
Abstract
Background:
Anatomical landmarks for templating of total hip arthroplasty (THA) that are visible both during surgery and on radiographs are rare. If surgery is performed through a direct anterior approach the external obturator tendon (EO) is consistently visible. To use this point as a reference the exact position and dimensions of the footprint need to be known.
Aim:
To determine the location and dimension of the EO footprint on pelvic radiographs by correlating the EO anatomy in CT scans with conventional radiographs.
Methods:
CT scans and radiographs of 200 patients were analysed. The EO tendon was identified on CT scans; the height of its footprint, and its distance to the tip of the greater trochanter and to the anatomical axis of the femur was measured. The accuracy and inter-rater reliability in the identification of the EO footprint was determined.
Results:
The EO tendon was visible on all CT scans and it’s footprint was identifiable on all corresponding radiographs. It’s cranio-caudal dimension was 6.4 ± 1.4 mm. It’s distance to the tip of the greater trochanter was 16.0 ± 3.1 mm. The EO footprint was located 5.2 ± 3.7 mm lateral to the femoral anatomical axis. There was no significant difference regarding the accuracy of EO footprint localisation on radiographs among the 2 readers.
Conclusion:
The EO footprint on the greater trochanter is consistently visible on CT scans and radiographs. As the variability of the footprint dimension is small, this structure may serve as a useful landmark in THA, particularly when performed through a direct anterior approach.
Keywords
Introduction
Leg length is an important parameter determining patient satisfaction and function after total hip arthroplasty.1,2 Eggli et al3, Müller, 4 and Knight and Atwater 5 , among many others, emphasised the role of preoperative planning in total hip arthroplasty to obtain an accurate reconstruction of the hip.6,7 While several modifications including CT-based 2D or 3D planning have been proposed, 6 templating on conventional radiographs has remained the most widely used form of planning. To implement a pre-operative plan in surgery, landmarks visible both on conventional radiographs as well as in the operative field during surgery are essential. In addition, an ideal landmark does not necessitate any additional dissection for exposure and is in proximity to the femoral stem.
All of the currently used femoral landmarks have specific shortcomings: the lesser trochanter might be flat,3-8 making it difficult to identify as a point of reference during surgery. In addition, the antero-posterior distance between the lesser trochanter and the tip of the taper is not taken into account if templating is performed on an anteroposterior radiograph, leading to an under-estimation of the true distance particularly in cases with a wide metaphysis.
As an alternative, the distance between the tip of the greater trochanter and the tip of the taper or the shoulder of the stem is used. However, due to insertions of the lateral capsule, the piriformis tendon, or the short external rotators the tip of the greater trochanter may be difficult to identify without significant dissection of these structures. 9 The lateral aspect of the femoral neck may serve as a landmark as well but is often removed to allow for an optimal entry point of the stem and cannot be used in all cases.
During a direct anterior approach for hip arthroplasty, the tendon of the external obturator muscle (EO) is almost always visible without any supplementary capsular release, particularly the cranial aspect of its insertion in the so called piriformis fossa (Figure 1).9,10 This piriformis fossa is the anatomical site of the EO insertion and is unrelated to the piriformis muscle, but is rather named for its somewhat pear-shaped appearance. 11 In our study we consistently use the term ‘EO footprint’ for the insertion of the EO tendon. While in our experience the EO footprint is visible on conventional radiographs in the majority of cases in, no data are available on this and the exact position and dimension of the EO footprint has not been described. However, in order to use this structure as a landmark the exact position and dimensions of the EO footprint needs to be known.
