
Abstract
Purpose
To characterize the spatiotemporal patterns of vascular remodeling following pterygium excision with amniotic membrane transplantation (AMT) using optical coherence tomography angiography (OCTA).
Methods
This observational study evaluated 43 eyes undergoing AMT. Serial OCTA imaging was performed over a 12-week postoperative period to quantify vascular dynamics in superficial and deep conjunctival layers. Quantitative parameters, including vessel density (VD), vessel length density (VLD), and vessel diameter index (VDI), were analyzed using automated image processing techniques.
Results
Early assessment at Week 1 showed minimal vascular in-growth. By Week 4, progressive remodeling was evident, primarily driven by deep-layer anastomoses between host tissue and the graft area. By Week 12, a structured vascular network emerged; however, superficial perfusion remained significantly reduced compared to baseline. While deep-layer VD demonstrated substantial recovery, VDI remained statistically stable. Notably, OCTA identified persistent flow voids and heterogeneous perfusion, suggesting irregular host-derived vascular integration beneath the graft.
Conclusion
Post-AMT healing is mediated predominantly by deep-layer episcleral vascular remodeling. OCTA serves as a sensitive, non-invasive tool for monitoring subclinical vascular integration, offering potential biomarkers for surgical success and early pterygium recurrence.
Introduction
Pterygium, a prevalent ocular surface disorder, is marked by a fibrovascular overgrowth extending onto the cornea, often leading to astigmatism, tear film disruption, or direct obstruction of the visual axis, thereby impairing vision.1,2 Although surgical excision remains the definitive treatment, postoperative recurrence and complications persist as clinical challenges. Advanced techniques, including conjunctival autograft (CAG) and amniotic membrane transplantation (AMT), have significantly reduced recurrence rates and complication ratescompared to the bare sclera technique.3,4
AMT is highly valued in ocular surgery for its anti-inflammatory, anti-fibrotic, and epithelial-promoting properties. 5 Because the amniotic membrane is inherently avascular, its clinical success depends on its integration with the recipient site rather than on its own vascularization. Consequently, vascular remodeling of the underlying host tissue is essential for providing the metabolic support and inflammatory control necessary for sustained epithelialization.6,7
Characterizing these postoperative vascular patterns is vital for monitoring the healing process and detecting early signs of graft failure or inadequate perfusion. Furthermore, quantifying vascular changes may provide insights into the mechanisms underlying pterygium recurrence, potentially guiding refinements in surgical approach and postoperative care. 8 Traditionally, monitoring sub-graft vascularization has been limited by a lack of high-resolution imaging. 9 While Indocyanine Green Angiography (ICGA) can assess functional perfusion and vessel maturity, its clinical utility is hindered by its invasive, dye-based nature. 10
Optical coherence tomography angiography (OCTA) has emerged as a non-invasive alternative, providing high-resolution, depth-resolved imaging of microvascular networks. 11 Although primarily utilized for posterior segment evaluation, recent technical adaptations—including improved resolution and motion artifact reduction—have optimized OCTA for corneal and limbal anatomy.11–15 Recent evidence suggests that OCTA can effectively track host-derived vascular dynamics and elucidate healing mechanisms following ocular surface surgery. 16
Accordingly, this study aims to quantify early postoperative vascular remodeling at the AMT surgical site following pterygium excision. By utilizing OCTA to measure vascular density (VD), vessel length density (VLD), and vessel diameter index (VDI), we sought to enhance understanding of host-tissue integration and provide a quantitative basis for optimizing postoperative outcomes.
Methods
Study design and ethical considerations
This prospective observational case series was conducted at Farabi Eye Hospital, Tehran, Iran. The study adhered to the Declaration of Helsinki and received ethical approval from the Institutional Review Board of Tehran University of Medical Sciences (IR.TUMS.FARABIH.REC.1402.004).All participants were informed of the study's purpose and alternative treatment options, and written informed consent was obtained from all patients prior to enrollment.
Patients and preoperative evaluation
Forty-three eyes of 43 patients with primary pterygium were enrolled. Indications for surgery included visual impairment or cosmetic concerns. Exclusion criteria consisted of severe dry eye, systemic disease, contact lens use, inability to complete imaging, and a history of previous ocular surface surgery. Preoperative assessments included visual acuity testing, slit-lamp and fundus examinations, and baseline clinical photography.
OCTA imaging technique
OCTA imaging was performed using the AngioVue system (RTVue XR 100 Avanti, Optovue, Inc., Fremont, CA, USA) utilizing the split-spectrum amplitude-decorrelation angiography (SSADA) algorithm. Sessions were conducted at baseline (one week preoperatively) and at 1, 4, and 12 weeks postoperatively.
To optimize imaging of the anterior segment, the autofocus function was disabled, and XYZ focal settings were manually adjusted until the desired vascular structures were clearly visualized. The system utilized an 840 nm light source, achieving an axial resolution of 5 µm, a beam width of 22 µm, and a penetration depth of 2.3 mm. A 3D scan cube was constructed from B-scans comprising 304 × 304 A-scans acquired at 70,000 scans per second. Three scans were performed per session for each patient; the image with the highest signal strength and minimal noise was selected for analysis.
