
Abstract
Introduction:
Radiological inclination (RI) is determined in part by operative inclination (OI), which is defined as the angle between the cup axis or handle and the sagittal plane. In lateral decubitus the theatre floor becomes a surrogate for the pelvic sagittal plane. Critically at the time of cup insertion if the pelvic sagittal plane is not parallel to the floor either because the upper hemi pelvis is internally rotated or adducted, RI can be much greater than expected. We have developed a simple Pelvic Orientation Device (POD) to help achieve a horizontal pelvic sagittal plane.
Methods:
A model representing the posterior aspect of the pelvis was created. This permitted known movement in 2 planes to simulate internal rotation and adduction of the upper hemi pelvis, with 15 known pre-set positions. 20 participants tested the POD in 5 random, blinded position combinations, providing 200 readings.
The accuracy was measured by subtracting each reading from the known value.
Results:
Two statistical outliers were identified and removed from analysis. The mean adduction error was 0.73°. For internal rotation, the mean error was −0.03°. Accuracy within 2.0° was achieved in 176 of 190 (93%) of readings. The maximum error was 3.6° for internal rotation and 3.1° for adduction.
Conclusion:
In a model pelvis the POD provided an accurate and reproducible method of achieving a horizontal sagittal plane. Applied clinically, this simple tool has the potential to reduce the high values of RI sometimes seen following THA in lateral decubitus.
Introduction
Accurate positioning of the acetabular component during total hip arthroplasty (THA) is both challenging and important. Poorly positioned components can result in instability, 1 leg length discrepancy, 2 wear, 3 osteolysis, 4 and in hard on hard bearings squeaking 5 and edge wear. 6
