
Abstract
Background:
We examined the blood conserving effect of tranexamic acid in total hip arthroplasty using the direct anterior approach with enoxaparin as deep vein thrombosis (DVT) chemoprophylaxis, and whether this translates to an effect on functional outcomes in the perioperative period. We also compare the effect of aspirin and enoxaparin as DVT chemoprophylactic agents.
Methods:
We conducted a single-centre randomised, double-blinded, placebo-controlled trial. 105 patients were randomised to receive either tranexamic acid or an equivalent volume of normal saline with enoxaparin used as DVT chemoprophylaxis. The primary outcome measure was thigh swelling. Blood loss and the incidence of blood transfusions was also recorded. Secondary outcome measures including postoperative functional scores and mobility, pain scores and length of stay. We also compared and pooled the results of a previous study with the same study intervention methodology which used aspirin as DVT chemoprophylaxis instead of enoxaparin.
Results:
There were no statistically significant differences between the primary outcome of thigh swelling. There was significantly less intraoperative blood loss observed in the tranexamic acid (TXA) group (0.510 L, SD 0.210) compared with the control group (0.698, SD 0.301) (p < 0.001). The estimated blood loss was also significantly less in the TXA group (1.130 L, SD 0.311) compared with the control group (1.48 L, SD 0.510) (p < 0.001). Pooled data of both consecutive trials showed there was a statistically significant reduction in length of stay for those that received TXA (3.72 days, SD 0.83 versus 4.24 days, SD 0.97, p < 0.001). There was also a statistically significant increased risk of a transfusion in the control group as compared those that received TXA (OR 5.5, 1.188 to 25.449, p = 0.029). There was no difference in blood loss between DVT chemoprophylactic agents.
Interpretation:
TXA is an effective agent in reducing blood loss in THR using the anterior approach and was not affected by choice of DVT chemoprophylaxis. Patients who received TXA had fewer transfusions and a reduction in their length of stay. The blood conserving effect of TXA was not associated with improved postoperative recovery across the measures of pain and mobility.
Clinical trials registration:
ANZCTR number: ACTRN12616000606482.
Introduction
Tranexamic acid (TXA) is an antifibrinolytic agent that has been established as an effective measure to minimise blood loss associated with total hip arthroplasty (THA) while not exposing patients to additional risks. 1 The use of TXA has been investigated across multiple surgical disciplines and found to reduce blood loss for several surgical procedures. 2
We have previously published data investigating the use of TXA in THA using an anterior approach and found it to be an effective agent in reducing blood loss. 3 Whilst the blood conserving effect of TXA was clear 0.460L (standard deviation [SD] 0.228) compared with the control group 0.687L (SD 0.283L) (p < 0.001), we were unable to correlate this effect with an improvement in measures of postoperative outcomes such as mobility or pain reduction. We were also unable to show a statistically significant reduction in transfusions.
TXA is a synthetic lysine derivative which acts to inhibit the interaction of plasminogen with fibrin, thereby decreasing fibrinolysis. 4 Given the pharmacokinetics of TXA, we were interested in whether the choice of deep vein thrombosis (DVT) chemoprophlaxis agent would influence the efficacy of the drug response. This question has been a focus of some interest recently with comparisons of efficacy of TXA with and without the use of enoxaparin. 5 It is possible that given agents such as enoxaparin act to inhibit the formation of thrombus, whilst TXA acts as an antifibrinolytic agent agent, using both these medications concurrently may diminish the blood conserving effect of TXA. This question has not been directly explored previously and provides further evidence into the use of TXA in the setting of total hip arthroplasty.
This study investigates whether TXA in the setting of THA using an anterior approach has a measurable effect on thigh swelling, functional measures and blood loss postoperatively. We conducted a single-centre, randomised, double-blinded, placebo-controlled trial to answer this question. 105 patients were randomised to receive either tranexamic acid or an equivalent volume of normal saline with enoxaparin used as DVT chemoprophylaxis. The primary outcome measure was thigh swelling. Blood loss and the incidence of blood transfusions was also recorded. Secondary outcome measures including postoperative mobility, pain scores and length of stay were also recorded. We then compared and pooled the results of a previous study which used aspirin as DVT chemoprophylaxis, 3 thereby examining the effect of choice of DVT chemoprophlyaxis agent on efficacy of TXA in the setting of total hip arthroplasty.
