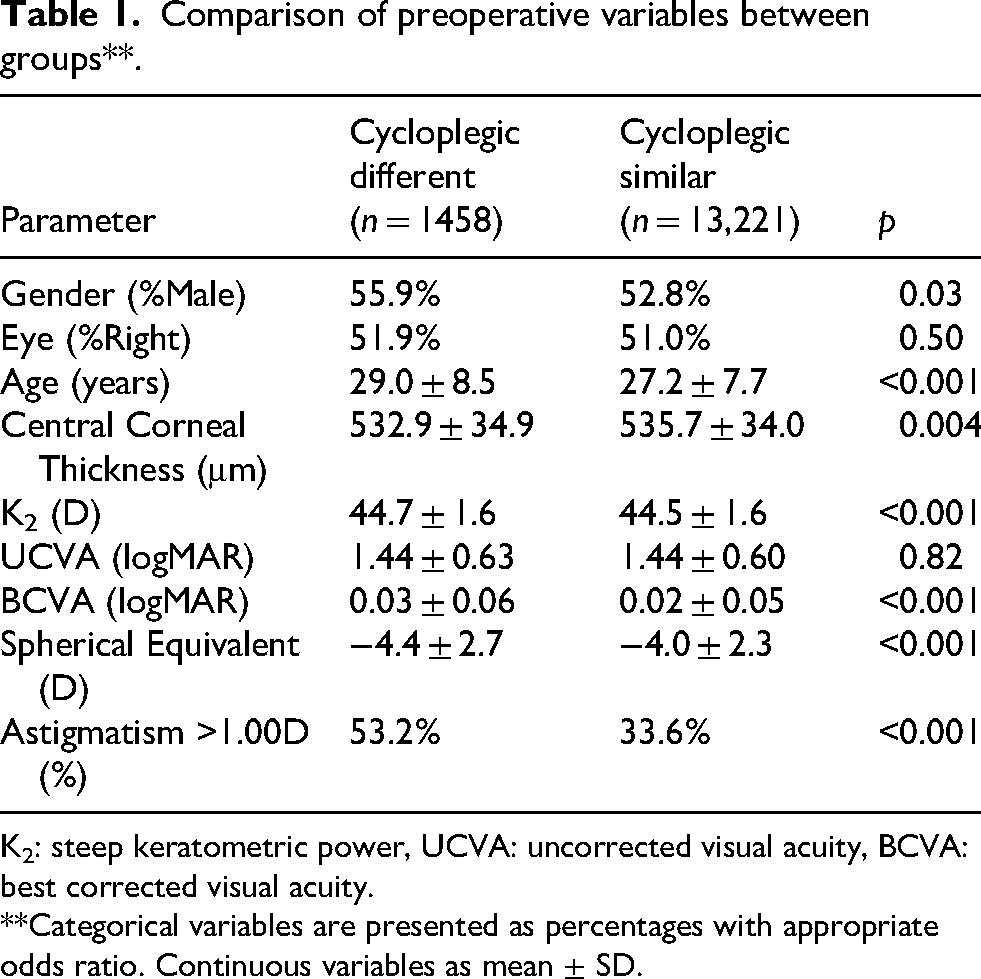
K2: steep keratometric power, UCVA: uncorrected visual acuity, BCVA: best corrected visual acuity.
**Categorical variables are presented as percentages with appropriate odds ratio. Continuous variables as mean ± SD.
A detailed distribution of cycloplegic spherical equivalent (SEQ) differences and their association with retreatment among eyes demonstrating a cycloplegic difference of ≥0.50 D (as predefined in the study criteria) is presented in Table 2. Retreatment rates were low across all categories and were not correlated with increasing magnitude of cycloplegic difference; no retreatments occurred in eyes with differences exceeding 1.0 D.
Distribution of cycloplegic SEQ differences and retreatment rates.