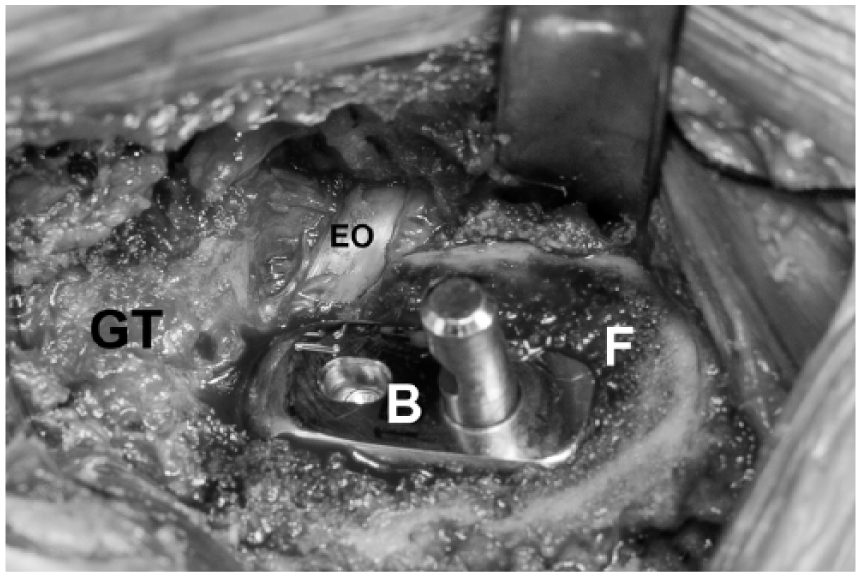
Intraoperative image through a direct anterior approach. The external obturator tendon (EO), particularly the insertion of its most cranial fibers is visible at the posterolateral aspect of the femoral osteotomy (F) and is in most cases close to the shoulder of the broach (B). GT, greater trochanter.
The purpose of this study was first to identify the EO footprint on CT scans and to describe its morphology, size and location in relation to the tip of the greater trochanter and the femoral shaft axis. Our 2nd aim was to determine the accuracy and inter-rater reliability regarding the identification of the EO footprint on radiographs.
Patients and methods
200 consecutive patients older than 18 years of age undergoing CT scanning of the pelvis for various reasons were retrospectively selected from a database. Patients were included if computed tomography (CT) of the pelvis with a high-resolution protocol and a standard anteroposterior radiograph of the pelvis were available. Only 1 hip was analysed per patient. The study was approved by the institutional review board.
CT scans were performed on a 64-slice CT scanner (Philips Brilliance 64, Philips Healthcare, Best, The Netherlands) using our standard protocol, consisting of tube voltage of 140 kVp, tube current of 250 mAs with automated modulation, collimation of 64 × 0.625 mm and rotation time of 0.5 seconds. Images were reconstructed with 1 mm slice thickness in bone and soft tissue kernel. Pelvic radiographs were performed in anteroposterior direction centred on the pubic symphysis.
Our Institutional Review Board approved and reviewed this study and informed consent was given by all individual participants included in this study.
Image analysis
The EO footprint was identified on multiplanar reconstructed thin-slice CT images after identification of the external obturator muscle, and by following its tendon to the footprint at the proximal femur (Figure 2). The craniocaudal dimension of the footprint was then measured on coronal CT sections.
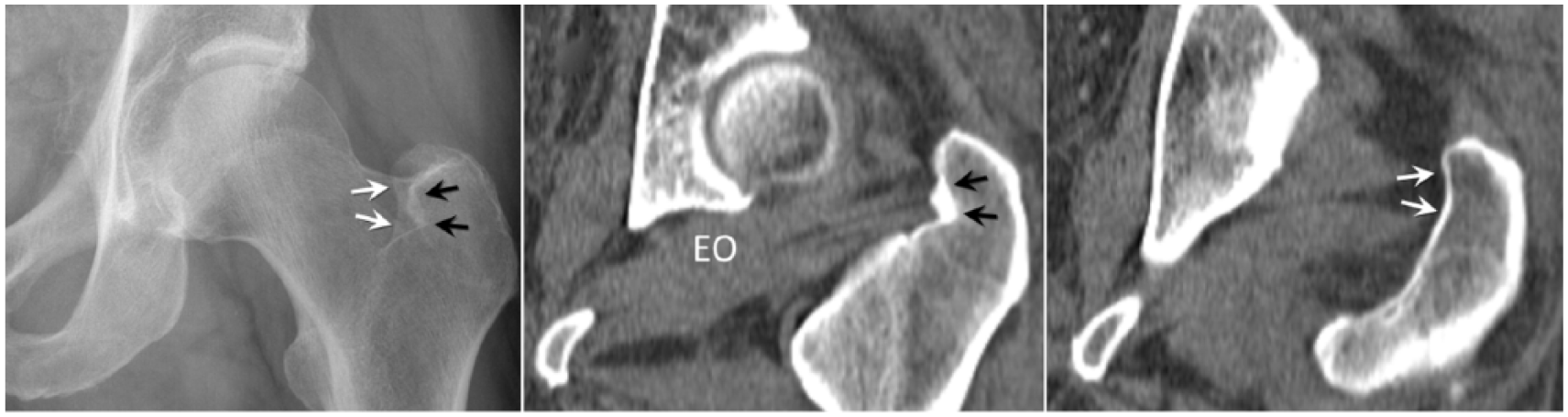
Radiograph of the hip showing the double contour of the medial aspect of the greater trochanter. The more lateral contour (black arrows) relates to the osseous border of the EO footprint, as demonstrated on the corresponding CT image. The more medial contour of the greater trochanter (white arrows) relates to the posterior and medial border of the greater trochanter. Of note, the footprint may occasionally be ossified as in this example. EO, external obturator muscle.
