
Abstract
Introduction:
Periprosthetic joint infection (PJI) is a serious complication after total hip arthroplasty (THA) and bearing material’s associations to PJI prevalence is largely unknown. The main purposes of this study were to determine if revision for infection varied depending on the type of bearing surface used in primary THA and to study whether patient or implant related factors had an effect on this variation.
Methods:
A total of 177,237 primary THA procedures from the Australian Registry (AOANJRR) were analysed. 3 bearing surfaces were compared. Metal-on-highly cross-linked polyethylene (MoXP) bearing had been used in 95,129 hips, ceramic-on-highly cross-linked polyethylene (CoXP) in 24,269 hips, and ceramic-on-ceramic (CoC) in 57,839 hips. Revision rates for infection were compared between the 3 groups.
Results:
Both MoXP and CoXP had a higher revision rate for infection compared to CoC hips (hazard ratio [HR] 1.46 (1.25, 1.72), p < 0.001) and HR 1.42 (1.15, 1.75), p = 0.001 respectively). Patients aged 70 years or less had a lower revision rate for infection when a CoC bearing was used. This difference was independent of sex, and prostheses selection. No difference was evident if the femoral component was cemented or a head size of 28 mm was used.
Discussion:
In this registry-based material, use of a CoC bearing was associated with a lower risk of revision for infection in patients younger than 70 years when cementless femoral components were used. Further studies are needed to verify this finding.
Keywords
Introduction
Periprosthetic joint infection (PJI) remains a serious complication following primary total hip arthroplasty (THA). Many factors including primary diagnosis, comorbidities, and duration of procedure are known to influence the rate of infection (1-3). Although the association between patient and surgical factors is becoming increasingly well understood, the evidence about the role of the prosthesis is still conflicting. A potential contributing factor to the development of PJI is the attachment of the infecting organism to the implant surface and the subsequent formation of biofilm (4). The known factors influencing bacterial adherence to a biomaterial surface include chemical composition of the material, surface charge, hydrophobicity, surface roughness or physical configuration (5, 6). Thus, it would be expected that the affinity of different pathogens to attach onto different biomaterials surfaces would vary.
A recent international consensus study based on the available medical literature concluded that the incidence of PJI does not differ between cemented (without antibiotics) and cementless arthroplasty components, nor does the presence of a hydroxyapatite coating influence the incidence of infection (7). The group also concluded that the incidence of PJI is higher following the use of a metal-on-metal (MoM) bearing in THA (7). However, the relationship between the use of other bearing surface materials in THA and PJI is not yet fully understood.2 recent meta-analysis including randomised controlled trials did not found connection between PJI and bearing material, whereas, 2 registry studies have associated ceramic bearings with lower PJI revision rates (8-11). The importance of registry data in providing valuable information about issues related to the bearing surface has been emphasised (12, 13). While clinical studies can prove causality for a specific study question, registry approach provides generalisable data and founds patterns. Registries strength lie in identifying unanticipated problems and raising questions for future clinical studies.
The main purposes of this study were to determine if revision for infection varied depending on the type of bearing surface used in primary THA and to study whether patient or implant related factors had an effect on this variation based on data from the Australian Orthopaedic Association National Joint Replacement Registry (AOANJRR).
Methods
The AOANJRR started collecting data in 1999, and includes data on more than 98% of the arthroplasty procedures performed in Australia since 2002 (13,14). Registry data are validated against patient-level data provided by each of the state and territory health departments in Australia using a sequential, multilevel process of matching. The matching program is used on a monthly basis to search for all primary and revision arthroplasty procedures recorded in the Registry that involve the same side and joint of the same patient, thus enabling each revision to be linked to the primary procedure. Data are also matched biannually with the National Death Index of the Department of Health and Ageing to obtain information about the date of death. The Registry also records the reasons for revision and the type of revision THA. Infection was defined as reported revision for infection in the registry.
3 different bearing surfaces, ceramic-on-ceramic (CoC), ceramic-on-highly-cross-linked polyethylene (CoXP) and metal-on-highly-cross-linked polyethylene (MoXP) were compared. The study population included all primary THA procedures undertaken for osteoarthritis using these bearing surfaces and reported to the AOANJRR over a 14-year period (between 1999 and 2013). During the study period there were 177,237 primary THA procedures reported to registry that met the inclusion criteria (57,839 CoC, 24,269 CoXP and 95,129 MoXP) (Table 1).
Revision rates for infection of primary total hip arthroplasty by bearing surface.
