
Abstract
Introduction:
Adequate initial stability of the acetabular cup is essential for total hip arthroplasty (THA). However, changes in the alignment of the acetabular component caused by screw fixation are concerning in patients with inadequate bone stock. This study aimed to investigate the effects of screw fixation on the alignment of the acetabular component in THA patients with hip dysplasia.
Methods:
We retrospectively examined 256 hips (range 28–87 years) that underwent THA using a navigation system. Patients were divided into 2 groups based on the presence or absence of changes in the alignment of the intraoperative acetabular cup, and univariate and multivariate analyses were performed to identify factors that were predictive of changes in acetabular component alignment after screw fixation in 2 dimensions: inclination and anteversion.
Results:
Screw fixation led to a mean change in inclination of 1.6° (range 0–10°) and a mean change in anteversion of 1.4° (range 0–14°). The Crowe classification, the presence of bone cysts, and the use of an inferior quadrant screw were identified as factors that correlated with acetabular cup alignment changes in inclination (odds ratios, 6.01, 5.94 and 0.03, respectively). Only the Crowe classification was identified as a factor that correlated with intraoperative alignment changes in anteversion (odds ratio, 2.08).
Conclusions:
Screw fixation altered the acetabular cup alignment. The inclination changes were related to the extent of the dysplasia, and the risk was reduced when the inferior quadrant screw was used. Surgeons should use caution during screw fixation in THAs performed on severely dysplastic hips.
Introduction
Adequate initial fixation of the acetabular cup can be achieved without using supplemental screws in a total hip arthroplasty (THA) when a patient’s bones are of good quality.1,2 Because insufficient primary cup fixation may lead to early loosening, 3 THA in osteoporotic patients with poor bone quality requires 1 or more screws to achieve adequate initial cup fixation.4–6 However, screw fixation may cause changes in cup alignment, particularly when multiple screws are used. 7
Intraoperative positioning of the acetabular component influences the THA periprosthetic dislocation rates and material wear characteristics. 8 Therefore, implanting the acetabular component in the optimal position and at the optimal angle is crucial to avoid dislocation after a THA. 9 A computer navigation system may precisely determine acetabular cup position. 10 Although we have performed THAs using a computed tomography (CT)-based navigation system for precise implantation, the successful performance of uncemented acetabular cup implantation in patients with dysplastic hips remains challenging. 11 The use of porous tantalum modular acetabular components for dysplastic hips has resulted in satisfactory mid-term clinical and radiographic results. 12 These materials promote bony ingrowth and enable strong fixation in dysplastic hips. Compared to patients with adequate acetabulum coverage, such as patients with primary osteoarthritis of the hip or idiopathic osteonecrosis of the femoral head, the rigidity of the acetabular component and alignment changes after screw fixation warrant concern in patients with developmental dysplasia of the hip (DDH). The purpose of this study was to examine the risk factors for acetabular component alignment changes in THA procedures, specifically in DDH patients.
Methods
Patient background characteristics
This study was approved by the institutional review board at our hospital (K1609-507-001). This was a retrospective study of 256 hips in 229 consecutive patients (210 hips in 187 women and 46 hips in 42 men) who underwent a THA using a CT-based navigation system (VectorVision HIP 3.5; BrainLAB, Tokyo, Japan) at our hospital between January 2011 and August 2015. All patients were retrospectively identified from the hospital database. For all patients, surgeons planned to use a cementless cup (AMS HA cup, Kyocera, Kyoto, Japan) for the THA. The mean patient age at the time of surgery was 62 years (range 28–87 years). The femoral head subluxation severity was graded according to the Crowe classification. 13 In this study, 195 hips were Crowe grade 1, 43 hips were grade 2, 9 hips were grade 3, and 9 hips were grade 4.
Preoperative planning and navigation system
Preoperative CT images were acquired from the pelvis to the knee joint using a multi-slice CT scanner (Discovery CT750HD; GE Medical Systems, Milwaukee, WI, USA). Imaging settings were as follows: tube voltage, 120 kV; tube current, 150 mA; slice thickness, 2 mm; and slice pitch, 2 mm. CT image data was saved in the DICOM (digital imaging and communications in medicine) format and were transferred into the navigation system for preoperative planning and intraoperative registration. In the planning module, the anterior pelvic plane, containing the bilateral anterior superior iliac spine (ASIS) and the pubic tubercle, was identified. Before the surgery, 2 Schantz screws, 4 mm in diameter, were inserted percutaneously through stab incisions into the ipsilateral iliac crest approximately 5 mm proximal to the ASIS while the patient was in the supine position. A T-shaped reference array with 3 infrared reflection spheres was then fixed to the Schantz screws. Pelvic registration was performed using landmark matching on the patient’s body. Real-time information was provided to the surgeon by linking the 3-dimensional image of the patient’s pelvis that was constructed from a preoperative CT to the positions of the landmarks. The surfaces of the ASIS and the iliac crest were registered. The navigation accuracy was confirmed by touching the ASIS and the iliac crest using a pointer. Implantation was initiated once the navigation accuracy was ⩽2 mm.