The shape of the EO footprint was defined as ‘flat’ or ‘grooved’ depending on its appearance on CT images: a ‘grooved’ fossa was defined as a pit-shaped structure bulging into the cortical bone of the medial aspect of the greater trochanter, appearing as a circle in the sagittal plane. In ‘flat’-shaped fossae, no such bulging existed (Figure 3).
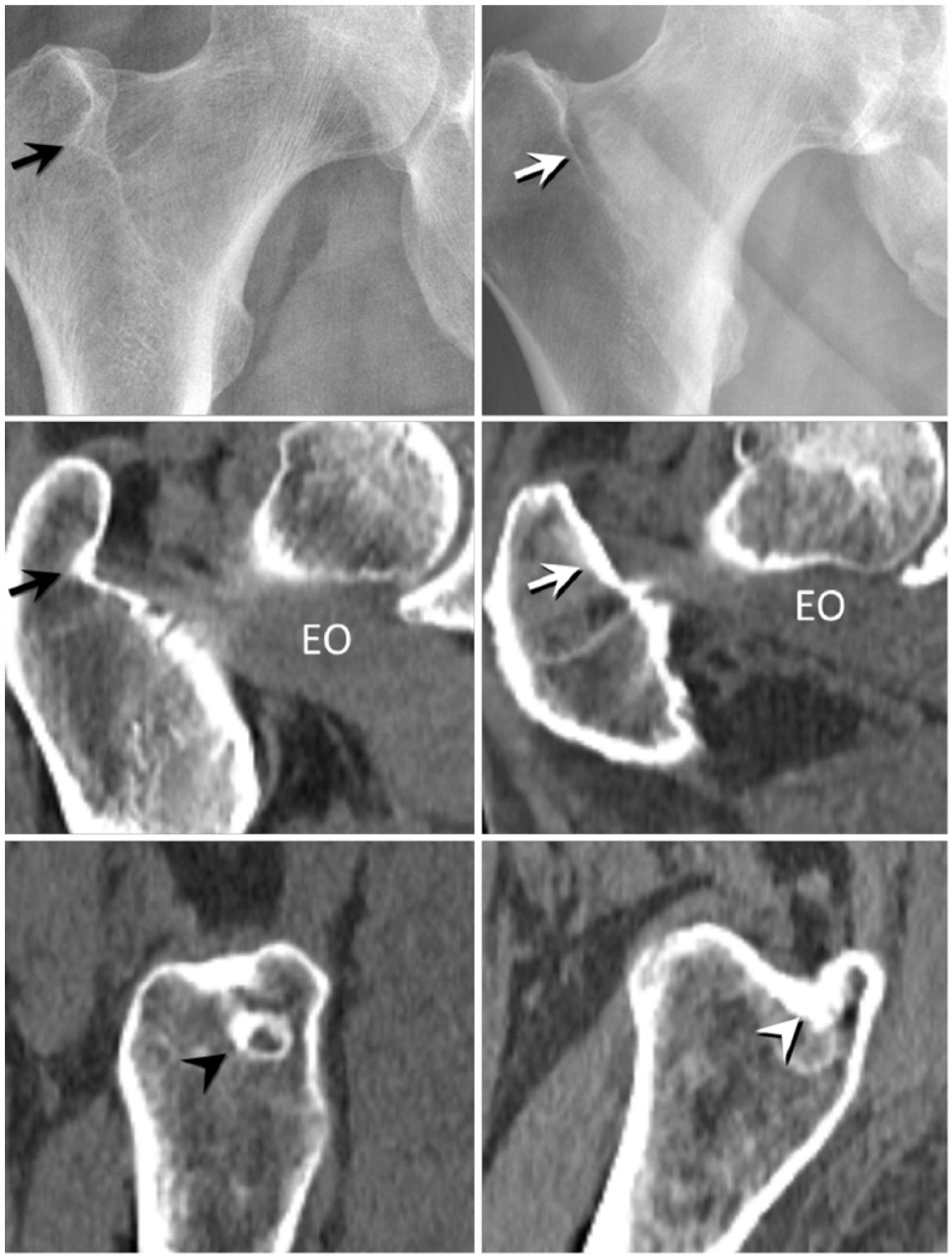
Radiographs and corresponding CT scans of a “groove”-shaped (first column) and a “flat”-shaped (second column) footprint. The grooved footprint protrudes into the greater trochanter (black arrows) and is visualised as a circle on sagittal images, which is not the case if the footprint is flat. EO, external obturator muscle.
