
Abstract
Background:
Our main aim was to investigate whether obese patients were at increased risk of elevated metal ion levels and/or adverse local tissue reaction (ALTR) after being treated with articular surface replacement (ASR) hip arthroplasty.
Methods:
This study included 360 patients who underwent metal-on-metal (MoM) hip resurfacing (HRA) or total hip arthroplasty (THA). 95 patients (26%) were underweight/normal weight (BMI < 25 kg/m2), 139 (39%) were overweight (BMI 25–30 kg/m2), and 126 (36%) were obese (BMI ⩾ 30 kg/m2). Blood metal ion levels and patient-reported outcome measures (PROMs) were obtained, and a sub-cohort of 85 patients had MARS MRI performed. Logistic regression analyses were used to assess the associations between obesity and metal ions, as well as ALTR.
Results:
BMI was not associated with either elevated metal ion levels or ALTR. In HRA patients, female gender (OR 3.0; p = 0.019) and pain (OR 2.3; p = 0.046) were associated with elevated Co levels. Female patients had increased risk of elevated Cr levels (OR 3.0; p = 0.02). In THA patients, female gender (OR 2.2; p = 0.004) and VAS satisfaction (OR 2.1; p = 0.01) were associated with elevated Co levels. Female gender (OR 3.6; p = 0.001) and time from surgery (OR 1.4; p = 0.005) were associated with Cr levels. In the sub-cohort, ALTR was associated with Co levels (OR 16.1; p = 0.002) in HRA patients.
Conclusion:
Patients with BMI ⩾ 30 kg/m2 present no increased risk for elevated metal ion levels or development of ALTR.
Introduction
Obesity is defined as having a body mass index (BMI) of 30 kg/m2 or greater and has more than doubled worldwide since 1980. 1 According to the most recent figures from the World Health Organization, 13% of adults are obese and 39% are overweight (BMI 25-30 kg/m2). 1 Obesity is associated with several significant co-morbidities, such as cardiovascular disease, diabetes mellitus, hypertension, certain forms of cancers, and osteoarthritis (OA). 1 OA is the most common primary indication for total joint replacement surgery. Therefore, it is unsurprising that a higher BMI increases the risk for both total hip arthroplasty (THA) and total knee arthroplasty.2,3 Furthermore, the longevity of an implanted prosthesis should be maximised, because these patients are generally younger upon initial surgical intervention. 4
Since the advent of THA, various prosthetic materials have been used in an effort to achieve the most durable, effective, and safe implant. Metal-on-metal (MoM) hip articulations, used in both hip resurfacing arthroplasty (HRA) and THA, were implanted in more than 1 million patients worldwide during the 1990s and early 2000s with the hope of providing lower wear and decreased rate of dislocation compared to the metal-on-polyethylene designs of the time. 5 By 2010, the use of MoM declined after registry reports of higher than expected failure rates and concerns about adverse local tissue reactions (ALTRs). 6
Metal wear and corrosion can emanate from the prosthesis into the surrounding tissues and have been associated with ALTRs. 7 Understanding the factors that may increase the generation of these metal ion particles remains complex and critical to the follow-up of the thousands of patients in whom MoM hip implants remain in situ. It has been hypothesised that patients with higher BMIs will have increased edge loading and wear of the hip joint, which may contribute to higher metal ion levels. The effect of obesity on the failure of MoM hip resurfacing and THA remains unclear in the literature. Some studies have shown obesity has no association with elevated metal ion levels,8,9 while others have found high BMI to be associated with failure of MoM hip resurfacing secondary to ALTR.10,11
The primary aim of this study was to investigate whether obese patients (⩾30 kg/m2 BMI) were at increased risk of elevated blood metal ion levels if they were treated with the Articular Surface Replacement (ASR) Hip System (DePuy Orthopaedics, Warsaw, IN, USA). The secondary aim of this study sought to investigate if obesity was associated with a higher prevalence of ALTR in a sub-cohort of patients with annual metal artifact reduction sequence magnetic resonance imaging (MARS MRI).
Materials and methods
Patients who underwent hip arthroplasty with the Articular Surface Replacement (ASR) (DePuy Orthopaedics, Warsaw, IN, USA), resurfacing arthroplasty (HRA) or total hip arthroplasty (ASR XL), were enrolled in a prospective, multicentre study between May 2012 and June 2015 following the voluntary recall of this system. Details of this study are explained in previous literature.12,13
BMI was not required data in the follow-up study of the ASR hip system but was reported nonetheless by many sites. We only included data from centres that reported BMI data on 90% or more of the patients in our analyses in order to eliminate selection bias. Additionally, patients with a contralateral MoM THA or HRA or missing component information were excluded. All patients had a valid anteroposterior pelvis radiograph and blood metal ion level assessment (in parts per billion, ppb) within 6 months of enrollment. The final study (Cohort A) consisted of 360 patients (Figure 1).