Correct acetabular component positioning includes both orientation and the restoration of hip centre. Orientation is determined by version and inclination and hip centre by offset and height. The transverse acetabular ligament can be used to guide version, height and offset 7 but not inclination. Achieving correct Radiographic Inclination (RI) on the postoperative X-ray remains a challenge. As described by Murray 8 Operative Inclination (OI) is the angle between the acetabular axis and the sagittal plane and RI is the angle between the longitudinal axis and the acetabular axis when projected on to the coronal plane. The latter is what is measured on the X-ray whereas operative inclination is what the surgeon measures during surgery. In lateral decubitus the theatre floor acts as a surrogate for the pelvic sagittal plane.
Although in lateral decubitus it is assumed that the pelvic sagittal plane is parallel to the floor, in reality the upper hemipelvis is commonly adducted or internally rotated (rolled forward) as shown in Figure 1a and b. This means that apparent OI, which is the angle between the cup introducer handle (cup axis) and the floor of theatre will be less than the true OI, which is the angle between the cup axis and the sagittal plane of the pelvis. As a result, true operative and radiographic inclination angles are greater 9 than expected.
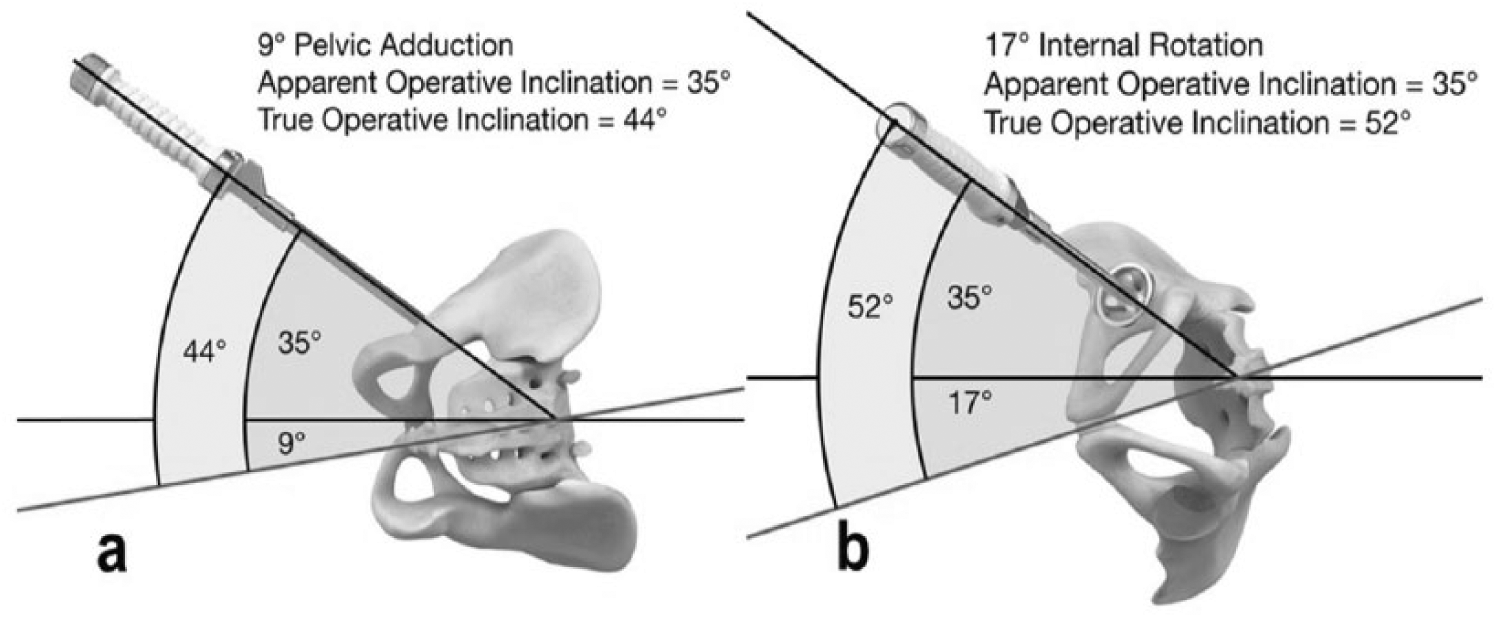
Graphic demonstrating how occult pelvic adduction and internal rotation leads to an ‘apparent’ and ‘true’ operative inclination mismatch.
To minimise this problem, preoperatively we sit each patient on a flat surface and use a perspex ruler with a built-in spirit level to draw a horizontal line across the lower back at the level of the posterior superior iliac spines (PSISs) (Figure 2).
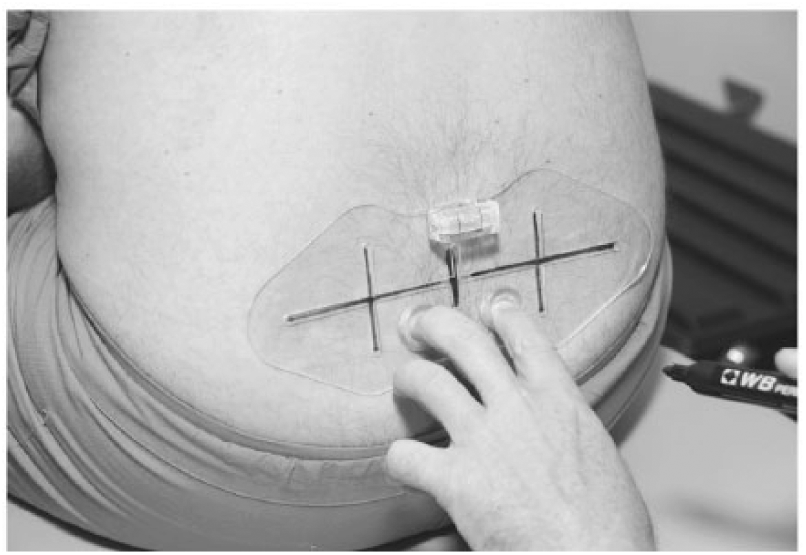
Horizontal line between posterior superior iliac spines.
Once anaesthestised, we use the pelvic orientation device (POD) to ensure a horizontal sagittal pelvic plane. As shown in Figure 3 this has 2 limbs 100 mm apart with flat 40 mm diameter discs on the end of each limb to cover the spectrum of inter PSIS distances.