Images were segmented into superficial (epithelium to 200 µm depth) and deep layers (beyond 200 µm) in the nasal quadrant, following the methodology described by Akagi et al. 14 representative superficial and deep en face OCTA images, alongside corresponding slit-lamp photographs, are illustrated in Figure 1.
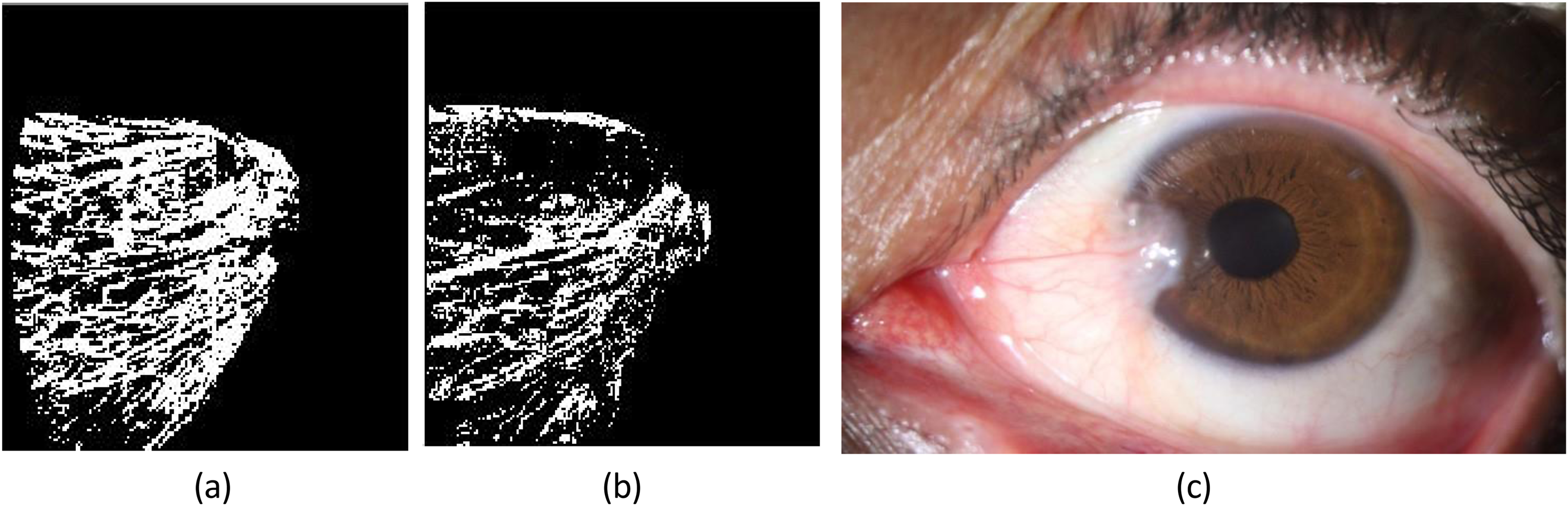
Preoperative imaging of a 40-year-old male patient with pterygium. (a) Superficial en face optical coherence tomography angiography (OCTA) image of conjunctival vessels in the pterygium region, demonstrating straightened and displaced vascular patterns. (b) Deep en face OCTA image revealing prominent, large-caliber, straightened, and dragged vessels within deeper ocular surface layers. (c) Slit-lamp photograph illustrating the clinical appearance of the pterygium.
Quantitative and qualitative analysis
High-quality OCTA scans were processed using internal software (ReVue4.0; Optovue, Inc.) to reduce motion artifacts, including transverse saccadic and axial motion errors. Additional processing was performed via ImageJ (National Institutes of Health, Bethesda, MD, USA) to correct horizontal artifacts caused by involuntary ocular movements. 17
A 6 × 6 mm AS-OCTA scan was acquired for each subject to capture en face images of the superficial and deep vascular layers. Quantitative measurements were performed on separately segmented images using MATLAB R2022a. To mitigate artifacts and enhance vessel contrast, contrast-limited adaptive histogram equalization (CLAHE) and median filtering were applied to grayscale images.
To ensure precise quantification, the region of interest (ROI) was defined as the exact area of the pterygium excision, corresponding to the site of the AMT graft. Delineation was performed manually on the en face infrared (IR) reflectance images rather than flow-based OCTA maps, as IR reflectance provides superior structural contrast for identifying the surgical margins and graft boundaries. To minimize inter-operator variability and ensure internal consistency across the longitudinal dataset, all ROI selections were performed by a single experienced observer. However, we acknowledge that manual ROI delineation remains an inherently operator-dependent process.