Patients and methods
This research reports on 2 consecutive single-centre single-surgeon randomised, double-blinded, placebo-controlled trial conducted in Melbourne, Australia between February 2015 and March 2016. Eligibility criteria for patients enrolled in the study included patients undergoing elective total hip arthroplasty for the treatment of osteoarthritis over the age of 40 years. All patients received an uncemented hip prosthesis (Quadra/Versafit Medacta, Strada Regina, Switzerland) using an anterior approach with a Mobile Leg Positioner (Medacta, Strada Regina, Switzerland). All patients received a general anaesthetic in conjunction with a spinal anaesthetic. The exclusion criteria included patients with contraindications to the use of tranexamic acid such as known drug reaction to TXA, active intravascular clotting (DVT, pulmonary embolism [PE] or cerebral thrombosis), predisposition to thrombosis (previously documented DVT or PE) or a subarachnoid hemorrhage. Patients with rheumatoid arthritis were also excluded.
No study has compared thigh swelling following total hip replacement surgery as an outcome measure. Due to this lack of precedent, we extrapolate that the mass effect of blood loss reduction will correlate with the mass effect of reduction in thigh swelling. Based on this extrapolation, we used previous measures of reduction in blood loss with TXA to calculate a sample size for this study. Using the results reported by Johansson et al., 6 to show a difference of 300 ml of blood loss with a 2-sided 1% significance level and a power of 90%, we would need to recruit at least 47 patients in each arm of the study. Simple randomisation was utilised through generation of a random number sequence with an allocation of 1:1 using the STATA software package. Surgeons, anesthetists and physiotherapists involved in collecting data for the trial were blinded to study allocation. The randomised sequence was held by the hospital pharmacist. Anaesthetists charted the TXA according to the study protocol and the pharmacist dispensed either the study drug or an equal volume of normal saline according to the randomisation sequence.
Patients allocated to the intervention group in the first trial received one 15 mg/kg intraoperative bolus of TXA intravenously at the time of induction of anesthesia. A further 15 mg/kg bolus was delivered 8 hours and 16 hours following commencement of the procedure. This dosing regime was selected with reference to data showing increased efficacy with prolonged rather than once off dosing. 7 Those in the control arm received an injection of an equal volume of normal saline at induction of anaesthesia and a further bolus of normal saline at 8 hours and 16 hours after the initial normal saline bolus. In this trial, patients received 40 mg of enoxaparin daily for 30 days and mechanical foot compression pumps for the duration of their inpatient stay for DVT prophylaxis. The initial dose of enoxaparin was given 12 hours after the surgery, then daily thereafter. Patients received a transfusion if their haemaglobin (Hb) was < 8 g/dL or 8.5 g/dL in the setting of pre-existing ischaemic heart disease.
The primary outcome measure was thigh swelling. We hypothesised that patients who bled more would have more perioperative swelling and as such increased pain and poorer short term functional outcomes. Whilst the blood conserving effect of TXA as previously been investigated, a correlation with clinical outcomes associated with this effect is less well described and as such thigh swelling was investigated as a clinical marker of reduced blood loss. 1 To test this hypothesis we measured thigh swelling using the Frustrum method. 8 The Frustum method has previously been compared to water displacement volumetry which is considered to be the gold standard in accurately measuring limb volume, and there is good correlation between the 2 methods of measurement. 8 Further secondary outcome measures of pain and mobility were investigated using the visual analogue pain scale, timed up and go test and the 10 metre walk test. These functional measures as well as thigh swelling were recorded preoperatively as well as day 1, day 3 and 2 weeks postoperatively. We recorded the patients’ length of surgery and length of hospital stay. Their opiate requirements whilst an inpatient were also recorded and converted to average daily intravenous (IV) morphine equivalent doses. 9
Blood loss was measured both directly through observed blood loss intraoperatively as well as through an estimation of absolute blood loss using postoperative blood results, particularly haematocrit (HCT). Intraoperative blood loss was measured by weighing blood soaked packs as well as calculating volume of blood in the suction canister minus any infiltrated fluid. Estimated blood loss was determined using the formula described by Gross 10 :

The reduction in HCT was the difference between the preoperative HCT levels and the lowest recorded postoperative HCT levels. Estimated blood volume was calculated using the formula proposed by Nadler et al. 11 We recorded any allogenic blood transfusions that were required secondary to postoperative anaemia.
