
Abstract
Purpose:
The aim of our study was to investigate the relationship between self-reported and performance-based tests in the assessment of patients with total hip arthroplasty (THA).
Methods:
Ninety four patients (35 males, 59 females) were included in the study with mean age 57.1 ± 14.6 years. Patients performed four performance tests (Timed “Up & Go” Test, Sit to Stand Test, Self-paced Walk Test and Stair Test) and two self-reported measurements (Harris Hip Score [HHS] and SF-36 [36-Item Short Form Health Survey]) were preferred to assess patients.
Results:
There were varying correlations between performance tests and subscales of the SF-36 including physical function, energy/fatigue, pain, general health. Strong correlation was found between HHS and Timed “Up and Go”(r = −0.59, p < 0.001), self-paced walk test (r = −0.58, p < 0.001). Moderate correlation was found between HHS and sit to stand test (r = −0.406, p < 0.001), stair test (r = 0.32, p < 0.001).
Conclusions:
There were especially moderate-to-strong correlations between self-reported measurements and performance-based tests in the evaluation of patients with THA. Therefore, outcomes assessment after THA may include self-reported measurements or performance-based tests.
Introduction
Hip osteoarthritis (OA) is a debilitating condition that will affect nearly 25% of all individuals within their lifetime.1,2 Patients with hip OA report reduced functional ability on self-reported questionnaires and demonstrate functional impairments on objective performance-based tests compared to age-matched individuals without lower extremity pathology. 1 Outcome data are necessary for both clinical and research purposes in order to measure the success (or not) of surgical treatments for individual patients and cohorts in. 3 Orthopaedic outcome measurements often focus on objective clinical-based parameters such as radiograph measures or other technical aspects. However, these parameters are weakly related with outcomes that are more relevant to patients, that is patient-based outcomes such as functional status and symptoms. In the last 10 years, patient-based measures have become an important aspect of orthopaedic clinical outcome evaluation. Performance-based measurement methods (such as timed walk tests and chair stand test) and self-reported questionnaires (such as Harris Hip Score [HHS] and 36-Item Short Form Health Survey [SF-36]) are commonly used for measuring physical function in patients which are planned or implemented total hip arthroplasty (THA).1,4 There are many different techniques to assess function after THA, however many of them are not used because of patients’ fatique or time constraints in clinic and research appointments. 5
The relationship between results of self-reported and performance-based tests in assessment of patients with THA and total knee arthroplasty (TKA) have been reported. 4 It is recommended that THA and TKA measurements results should be considered separately mainly because improvements in outcomes following hip joint surgery are significantly greater than knee surgery.6–8 Patients undergoing TKA revealed higher odds of developing post-surgical pain, when compared to THA patients. 9 This study only attempts to investigate the relationship between self-reported and performance-based tests in patients with THA. The purpose of our study was to determine which outcome measures are the most useful in assessing function of patients with THA.
Patients and methods
Between 2010 and 2011, 184 patients were identified who had undergone THA at least 6 months prior and were recruited into the this study. The median time from surgery was 4 years (range 6 months to 10 years). We excluded 38 patients because of missing or incorrect demographic information and a further 52 patients were excluded because of having exclusion criteria as given below. As a result, 94 (59 female and 35 male) THA patients were included in our study. All patients were operated on by a single surgeon with identical implants, all undergoing the same rehabilitation programme.
The inclusion criteria were: 18 years old or above with unilateral THA due to osteoarthritis, dysplasia or avascular necrosis. The exclusion criteria were: (i) arthritis in other joints required treatment; (ii) THA due to hip fracture; (iii) neurological or medical conditions causing locomotor disability; and (iv) revision hip prosthesis.
Our study was not blinded, all patients were evaluated by the same physical therapist who had 3 years of experience in orthopaedic physical therapy. All patients gave informed consent that was obtained in accordance with the Declaration of Helsinki. This study was approved by the Ethics Committee of Dokuz Eylül University.