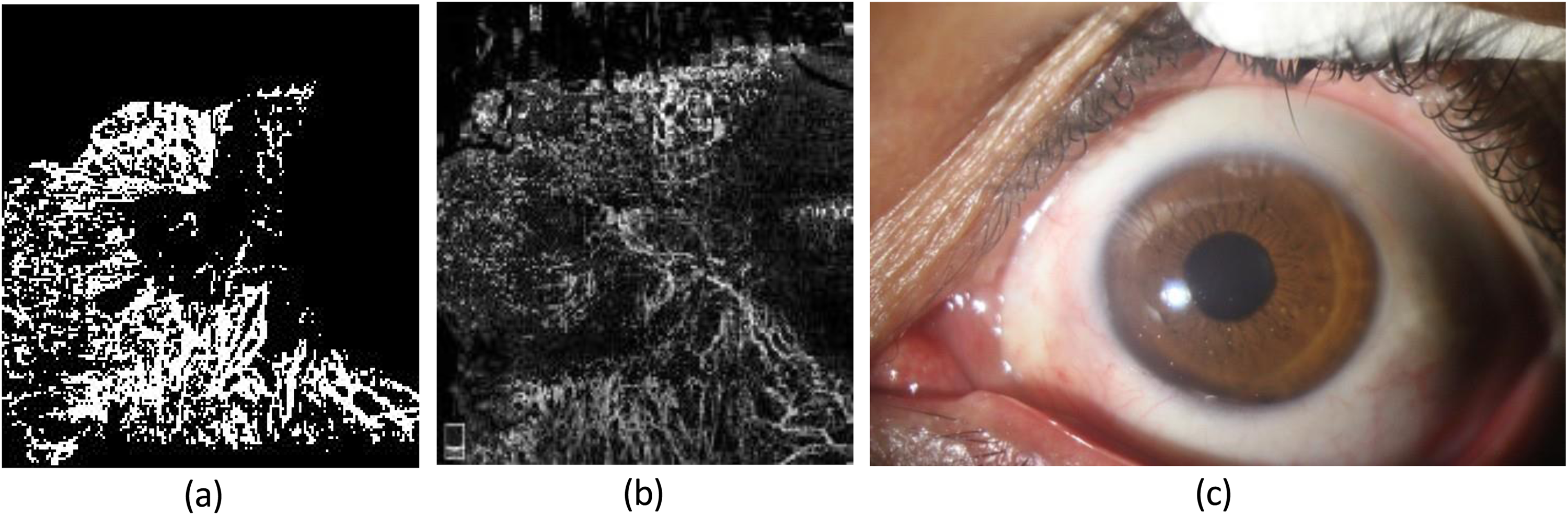
The Otsu thresholding method was utilized to binarize grayscale images, effectively isolating vessels by selecting a threshold that minimizes intra-class variance. Skeletonization techniques were then employed to calculate vessel length. These steps—from raw OCTA (a) to binarized (b) and finally skeletonized (c) images—are illustrated in Figure 2. Quantitative parameters were calculated within the ROI using methodologies previously validated in OCTA literature:18,19
Vessel Density (VD): Calculated as the ratio of the area occupied by perfused vessels (binarized pixels) to the total ROI area. It represents the total surface area of blood flow within the graft. Vessel Length Density (VLD): Calculated as the total length of the vascular network (derived from skeletonized images) normalized to the ROI area. This metric reflects the linear extent and branching complexity of the vessels. Vessel Diameter Index (VDI): Calculated by dividing the total vessel area (from binarized images) by the total vessel length (from skeletonized images). This serves as a surrogate for average vessel caliber, allowing for the detection of changes in vessel thickness independent of density.