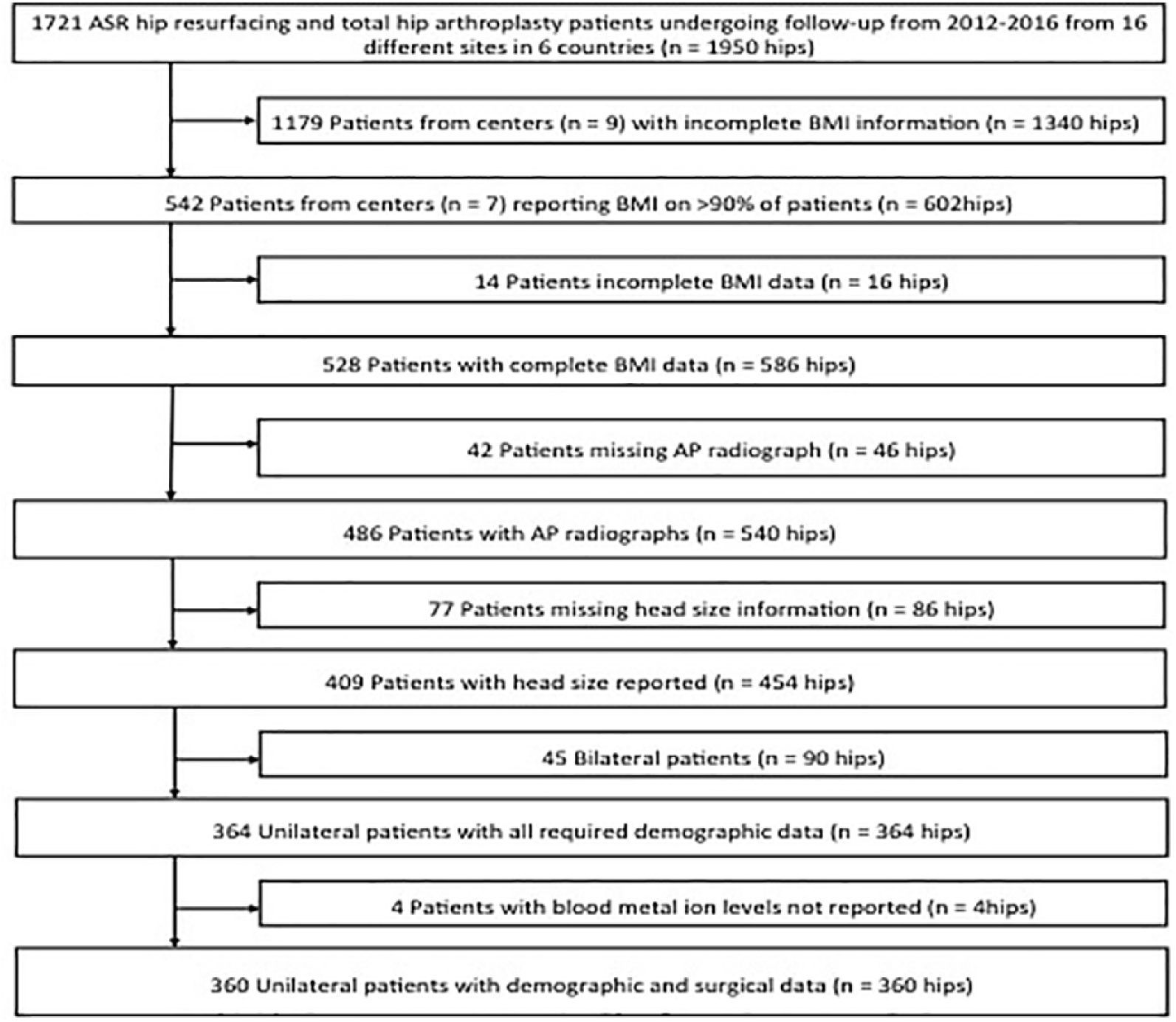
Flowchart of patient selection.
A subset of patients from Cohort A came from a single centre that performed MARS MRI at annual follow-up visits regardless of symptoms. This cohort (Sub-Cohort B) consisted of 85 patients (Figure 1). MRIs were assessed for the presence, location, and severity of ALTRs. The severity was classified using the grading system of Anderson et al.14,15 MRI assessment was performed by 1 of the authors with 2 years of experience reading MARS MRIs and was validated by a musculoskeletal radiologist with more than 10 years of experience reading MARS MRIs. This assessment was blinded to all clinical and surgical patient data.
Statistical analysis
Analyses were performed separately for patients with ASR HRA and ASR XL THA. First, binary logistic regression analysis was used to investigate the relationship between obesity, and other explanatory variables, with elevated blood metal ion levels. Cobalt levels ⩾ 4.0 ppb and Cr levels ⩾ 4.6 ppb were considered elevated according to the established cutoffs by Van Der Straeten et al. 16 BMI values were classified into 1 of 3 categories: underweight/normal weight (BMI < 25 kg/m2), overweight (25 ⩽ BMI < 30 kg/m2), and obese (BMI ⩾ 30 kg/m2). Continuous explanatory variables tested included time from surgery, Harris Hip Score (HHS), and Euro-QoL 5-D (EQ-5D), while the University of California at Los Angeles (UCLA) activity score was classified as an ordinal explanatory variable. Nominal explanatory variables included acetabular inclination angle (⩾ 55° or < 55°), large femoral head size (> 52 mm for men and > 48 mm for women), gender, visual analogue scale (VAS) pain (< 2 or ⩾ 2), VAS satisfaction (< 2 or ⩾ 2), EQ-5D mobility, and EQ-5D pain. The mobility and pain dimensions of the EQ-5D were converted to binary variables; none or some/extreme problems. Multivariable logistic regression analysis was conducted to control for confounding variables and identify significant independent risk factors if multiple variables from the binary logistic regression models were significant.