Operative technique
All operations were performed by the same experienced surgeon using a direct lateral (Hardinge) approach. The anterior 1/3 of the gluteus medius was detached from the greater trochanter. We used the 2-mm under-reaming technique to prepare the acetabulum. In all patients, a hemispherical, uncemented acetabular component (AMS HA cup, Kyocera) was placed on the acetabular side and fixed with 1 or more screws. The rough surface of the AMS hemispherical titanium acetabular cup, on which hydroxyapatite (HA) was coated, was created using titanium arc spraying with an average 40 µm surface roughness and 400 µm maximum roughness. 14 The screws employed were 15-mm long with a 6.5-mm outer diameter. The inferior quadrant screw was fixed in the inferoposterior part of the acetabular component prior to fixation of the other screws (Figure 1). The inferior quadrant screw was not used in the first 104 hips but was used in the subsequent 152 hips. We aimed for a cup placement with a cup centre-edge (CE) angle of ⩾ 10° and < 2 cm of maximum superior shift from the inter-teardrop line. 15 Bulk bone grafting was used to obtain a reliable cup fixation in patients whose cup-CE angle was <10°. A PerFix 910 stem (Kyocera) was used for the femoral side. After hand reaming, the stem was broached until tight contact was achieved. Before final fixation, we confirmed the stability, leg length, and joint range of motion. A PerFix stem of the same size as the stem used in the trial was fixed, and a femoral head of appropriate size was selected. Finally, the gluteus medius was re-attached to the greater trochanter.
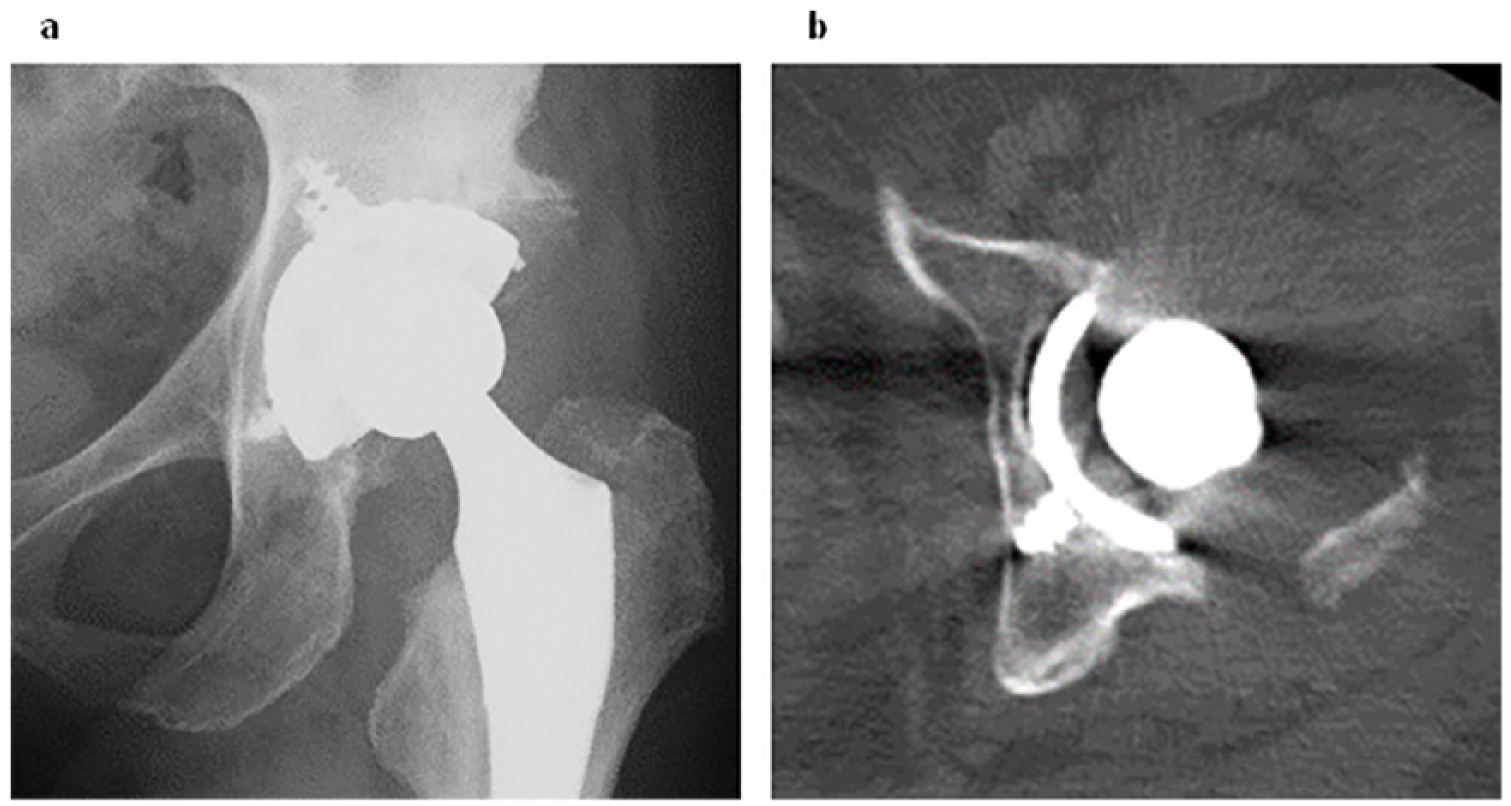
The inferior quadrant screw was fixed in the inferoposterior part of the acetabular component prior to fixation of the other screws (a). An axial computed tomography scan shows the inferior quadrant screw inserted towards the ischium (b).
