
Abstract
Purpose:
The aim of this study was to determine the prevalence of asymptomatic radiographic findings of femoroacetabular impingement (FAI) in paediatric football players in different age groups and to investigate aetiological factors.
Methods:
Paediatric male athletes between 10 and 17 years of age from 8 soccer teams were recruited. In addition to an annual control check-up, anteroposterior pelvis and frog-leg radiographs as well as the curriculum vitae of the athletes, their injuries, and real-time complaints were recorded. The alpha angle, lateral centre-edge angle, Tönnis angle, and collodiaphyseal angle were measured and morphological abnormalities were noted.
Results:
There were 214 male football players with a mean age of 13.4 ± 3.2 years included in the study. In the morphological analysis of hips, there was FAI in 30% of the athletes. In the analysis of FAI prevalence in 3 subgroups based on age (Group 1: 10–12 years [n = 25], Group 2: 13–15 years [n = 104], Group 3: 16–17 years [n = 85]), there was 0% FAI in Group 1, 19.1% in Group 2 and 60% in Group 3. In the analysis of aetiological factors, there was no significant difference between the right and left hips of players regarding alpha angles and FAI prevalence. However, the prevalence of FAI was higher in players who had been playing football for 3 years or more and who had been training for 12.5 hours/week or more.
Conclusion:
Training for 12.5 hours or more per week in paediatric football players doubled the risk development of FAI morphology.
Keywords
Introduction
Femoroacetabular impingement (FAI) is abnormal contact between the acetabular rim and femoral head-neck junction secondary to the abnormal morphology of the hip joint.1,2 Diagnosis and treatment of FAI has become more frequent following the description of the mechanical theory by Ganz et al. 3 and its acceptance as a predisposing factor for osteoarthritis.4,5 The prevalence of FAI is higher in athletes due to physical activities that push the limits of the hip joint. 6 Some studies have shown that the prevalence of asymptomatic FAI in athletes was higher than the normal population, and the prevalence of FAI in asymptomatic athletes ranges from 30% to 72% according to the sports they participate in.7–10
The aetiology of FAI is still unclear, and the increased incidence of FAI has led to more investigation of aetiological factors. 11 Although genetic factors, acquired or developmental factors and the sequelae of paediatric diseases have been implicated, most authors have focused on acquired or developmental factors.12–15 A number of studies have investigated this issue in small numbers of volunteer paediatric athletes, with the activity level during the physeal closure period being implicated in contributing to the development of FAI.13,14,16
The aim of this study was to determine the prevalence of asymptomatic radiographic findings of FAI in paediatric football players of different age groups and to investigate aetiological factors, such as the dominant extremity, training hours and duration of sports participation, in FAI development.
Methods
Study groups
Between September 2015 and January 2016, 214 asymptomatic paediatric male football players with ages between 10–17 years were included in this study. These players were playing in the youth league of 1 super league club and 7 amateur clubs. The players who had any medical history of paediatric hip disease, fracture of lower extremity, neuromuscular, inflammatory or metabolic disease were excluded from the study.
This study was approved by the Institutional Review Board (IU2016/253) and informed consent form was voluntarily signed by all participants and parents who were included in the study.
In addition to the standard physical examination performed as a part of the seasonal controls for the players, a standard radiographic examination was performed by a trained radiographer using a low-dose, digital radiography technique (Digital Diagnost X-ray System, release 1.5, Philips Medical Systems DMC GmbH, Hamburg, Germany). Hips were kept in a neutral abduction-adduction position with the toes directed forward for the anteroposterior (AP) view. The radiographer ensured the volunteer was in the correct posture to avoid excessive tilt or rotation of the pelvis. Film and focus distances of 1.2 m were used with the beam centred 2 cm proximal to the pubic symphysis for the AP view and at the pubis symphysis for the frog-leg view. All radiographs had identifying information removed for patient confidentiality and were assessed by gross visual inspection on a high-resolution screen by 2 authors (GP and UA). Positioning of the pelvis on the AP view and presence or absence of any of the qualitative cam-type and pincer-type radiographic findings on the 2 views were noted. In AP and frog-leg views of the patients, the alpha angle, centre-edge (CE) angle, anterior femoral offset, Tönnis angle (TA), and collodiaphyseal angles (CDA) were measured with a digital program (Extreme-PACS, Ankara, Turkey) and morphological abnormalities (i.e., FAI, acetabular dysplasia, coxa valga and coxa vara) were noted.