Secondly, in the analysis of Sub-Cohort B, outcomes were identified as either moderate or severe ALTR. The same methods used for the analysis of Cohort A were employed. Interobserver reliability for the assessment of ALTR grade was performed using Cohen’s kappa (κ). Interobserver reliability for assessment of ALTR grade (κ = 0.64) was substantial. A probability of < 0.05 was considered significant. Statistical analyses were performed using SPSS Version 19.0 (SPSS Inc., Chicago, IL, USA).
Results
ASR HRA
137 (38%) of the 360 patients in Cohort A underwent ASR HRA (Table 1). There were 28 females and 109 males in this group. 36 patients (26%) were underweight/normal weight, 63 patients (46%) were overweight, and 38 patients (28%) were obese. The median (interquartile range [IQR]) BMI for these patients was 26.8 kg/m2 (IQR 24.9–30.7). Median Co and Cr values were 1.3 ppb (IQR 0.6–3.3) and 1.6 ppb (IQR 0.9–3.6), respectively and were not statistically different among the 3 BMI categories (p = 0.620; p = 0.276) (Figure 2(a)). Elevated Co values (⩾ 4.0 ppb) were observed in 23% of patients, and elevated Cr values (⩾ 4.6 ppb) were observed in 20% of patients. There was no difference in the proportion of patients with elevated ions among the 3 BMI categories (p = 0.540; p = 0.148).
Demographics. SD = standard deviation.
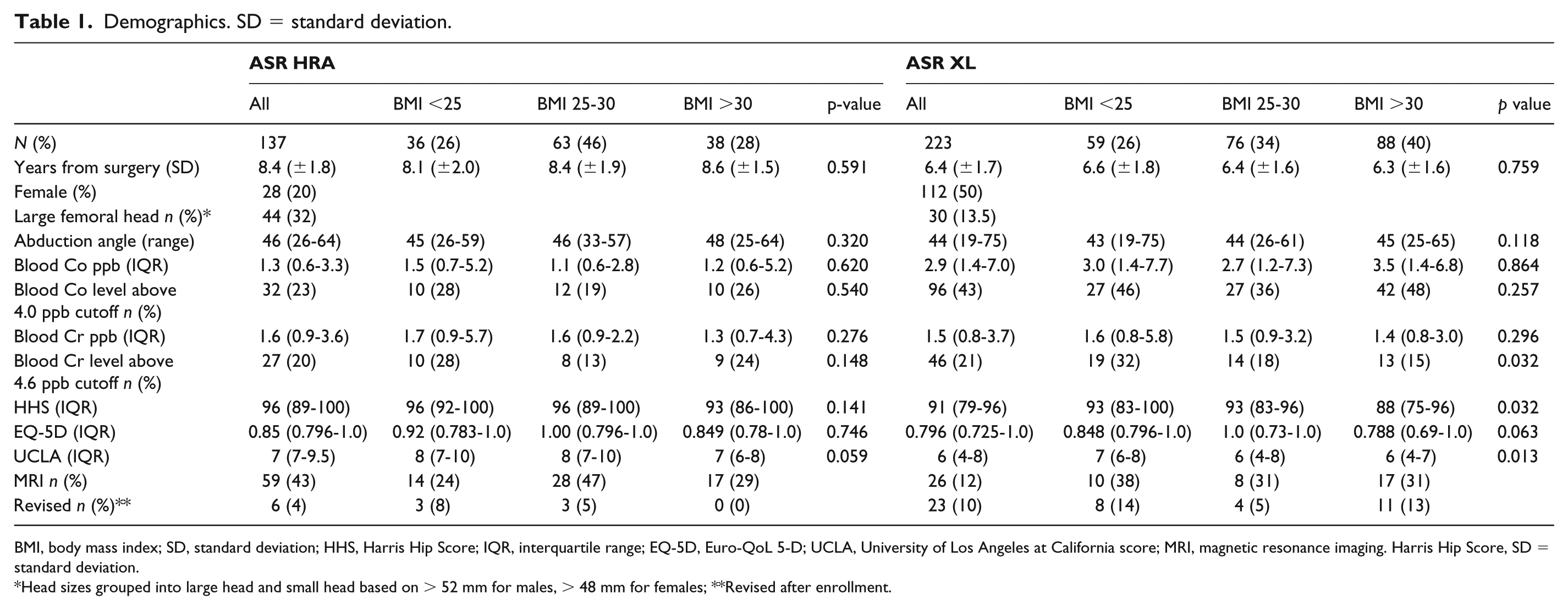
BMI, body mass index; SD, standard deviation; HHS, Harris Hip Score; IQR, interquartile range; EQ-5D, Euro-QoL 5-D; UCLA, University of Los Angeles at California score; MRI, magnetic resonance imaging. Harris Hip Score, SD = standard deviation.