Intraoperative measurements
During cup fixation, the surgeon adjusted the cup placement angle in real time using the navigation system (Figure 2). The inclination and anteversion of the acetabular component were measured during the press-fit of the cup and after screw fixation by the surgeons, who checked 5 points on the outer edge of the cup using the pointer. The measurement was carried out 3 times, and the average values were recorded as the cup inclination and anteversion angles. On the navigation system screen, cup angle was displayed in the operative definition. 16 The total number of screws that were required for fixation, including the inferior quadrant screw, was documented.
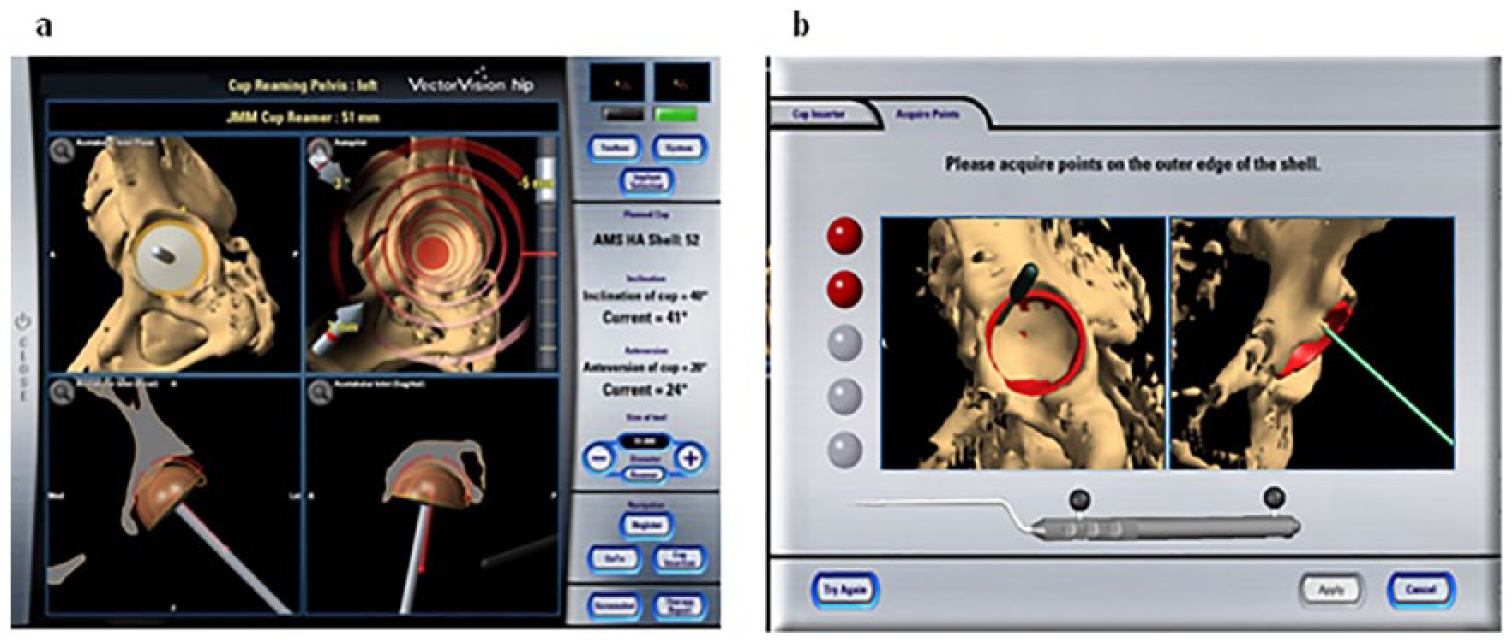
The acetabular component was fixed using a computed tomography-based navigation system in accordance with the preoperative planning (a). Cup inclination and anteversion angles were calculated by determining 5 peripheral cup edge points before and after screw fixation (b).