We recorded demographic data including age, gender, body mass index (BMI), and American Society of Anesthesiologists (ASA) score. DVT was screened for clinically with no investigations being performed unless there was clinical suspicion of occurrence of DVT.
Statistical analysis was performed using Statistica (StatSoft Inc). Continuous data such as blood loss was reported in terms of the mean and standard deviation. The mean of continuous data between intervention arms was compared using the t-test. Binary data such as blood transfusions was compared using an odds ratio. Gender was compared using the chi-square test. Multivariate analysis of variance (MANOVA) was performed on participant demographic data, blood loss (measured intraoperatively), length of surgery, length of stay, and opioid use, to identify significant intervention group differences. To identify intervention effect on thigh swelling, timed up and go test, 10 metre walk test, and pain scale measured preoperative, 1 day, 3 days, and 2 weeks follow-up, a repeated analysis of variance was used. For the pain scale the Friedman ANOVA was selected for analysis. Statistical p values < 0.05 were acceptable levels for statistical significance.
Ethics approval for this study was sought and obtained from the Human Research Ethics Committee on 12 November 2013. The ethics committee approval number for this study is R0205/13.
As well as analysing the results of this trial, we compared the findings of this trial to a previously conducted study, which used the same methodology other than choice of DVT chemoprophylactic agent, which was 100 mg of aspirin for 30 days rather than enoxaparin. 3
Results
Following exclusions and loss to follow-up, 105 patients were analysed (Figure 1). Table 1 shows the preoperative details of the patients enrolled in this study. Demographics, ASA score and preoperative blood volume, Hb and HCT levels were similar across both groups. The length of surgery was not significantly different between the 2 groups (Table 2).
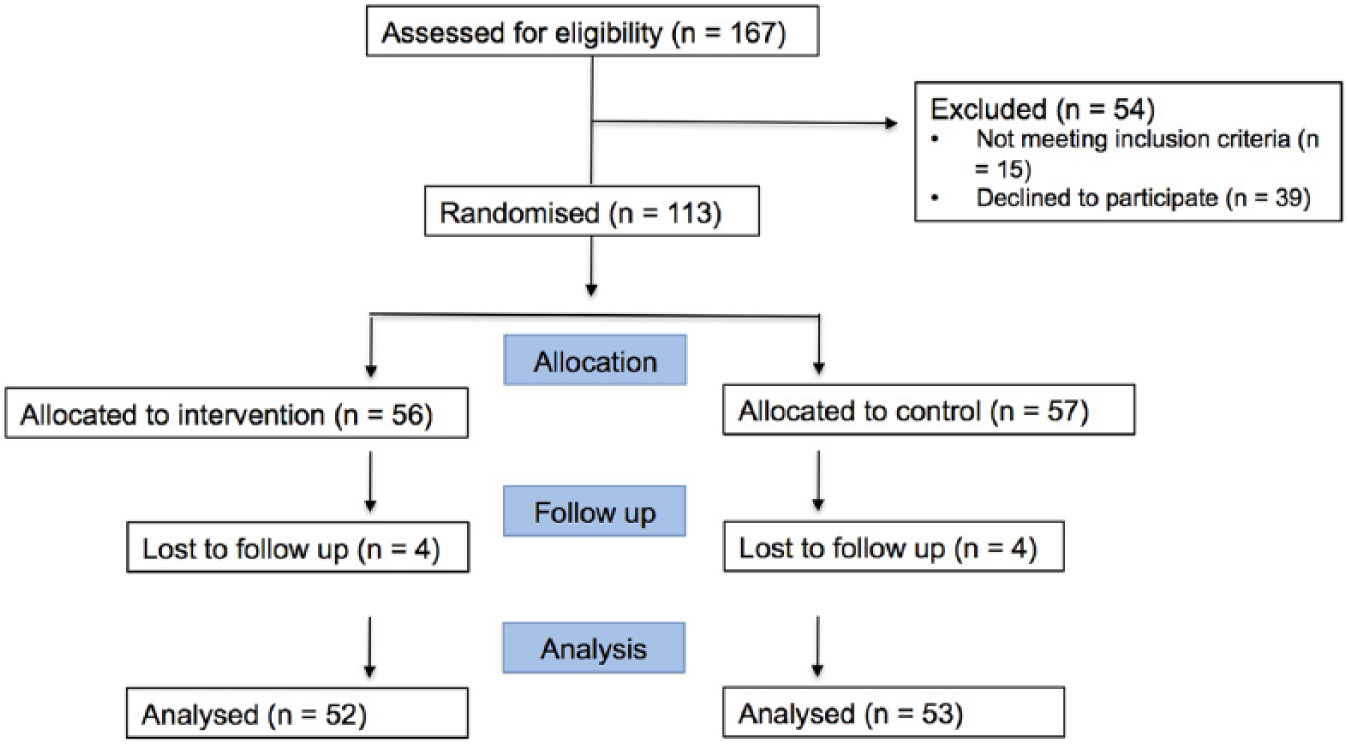
Trial Recruitment.