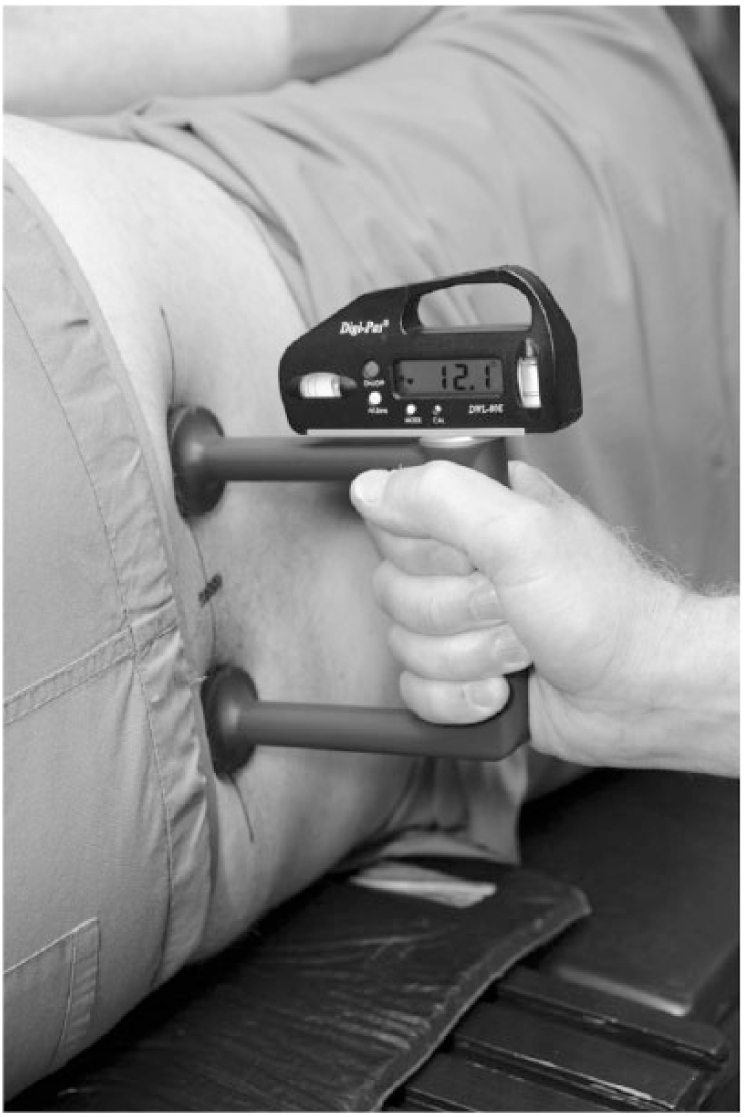
Picture demonstrating POD and inclinometer in use to measure pelvic internal rotation.
The device is placed directly against the previously drawn inter PSIS line. An inclinometer is then placed on top of the POD as shown in Figure 4 to firstly; assess whether the upper hemi pelvis is internally rotated and secondly; after turning the inclinometer through 90°, whether it is adducted. If necessary, the patient and or table can be adjusted until the pelvic sagittal plane is horizontal. The patient is then prepared and draped as normal.

Picture demonstrating POD and inclinometer in use to measure pelvic adduction.
The primary aim of this study was to test the validity and reproducibility of the POD in a pelvic model.
Methods
We developed a simple model to simulate the patient’s lower back in lateral decubitus. This consisted of an upholstered board 50 cm by 30 cm that was placed upright on a stand with hinges allowing movements in 2 planes. This allowed the board to be placed in variable amounts of internal rotation (0°, 5°, 10°, 15°, 20°) and adduction of the upper hemi pelvis (0°, 5°, 10°) relative to the floor. With the board in neutral position, it was marked with a line perpendicular to the floor representing the line between the 2 PSIS’. The POD was then placed against the model, as if placing it against a patient. The exact positions of the 15 possible combinations of adduction and internal rotation were verified by using a calibrated digital inclinometer (DWL-80E, Digi-Pas™, Dundee, UK) placed on a metal set-square and using the average of 3 blinded readings. These 15 position readings were then used as our true values to which we compared all subsequent readings obtained in each position.