Statistical analysis
Paired t-testing was used to compare the differences in each value before and after screw fixation. For data without a normal distribution, a Wilcoxon signed-rank test was used. Variables with a normal distribution were compared using Student’s t-test, and variables with a non-normal distribution were compared using the Mann-Whitney U-test. Chi-squared tests were used to compare the differences in the sex ratio and the Crowe classification. The patients were divided into 2 groups, either with or without a 5° change in acetabular component alignment, and univariate analyses of cup inclination and anteversion were performed by comparing the 2 groups. A multiple logistic regression analysis was performed with the acetabular component alignment change as the response variable and the potential predictive variables as the explanatory variables. Potential predictive variables were included in the multivariate model when values of p < 0.05 were obtained in the univariate analysis. Cohen’s d values were calculated to evaluate effect sizes (ESs). The ES values of < 0.5, 0.5 to < 0.8, and ⩾ 0.8 have been suggested to represent small, medium, and large treatment effects, respectively. 17 The values are shown as the mean ± standard deviation, and values of p < 0.05 were considered statistically significant. Statistical analysis was conducted using SPSS version 18 software (IBM Corporation, Armonk, NY, USA) for Windows (Microsoft Corporation, Redmond, WA, USA).
Results
Intraoperative cup alignment
On average, 3.6 screws were used (range 1–6) per patient. The mean inclination and anteversion angles at the time of surgery are shown in Table 1. The mean changes in intraoperative acetabular cup position were 1.2 ± 2.1° (range -4–10°) for inclination and 0.2 ± 2.2° (range -14–11°) for anteversion. The cup inclination after screw fixation was significantly greater than during the press-fit (p < 0.0001; ES, 0.44), while no significant difference in cup anteversion (p = 0.75; ES, 0.03) was observed between the measurements obtained at press-fit and screw fixation. The mean absolute values of intraoperative acetabular cup position changes were 1.6 ± 1.9° (range 0–10°) for inclination and 1.4 ± 1.7° (range 0–14°) for anteversion. The ES was medium for the absolute value of intraoperative change for both cup inclination and anteversion (0.53 and 0.51, respectively). These results indicate that cup position was significantly altered after screw fixation.
Intraoperative changes in inclination and anteversion.
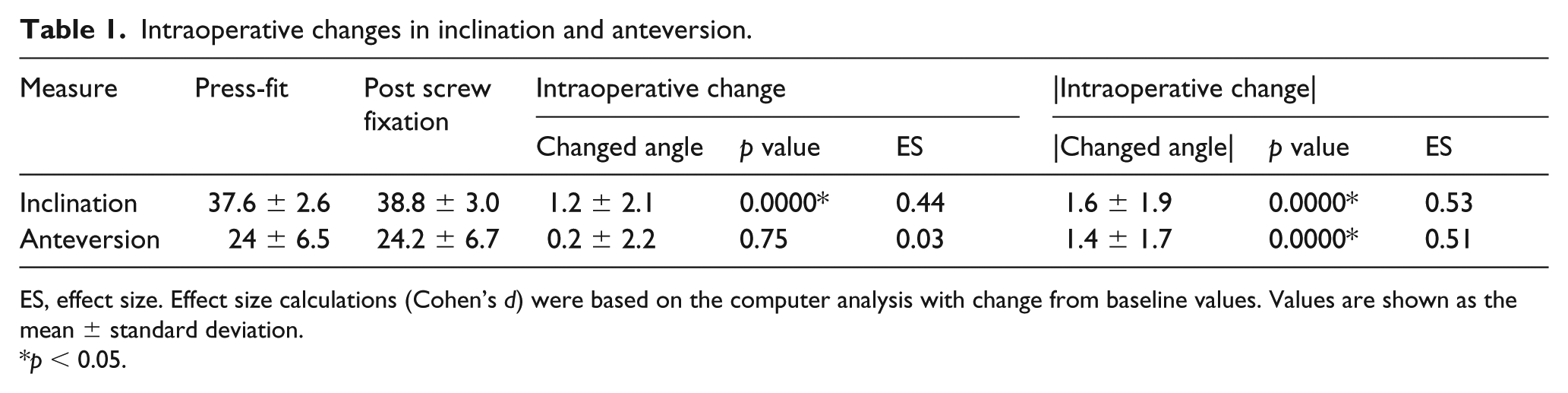
ES, effect size. Effect size calculations (Cohen’s d) were based on the computer analysis with change from baseline values. Values are shown as the mean ± standard deviation.
p < 0.05.