Head sizes grouped into large head and small head based on > 52 mm for males, > 48 mm for females; **Revised after enrollment.
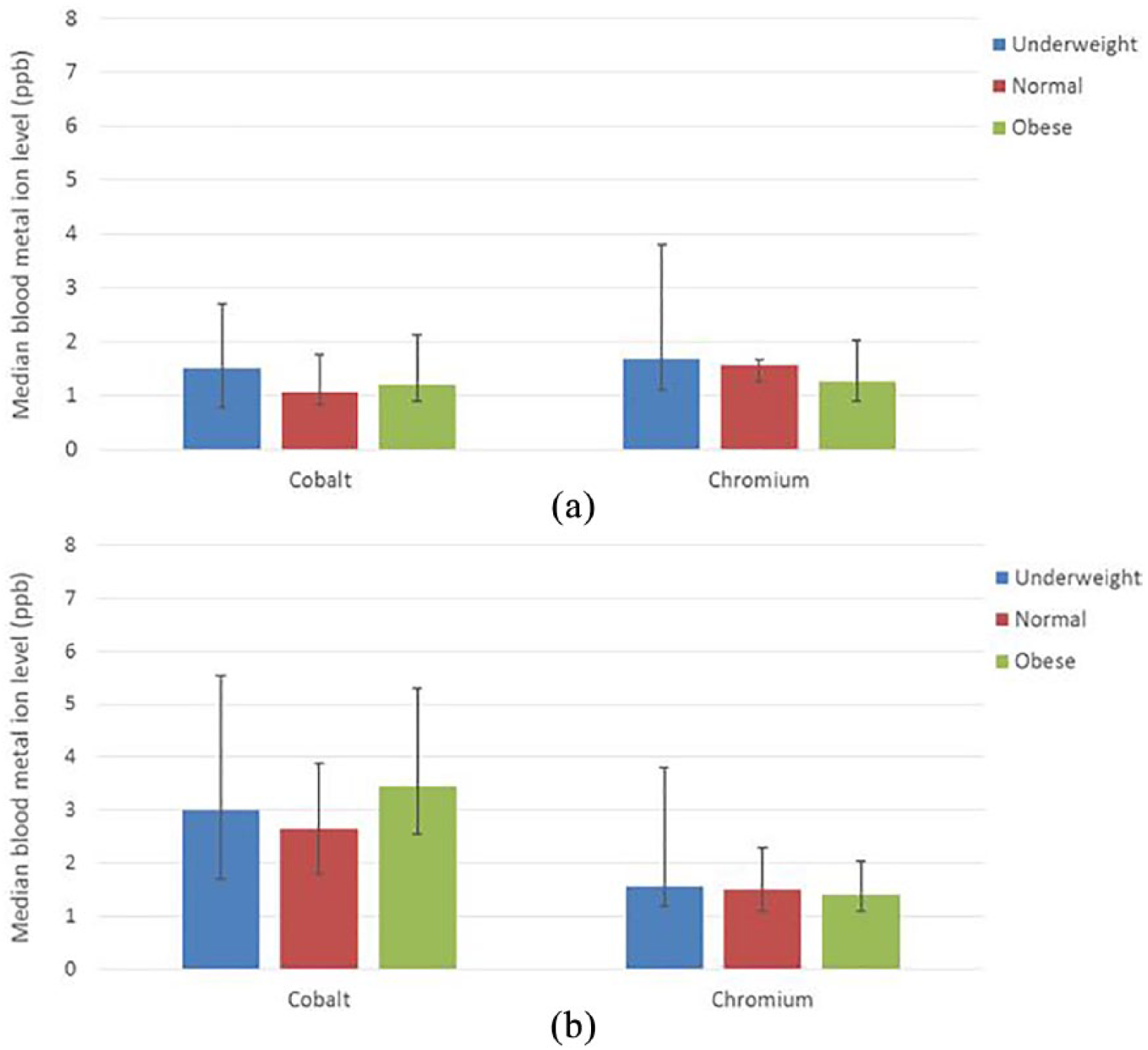
Median blood metal ion values divided by BMI category for patients treated with (a) ASR HRA and (b) ASR XL THA. Error bars show 95% confidence interval.
Multivariable logistic regression models built from the results of the univariate analysis (Table 2(a)) showed that the independent variables associated with elevated Co levels were female gender (odds ratio [OR] 3.0; 95% confidence interval [CI] 1.2–7.4; p = 0.019) and pain as reported by the EQ5D (OR 2.3; 95% CI 1.0 to 5.4; p = 0.046). The only significant independent predictor of elevated Cr levels was female gender (OR 3.0; 95% CI 1.2 to 7.6; p = 0.02) (Table 2(b)).