The craniocaudal distance from the base of the EO footprint to the level of the tip of the greater trochanter was measured (Figure 4). The base of the EO footprint was defined as the most caudal area of EO tendon fibres attaching to the cortical bone on the medial aspect of the greater trochanter. The level of the tip of the greater trochanter was defined as the most cranial osseous border of the greater trochanter. The distance between these 2 levels was measured on coronal images in craniocaudal direction.
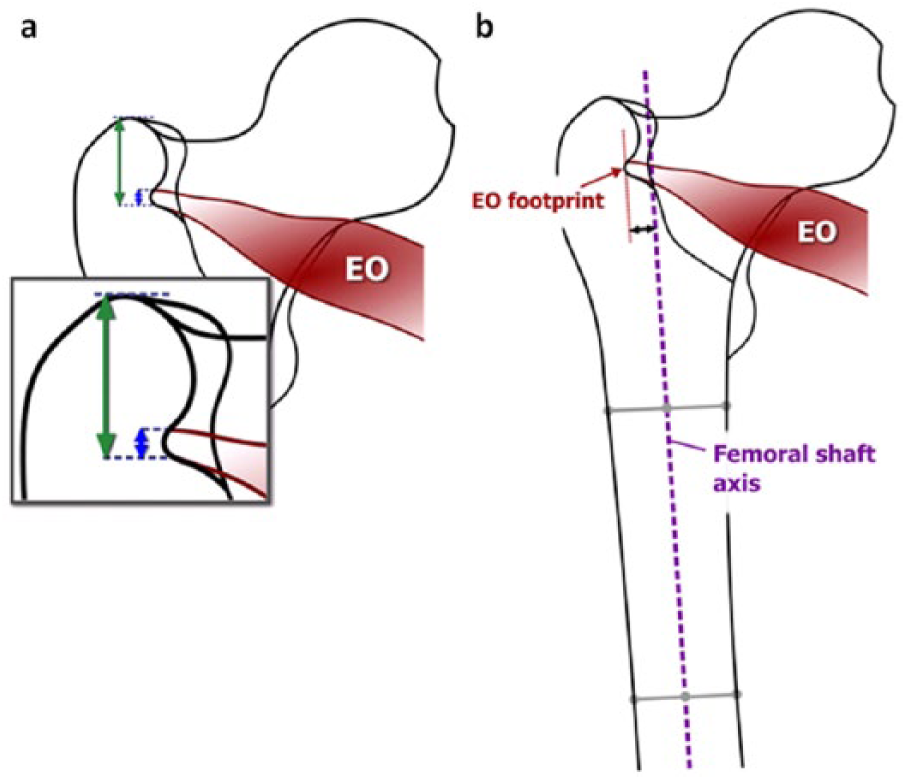
Schematic drawing of EO footprint measurements. (a) The height of the EO footprint (blue arrow) and the distance between the tip of the greater trochanter and the base of the EO footprint (green arrow) were measured in cranio-caudal direction and (b) The distance (black arrow) between the longitudinal axis of the femoral diaphysis and the base of the EO footprint was measured perpendicular to the femoral diaphyseal axis. In the majority of patients the EO footprint was located lateral to the femoral shaft axis.
The distance between the EO footprint and the femoral shaft axis was assessed on standard anteroposterior pelvic radiographs perpendicular to the femoral shaft axis (Figure 4). The axis of the femoral shaft was defined by a line crossing the centre of the femoral diaphysis on 2 different levels, located 2 cm and 12 cm below the lesser trochanter. If the EO footprint appeared lateral to the femoral axis, the perpendicular distance between these points was defined to have positive values, otherwise negative values.