Next, we investigated if the severity of preoperative hip deformity influenced the cup alignment change after screw fixation (Figure 3(a) and (b)). There were significant differences in both cup inclination and anteversion depending on the severity of preoperative hip deformity. We also performed univariate analyses to investigate the inhibitory effect of using the inferior quadrant screw on the acetabular cup alignment change during supplemental screw fixation (Figure 3(c) and (d)). No significant differences were identified between the 2 groups in the population data (age, gender ratio, body mass index, Crowe classification, bone cysts, and bone graft), except for the number of screws required (Supplementary Table 1). The cup alignment change in inclination was significantly smaller in patients with an inferior quadrant screw fixation, while the cup alignment change in anteversion was not influenced by the use of the inferior quadrant screw.
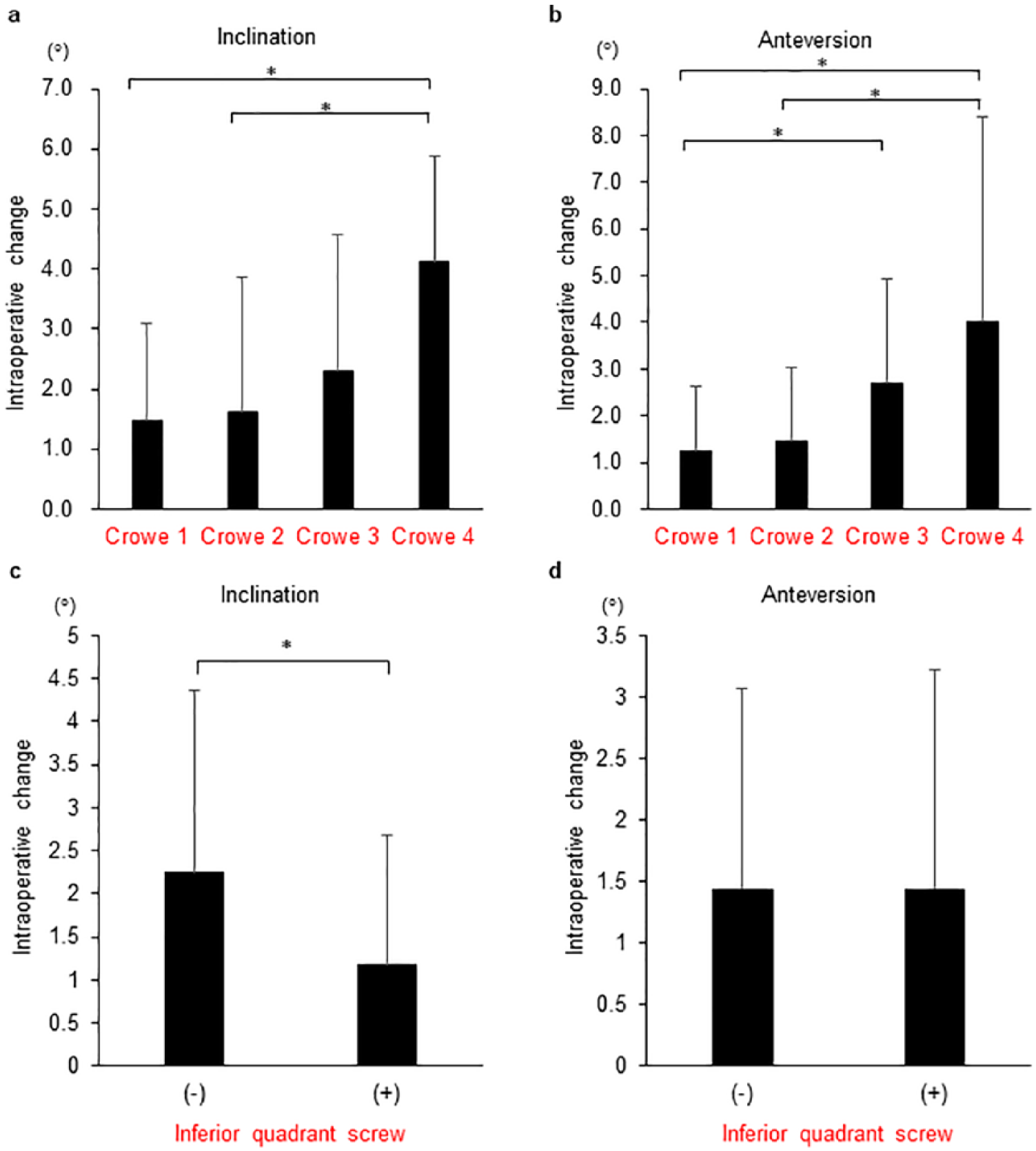
The absolute values of intraoperative cup alignment changes in inclination (a) and (c) and anteversion (b) and (d). The more severe the deformity of the hip joint, the more the cup alignment changes. Inferior quadrant screw fixation minimised the acetabular cup inclination change after additional screw fixation. *indicates p < 0.05. Data are presented as the mean ± standard deviation.