HHS was used to assess patients hip functions and SF-36 was used to evaluate patient quality of life. 10 Timed “Up & Go” Test (TUG), sit to stand test (STS), self-paced walk test (SPWT) and stair test (ST) were used as performance tests. TUG is an easy to apply and confidential test to assess balance functionality. Patients sit on a height adjustable chair such that a 90° angle is formed when the femur is horizontal and tibia vertical with their feet shoulder width apart and their arms crossed against their chest. Patients are timed as they stand up from chair without using their hands, walk normal pace past a marker 3 m away, turned around, walk back and sit down again. Duration was recorded as seconds. 11 The STS test is an objective functional measure of strength correlating with ambulatory independence. 12 Patients stand up and sit down again 10 times without using their hands from a standard chair as described for the previous test, duration was recorded as seconds. 13 The 10-m timed walk test (in seconds): this measures functional physical activity in the elderly. The patients were asked to complete the 10 m distance between the 2 points at a normal walking speed. 12 In ST, patient step up 10 stairs with a height of 20 cm with the contra-lateral leg and then step down to the start point. 11
Statistical analysis
Statistical Package for Social Science for Windows (SPSS) version 16.0 was used for statistical analysis. Correlations among self-reported and performance-based tests were assessed with the Pearson correlation coefficient (r) for data. The degree of correlation was defined as low if the coefficient was less than 0.3, moderate if it was between 0.3 and 0.5, and strong if it was greater than 0.5. 4
Results
Demographic characteristics of the patients are reported in Table 1. Scores from HHS, eight sub-parameters of SF-36 and four performance tests are presented in Tables 2 and 3.
Demographic characteristics and diagnosis of patients before total hip arthroplasty.
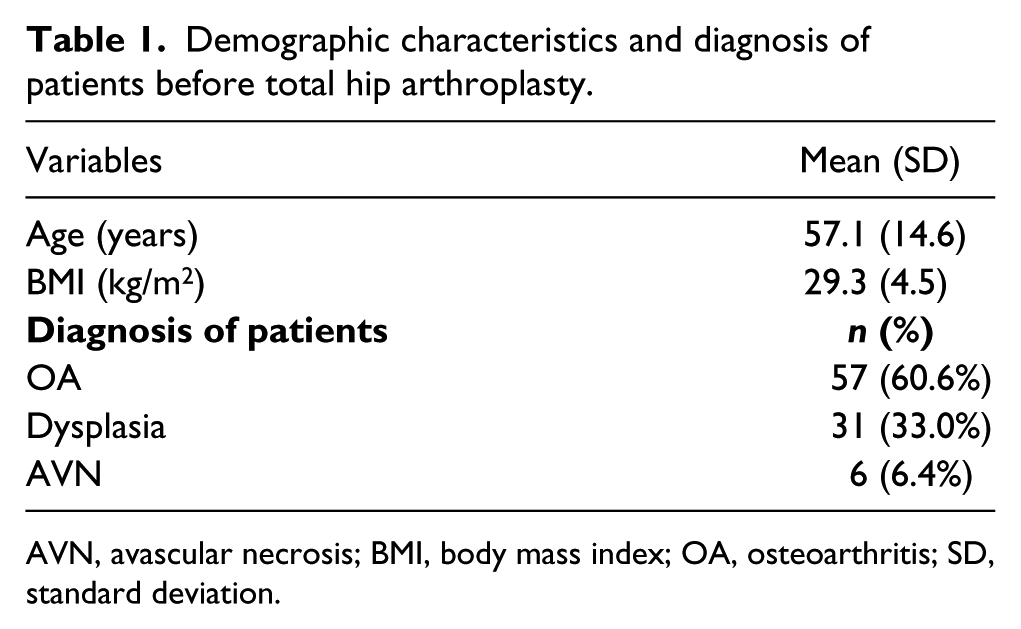
AVN, avascular necrosis; BMI, body mass index; OA, osteoarthritis; SD, standard deviation.