Demographics.
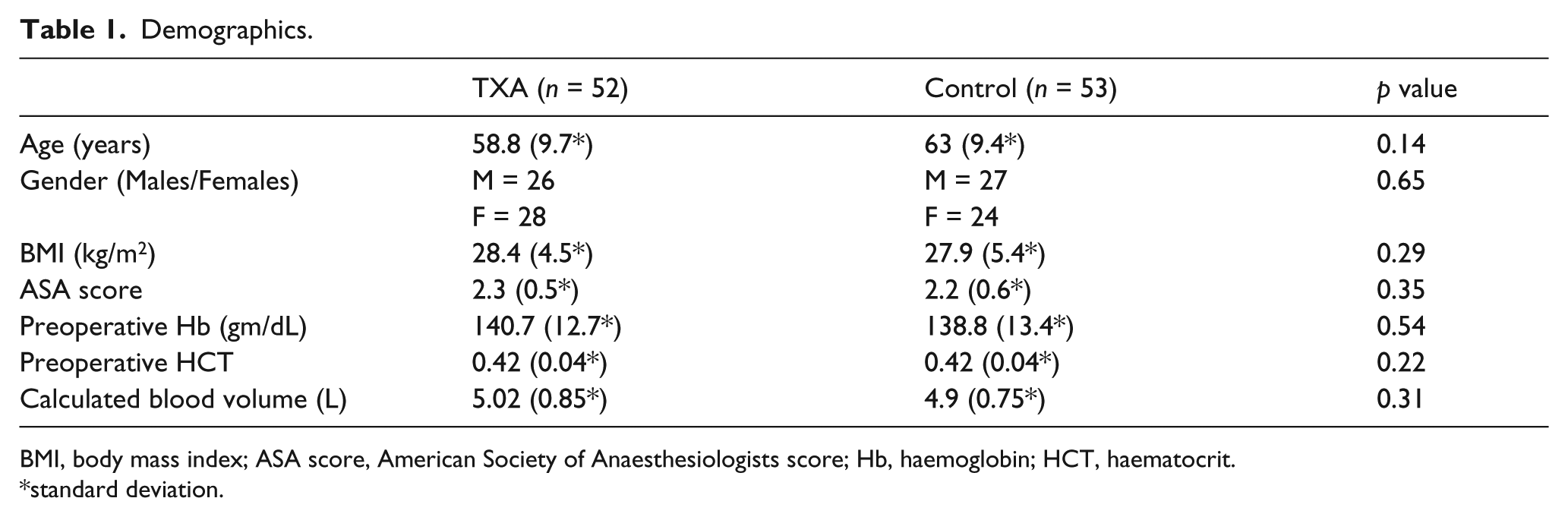
BMI, body mass index; ASA score, American Society of Anaesthesiologists score; Hb, haemoglobin; HCT, haematocrit.
standard deviation.
Analysis.