18
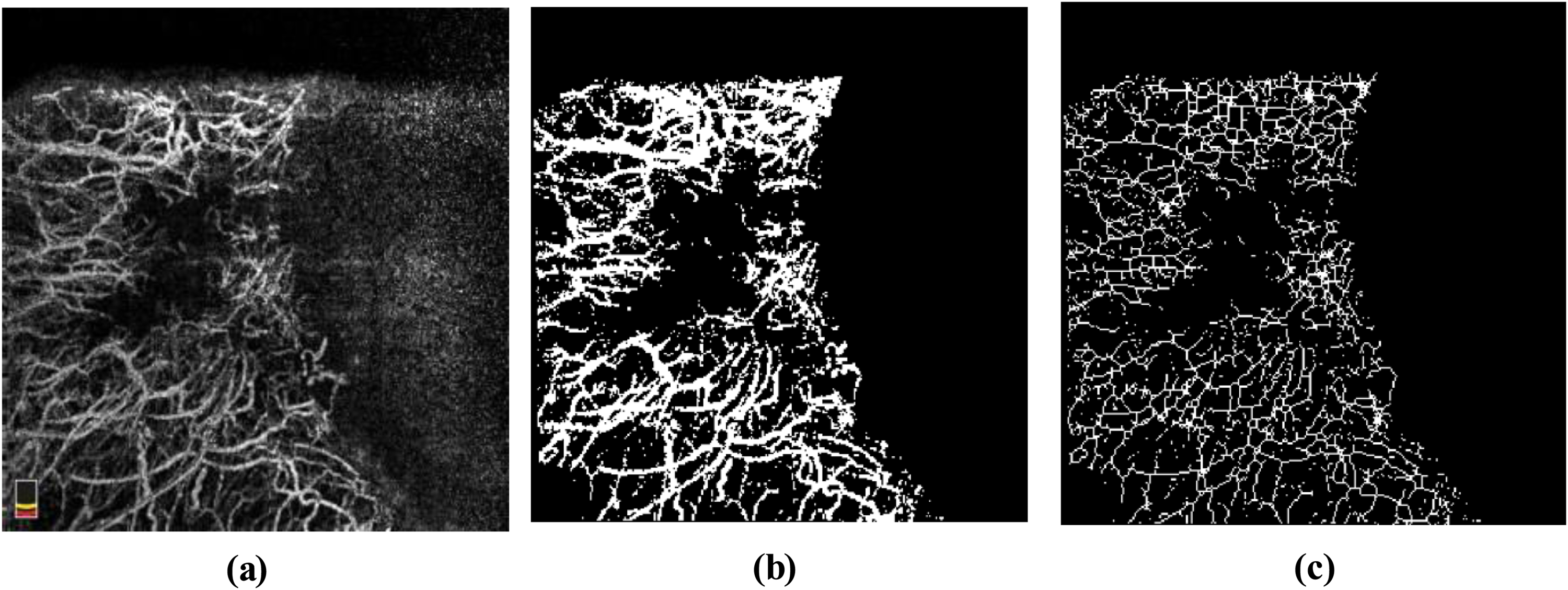
Image processing workflow. (a) Raw OCT scan. (b) Preprocessed and binarized image within the AMT graft ROI using CLAHE and Otsu thresholding. (c) Skeletonized vessel map used for length quantification.
Surgical technique and postoperative management
Local anesthesia was administered via sub-Tenon's injection of 0.5–1.5 ml of 2% lidocaine using a 26-gauge needle. The eye was prepared using sterile techniques and held open using a wire speculum. To minimize inter-operator variability, all surgical procedures were performed by a single expert ophthalmologist using a standardized technique. The pterygium body was excised at the limbal plane, and the head was removed from the cornea using blunt Westcott scissors. Tenon's tissue and episcleral fibrosis were meticulously excised to minimize risk of recurrence. Residual corneal tissue was cleared using a Beaver blade.
The amniotic membrane (AM), obtained from cryopreserved or lyophilized samples on a cellulose nitrate filter, was positioned with the epithelial side facing upward. AM was secured to surrounding conjunctiva using 10-0 nylon sutures.
Postoperative management included betamethasone drops (1 drop every 4 h, tapered over 6 weeks), ciprofloxacin drops (1 drop every 6 h, continued until bandage lens removal), and lubricants (6 times daily for 4 weeks). Bandage lenses were removed upon complete corneal epithelialization (typically within one week), and sutures were removed after 3–4 weeks once graft stability was confirmed.
Statistical analysis
Data were analyzed using SPSS v27.0 (IBM, USA). Longitudinal changes were assessed using linear mixed models to account for repeated measures, with Sidak correction applied for multiple comparisons. A p-value < 0.05 was considered statistically significant.
Results
Patient demographic and baseline characteristics
Forty-three eyes of 43 patients (34 males [79.06%] and 9 females [20.93%]) with primary pterygium underwent surgical excision with the AMT technique. The mean age of the patients was 38 years (range, 22–54 years). While 43 patients were initially enrolled, five patients were lost to follow-up and were excluded from the longitudinal analysis. No significant intraoperative or immediate postoperative complications were observed.
Qualitative clinical and OCTA observations
First postoperative week
During the first postoperative week, the vascular network within the surgical site was poorly defined, with no detectable vascular integration between the host tissues and the amniotic membrane. Limbal vascular loops were absent in the excised region, and the area exhibited mild, transient graft swelling. These findings, illustrated in Figure 3, highlight reduced vascular signals on OCTA corresponding to the early stages of clinical healing.