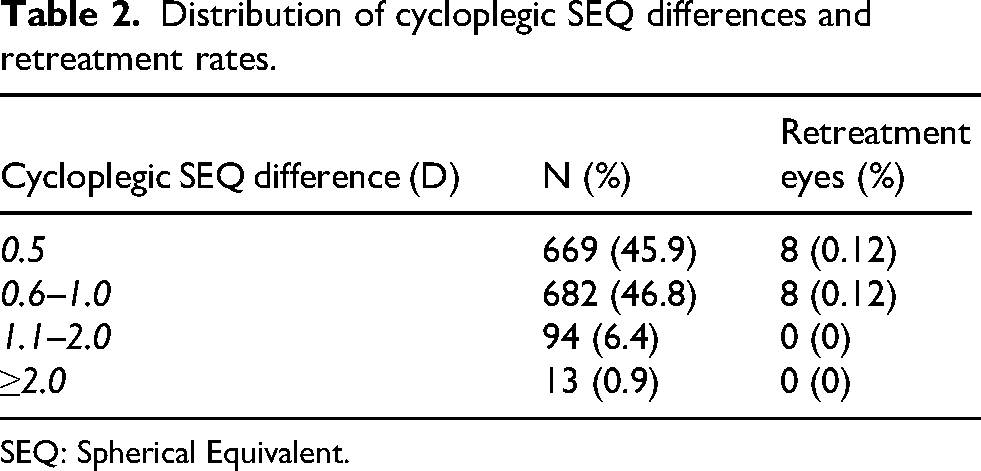
SEQ: Spherical Equivalent.
Intraoperative comparison between groups
Table 3 depicts a comparison of intraoperative parameters between groups. Briefly, the cycloplegic different group had a lower proportion of patients with a large treatment optic zone (p < 0.001), greater proportion of PRK (p < 0.001), smaller proportion of patients operated on with the EX200 (vs EX500) (p < 0.001) and had a significantly larger maximum ablation depth (p < 0.001).
Comparison of intraoperative variables between groups*.
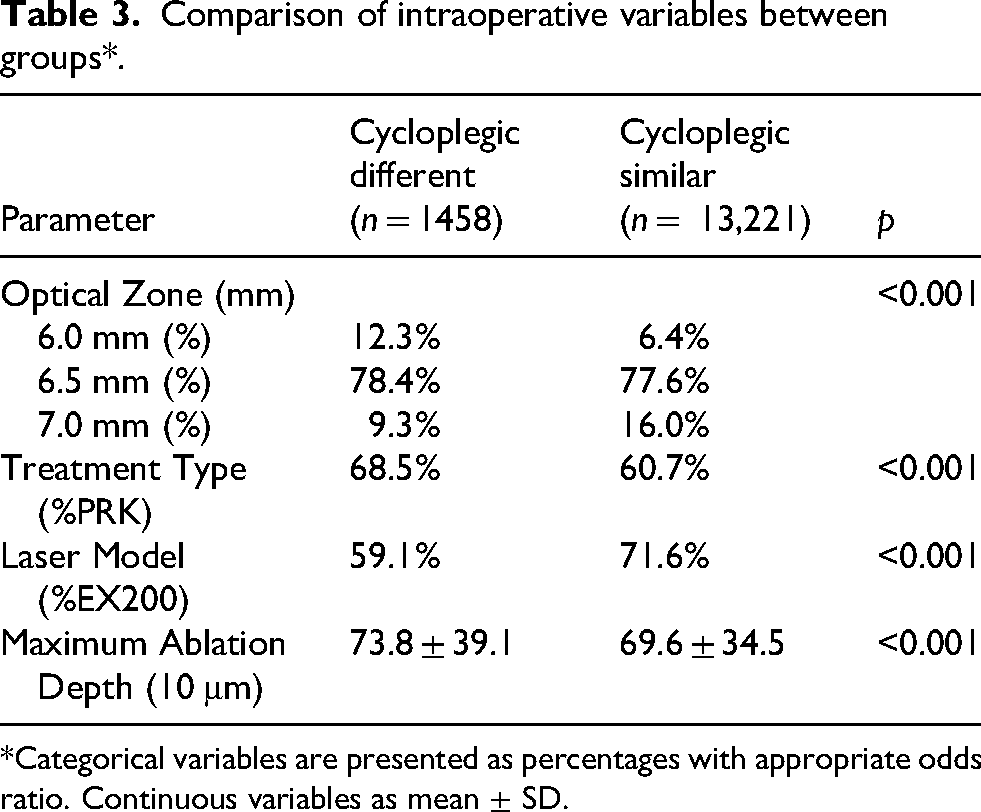
*Categorical variables are presented as percentages with appropriate odds ratio. Continuous variables as mean ± SD.