We asked volunteers to use the POD and the inclinometer to measure the internal rotation and adduction of the pelvis at pre-set variations. 20 volunteers were included. They had no prior experience of using the POD and inclinometer and received brief standardised instructions prior to participation. Each volunteer randomly picked 5 envelopes containing different combinations of adduction and internal rotation. They were blinded to the combinations they had picked, and the model pelvis was adjusted to the selected position prior to measurement. The inaccuracy in the measurement by the participant for internal rotation and adduction was then calculated by subtracting the participants reading from the true reading.
The data is presented as deviation from the true readings, referred to as error. This data was distributed normally, and thus is presented as mean and standard deviation (SD). This data was statistically analysed using Dixon’s outlier test and Student’s t-test on SPSS (IBM Corp. Armonk, New York, USA).
We also present the data as unsigned error. This does not take the direction of error into account, which in doing so removes normality.
Results
Six of 20 participants were consultant orthopaedic surgeons, 5 were orthopaedic registrars and 9 were theatre nurses.
Firstly, the data was analysed using Dixon’s test to assess if there were any statistical outliers that would skew further interpretation. This test identified 1 outlier in measuring adduction and 1 in measuring internal rotation (p =< 0.05). They were 2 different volunteers. Both were removed from further interpretation, resulting in 190 readings for further analysis.
The mean error recorded in measuring adduction was 0.73° (SD 0.96) and internal rotation −0.03° (SD 0.98). The maximum error for each was 3.1° and 3.6° respectively. The data is distributed normally (Figure 5). When the mean values of adduction and internal rotation were analysed using Student’s t-test, there was a statistically significant difference (p =< 0.05).
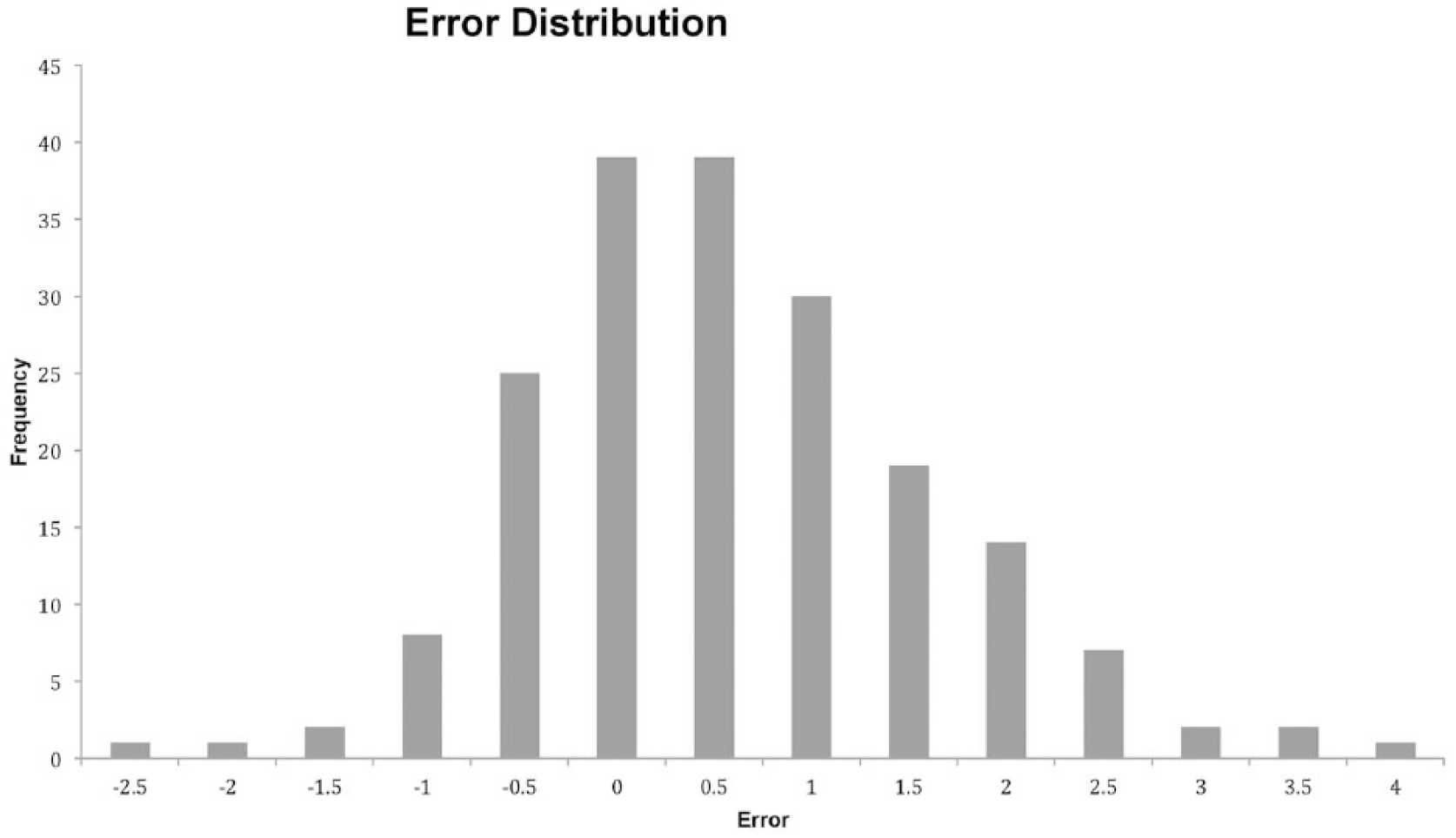
Histogram of error including all readings demonstrating normal distribution.
When the data is unsigned (i.e. the ‘negative’ sign removed) the distribution shows that an accuracy within 1° was achieved in 135 of 190 (71%) of readings and within 2° in 176 of 190 (93%) (Figure 6).

Graph demonstrating distribution of error when data is unsigned.
We assessed whether there was a difference in the outcomes between consultant surgeons and non-consultant staff.