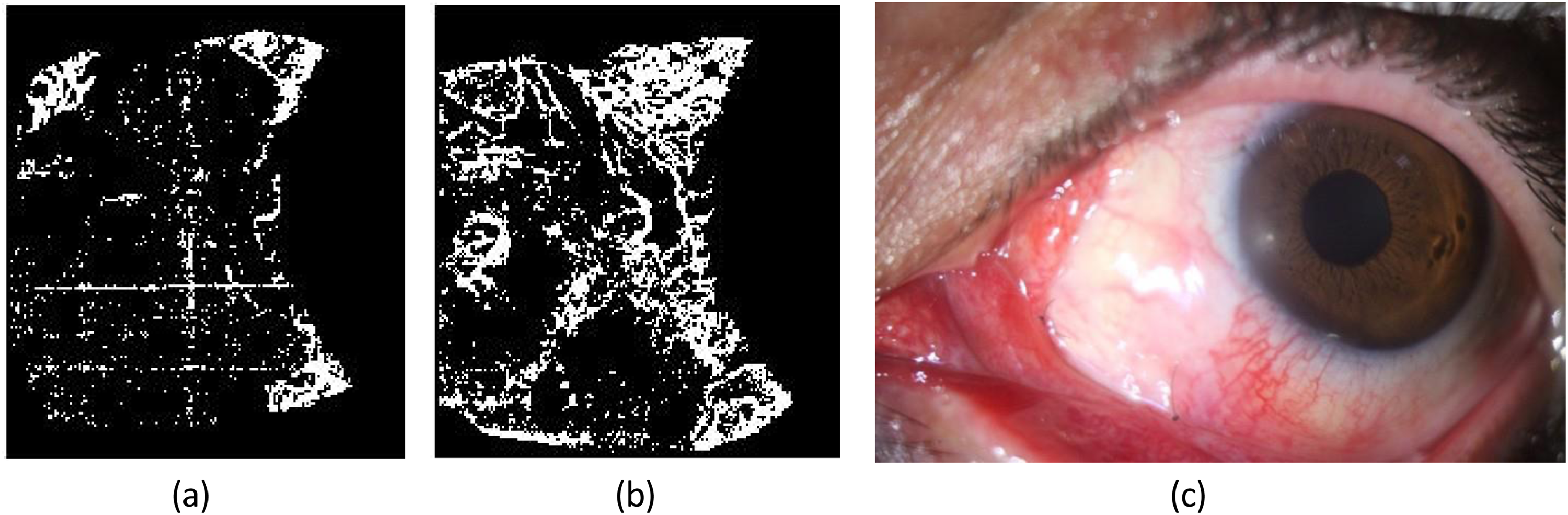
Postoperative evaluation one week after pterygium excision with amniotic membrane transplantation in the same patient. Left to right: (a) Superficial en face OCTA image demonstrating a relative absence of vascular signals within the graft area; (b) Deep en face OCTA image showing vascular quiescence and abrupt termination of vessels at the graft margin. The episcleral vessels are observed running beneath the amniotic membrane graft; (c) Slit-lamp photograph indicating early healing with mild conjunctival injection.
Fourth postoperative week
By the fourth week, a reduction in the initial transient graft edema allowed improved visualization of the underlying vascular structures. Fine vascular anastomoses began to form between the host conjunctiva and the AMT graft site, primarily within the deeper layers. Large-caliber vessels exhibited a segmental pattern and appeared to connect with the episcleral bed. Apparent non-perfusion zones were observed in areas of intragraft hemorrhage; however, these likely represented masking artifacts due to signal attenuation from overlying blood rather than true vascular absence. Figure 4 demonstrates this progressive host-derived vascular remodeling on OCTA and improved conjunctival clarity with successful graft integration on slit-lamp examination.
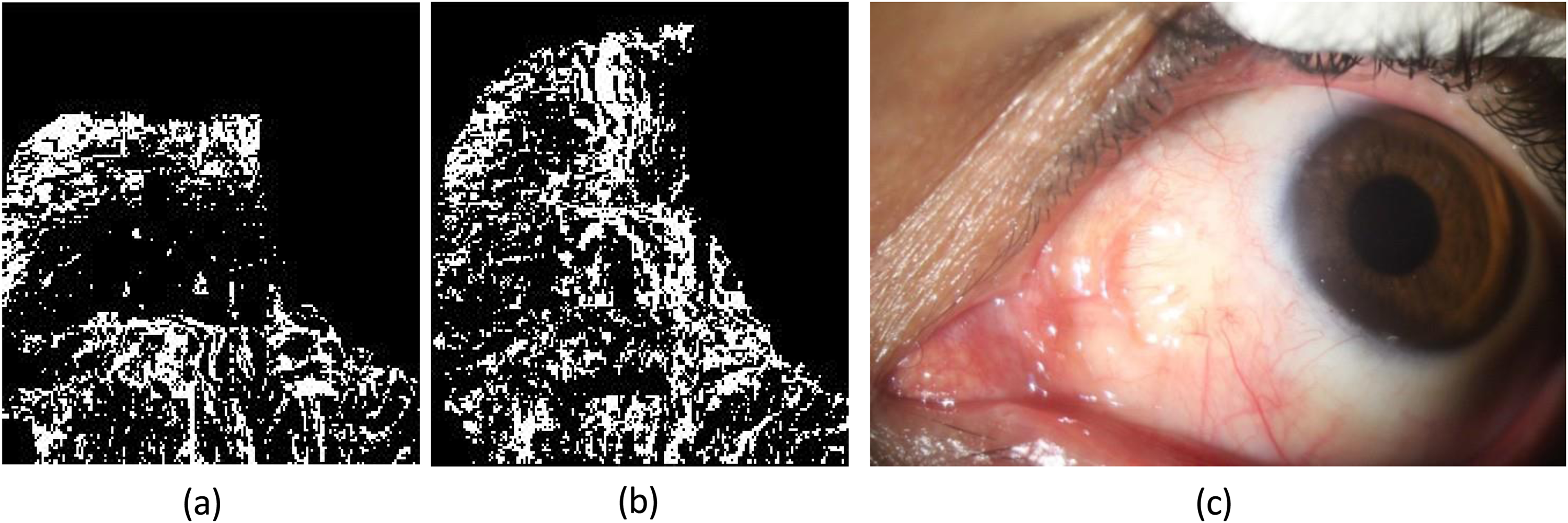
Postoperative assessment at 1 month. (a) Superficial en face OCTA image demonstrating revascularization at the site of pterygium excision, originating from the excision margins; (b) Deep en face OCTA image revealing a well-developed vascular network, with complete anastomosis between the surrounding conjunctival vessels and those within the excision area;(c) Slit-lamp photograph showing enhanced conjunctival clarity and successful graft integration. A blanched area is noted at the site of excision, corresponding to a region of relative vascular absence observed in the superficial en face OCTA image.