To assess the precision of determining the position of the EO footprint on pelvic radiographs, a correlation with CT images was performed in 50 patients. For this purpose, 2 readers (an orthopaedic surgeon [reader 1] and a musculoskeletal radiologist [reader 2]) independently marked the base of the EO footprint on pelvic radiographs in a total of 50 patients (25 patients with groove-shaped and 25 patients with flat-shaped EO footprints) and made screenshots of the chosen position (including the position marker). In order to assess the inter-rater accuracy these markers have then been transferred in a separate session onto simulated radiographs, consisting of thick-slap coronal CT sections calculated with average intensity projection. These simulated radiographs were then re-converted to thin-slice CT sections, while keeping the marker that was positioned by reader 1 and reader 2, respectively.
In the final step of this analysis, the craniocaudal difference (in mm) between the positions marked by reader 1 and reader 2, respectively (test measurements) and the base of the EO footprint on CT (reference standard) was measured on the thin-slice CT in the coronal plane. If the EO footprint appeared caudal to the marked positions of reader 1 and 2, the distance between these points was defined to have positive values, otherwise negative values.
Statistical analysis
Data describing the EO footprint identified on CT scans have been presented as mean, standard deviations and range. The accuracy and inter-rater reliability in the identification of the EO footprint on a simulated radiograph was calculated using the Intraclass Correlation Coefficient and reporting the mean error with corresponding confidence interval (CI) (95%). The difference in the errors between footprint morphology (flat vs. groove) was examined using unpaired t-tests. Significance was set at an alpha value < 0.05. Analyses were performed using SPSS (IBM).
Results
Mean age of the patients was 55.9 ± 15.9 years (range 18–92 years). The EO tendon including its footprint on the greater trochanter was visible in all cases on the CT scans. Quantitative data on footprint dimension and localisation is detailed in Table 1.
Quantitative data on external obturator (EO) footprint dimension and localisation (n = 200).

positive values indicate a position of the footprint lateral to the mechanical axis.
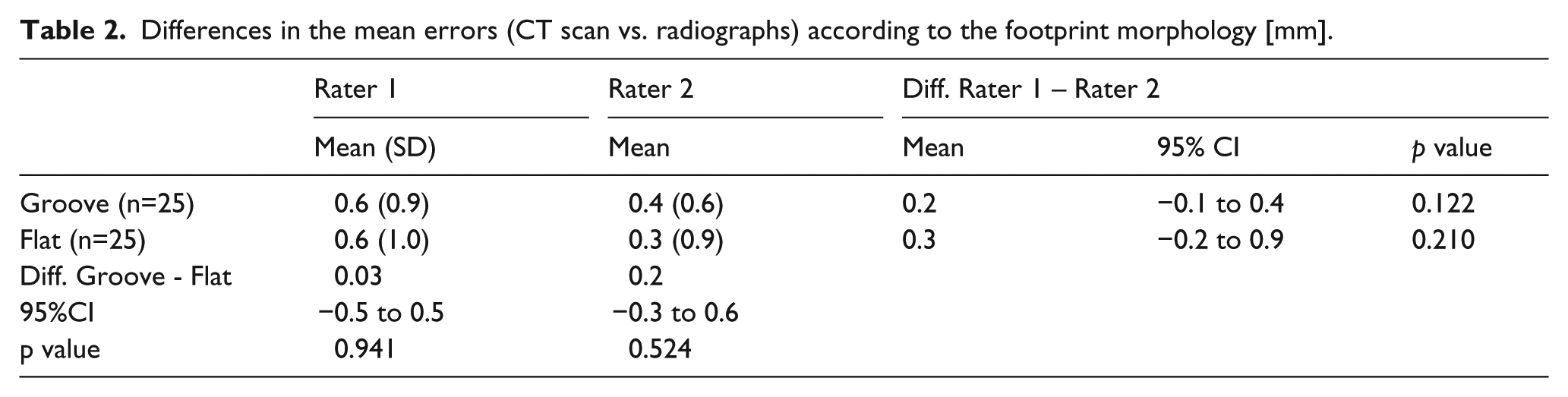
There was no difference between the mean error (difference between radiographs and CT scan) of rater 1 compared to rater 2 (0.3 mm, −0.06 mm to 0.6 mm, p = 0.105; Figure 5), and the Intraclass Correlation Coefficient between raters was 0.84 (95% CI 0.72–0.91), which corresponds to an excellent accuracy and inter-rater reliability. When compared according to footprint morphology (flat vs. groove), no differences in the mean error were found within and between raters (Table 2).