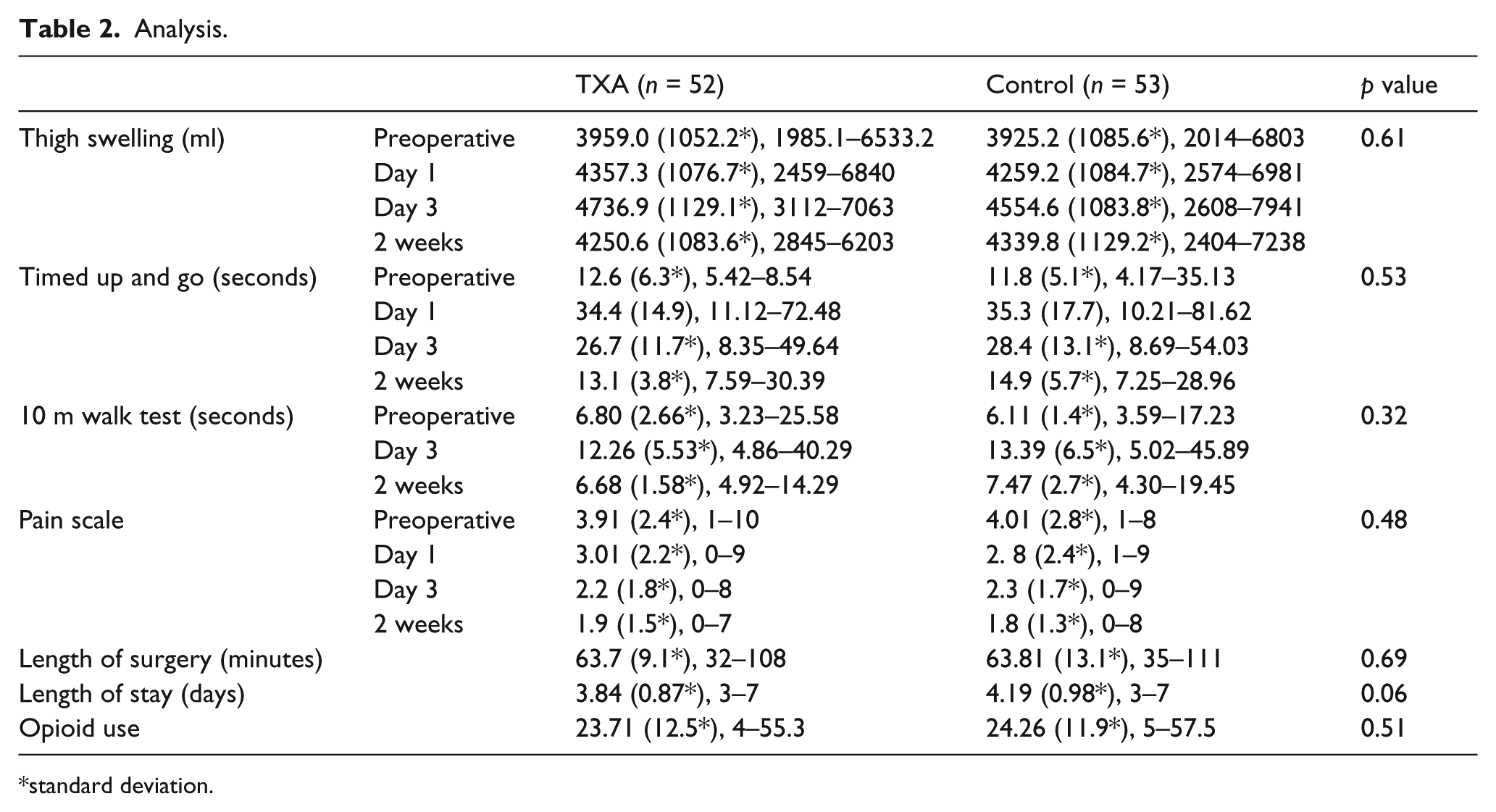
standard deviation.
Patients who received tranexamic acid did not have significantly less measurable thigh swelling as compared to the placebo group. There were no statistically significant differences between the measures of timed up and go and 10 m walk test across the 2 groups. There were also no differences in the postoperative pain scores nor opiate requirements. There was a reduction in length of stay for those who received TXA however this failed to show statistical significance (3.84 days, SD 0.87 versus 4.19 days, SD 0.98, p = 0.06) (Table 2).