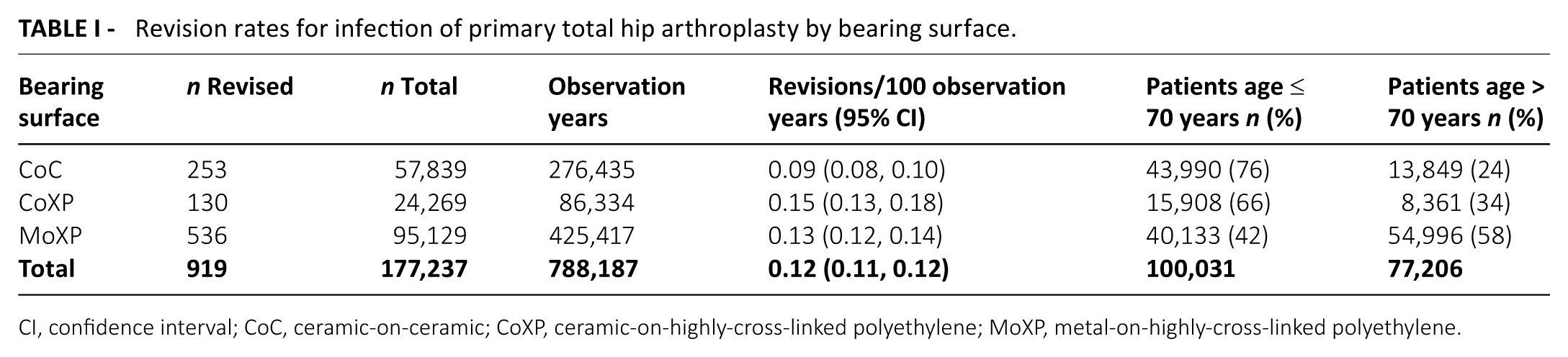
CI, confidence interval; CoC, ceramic-on-ceramic; CoXP, ceramic-on-highly-cross-linked polyethylene; MoXP, metal-on-highly-cross-linked polyethylene.
The AOANJRR uses Kaplan-Meier estimates of survivorship to estimate the time to the first revision of an arthroplasty, with censoring at the time of death or closure of the database at the time of analysis. The unadjusted cumulative percentage revision (CPR) after the primary arthroplasty, with an accompanying 95% confidence interval (CI), was calculated using unadjusted pointwise Greenwood estimates. Hazard ratios (HR) were calculated using Cox proportional-hazards models, adjusting for age and sex, and were used to make statistical comparisons of the revision rates between groups. A sub analysis examining the effect of age, sex, fixation of the femoral stem, and femoral head size was also performed. To ensure that confounding due to differences in femoral and acetabular component selection was minimised a further analysis was undertaken: we compared the 3 different bearings with the same well performing stem and acetabular component combinations (Pinnacle acetabular component paired with Summit or Corail femoral stem [DePuy, Warsaw, IN]). All tests were 2-tailed at the 5% level of significance. Statistical analysis was performed using SAS software version 9.3.
IRB/Ethics Committee decided approval was not required for this study.
Results
A higher revision rate for infection was found for both MoXP and CoXP compared to CoC (HR 1.46 (1.25, 1.72), p < 0.001, and HR 1.42 (1.15, 1.75), p = 0.001 respectively) (Figure 1). There was no difference in the revision rate for infection when MoXP and CoXP were compared (HR 0.97 (0.80, 1.18), p = 0.742).
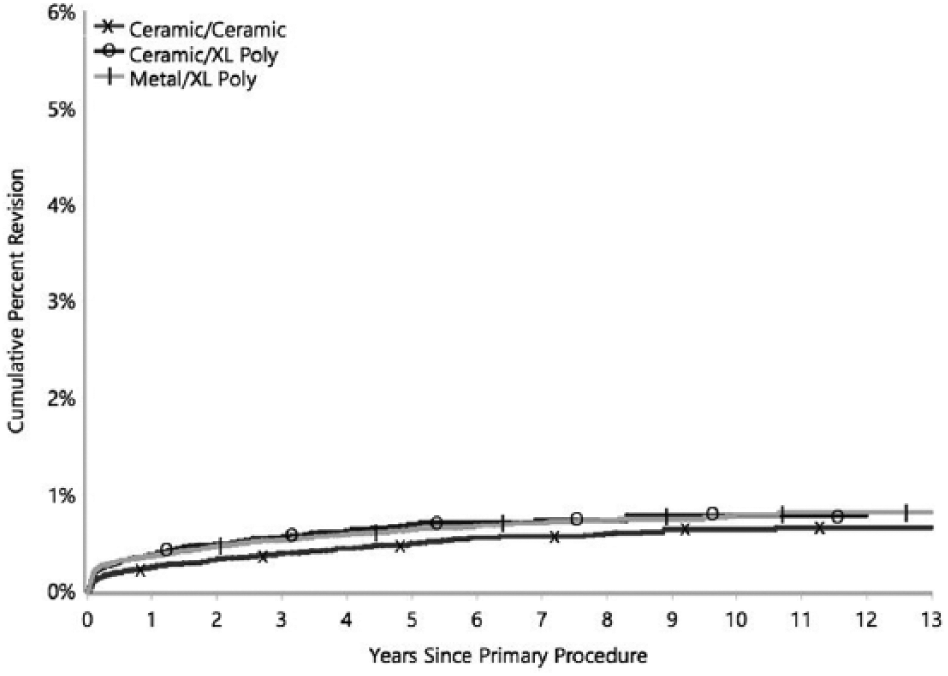
Cumulative percentage revision for infection of primary total hip arthroplasty by bearing surface over a period of 13 years from index surgery.