Results of self-reported tests in patients with total hip arthroplasty.
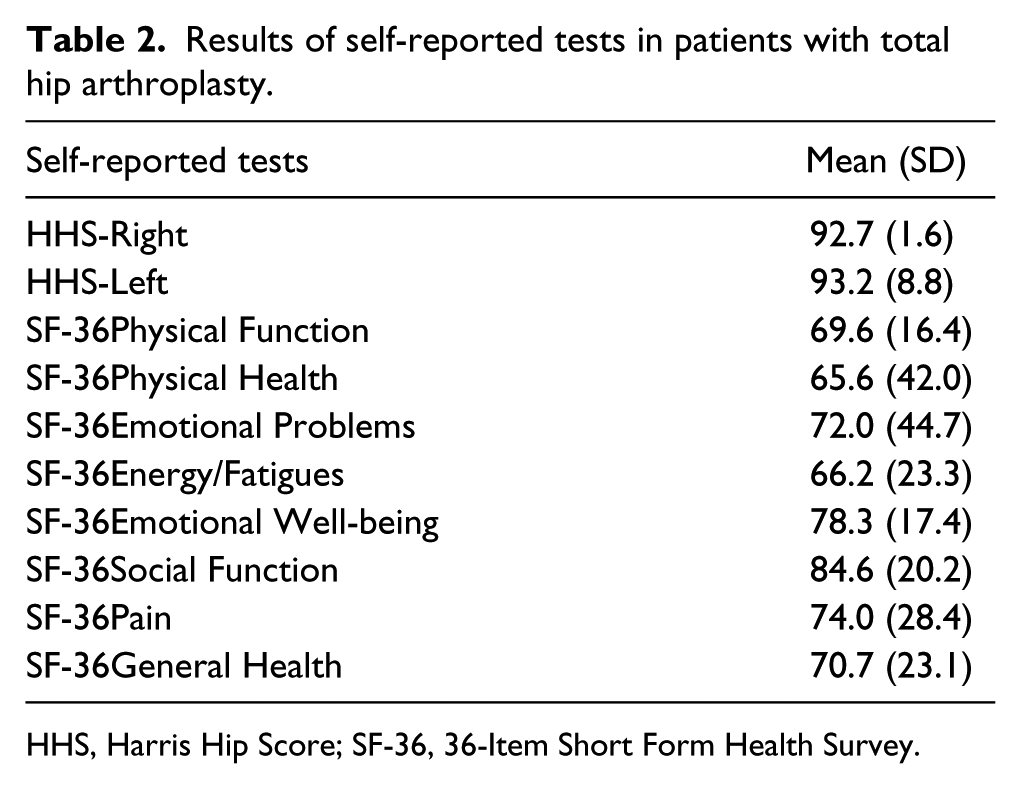
HHS, Harris Hip Score; SF-36, 36-Item Short Form Health Survey.
Results of performance-based tests in patients with total hip arthroplasty.