Differences in the mean errors (CT scan vs. radiographs) according to the footprint morphology [mm].
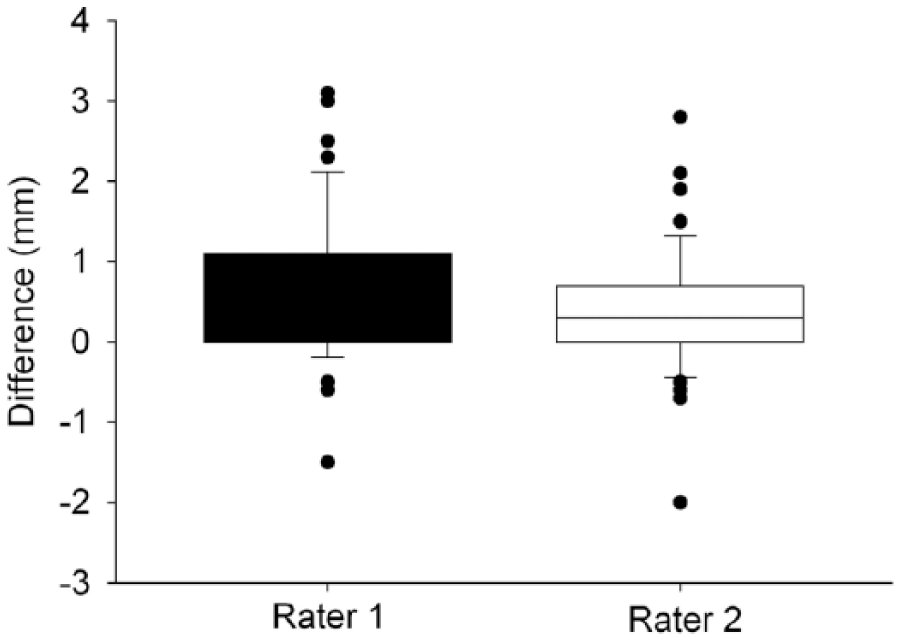
Box plot of the difference (in mm) between radiographs and CT scan for rater 1 and rater 2.
Discussion
Preoperative templating is an integral part of the surgical technique of THA, helping to improve the accuracy of leg length and femoral offset. In order to implement a preoperative plan during surgery, it is mandatory that landmarks are identifiable both radiologically and in situ, ideally without any further dissection. The tendon of the external obturator muscle and its footprint on the greater trochanter are consistently visible during THA through a direct anterior approach. In this study we demonstrated that the EO footprint can be identified with excellent accuracy and reliability on conventional radiographs, making it a solid landmark for THA.
While both Ito et al. 9 and Tamaki et al 12 have described the insertion of the EO tendon in the so called piriformis fossa, we are not aware of any data regarding the exact location and dimension of the EO footprint, nor of its location on a conventional radiograph. We believe such data is mandatory because the footprint is not fully visible during surgery without completely detaching the tendon insertion. In fact, during surgery, the most apical aspect of the footprint is always accurately visible. We here demonstrate that this point is 6.4 ± 1.4 mm proximal to the base of the footprint, which is well visible on conventional radiographs. Often, the tendon insertion is calcified, making the apical aspect readily identifiable (Figure 2). The EO footprint was identifiable on radiographs independent of the morphological type of the footprint (grooved vs. flat).
The EO footprint as a landmark has several advantages. 1st, it is consistently visible during a direct anterior approach to the hip joint. No relevant additional dissection is necessary to expose it. The tendon itself may be covered in some cases by a thin layer of fat tissue, which can be easily removed. 2nd, unlike the lateral aspect of the neck of the femur, which occasionally is removed during surgery to allow for an optimal entry point of straight stems, the EO tendon never has to be released. In our experience, such a release does not improve femoral exposure. 3rd, the EO footprint is in most cases located in close proximity to the shoulder of the femoral stem, allowing for an easy qualitative assessment of the depth of the stem (Figure 6).