Both men and women had a lower revision rate when CoC was used. However, there was an age variation with the observed lower revision rate for infection in CoC hips being evident in patients aged 70 years or younger (CoXP vs. CoC: HR 1.60 (1.25, 2.05), MoXP vs. CoC: HR 1.49 (1.21, 1.84), p < 0.001). This difference was not observed for patients older than 70 (CoC vs. CoXP: HR 1.02 (0.69, 1.53), p = 0.91, CoC vs. MoXP: HR 0.99 (0.76, 1.29), p = 0.94) (Figure 2).
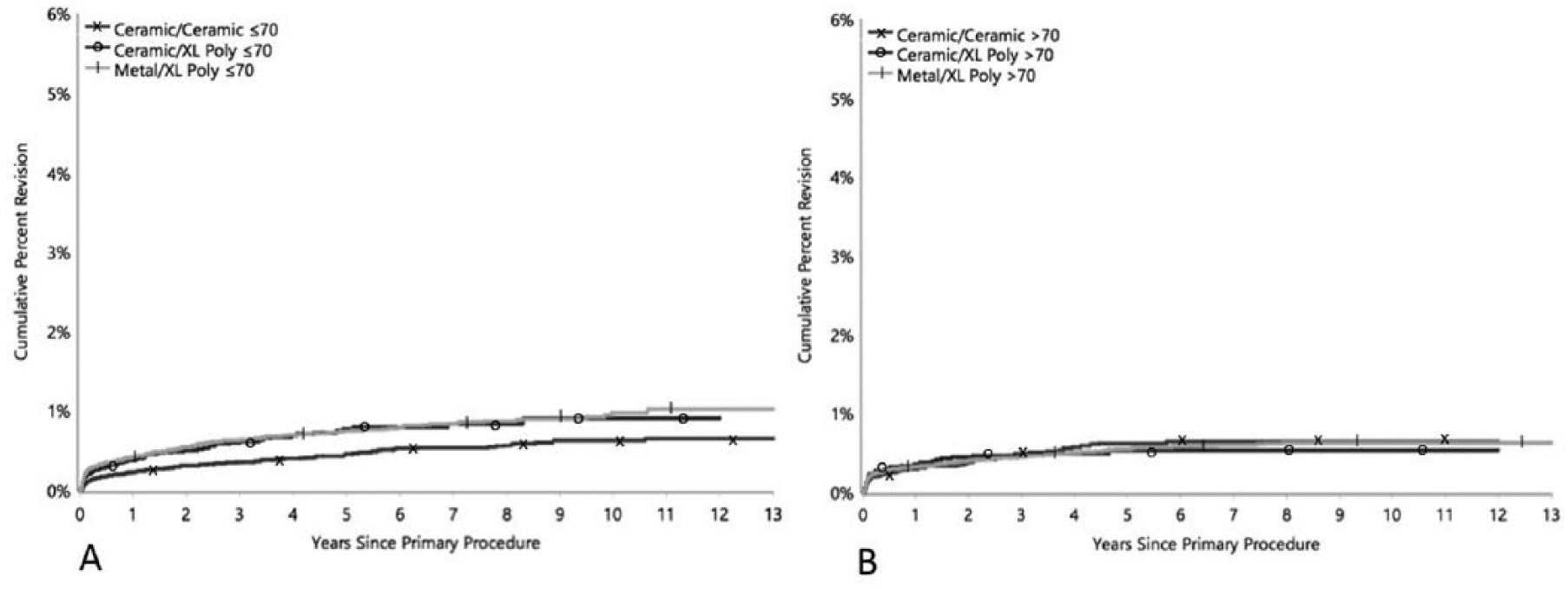
Cumulative percent revision for infection of primary total hip arthroplasty by bearing surface stratified by age ≤70 years (A) and >70 years (B).