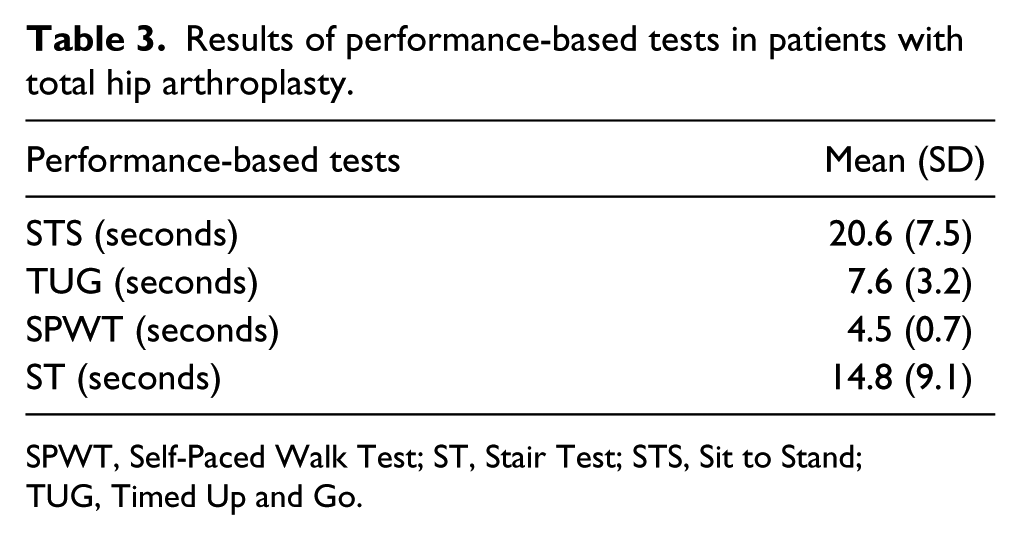
SPWT, Self-Paced Walk Test; ST, Stair Test; STS, Sit to Stand; TUG, Timed Up and Go.
SF-36 health quality ındex and performance-based tests
We found strong correlations between SF-36 “Physical Function” and TUG (r = −0.56, p < 0.001), STS (r = −0.60, p < 0.001), ST (r = −0.61, p < 0.001), there was moderate correlation with SPWT (r = −0.44, p < 0.001).
We found moderate correlation between SF-36 “Energy/Fatigue” and STS (r = −0.31, p = 0.002) and we found low correlations between SF-36 parameter and TUG (r = −0.24, p = 0.016), SPWT (r = −0.26, p = 0.011), ST (r = −0.22, p = 0.029).
There were moderate correlation between SF-36 “Pain” and TUG (r = −0.39, p < 0.001), STS (r = −0.31, p = 0.002), SPWT (r = −0.41, p < 0.001), ST (r = −0.32, p = 0.002).
We found moderate correlation between SF-36 “General Health” and STS (r = −0.31, p = 0.002) and we found low correlations with TUG (r = −0.26, p = 0.002), SPWT (r = −0.21, p = 0.034), ST (r = −0.29, p = 0.004).
There was not significant correlation between the other subscale of SF-36 and performance tests.
Harris Hip Score and performance-based tests
Strong correlations were found between HHS and TUG (r = −0.59, p < 0.001), SPWT (r = −0.58, p < 0.001), moderate correlations were found with STS (r = −0.406, p < 0.001), ST (r = 0.32, p < 0.001).
Discussion
We assessed patients with self-reported questionnaires (HHS, SF-36) and performance-based tests in our study and we found moderate to strong correlations among two types of outcome measurements as the primary finding. Strong correlation was found with the SF-36 physical subscale and the TUG, STS and ST. Strong correlations were also found with HHS and both the TUG and the SPWT. Our findings are similar to the study of Unnanuntana et al. 14 that included an hip osteoarthritis population and different from the study of Gandhi et al. 4 that included both hip and knee arthroplasty populations.
Assessment of patients’ function is important for identifying patients’ outcome at a point in time and assessing changes by the time. 11 Combined measurement methods consisted of self-reported measurements and performance tests are used after total joint arthroplasty. However, in clinical practices and studies, using too many measurement methods is exhausting and boring for patients and causes a loss of time for clinicians and researchers. 5 Because of this, relationship between self-reported measurements and performance tests must be investigated in order to determine which is the most necessary measurement method in assessment of function.