Factors predicting changes in cup alignment
There were no intraoperative changes in cup inclination in 237 hips (no-change group), while there were 19 hips in which a change in intraoperative cup inclination was observed (change group). Regarding intraoperative changes in cup anteversion, there were no changes in 243 hips (no-change group), while 13 hips showed changes in cup anteversion (change group). Univariate analyses of the intraoperative cup alignment changes in inclination showed significant differences in the Crowe classification (p = 0.005), the presence of bone cysts (p = 0.018), and the use of an inferior quadrant screw (p = 0.012) between the no-change and change groups (Table 2). Univariate analyses of the intraoperative cup alignment changes in anteversion showed significant differences in the Crowe classification (p = 0.009) and the use of bone grafting (p = 0.009) between the no-change and change groups (Table 2).
Univariate analyses of intraoperative change in cup inclination and anteversion.
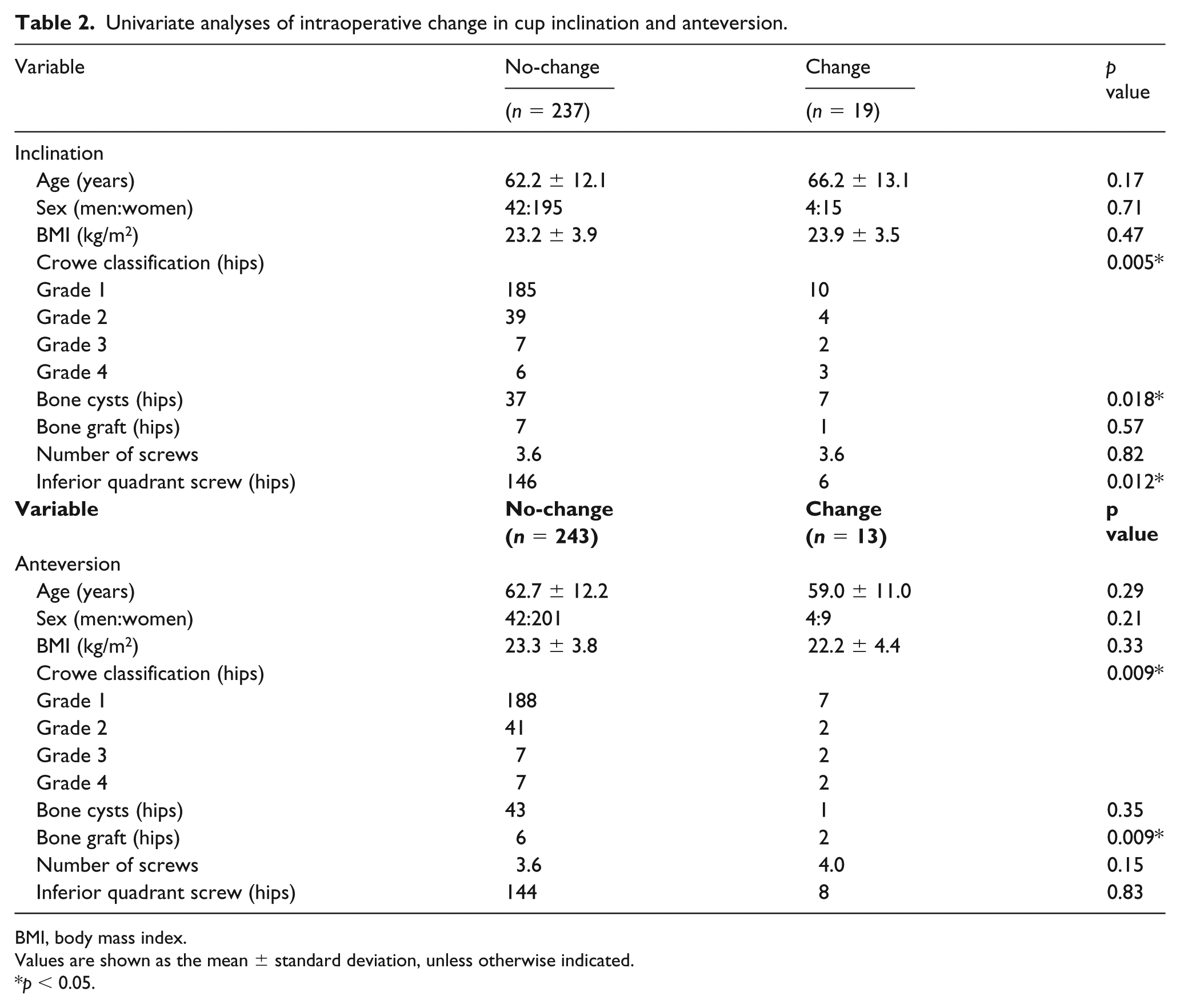
BMI, body mass index.
Values are shown as the mean ± standard deviation, unless otherwise indicated.
p < 0.05.