After measuring the angles, a last gross visual inspection for all participants was conducted by 1 author (GP) to determine the presence of any specific deformities related to FAI, such as pistol grip, crossover sign, and lateral overcoverage, among others. The presence of a pincer-type deformity was determined by increased CE angles (>39°), decreased Tönnis angles (<0°) on AP views and any gross visual inspection findings, such as crossover signs. Cam-type deformities were determined by increased alpha angles (>55°), decreased anterior femoral offset (<10 mm) and any gross visual inspection finding, such as the pistol grip deformity in AP or frog-leg views.
In addition to the annual control check-up for the athletes, a previous medical profile regarding previous injuries, the athletes’ present complaints, hip range of motion, players’ dominant feet (the one that they hit the ball with), weekly training time (hours/week) and time between beginning playing football until their last annual check-up were collected and noted.
Statistical analysis
All statistical analyses were performed with the Statistical Package for the Social Sciences (SPSS) 20.0 (SPSS Inc, Chicago, IL, USA). Descriptive statistics were used to summarise patients’ demographic and baseline characteristics. We calculated the numbers and percentages of FAI prevalence for different age groups. One-way analysis of variance (ANOVAs) and Student’s t-tests were used to investigate differences in age, dominant feet, weekly training time (hours/week) and duration of playing football. The level of significance was set at p ⩽ 0.05.
Results
There were 214 paediatric male football players with a mean age of 13.4 ± 3.2 (range 10–17) years who were included in the study. The mean duration of sports participation was 3.9 ± 5.3 years. In the radiological measurements of the roentgenograms, the mean alpha angle was 50.7° for right hips and 50.3° for left hips, the mean lateral centre-edge angle (LCEA) was 28.6° for right hips and 29.5° for left hips, the mean TA was 6.6° for right hips and 5.0° for left hips, and the mean CDA was 133.9° for right hips and 134.7° for left hips. Measurement results of the players according to different age groups are summarised in Table 1.
The mean results of morphological analysis.
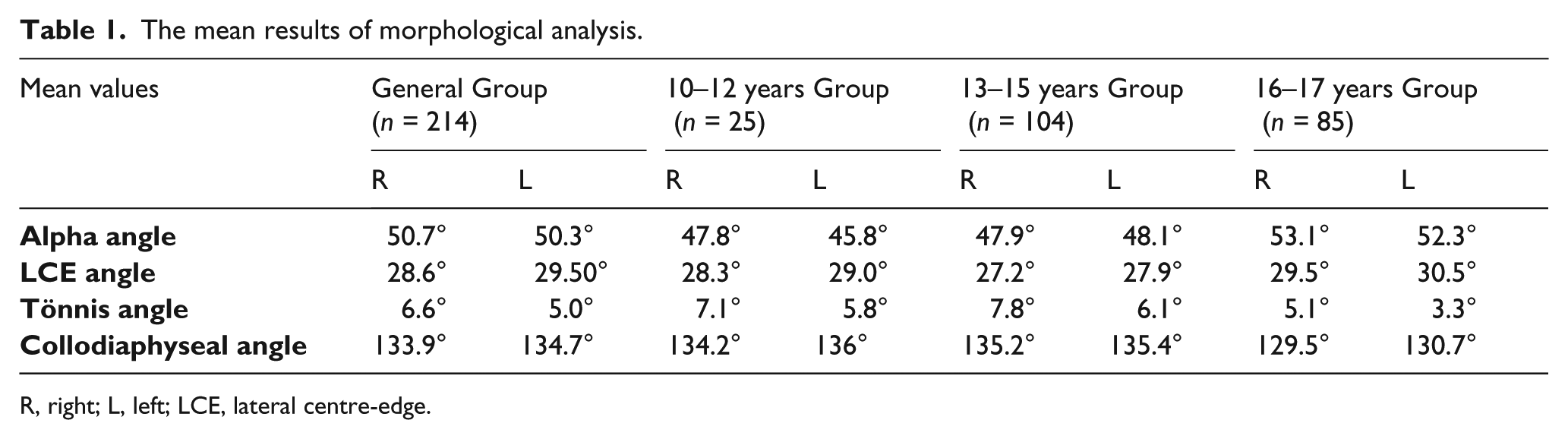
R, right; L, left; LCE, lateral centre-edge.