Univariate analysis for ASR HRA.
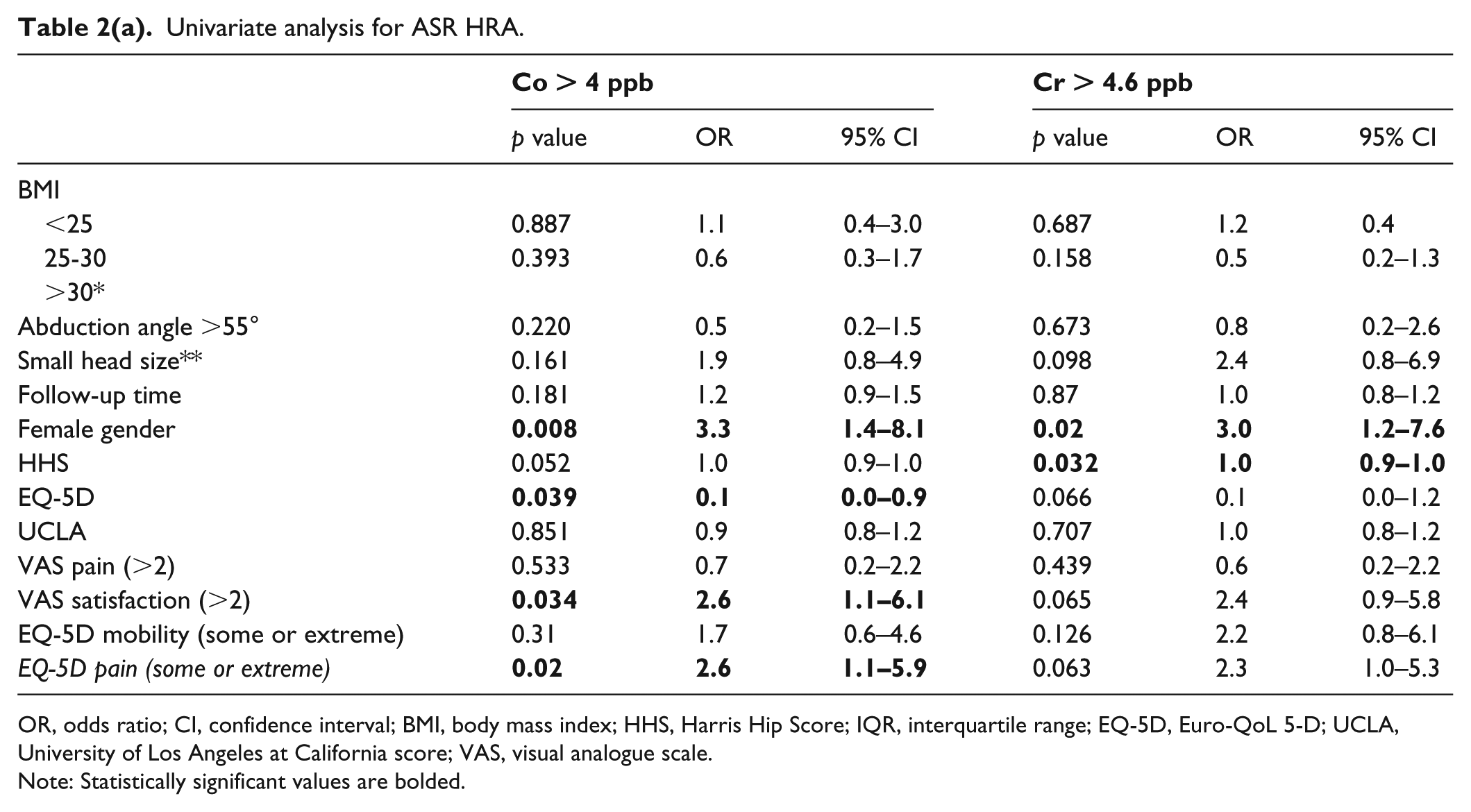
OR, odds ratio; CI, confidence interval; BMI, body mass index; HHS, Harris Hip Score; IQR, interquartile range; EQ-5D, Euro-QoL 5-D; UCLA, University of Los Angeles at California score; VAS, visual analogue scale.
Note: Statistically significant values are bolded.
Multivariate analysis for ASR HRA.