There was significantly less intraoperative blood loss observed in the TXA group (0.510 L, SD 0.210) compared with the control group (0.698, SD 0.301) (p < 0.001). The estimated blood loss was also significantly less in the TXA group (1.130 L, SD 0.311) compared with the control group (1.48 L, SD 0.510) (p < 0.001) (Table 3). There were 5 patients requiring transfusion in the control group as compared to 1 in the TXA group however this failed to show statistical significance with an odds ratio (OR) of 5.00 (confidence interval [CI] 0.56–44.34) and a p value of 0.1484.
Blood loss.
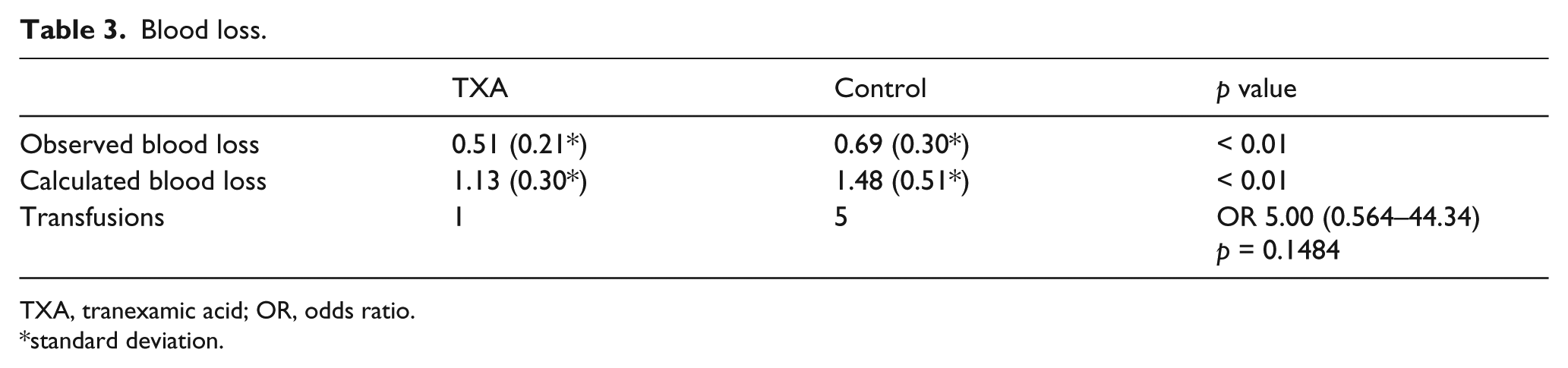
TXA, tranexamic acid; OR, odds ratio.
standard deviation.
There were no DVTs or PEs diagnosed in either the control or the experiment group. There were no wound infections, fractures or dislocations in either group.
When we compared the results to those of a OBTAIN A, 3 which followed the same methodology but used aspirin as the DVT chemoprophylaxis agent rather than enoxaparin, there was no difference in either thigh swelling at day 1 (4357.3 ml [SD 1076.7] versus 4509.5 ml [SD 884.8] p = 0.434), day 3 (4736.9 ml [SD 1129.1] versus 4633.4 ml [SD 961.5], p = 0.616) or 2 weeks (4250.6ml [SD1083.6] versus 4269.5 ml [SD 841.1] p = 0.921). There was also no difference in either the observed blood loss (0.51 L, SD 0.21 versus 0.460 L, SD 0.228, p = 0.442) or the calculated blood loss (1.13 L, SD 0.3 0 versus 1.084 L, SD 0.440, p = 0.760) of those that received tranexamic acid across the 2 trials. There was no significant difference in the age, gender, BMI or ASA score across these 2 trials.
Given that the blood conserving effect of TXA was not measurably different between the 2 DVT chemoprophlaxis agents, we performed an analysis after combining the data from the 2 trials. Our measures of thigh swelling, postoperative mobility and pain still showed no measurable difference between the control and experiment groups. There was a statistically significant reduction in length of stay for those that received TXA (3.72 days, SD 0.83 versus 4.24 days, SD 0.97, p < 0.001). There was also a statistically significant increased risk of a transfusion in the control group as compared those that received TXA (OR 5.5, 1.188 to 25.449, p = 0.029).