In the morphological analysis of hips, there were FAI in 30% of the athletes. There were cam-type FAI in 26.2%, pincer-type FAI in 1.9% and combined type FAI in 1.9% of the athletes. In addition, there were 7 asymptomatic athletes (3.3%) who had acetabular dysplasia. After categorising the players according to the age groups that they played sports in, 25 players aged between 10 and 12 years old were enrolled in Group 1, 104 players aged between 13 and 15 years old were enrolled in Group 2 and 85 players aged between 16 and 17 years old were enrolled in Group 3. According to the age groups, FAI prevalence was 0% in group 1, 19.1% in group 2 and 60% in group 3. These findings showed a significantly increased prevalence of FAI correlated with age in paediatric athletes (p < 0.05). The results of morphologic analysis of players in the subgroups are summarised in Table 2.
The results of the morphological analysis.
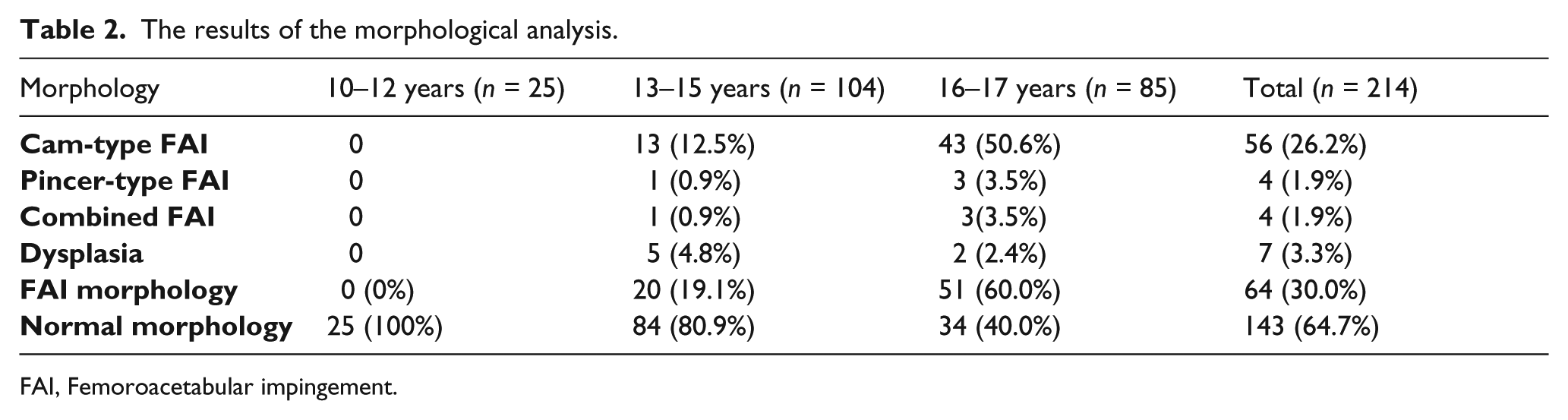
FAI, Femoroacetabular impingement.