Retreatment surgeries
Overall, 0.62% (n = 91) of eyes of 91patients underwent retreatment. The interval time between initial treatment and the retreatment was 858.9 ± 810.5 days. Pre-retreatment SEQ was −0.80 ± 1.31 D and post-retreatment SEQ was −0.15 ± 0.43 D, representing a meaningful improvement, with 71.4% of eyes demonstrating improved SEQ (p = 0.015). Table 4 described the retreatment information and outcomes.
Retreatment outcomes.
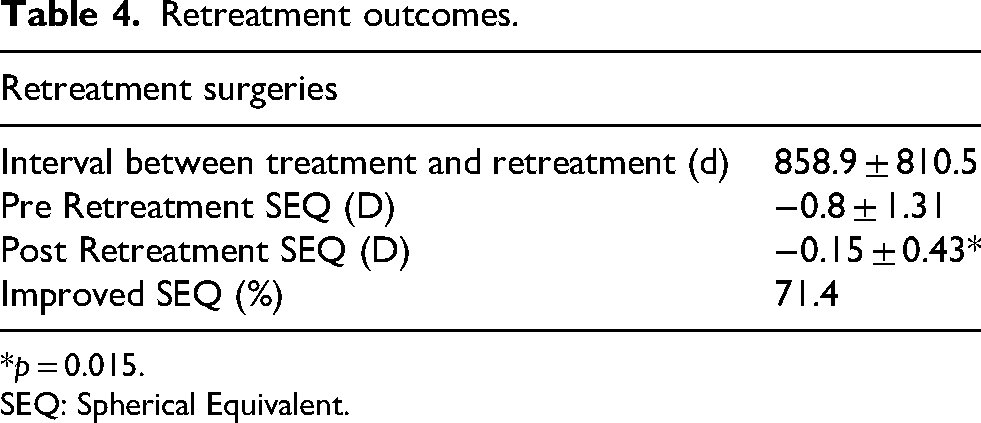
*p = 0.015.
SEQ: Spherical Equivalent.
Comparison of retreatment rates between groups
The cycloplegic different group had a significantly greater retreatment rate (1.10% versus 0.57%, p = 0.01) and eyes which demonstrated a cycloplegic difference were 1.94 times more likely (95% CI 1.13 to 3.35) to undergo retreatment. In stepwise binary logistic regression analysis, after accounting for potential confounders (all variables that were p < 0.05 in univariate analysis), cycloplegic difference remained a significant predictor of retreatment (OR = 1.80, 95% CI 1.01–3.18, p = 0.04).
Discussion
Refractive surgery retreatment rates are an important indication of real-world surgical efficacy. Therefore, identifying and understanding risk factors for retreatment is an important task. Preoperative dry and cycloplegic refraction are the basis for refractive surgery planning, 20 and in cases where there is significant discrepancy between the two, surgical planning is challenging and controversial.10–11 This study compared retreatment rates between patients who demonstrated clinically significant cycloplegic differences and those who did not. Patients with a clinically significant cycloplegic difference demonstrated higher retreatment rates both in univariate analysis (OR = 1.94) and in multivariate analysis (OR = 1.80) after accounting for potential confounders. To the best of our knowledge, this is the largest study to date to investigate and compare cycloplegic and dry refraction prior refractive surgery.