Performance-based tests assess only 1 property. They are objective outcome measurements of the physiological and functional state for that moment and can also change in time. They are suitable for the assessment of patients with cognitive disorders. 15 While self-reported tests assess long term perception of patients’ functional abilities, performance tests assess instant views of patients’ functional abilities. For that reason, factors such as short term disorders and motivation will affect results. 4
General outcome measurements are developed for assessing health quality. 10 Quality of life is a major determinant of the patients’ global assessment of satisfaction with their health status. The SF-36 is more relevant and more responsive than the Sickness Impact Profile as a general health status measurement tool. Also it is the preferable general health status measurement tool in patients with hip replacement. 7 Due to these properties, we preferred SF-36 for assessment of quality of life in patients with THA.
Many different hip scoring scales are used in assessment of THAs’ results.16,17 HHS is a joint specific outcome measurements and the most frequently used in assessment of THA patients.10,17 It has been used in many f studies over the years and has been shown to have high validity and reliability.10,17 Mahomed et al. 18 supported the use of the HHS as a self-report instrument that they compared reponses the individual items on the self-report HHS and surgeon-assessed HHS and overall the self-report and surgeon-assessed HHS showed excellent concordance. The HHS was used in this study.
Performance-based tests are important in assessment of functional states of patients. These tests are used to observe efficiency level and changes in functionality, patients performing these functional activities by themselves. Physical performance tests have an important role in the assessment of functionality of patients with THA. Walking, standing up from a chair and stair climbing are important and critical functional activities for clinicians and patients before and after THA.4,19,20 We chose these activities because they are typical “core activities” at self-reported questionnaires. For example, the HHS include items pertaining to stairs, walking, and sitting. Also in a recent study by Dobson et al. 21 , a consensus derived in relation to a minimal core set of performance-based tests to assess physical function in patients with hip and knee OA has been recommended, including walking short distances, sit-to-stand and step-up transfers. Short walking tests, STS test and stair climbing test are more suitable because they do not take a long time to perform, do not require any equipment and they also cost less. For these reasons, the SPWT,TUG test, STS test and ST to assess functions of patients were used in this study.
Results from studies that examined the relationship between physical function and sub-parameters of SF-36 questionnaires, are contradictory. Gandhi et al. 4 found a low degree of correlation between TUG performance test and physical function subscales of SF-36 in patients with THA and TKA; while Unnanuntana et al. 14 found a strong correlation between performance tests (2 minutes walking test, TUG test that are used in clinical practices) and physical function sub-parameters of SF-36. Kennedy et al. 15 found a low-to-moderate correlation between the self-report (Lower Extremity Activity Profile) and physical performance (fast self-paced walk test, stair climb, and TUG) measures in total hip and knee arthroplasty candidates preoperatively. Unnanuntana et al. 14 and Kennedy et al. 15 investigated the relationship between 2 types of measurement tool in pre-operative arthroplasty populations. Gandhi et al. 4 , investigated the relationship in TKA and THA populations and they used only one objective measure of function (TUG). Our study design was different from previous studies as in terms of the study patient population and assessment tools utilised.
While our study’s results were different from the results of Gandhi et al. 4 and Kennedy et al. 15 they are similar to the results of Unnanuntana et al. 14 In our study, we found a strong correlation between performance-based tests (except SPWT) and SF-36 physical function parameters in patients with THA. We also found a strong correlation between HHS and both the TUG and the SPWT. Among the performance-based tests, TUG and SPWT are important tests of achieving balance and muscle endurance. Also patients’ HHS functionality parameter that evaluates walking function, has the highest correlation. We therefore concluded that a strong correlation exists between HHS and two performance-based tests (TUG, SPWT).
There are limitations to this study. Follow-up periods are wide ranging, methodology included no blinding of the assessing physical therapist and no preoperative baseline scores were available for comparison.
We conclude by supporting the use of self-reported questionnaires and/or performance-based tests in the assessment of patients after THA. Practically, perfomance-based tests are quicker to perform, incur few costs and may lead to increased patient patient participation in outcomes research. Our study findings may differ when applied to other joints or specific pathology so future studies are required to investigate relationships between self-reported tests and performance-based tests in these areas.
Footnotes
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.