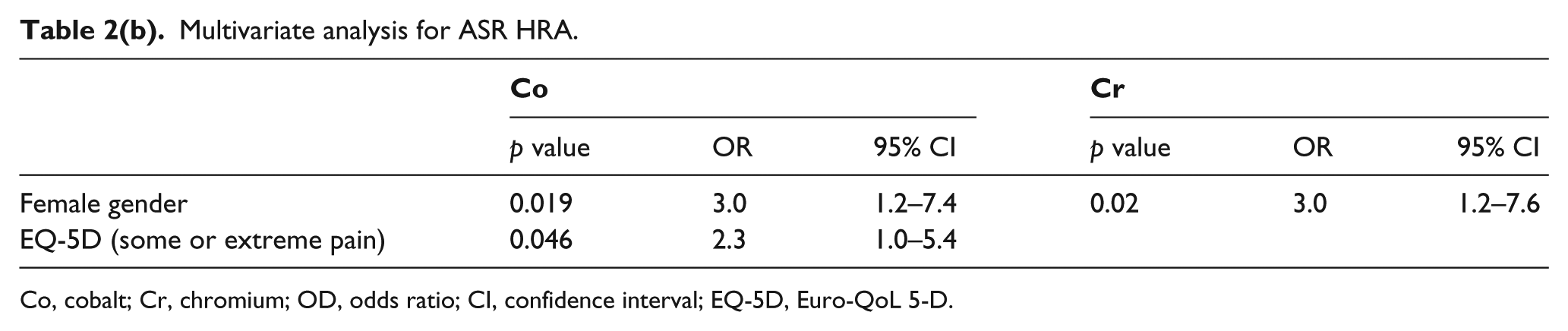
Co, cobalt; Cr, chromium; OD, odds ratio; CI, confidence interval; EQ-5D, Euro-QoL 5-D.
ASR XL
223 patients were treated with the ASR XL implant; 112 were female and 111 were male (Table 1). 59 patients (27%) were underweight/normal weight, 76 patients (34%) were overweight, and 88 patients (40%) were obese. The median BMI for these patients was 28.2 kg/m2 (IQR 24.8–32.7 kg/m2). Median Co and Cr values were 2.9 ppb (IQR 1.4–7.0) and 1.5 ppb (0.8–3.7), respectively and were not statistically different among the three BMI groups (p = 0.864; p = 0.296) (Figure 2(b)). Elevated Co values (⩾ 4.0 ppb) were observed in 43% of patients and elevated Cr levels (⩾ 4.6 ppb) were observed in 21% of patients. There was no difference in the proportion of patients with elevated Co levels among the 3 BMI categories (p = 0.257), but underweight/normal weight patients had a higher proportion of patients with elevated Cr levels (p = 0.032).
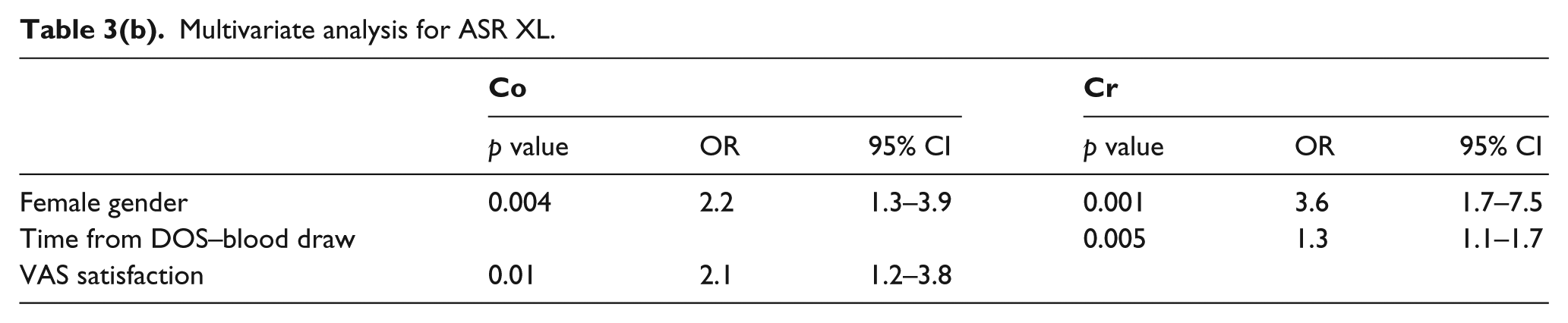
Multivariable logistic regression models built from the results of univariate analysis (Table 3a) showed that the only significant independent predictors of elevated Co levels were female gender (OR 2.2; 95% CI 1.3–3.9; p = 0.004) and VAS satisfaction (OR 2.1; 95% CI 1.2–3.8; p = 0.01). Female gender (OR 3.6; 95% CI 1.7–7.5; p = 0.001) and time from index surgery (OR 1.3; 95% CI 1.1–1.7; p = 0.005) were associated with elevated Cr levels (Table 3b).
Univariate analysis for ASR XL.