Of the 214 athletes, 172 had a right side dominant extremity and 42 had left side. There were no significant differences (n.s.) between the morphological analysis of right and left hips of the players regarding alpha angles and FAI prevalence in the study group. The mean duration of sports participation of the study population was 3.9 ± 5.3 years. In the subgroup analysis of athletes, the players who had been playing football for less than 3 years had a FAI prevalence of 13.7%. The players who had been playing football for 3 or more years had a FAI prevalence of 39.5%, which was statistically significant (p = 0.01). Weekly training hours of the players were analysed as an aetiological factor, and the players were grouped into 2 subgroups according to the classification of the amount of training that the football clubs required. Subgroup 1 had a weekly training of less than 12.5 hours and the other subgroup trained for 12.5 hours or more. According to morphological analysis of the players, there was FAI in 31 of 135 players (22.9%) in subgroup 1 and 33 of 79 players (41.7%) in subgroup 2. There was a positive correlation between weekly training hours and FAI prevalence, and the study showed that the prevalence of FAI was higher in players who trained for more than 12.5 hours/week (p = 0.03) (Table 3).
Subgroup comparisons related to aetiological factors.
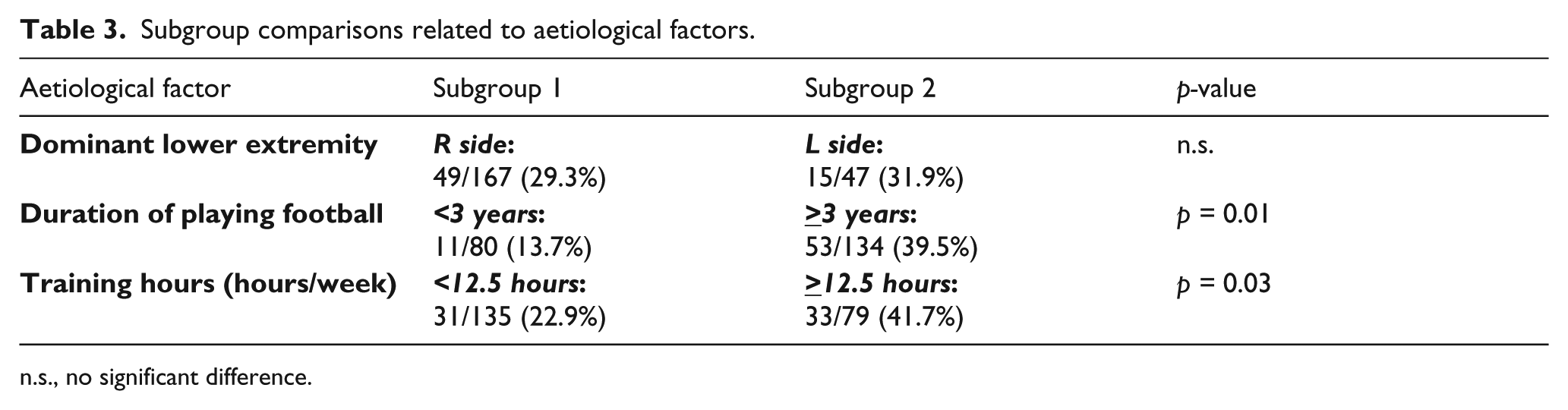
n.s., no significant difference.
There were 28 goalkeepers, 30 defenders, 21 strikers, 49 midfielders, 56 right wingers and 30 left wingers in the study population. According to the analysis, there were no statistically significant differences in FAI prevalence between the playing positions of the players.
Discussion
FAI received more focus after it was considered to be a predisposing factor for osteoarthritis.3,17 A higher frequency of FAI is seen in sports that are performed by leaning forward, such as ice hockey and football, among others. 9
It has been reported that this deformity, which is encountered to different degrees in different sports, can be found in up to 70% of asymptomatic athletes.7,9,18–20 Although the most frequent factor in the aetiology is the development of the hip deformity with acquired factors, there are publications that suggest that the deformation develops in paediatric or adolescent athletes during the femoral physeal closure period.11,13–15
In our study, we researched factors, such as the athlete’s dominant foot (the one that they use to kick the ball), weekly training period and duration of sports participation, which may have roles in the aetiology of FAI; we also investigated FAI frequency in 214 asymptomatic paediatric and adolescent football players.