Twelfth postoperative week
At the three-month follow-up, the vascular network demonstrated increased density and interconnectivity, particularly in the deep layers. Robust anastomotic connections were established at the junction of the host conjunctiva and the excision site, with vessels clearly extending from the underlying episclera. Although the network appeared stable, flow patterns remained irregular compared to the healthy surrounding conjunctiva, with persistent focal flow voids, these findings are illustrated in Figure 5.
Postoperative assessment at 3 months. (a) Superficial en face OCTA image demonstrating a mature and established vascular network, with vessels extending centripetally toward the center of the pterygium excision site;(b) Deep en face OCTA image confirming well-established revascularization within the deeper vascular plexus; (c) Slit-lamp photograph revealing a stable ocular surface.
Quantitative assessment of vascular biomarkers
The quantitative analysis revealed significant increases in VD and VLD over the 12 week-follow-up period in both the superficial and deep layers (p < 0.05).
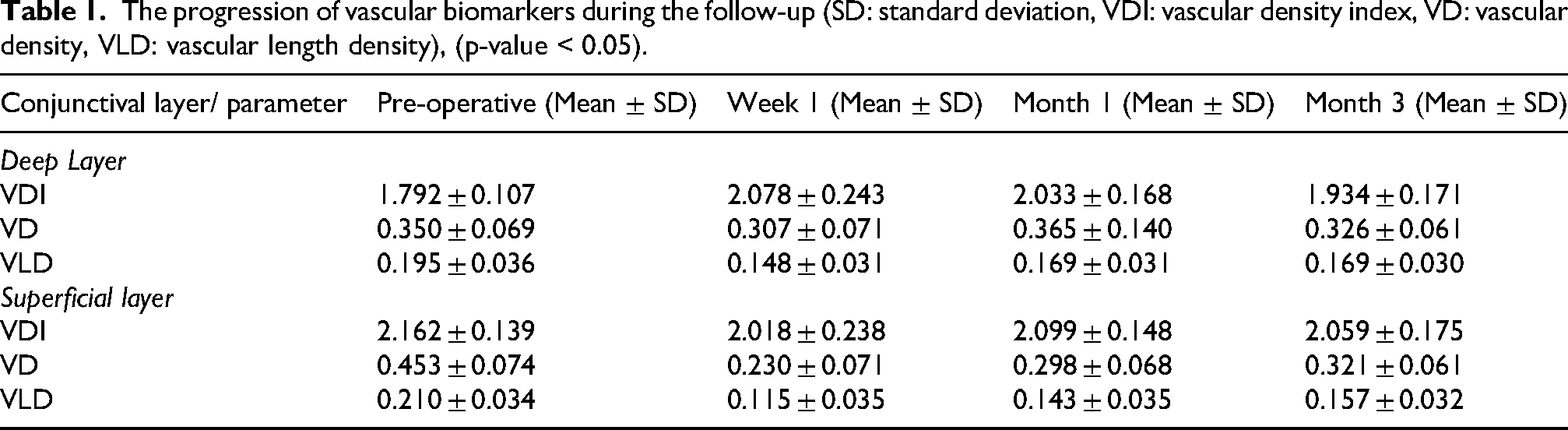
Deep layer VD: The preoperative baseline VD was 0.350 ± 0.069(p < 0.05). At Week 1, VD significantly decreased to 0.307 ± 0.071(p < 0.05), reflecting the absence of perfused host conjunctival vasculature within the pterygium excision site. By Month 1, VD recovered to 0.365 ± 0.140 (p > 0.05 vs. baseline) and remained stable at Month 3(0.326 ± 0.061, p > 0.05 vs. baseline). Superficial layer VD: This layer showed a more pronounced initial decline, dropping from a baseline of 0.453 ± 0.074 to 0.230 ± 0.071 at Week 1 (p < 0.001). While gradual recovery was observed at Month 1(0.298 ± 0.068) and stabilization at Month 3 (0.321 ± 0.061), superficial VD did not return to pereoperative levels by the end of the study(p < 0.05). VLD: In the deep layers, VLD significantly decreased from 0.195 ± 0.036 at baseline to 0.148 ± 0.031 at Week 1 (p < 0.05), returning to near-baseline values by Month 1(0.169 ± 0.031, p < 0.05). Similarly, superficial VLD declined sharply from 0.210 ± 0.034 to 0.115 ± 0.035 at Week 1 (p < 0.001) and, despite recovering to 0.157 ± 0.032 by Month 3, remained significantly lower than baseline (p < 0.05). VDI: In contrast to density metrics, changes in VDI were not statistically significant throughout the follow-up period (p = 0.545) The longitudinal progression of vascular biomarkers during the follow-up is summarized in Table 1.