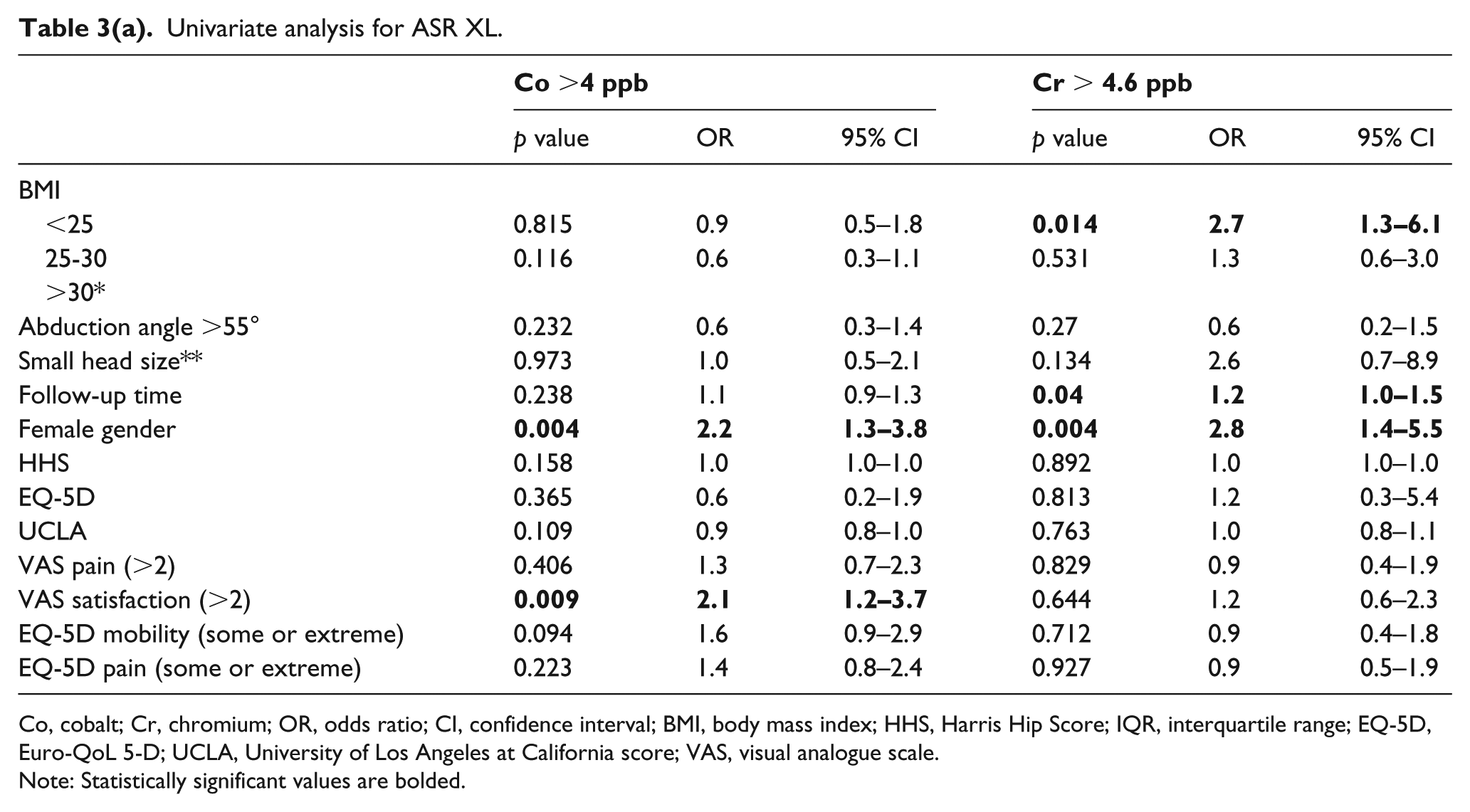
Co, cobalt; Cr, chromium; OR, odds ratio; CI, confidence interval; BMI, body mass index; HHS, Harris Hip Score; IQR, interquartile range; EQ-5D, Euro-QoL 5-D; UCLA, University of Los Angeles at California score; VAS, visual analogue scale.
Note: Statistically significant values are bolded.
Multivariate analysis for ASR XL.
Sub-Cohort B
Sub-Cohort B consisted of 85 patients (59 ASR HRA, 26 ASR XL) from a single centre with MARS MRI performed at a mean of 9.0 ± 1.6 years (ASR HRA) and 7.5 ± 1.6 years (ASR XL). The median BMI for the ASR HRA patients was 26.8 kg/m2 (range 20–41 kg/m2) and 28.2 kg/m2 (range 18–37 kg/m2) for ASR XL patients. For ASR HRA patients, only elevated Co levels (⩾ 4 ppb) were associated with the presence of ALTR (OR 16.1; 95% CI 2.7–94.6; p = 0.002). For ASR XL patients, no variables were found to be significantly associated with the presence of ALTR.
Discussion
Currently, thousands of patients implanted with MoM articulations are undergoing follow-up, and understanding factors that may contribute to the failure of these implants is imperative. Furthermore, literature on the effect of obesity on metal ion generation and the development of ALTR has been inconsistent. This study investigated the relationship between obesity and elevated blood metal ion levels. This study also examined whether obesity had any effect on the development of ALTR in a subset of patients where MARS MRI was performed. We found that obesity was not associated with elevated blood metal ion levels or the presence of ALTR.
In ASR HRA patients, female patients were found to be at increased risk for both elevated Co and Cr, and patients with pain were at risk for elevated Co. In patients with ASR XL THA, female patients, as well as patients who reported low satisfaction with their surgery, were at increased risk for elevated Co levels. Female gender and increased time from surgery were associated with elevated Cr levels. ASR HRA patients with Co levels ⩾ 4 ppb who underwent MARS MRI were at increased risk of developing moderate/severe ALTR. No variables were associated with the presence or severity of ALTR in ASR XL patients.