In a study of 95 adult elite football players (20 females, 75 males), FAI was detected in 72% of the asymptomatic male and 50% of the female football players. 7 In this study, it was reported that cam-type deformities were detected in 68% of male athletes and 76.5% of these cases demonstrated bilateral cam lesions. 7 In a study evaluating 22 semi-professionals and 22 amateur football players, it was reported that the prevalence of FAI was higher in semi-professional players. 22
Studies on the aetiology of FAI have implicated genetic and racial causes as well as sequelae of paediatric diseases and developmental factors.12,15,23,24 Nevertheless, in recent studies of the paediatric athlete population, acquired factors became more prominent. 25 Activities that pushed the limits of the hip joint during the paediatric period and shearing forces at the hip joint during the femoral physeal closure period caused cam deformity.15,26 Although there have been several studies in the literature that investigate the prevalence of FAI in paediatric athletes, many studies have been conducted in a limited number of athletes, and few studies are available on paediatric football players.18,27–29 In 1 study, the authors examined the hip morphology of 89 football players and a control group of 92 individuals aged between 12 and 19 years. The authors reported a cam deformity ratio of 44% in the athlete group and reached the conclusion that the “cam-type deformities were recognisable and present from the age of 13 years and were more prevalent in football players than their nonathletic peers.” 29 In another prospective study of the same group, it was reported that FAI frequency and alpha angles increased in parallel with skeletal development in paediatric athletes. 30 In our study, we evaluated 214 paediatric athletes in different age groups. In the 10–12 age group, we did not have any patients with FAI morphology. However, we found a FAI prevalence of 13.1% in patients who were 13–15 years old and 45.1% for patients who were 16–17 years old. In our study, we observed that the development of deformities was more frequent in the age groups after closure of the femoral physis, and the frequency of FAI and alpha angles was positively correlated with age (p < 0.05).
In cam aetiology, the level of sporting activity, the dominant feet with which they hit the ball, the position of the player, and the athlete’s history of playing sports have been implicated. In a study that focused on the dominant feet of the athletes, it was reported that the alpha angles were significantly higher in the dominant feet. 22 We found no difference between the prevalence of FAI and alpha angle measurements between the dominant and non-dominant sides of the athletes in the evaluation of the 214 patients in our study group (n.s). There was no relationship between the development of FAI and the positions of the players (n.s). Another aetiological factor in the development of FAI was the amount of load on the hip joint during skeletal development.
In a study investigating the load on the hip joint, the authors concluded that the prevalence of cam deformities in adult elite athletes who started sports activities before they were 12 years old and trained 4 times a week was statistically higher than that in those who started after 12 years of age. 31 In our study, the mean age of starting sports was 8.9 ± 1.3 years. In comparing the 3 years or less to the 3 years or more group, the prevalence of FAI was statistically significantly higher in the athletes with more than 3 years of playing sports (p = 0.001). Along with the results of the subgroup analysis of the training hours they performed weekly in the clubs, the prevalence of FAI was higher in the group with 12.5 hours/week or more (41.7%) than the group of 12.5 hours/week or under (22.9%) (p = 0.01).
This study had some limitations. Firstly, the prevalence of cam deformities might have been underestimated because conventional radiographs were used. 3-dimensional imaging, such as computed tomography or magnetic resonance imaging, may be used for diagnosing FAI. However, due to high-dose exposure with computed tomography (CT) and the unavailability of magnetic resonance imaging (MRI) for a large group of asymptomatic paediatric volunteers, we chose to use 2 conventional graphs for radiological analysis. This study was one of the largest series that investigates paediatric FAI prevalence and aetiological factors to date.
Conclusion
In paediatric athletes, the most discussed aetiological factors that lead to the development of FAI are the shear forces on the hip joint during closure of the physis.31,32 Asymptomatic FAI deformities in paediatric athletes who participate in high-impact sport activities, such as football, were not seen in the 10–12 age group, however, the prevalence of these deformities can reach up to 60% in the 16–17 age group. It was put forth that changes during the physeal closure were relevant to the loads on the hips of football players. In our study, we have shown that the risk of developing FAI is doubled in paediatric athletes who trained 12.5 hours or more per week compared to those who train for less time.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.