Cycloplegic and dry refraction may differ among a significant portion of refractive surgery patients, some presenting with significantly large differences. The importance of performing both refraction methods has been extensively described in published literature, especially so among young individuals since they hold inherently large accommodative potential.21–23 Interestingly, in the current study, the Cycloplegic Different group was slightly older with age difference between the groups not being of clinically significant magnitude. This implicates other factors to be more significant contributors to the increased accommodative tone seen in the Cycloplegic Different group.
Hashemi et al. investigated the difference between cycloplegic and dry refraction among more than 3400 patients showing a mean difference of 0.52 to 0.89 D (95% Limits of Agreement) between the two methods among myopic patients. Frings et al. investigated the preoperative cycloplegic refraction of 186 hyperopic LASIK eyes, and found that in 13% of cases, there was a difference larger than 1.00D. 11 In our study, we found that the vast majority of patients (90.1%) had a difference of less than 0.50D.
A large difference between cycloplegic and non-cycloplegic refraction is usually correlated with younger age, hyperopia, and according to some reports, among those of Hispanic descent.23–25 A large accommodative tone may also be more common among individuals with anisometropia and those with low-grade myopia.26–28 In hyperopia, a larger accommodative tone is present to induce manifest myopization and reduction of the hyperopic refractive error. In patients with anisometropia, accommodation may be the result of a reflective attempt to compensate for the refractive difference between both eyes.29–30 An accommodative spasm may also be present as a fusion mechanism in certain tropias. Also, chronic spectacle over-myopization may lead to a chronically increased accommodative tone. Although there are several scenarios and mechanisms leading to an increased accommodative tone, in some cases there is no apparent cause for this finding. Refractive surgery candidates presenting with an increased difference between cycloplegic and dry refraction undergo repeat strabismus evaluation and a repeat dry refraction to try and “push plus” (reduce minus) in order to approximate their dry refraction to their cycloplegic refraction. Some surgeons conduct a slow “over minus” withdrawal by prescribing temporary spectacles of a more hyperopic prescription with repeat evaluations and prescription tuning until refraction stabilizes. These measures may reduce the number of refractive surgery patients undergoing surgery while having an increased accommodative tone.
Retreatment was performed in 0.62% of eyes and was associated with a meaningful improvement, with 71.4% of eyes demonstrating improved SEQ (p = 0.015). Importantly, increasing magnitude of cycloplegic SEQ difference was not associated with higher retreatment rates, suggesting that the observed cycloplegic discrepancies were not clinically significant in terms of residual refractive error or regression.
The importance of performing both cycloplegic and dry refraction prior to refractive surgery is considered common knowledge. Surprisingly, there is little published data available on refractive surgery outcomes and their association with cycloplegic and dry refraction differences. Frings et al. found in their hyperopic cohort that with increasing cycloplegic difference, hyperopic regression occurred 3 months following surgery. 11 Our study demonstrated a similar trend of higher retreatment rate among patients with larger cycloplegic differences. These results stress the importance of performing both refraction techniques prior to refractive surgery. Given these findings, we recommend careful reevaluation and surgical planning among patients who demonstrate a cycloplegic difference of more than 0.50D.
This study has several limitations, the first being its retrospective nature. Second, Tropicamide was used as a cycloplegic agent and not Cyclopentolate, which is considered a stronger cycloplegic agent. Third, the study groups demonstrated some baseline differences, however this was accounted for in multivariate analysis. Future studies could attempt to produce nomograms accounting for cycloplegic differences in order to optimize outcomes.
In conclusion, a difference of 0.50D or more between cycloplegic and dry refraction is associated with increased risk for future retreatment. Such cases require careful reevaluation and planning. Patients and physicians should be aware of the higher likelihood of retreatments in this scenario.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.