Multiple logistic regression analyses were performed with the intraoperative cup alignment change in inclination as the response variable and Crowe classification, bone cysts, and inferior quadrant screw fixation as the explanatory variables, along with the intraoperative cup alignment change in anteversion as the response variable and Crowe classification and bone graft as explanatory variables (Table 3). The Crowe classification, the presence of bone cysts, and the use of an inferior quadrant screw were identified as factors related to intraoperative cup alignment changes in inclination (odds ratios, 6.01, 5.94, and 0.03, respectively; p < 0.0001, p = 0.004, and p = 0.0002, respectively), whereas only the Crowe classification was identified as a factor related to intraoperative cup alignment changes in anteversion (odds ratio, 2.08; p = 0.007).
Multiple logistic regression analysis of cup inclination and anteversion.
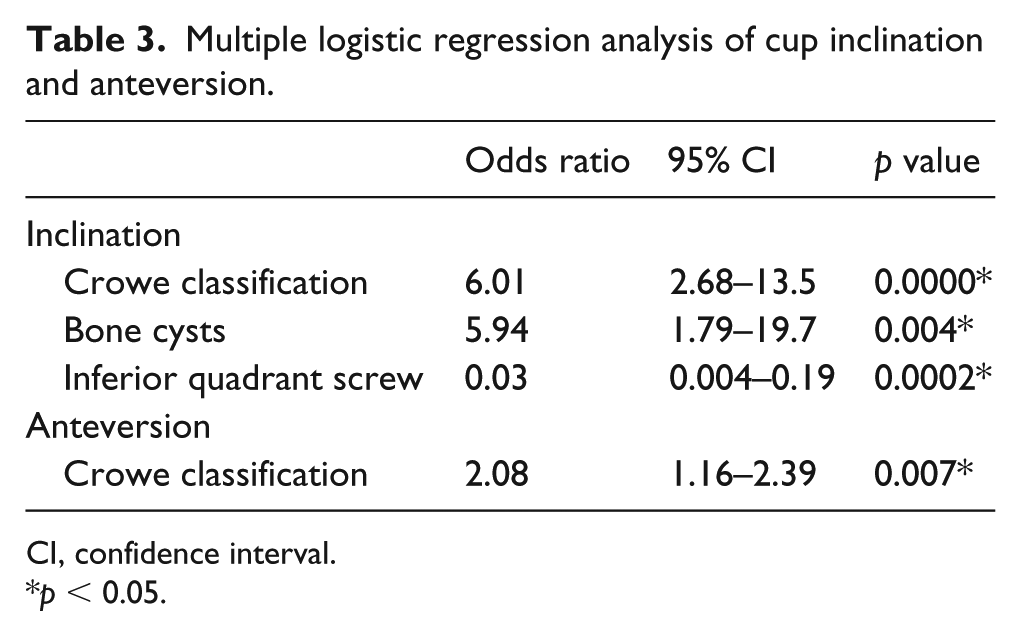
CI, confidence interval.
p < 0.05.
Discussion
In this study, acetabular component alignment changes secondary to screw fixation were studied in patients who underwent an uncemented THA. The mean intraoperative change in the acetabular cup position was 1.6° for inclination and 1.4° for anteversion. In this series, the greatest change in inclination was 10°. Although these results were comparable to those of Fujishiro et al., 7 our results described the degree of cup alignment change for each group of the Crowe classification. The acetabular cup inclination changes were affected by both the preoperative hip deformity and the presence of bone cysts at the load position, and the changes were minimised by the use of an inferior quadrant screw. In contrast, the acetabular cup anteversion changes were affected only by the degree of preoperative hip deformity and were not minimised by inferior quadrant screw use.
Most uncemented acetabular components provide adequate initial fixation in primary THA, although additional screws are sometimes necessary to achieve primary stability of the cup.4–6 Interfacial gaps and relative micromotion between the bone and cup during activities are widely considered to restrict the bony ingrowth process of uncemented acetabular components. 18 Cup press-fit fixation in an uncemented THA depends on sex, acetabular shape, and surgical technique. 5 Acetabula with peripheral defects lose considerable stability, which are determined by the bony anatomy and bone quality of each individual. 19 Screws, whether locked or non-locked, enhance cup fixation by 26%. 3 In a THA with an HA-coated cup, the use of acetabular screws is associated with a lower rate of revision surgery due to aseptic loosening. 16 These experimental results indicate that acetabular screws lead to positive outcomes in primary cup fixation.