We observed a trend for an inverse relationship between blood Cr levels and BMI in both ASR HRA and ASR XL THA. This was neither statistically nor clinically significant, as the median Cr values were well below established safe upper limits. 16 A higher proportion of underweight/normal weight patients (BMI < 25 kg/m2) had elevated Cr levels (⩾ 4.6 ppb) compared to overweight and obese patients. A recent analysis of 113 patients with MoM HRA and THA identified no evidence of higher metal ion levels in obese patients, yet did observe a similar trend for lower metal ion levels in obese patients. 8 This trend did not reach statistical significance. The median values were lower than the established safe upper limits, which made it difficult to interpret any clinical significance. Few other studies have examined the effect of obesity on blood metal ion levels while accounting for appropriate confounding variables. Of those that have, none have identified a significant relationship between BMI and metal ion levels.9,17 These studies were limited in their analyses because they included either a mixture of HRA and THA implant designs or patients with bilateral implants.
Female patients were at increased risk for elevated Co and Cr levels in both ASR HRA and ASR XL patients. This is consistent with several studies reporting differences in metal ion levels between genders.12,13,18 Female patients seem to fare worse with these implants, as other studies also have indicated they are at increased risk for revision surgery and ALTR. 19 It has been suggested that the smaller femoral head size used in females undergoing hip arthroplasty may contribute to inferior outcomes. Interestingly, in our analyses, head size was not associated with either elevated metal ion levels or development of ALTR.
Most studies that have looked at the effect of obesity on the prevalence of ALTR have found no relationship between them. 20 Our results are consistent with this finding, as only elevated Co levels were found to be predictive of ALTR in ASR HRA patients. This is similar to other studies reporting an association between Co levels and joint failure secondary to ALTR.21,22 Only 1 study to date has suggested high BMI is a risk factor for failure of MoM HRA secondary to ALTR. 10
Several studies have acknowledged no clear relationship between the level of activity and metal ion concentrations in patients with MoM HRA, although it has been suggested that higher activity results in greater implant wear.23,24 No association between activity level and metal ion concentrations was observed in our univariate analysis in either MoM HRA or THA. It is interesting to note that neither BMI nor activity level were associated with elevated blood metal ion levels, because it has been hypothesised frequently that these 2 factors contribute to metal ion generation via edge loading.8,25,26
We acknowledge that our study had some limitations. First, we were able to use only BMI as a surrogate for a patient’s body composition, which may fail to distinguish between lean body mass and fat content. 27 Additionally, BMI was not a required variable in data collection. Therefore, our analyses were limited to analysing data from sites that reported BMI on over 90% of patients in order to avoid selection bias. This led to a significantly smaller sample size than would have been possible if analysing other covariates and blood metal ion levels. Finally, this study analysed the effects of obesity on the ASR Hip System only. The ASR and ASR XL are recalled implants, and this invariably results in challenges when trying to extrapolate the results of the present study to other MoM implants. The design of the non-hemispherical ASR acetabular component is unique. 28 Therefore, we believe it is critical to examine this implant on its own, as the process of metal ion generation has been hypothesized to be different for various MoM acetabular cup designs.23,29
This study reports analyses from the largest prospective multicenter dataset on this topic to date. Many previous studies have looked at cohorts with mixed MoM implant designs.8,9 However, this study narrows the focus by examining the effect of obesity and other covariates on blood metal ion levels and ALTR in the ASR Hip System specifically. Furthermore, we provide data separately on these relationships in both the ASR HRA and ASR XL THA cohorts. We believe this to be very important, because other studies have noted that the mode of failure in MoM THA is likely attributable to taper corrosion rather than edge loading, as seen in MoM HRA. 30 This study also accounted for important confounding variables such as acetabular inclination angle, femoral head size, gender, time from index surgery, and patient-reported outcome measures (PROMs), all of which aided in eliciting a much more robust analysis of the relationship between BMI and blood metal ion levels. Future research should investigate whether these relationships persist in patient populations with other MoM implants.
The effects of obesity on hip failure with revision as the endpoint warrants further investigation in this patient cohort, as our study did not have enough patients revised at the time of this report to provide accurate analysis. Previous research in patients with another MoM HRA implant indicated that patients with higher BMIs actually have better implant survival. 27 It is unknown if this effect holds true in patients with ASR HRA and ASR XL THA.
Conclusion
In conclusion, we provide evidence that BMI does not play a significant role in the generation of metal ion levels in patients with ASR HRA or ASR THA components. Long-term follow-up of MoM patients requires special considerations as recommended by several regulatory agencies, but our results demonstrate that patients with high BMI present no increased risk for elevated metal ion levels or development of ALTR. We did find female patients to be at greater risk for elevated blood metal ion levels, which aligns with the findings of other studies. We recommend the levels of metal ions be measured regularly for all patients with MoM arthroplasty, and do not believe that increased vigilance is required for obese patients.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This study was supported by DePuy Synthes.