The progression of vascular biomarkers during the follow-up (SD: standard deviation, VDI: vascular density index, VD: vascular density, VLD: vascular length density), (p-value < 0.05).
Discussion
This study utilized OCTA to characterize postoperative vascular remodeling at the surgical site following pterygium excision with AMT. By providing depth-resolved imaging, OCTA enabled longitudinal tracking of host-derived vascular patterns at 1, 4, and 12 weeks postoperatively. While prior studies have highlighted OCTA's potential for tracking vascular changes in ocular tissues, 20 our findings specifically elucidate the dynamics of host-tissue integration beneath an avascular graft.
A key finding was the emergence of irregular or “chaotic” vascular patterns in a subset of patients. These patterns represent novel morphological observations; however, their role as clinical predictors remains speculative given the 12-week follow-up and lack of recurrence data. 21 Despite evidence of progressive vascularization and interconnectivity, OCTA consistently revealed persistent flow voids. These irregularities may stem from surgical trauma, localized fibrovascular proliferation, or dysregulation of angiogenic mediators such as VEGF and MMPs.22,23 Furthermore, the gradual resorption of the amniotic membrane over weeks to months may itself contribute to these transiently chaotic vascular patterns. 24
Beyond the observed remodeling patterns, the persistence of residual vessels following surgical excision may significantly contribute to recurrence by functioning as structural scaffolds for aberrant angiogenesis. These vascular remnants are known to release pro-inflammatory mediators that may impede host-tissue integration beneath the amniotic membrane and facilitate fibrovascular proliferation.25,26 This mechanism underscores the importance of careful surgical technique and postoperative monitoring.
It is critical, however, to distinguish biological pathology from optical phenomena. The flow voids and irregular patterns observed—particularly in areas of early postoperative hemorrhage —may be partially attributed to the masking effect. In OCTA, dense structures such as blood or thick fibrovascular tissue attenuate the light signal, causing shadowing in deeper slabs that the software interprets as a lack of flow. 27 Consequently, these regions must be interpreted with caution as potential optical artifacts rather than pathological ischemia.
Comparative analyses indicate distinct vascular behaviors between AMT and conjunctival autografts (CAG). While CAG consistently showed organized vascular networks with lower recurrence rates,16,28 AMT exhibited delayed and irregular host-derived vascular remodeling. This disparity is likely due to the inherently avascular nature and anti-inflammatory properties of the amniotic membrane.20,29 While these properties are beneficial for suppressing acute inflammation, they may also modulate early superficial healing. 30 OCTA data demonstrated that AMT relies predominantly on deep episcleral vascular supply during early healing, whereas CAG displays more structured centrifugal vascular patterns. 31 The irregular remodeling in AMT likely reflects its unique anti-inflammatory properties; however, whether this pattern impacts long-term graft stability necessitates further investigation. 28
Graft swelling, commonly observed during the first postoperative week following CAG, was less pronounced with AMT. 28 This reduced graft swelling allows for improved visualization of the underlying ocular surface vasculature on OCTA. Postoperative complications such as graft edema, necrosis, inclusion cysts, subconjunctival hematoma, Tenon's granuloma, corneal thinning, and Dellen formation have been widely reported using CAG.29,32 These findings emphasize the impact of graft origin on healing, as the absence of intrinsic vasculature in AMT may delay stable vascular integration with the host tissue. 33
No recurrences were observed during the 12-week follow-up. However, longer follow-up (≥12 months) is generally required for accurate assessment of recurrence. 34 Although adjunctive mitomycin C (MMC) may reduce recurrence, its use carries potential complications.35,36 While combined AMT and MMC has shown benefit, 37 MMC was intentionally omitted in this study to preserve physiological healing and avoid confounding OCTA measurements.
By week 4, OCTA revealed fine vascular anastomoses predominantly in deeper layers, emphasizing the role of episcleral vasculature. 31 By week 12, increased VD and VLD suggested progressive vascular maturation, particularly in deeper layers. Given the avascular nature of AMT, these findings likely reflect host-derived epithelial and vascular coverage of the graft. This pattern is consistent with previous studies indicating delayed superficial remodeling. 28 However, persistent irregular vascular patterns in some patients may indicate variability in healing or potential recurrence risk. 20 VDI remained relatively stable, suggesting minimal changes in vessel caliber, although subtle variations cannot be excluded.