Of the 57,839 CoC hips, 27,753 (48%) hips had a modern ceramic-on-ceramic bearing (zirconia toughened alumina). The revision rate for infection for both MoXP and CoXP were also higher than for this subgroup (HR 1.56 (1.24, 1.95), p < 0.001, and HR 1.47 (1.13, 1.92), p = 0.004, respectively).
The observed lower rate of revision for infection in CoC hips compared to other bearing surfaces was only evident when a cementless femoral stem was used (CoXP vs. CoC: HR 1.59 (1.23, 2.04), p < 0.01, MoXP vs. CoC: HR 1.34 (1.07, 1.68), p = 0.010). There was no difference when the stem was cemented (CoC vs. CoXP: HR 1.13 (0.76, 1.69), p = 0.55, CoC vs. MoXP: HR 1.18 (0.90, 1.56), p = 0.23) (Figure 3). The decrease was present for all head sizes, although this decrease was not significant for size 28 mm heads (CoC vs. CoXP: HR 1.15 (0.61, 2.18), p = 0.67, MoXP vs. CoC: HR 1.37 (0.91, 2.06), p = 0.13). A total of 23,009 (13%) of the 177,237 THA procedures had been performed using the same type of acetabular component and one of 2 different stem types. The CoC hips also had a lower revision rate for infection in this sub cohort when comparing the 3 bearing surfaces (CoXP vs. CoC: HR 2.48 (1.46, 4.22), p < 0.001, MoXP vs. CoC: HR 2.03 (1.27, 3.23), p = 0.002).
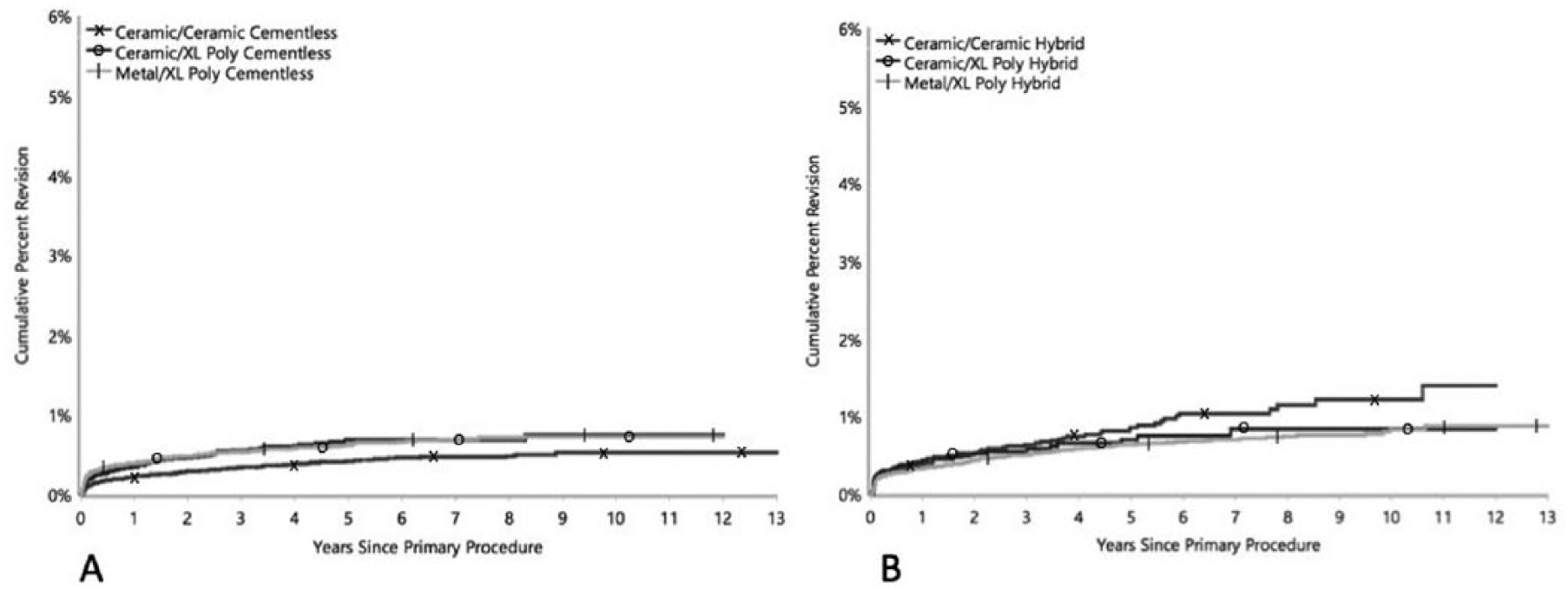
Cumulative percent revision for infection of primary total hip arthroplasty by bearing surface stratified by cementless (A) and hybrid fixation (B).