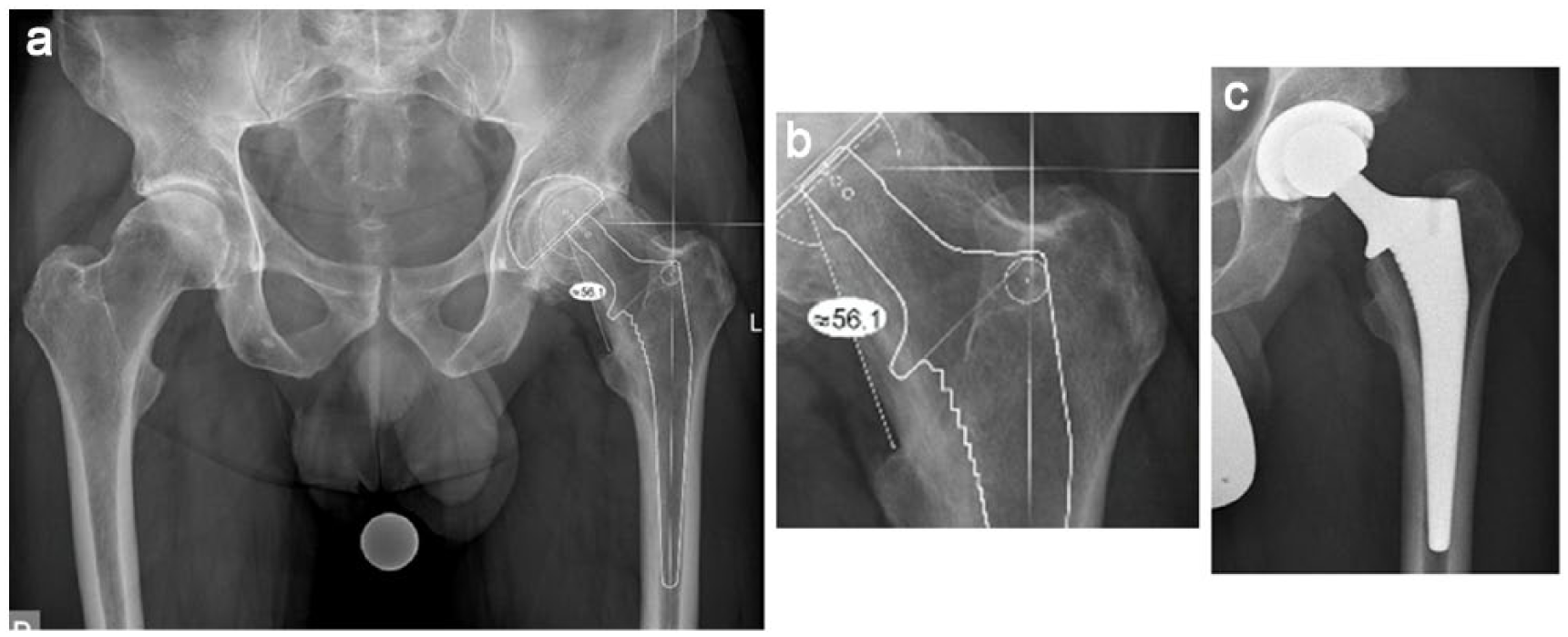
Preoperative templating (A), detail view (B) and postoperative X-ray (C) of one patient who underwent THA for primary osteoarthritis. Templating was performed using OrthoView software (Materialise Inc, Belgium). We template the position of the EO footprint in relation to the shoulder of the stem by marking the footprint with a circle of about 6mm in diameter. In addition, we do use the distance between the lesser trochanter and the tip of the Morse taper, 56 mm in this case.
We found a big scatterband regarding the distance between the EO footprint and the anatomical axis of the femoral diaphysis. Therefore, this landmark cannot be used as a general indicator of the femoral axis, which is consistent with the literature. 11 However, it may help to identify severe varus or valgus malalignment of the stem during surgery by comparing the distance of the footprint to the shoulder of the stem on the preoperative X-ray.
The study has several limitations. 1st, we did not assess the accuracy of the landmark by correlating intraoperative measurements to postoperative radiographs. As in the vast majority of cases the EO footprint is in very close proximity to the shoulder of the stem, it is our routine practice to assess the depth qualitatively (i.e. visually). 2nd, we did not compare the accuracy or usability of the EO footprint compared to other landmarks. In fact, we use the EO footprint always in combination with the other landmarks mentioned above.
Overall, we demonstrate that the footprint of the EO tendon is accurately and consistently identifiable on CT scans and on radiographs. The variability of the footprint dimension is small. In combination with a preoperative templating, this structure may serve as a useful landmark in THA, particularly when performed through a direct anterior approach.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.