Discussion
We examined whether the blood conserving effect of tranexamic acid in total hip arthroplasty using the direct anterior approach translated to a measurable improvement in functional outcomes. The primary outcome measure was thigh swelling. Secondary outcome measures included, visual analogue pain score, timed up and go test, a 10 m walk test and length of stay. Blood loss and the incidence of blood transfusions was also recorded. We were not able to show a correlation between blood loss and these functional measures and there were no differences shown between the choice of either aspirin or enoxaparin across 2 trials using the same methodology other than choice of DVT chemoprophylaxis.
The limitations of this trial were that whilst we compared the efficacy of TXA across 2 consecutive randomised controlled trials with 2 different DVT chemoprophylactic agents, we did not compare the efficacy of TXA with no concurrent DVT chemoprophylactic agent. Sharfman et al. 5 reported on the use of TXA in the context of a variety of DVT chemoprophylactic combinations including the use of mechanical foot pumps without any chemoprophylactic agent. They were able to show a reduction in both blood loss and transfusions through exclusion of enoxaparin. This was an area not covered by this research.
During the planning phase of this research we hypothesised that patients who had less bleeding associated with their total hip replacement would in turn have less thigh swelling and subsequently have improved mobility and decreased pain in the perioperative period. Investigations into the clinical significance of the blood conserving effect of TXA in the setting of THR have previously been limited. Our research across both consecutive trials has been unable to draw a correlation between a reduction in blood loss with improved functional measures in the perioperative period. This finding suggests that although there is a statistically significant measureable reduction in blood loss, this reduction does not provide an advantage to patients recovering from their surgery from the perspective of having less pain or improved mobility.
An interesting finding of this study was that patients who received TXA, had a reduced length of stay. This was shown in both the trial using enoxaparin as DVT chemoprophylaxis as well as the pooled data across both trials. This finding is contrary to our other finding that there was no improvement in the measures of postoperative mobility or pain. We hypothesised that this increase in length of stay in the control group may be due to the fact that more patients in this group received transfusion. However following exclusion of patients that received transfusion in both groups, the length of stay was still significantly different across both the pooled data as well as the enoxaparin group. It may be that a combination of variables that were not captured by this study led to this finding. It is also possible that the measures we employed were not sensitive enough to correlate the blood conserving effect with postoperative functional outcomes. A further possibility is that this finding is suggestive of a type II error either because the numbers recruited were too small or our outcome measures employed were not sensitive enough.
There were fewer transfusions in the TXA group across both trials. Transfusions were relatively rare events in both consecutive trials. Although in each of the consecutive trials, the difference in transfusions failed to show statistical significance, when we pooled the data across both trials, we were able to show a statistically significant reduction in transfusions for those patients that received tranexamic acid. In other trials where transfusion was a rare event, largely due to more stringent transfusion protocols, no conclusion could be drawn regarding the efficacy of TXA in reducing the incidence of transfusions post total hip arthroplasty.12–15 Due to the size of our pooled cohort, which was significantly bigger than any previous randomised controlled trial investigating TXA in THR, we were able to show a statistically significant reduction in transfusion.
There were no recorded deep vein thrombosis or pulmonary embolism in either the control or experiment groups of either trial. This would suggest that both aspirin and enoxaparin when used in conjunction with TXA is a safe therapy from the perspective of acceptable thromboembolic rates. However we cannot draw firm conclusions in this area as this trial was not powered to provide evidence for safety with respect to thromboembolic events. As these events are rare, in order to prove safety in this area we would need a significantly larger cohort.
In conclusion, TXA is an effective agent in reducing blood loss in THR using the anterior approach and was not affected by choice of DVT chemoprophylaxis. Patients who received TXA had fewer transfusions and a reduction in their length of stay. The blood conserving effect of TXA was not associated with improved postoperative recovery across the measures of pain and mobility.
Footnotes
Acknowledgements
Vivian Zhou, Elsa Valenton, Dianne Misiti and Paul Nguyen for their work in theatre performing measurements as per the study protocol. Michelle Rose for her tireless efforts in attending to the logistics of trial progression.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.