The cup was pressed towards the acetabulum with a compression force that induced a lifting displacement on the opposite side with screw fixation. 20 Although Fujishiro et al. 7 reported on the intraoperative changes in cup position, the risk factors for acetabular component alignment changes in THAs have not been fully examined. In this study, we clarified the risk factors of screw fixation for the first time, and hip deformity, based on the Crowe classification, was identified as a factor related to acetabular cup alignment changes in inclination with an odds ratio of 6.01. We conclude that the acetabular cup change in inclination after screw fixation in Crowe grade 1, 2, and 3 patients was affected by the low cup-CE angle. In contrast, the cause of acetabular cup alignment changes in inclination in Crowe grade 4 patients may differ from those of Crowe grade 1–3 patients because the bone quality of the acetabulum was quite different. The acetabula in Crowe grade 1–3 patients showed normal bone quality with subchondral bone sclerosis. Conversely, the bone quality of the original acetabula in Crowe grade 4 patients was quite poor, and this osteoporotic bone quality affected acetabular cup alignment changes in inclination. In general, the stability of the acetabular cup is influenced greatly by the extent and distribution of the host bone around the rim.21,22 A bone-cup contact of more than 8.4° in the cup-CE angle was large enough for press-fit cups to resist superior directed loads. 15 We implanted the cups to allow a cup-CE angle ⩾10°, 15 and we used bulk bone grafts to obtain reliable fixation of the cups in patients with a cup-CE angle < 10°. However, the results of our study, which used an AMS HA cup, indicated that the use of bone grafts had only a small effect in the acetabular cup changes in inclination after screw fixation.
Meneghini et al. 23 reported that an increase in mechanical stability was observed in acetabular components with supplemental screw fixation into the ischium compared to isolated dome fixation in revision THA procedures. In our study, the odds ratio associated with an acetabular cup alignment change was 0.03 when inferior quadrant screw fixation was used; cup alignment changes in inclination were notably reduced, by 97%, with the use of an inferior quadrant screw. However, the acetabular cup alignment changes in anteversion were not reduced by inferior quadrant screw fixation. These differences might be explained as follows. The acetabular cup alignment changes in inclination may be effectively reduced because the directions of the cup inclination change and the inferior quadrant screw location are radially opposed. Conversely, because an inferior quadrant screw is located in the quasi-inferoposterior part of the acetabular cup, anteversion of the acetabular cup may shift in a seesaw-like movement with additional screw fixation. Therefore, surgeons should direct close attention to cup anteversion changes in patients with severe hip dysplasia even if an inferior quadrant screw was used.
This study has some limitations. The formation of gaps in the polar region of the acetabular components is considered a disadvantage of using press-fit fixation with uncemented acetabular components. 24 In this study, the interfacial gap of the press-fit acetabular components was not considered. Second, this study analysed not optimal screw positions and their distribution pattern on cups, but the number of screws. Rigid and safe transacetabular screw fixation in THA is achieved by pursuing deeper bone stock and avoiding injuries to the neurovascular structures, but these efforts can be restricted by the distribution of screws on cups. 25 It is important to analyse changes in acetabular component alignment due to screw fixation, taking into consideration the screw positions. Third, our study was retrospective, and selection bias may have existed because inferior quadrant screw fixation was not conducted in a random manner. Finally, cup position was significantly altered after additional screw fixation, because the effect sizes for the cup alignment change in inclination and anteversion were medium (0.53 and 0.51, respectively). However, the mean absolute values of intraoperative acetabular cup position changes were relatively small (1.6° for inclination and 1.4° for anteversion). We consider that these results were influenced by the inhomogeneous distribution of cases in terms of the severity of hip deformity (Crowe grade 1: 195 hips, grade 2: 43 hips, grade 3: 9 hips, grade 4: 9 hips). If we examined a greater number of patients with more severely deformed hips, cup alignment change might have been considerable. If the initial press-fit fixation of an acetabular cementless component achieves rigid stability in patients with normal bone quality and adequate bone coverage, additional screw fixation is not necessary.1,2,26 We must recognise that cup alignment changes in both inclination and anteversion may present only in patients with osteoarthritis of the hip secondary to DDH or severe osteoporosis.
Acetabular components with various coatings are now available, and we believe that cup alignment changes vary depending on the coating. In this study, only the AMS HA cup was used. AMS HA cups are made of HA-coated titanium arc-sprayed cementless components, and they afford excellent implant fixation for a minimum of 10 years. 14 Further exploration is warranted to determine whether any cup alignment alterations occur with other types of implants, such as those made from 3-dimensional structures or conventional HA-coated implants.
In conclusion, inferior quadrant screw fixation was highly effective for avoiding changes in acetabular cup inclination in patients with severe hip dysplasia. If it is difficult to achieve an adequate press-fit fixation in patients with severe hip dysplasia, additional screws should be carefully inserted following inferior quadrant screw fixation.
Supplemental Material
Supplementary_Table_1 – Supplemental material for Changes in acetabular component alignment due to screw fixation in patients with hip dysplasia
Supplemental material, Supplementary_Table_1 for Changes in acetabular component alignment due to screw fixation in patients with hip dysplasia by Tomonori Tetsunaga, Kazuo Fujiwara, Hirosuke Endo, Tomoko Tetsunaga, Takamasa Miyake, Kazuki Yamada, Tomoaki Sanki and Toshifumi Ozaki in HIP International
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.