Discussion
This registry study aimed to determine if revision for infection varies according to the bearing surface used during primary THA. The results showed that patients aged 70 years or younger have a significantly lower rate of infection when a CoC bearing is used when compared to both CoXP and MoXP bearings. This difference was independent of sex. The difference also remained significant for a subset of patients with a modern ceramic bearing (zirconia toughened alumina).
Data published on bearing materials association on PJI prevalence is conflicting. Even though the use of a MoM bearing surface has been associated with a higher incidence of PJI, the data on the differences in the risk of PJI for other bearing surfaces varies more in the literature (15). While 2 recent meta-analyses including 1,747 and 2,488 hips respectively have compared CoC to CoXP bearings at short to mid-term follow-up and did not find a difference in the rates of deep infection, registry data suggest that ceramic bearings are associated with decreased revision for PJI rate (8-11). A recent study from the New Zealand Joint Registry evaluated 84,894 hips including metal-on-polyethylene (MoXP), ceramic-on-polyethylene (CoXP), CoC, and MoM bearings. The authors found no difference in the rate of early PJI (<6 months) by bearing surface. However, for the entire observation period (median 9 years) they found that CoC and CoXP hips had the lowest rate of revision for infection and MoM bearings had the highest rate of revision for infection (9). The authors of the study noted that the rates of early infection appeared lower than expected but do not include surgical procedures for PJI that did not require exchange of components and therefore were not recorded in the Registry. Another study reported lower PJI rates for both CoC and CoXP bearings compared to MoXP bearings in large Medicare population (10).
In contrast to aforementioned studies, in our material the incidence of revision for infection was not reduced for patients older than 70 years of age with a CoC bearing. This finding may be due to other risk factors for PJI associated with comorbidities in this older patient group. Ceramic particles are known to be very bio-tolerant, whereas corrosion products of metal particles can cause substantial tissue damage. Large head sizes are associated with a higher risk of mechanically assisted crevice corrosion as a consequence of high torque conditions at the taper junction (16). Furthermore, the use of ceramic heads has been shown to be associated with less corrosion than cobalt-chromium heads (17, 18). It is also possible that the surface properties of ceramic are less favourable for bacterial adhesion as even nanoscale roughness can strongly influence initial attachment of bacteria, which may explain the early differences in revision rates for infection observed between the bearing surfaces (19). Larger head sizes are also associated with larger volumetric wear of highly cross-linked polyethylene. Thus, these issues may not be as relevant for small head sizes as observed in the current study. Finally, the lack of observed differences for cemented femoral components may be due to the confounding effect of antibiotic use in cement. Almost all cements used in Australia contain antibiotic, which could overshadow protective effects of a superior bearing surface regarding wear and corrosion. Uncemented stems are often used among the younger patients and based on our results this is the patient population that would benefit the most of CoC bearings infection wise.
In the prosthesis specific subgroup analyses the decrease in infection in CoC bearings was also maintained. This indicates that the differences in PJI risk between bearing materials was not caused by some underperforming devices.
To our knowledge this is the largest study to date comparing different bearing surfaces revision for infection as the endpoint. In addition to the large number of procedures, the use of population-based data, and the long-term follow-up are noteworthy strengths of the current study.
This study had some limitations. We were unable to take patient related factors, such as comorbidities and body mass index, into consideration as possible risk factors for deep infection. This might have caused selection bias. However, the study did adjust for confounders such as age, component head size, sex, stem type and fixation to reduce this bias. Further, our study design was retrospective, and we were only able to study association between revision for PJI and bearing material. This does not prove causality. An important role for registry studies is to identify patterns and raise study questions for upcoming clinical studies. While registries have the best capability to detect unanticipated problems, clinical studies have the ability to prove causality for specific study questions. Our results are registry based and further clinical studies are needed to verify our findings.
In conclusion, the use of a CoC bearing is associated with a lower risk of revision for infection in patients younger than 70 years when cementless femoral components were used. Data from other registries, together with laboratory studies assessing the role of bearing surface in bacterial adhesion and host defences, and clinical studies, will be needed to confirm these findings.
Footnotes
Disclosures
Financial support: No financial support.
Conflict of interest: None of the authors has financial interest related to this study to disclose.