Six consultant surgeons took part in the experiment, achieving a mean error for internal rotation of −0.19° (SD 0.97) and adduction 0.81° (SD 0.92). The 14 non-consultant (registrar and nursing) staff had a combined mean error in measuring internal rotation of −0.10° (SD 0.96) and adduction 0.69° (SD 0.98). Although there is a trend towards a higher degree of accuracy among the non-consultant staff, this is not statistically significant for either internal rotation or adduction.
Discussion
The primary purpose of this study was to identify whether the POD provided a reproducible and accurate means of determining the degree of adduction and internal rotation of a model pelvis. We feel that the data collected confirms this, with an overall mean error of 0.35° (SD 1.03).
Participants in the study had no prior experience using the POD. Despite this, they achieved an accuracy to within 1° in 71% of cases with a maximum error of 3.6°. This demonstrates that acceptable degrees of accuracy can be achieved with minimal training. There was no statistically significant difference between consultant and non-consultant performance, suggesting that surgical experience confers no benefit in using the POD and inclinometer.
The mean value for error in measuring adduction was 0.73°. The data was distributed normally, however, this demonstrates a bias towards a positive value, as a true normal distribution should have a mean value of 0°. The cause of this bias is not clear. It is possible that the padded nature of the board allowed the handle to tilt, whereas placement on a more solid prominence (such as the PSIS) would negate this.
There are limitations to this study. Firstly, this model doesn’t provide a good surrogate for the obese patient in whom the PSISs can be hard to locate and the line becomes distorted. Secondly, although this device may help to ensure that the pelvic sagittal plane is horizontal prior to skin prep it does not guarantee that the pelvic sagittal plane is still horizontal at the time of cup insertion.
Conclusion
Within the stated aims of this validation study, we feel that the POD provides an easy to use, accurate and reproducible means of ensuring accurate positioning of a model pelvis with respect to internal rotation and adduction prior to surgery. We feel that this simple device and method has the potential to significantly reduce the number of radiographic inclination outliers in THA when operating in lateral decubitus.
Footnotes
Acknowledgements
We thank Mr Michael Stevenson, Senior Lecturer in Medical Research, Queen’s University, Belfast, for consultation regarding and assistance with statistical analysis.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: There were no sources of funding for this study. The senior author’s research unit has received funding and or consultancy from Zimmer Biomet and Depuy Synthes but this was unrelated to this work.