The inclusion of multiple vascular indices allowed for a comprehensive biological assessment: while VD and VLD characterize the overall extent and complexity of host-derived revascularization, VDI specifically reflects changes in vessel caliber, helping to distinguish between the maturation of existing vessels and the sprouting of new, finer microvasculature.
OCTA provides a non-invasive method for monitoring vascular remodeling and may help identify features associated with recurrence.16,38,39 Although widely used in conditions like myopia, 40 diabetic retinopathy, 41 glaucoma, 42 and thyroid-associated ophthalmopathy,39,43 its application in evaluation of vascular changes in ocular surface disorders remains limited. Our findings contribute to this emerging field.
This study primarily characterized structural remodeling; a direct correlation between OCTA metrics and clinical findings (e.g., slit-lamp features, symptoms) was not established. Explicit acknowledgment of this absence is essential for the proper clinical contextualization of our results.
Several limitations warrant consideration. A primary limitation is the selection of the preoperative baseline, which was obtained directly from the area affected by the pterygium. Because this region already exhibited abnormal vascular architecture, it serves as a pathologic baseline rather than a normative baseline. This issue is closely linked to the absence of a control group—either in the form of a separate cohort of healthy eyes or a non-pathologic region within the same eye. Without comparison to normal conjunctival microvasculature, it is challenging to determine whether the observed postoperative changes reflect true physiological remodeling or merely variations from an already altered baseline. Additionally, the small observational cohort and the relatively short 12-week follow-up period may limit the generalizability of our findings.
Furthermore, significant technical limitations are inherent in the adaptation of posterior-segment spectral-domain OCTA (SD-OCTA) for anterior-segment imaging. 11 Motion, segmentation, projection, and shadowing artifacts—compounded by postoperative inflammation and surface irregularities—may introduce measurement variability in quantitative metrics such as VD, VLD, and VDI. 11 The inferior penetration depth and resolution of SD-OCTA relative to swept-source technology (SS-OCTA) also restrict the clear visualization of the deep episcleral microvasculature.
As a flow-based modality, OCTA is incapable of detecting slow flow or dye leakage. Unlike FA or ICGA, it cannot assess blood-conjunctival barrier integrity or vessel maturity; 44 consequently, our findings characterize structural remodeling rather than functional perfusion. Moreover, the absence of a standardized pterygium grading system remains a significant limitation. Because baseline vascular parameters are likely influenced by lesion vascularity and clinical severity, the lack of a formal grading scale may have introduced unaccounted variability.
Finally, the absence of a comparative surgical group and the reliance on manual region-of-interest (ROI) delineation may have introduced additional measurement bias. Future multicenter, controlled studies utilizing dedicated AS-OCTA platforms, normative control groups, and standardized image analysis protocols are essential to provide the necessary context for these vascular changes and to validate our findings. 15
In summary, vascular remodeling following AMT occurs predominantly through host-derived deep episcleral vessels, characterized by delayed and irregular superficial remodeling compared to CAG. The preservation of the episcleral bed is a critical surgical determinant for graft support. OCTA serves as a valuable, non-invasive tool for monitoring these subtle vascular changes, offering a potential biomarker for predicting surgical success and the risk of recurrence.
Conclusion
In conclusion, this study demonstrates the clinical utility of OCTA for the non-invasive monitoring of host-derived vascular remodeling following pterygium excision with AMT. As a depth-resolved imaging modality, OCTA facilitates the longitudinal visualization of microvascular changes within the surgical bed, offering a potential framework for evaluating graft stability and predicting recurrence risks. These findings provide a basis for optimizing postoperative care through the early identification of aberrant vascular patterns. While current technical constraints exist, continued advancements in dedicated anterior-segment OCTA technology are paramount to fully realizing its potential in characterizing ocular surface vascular dynamics and refining surgical outcomes.
Highlights
Optical coherence tomography angiography (OCTA) visualizes AMT post-operative changes.
Revascularization predominantly occurs via deep episcleral vessels post-AMT.
Vessel density and vessel length decline post-surgery and progressively recover by week 12.
Vessel diameter remains stable, indicating consistent vessel calibers postoperatively.
Irregular vascular patterns may signal recurrence risk or incomplete healing.
Compliance with ethics guidelines
This study has been approved by the local institutional review board of Tehran University of Medical Sciences IR.TUMS.FARABIH. REC.1402.004. The study was performed in accordance with the Helsinki Declaration of 1964, and its later amendments. All patients provided informed consent to participate in the study.
Footnotes
CRediT authorship contribution statement
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of competing interest
All authors certify that they have no affiliation with or involvement in any organization or entity with any financial interest or non-financial interest in the subject matter or materials discussed in this manuscript.
Data availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.