
Abstract
Introduction:
Breakage of the femoral stem component of a total hip replacement is now uncommon but continues to be seen with certain stem designs and in certain patient groups. Data previously published on this topic has been limited, either gathered from a single surgeon or centre, or included only a single stem design.
Methods:
We reviewed the data from the Australian Orthopaedic Association National Joint Replacement Registry (AOANJRR), identified and analysed 143 stem breakages over a period of 16 years, covering 44 different stem designs.
Results:
Our data confirms previously published findings that risk factors for stem breakage include patient age at implantation of under 70, male gender, as well as the use of exchangeable necks. We found no association with initial diagnosis, or type of acetabular component implanted. We did however also find, excluding exchangeable neck designs, that after 4.5 years a cemented stem had a significantly higher risk of breakage then a cementless stem.
Discussion:
To our knowledge this is the 1st paper to suggest cemented fixation as a specific risk factor for stem breakage. The analysis of rare complications such as stem breakage is only possible through large data collection systems such as the AOANJRR. Whilst there have been recent advances in materials and manufacturing techniques, we recommend that surgeons are aware of all the specific risks when considering implant choices for individual patients.
Keywords
Introduction
Stem breakage can be defined as a complete fracture of the femoral component of a total hip replacement (THR) either at the neck, trunnion, modular junction or the stem. Breakage of the femoral stem component of a THR is a rare event. Reports of these occurrences are generally confined to isolated case studies or small retrospective reviews. 1 The introduction of stems with fully exchangeable necks however has led to an increased number of reports of femoral component breakage.2–13 Improvements in component designs, newer materials and manufacturing techniques have likely led to a reduction in femoral stem component breakage. Overall, revision for femoral stem breakage occurs far less frequently compared to the common revision diagnoses of loosening, dislocation and infection. 13
Non-modular cemented or cementless stem breakages at the level of the stem have been traditionally attributed to cantilever bending and fatigue failure due to reduced proximal implant support.14–16 In cementless implants, this has been shown to be more common in extensively coated distally well-fixed small diameter stems.17,18 Non-union of an extended trochanteric osteotomy and a heavy patient have also been shown to be risk factors for stem breakage. 19 Most of the reported stem fractures in cemented stems have occurred at the stem body and were likely to be due to proximal cement overloading and loosening, creating a cantilever bending force on the stem.1,20,21 More rarely, stems can break at the level of the neck possibly thought to be due to notching, increased body mass index (BMI) or increased femoral head size or horizontal offset.22,23 Whilst the exact aetiology for stem breakage is not well delineated the general risk factors are thought to include male gender, high BMI, small implanted stem size, proximal femoral bone defect, and reduced calcar support. 24
National joint registries have the advantage of large datasets and have the ability to report and analyse rare events such as stem breakage. A recent systematic review of the literature assessed 23 case reports and small clinical series to conclude that national joint registries are better placed to allow a more general evaluation of this rare complication. 25 Of course, there are inevitable limitations of such registry studies which will be discussed in this paper. However, the aim of this study was to review the rate of revision for femoral stem breakage following primary THR using data from the Australian Orthopaedic Association National Joint Replacement Registry (AOANJRR) and analyse the retrieved data to identify associated risk factors.
Methods
Data was obtained from the AOANJRR regarding primary THR’s that had been revised for ‘femoral stem breakage’. The study excluded femoral stem breakages in revision THRs as the differences between the primary and revision THR groups were considered too distinct to allow conclusions to be drawn from the combined data. Out of all primary THRs performed for any diagnoses between 1 September 1999 and 31 December 2015 the study group included all patients who underwent revision where ‘femoral stem breakage’ was listed as a reason for revision. We performed further analyses on both patient and prosthesis characteristics. Due to a previously identified higher rate of revision for breakage of femoral stems with fully exchangeable necks and modular stem components, a separate analysis was undertaken with these devices excluded.
The Registry uses Kaplan-Meier estimates of survivorship to describe the time to 1st revision of an arthroplasty with censoring at the time of death or closure of the database at the time of analysis. The unadjusted cumulative percent revision with an accompanying 95% confidence interval (CI) was calculated with use of unadjusted pointwise Greenwood estimates. Hazard ratios were calculated using Cox proportional hazards models adjusting for age and gender and were used to compare the rate of revision between groups. The assumption of proportional hazards was checked analytically for each model; if the interaction between the predictor and the log of the postoperative time was significant in the standard Cox model, then a time varying model was used. All tests were 2-tailed set at the 5% of level of significance. All statistical analysis was performed using SAS software version 9.4 (SAS Institute Inc, Cary, NC, USA).
Results
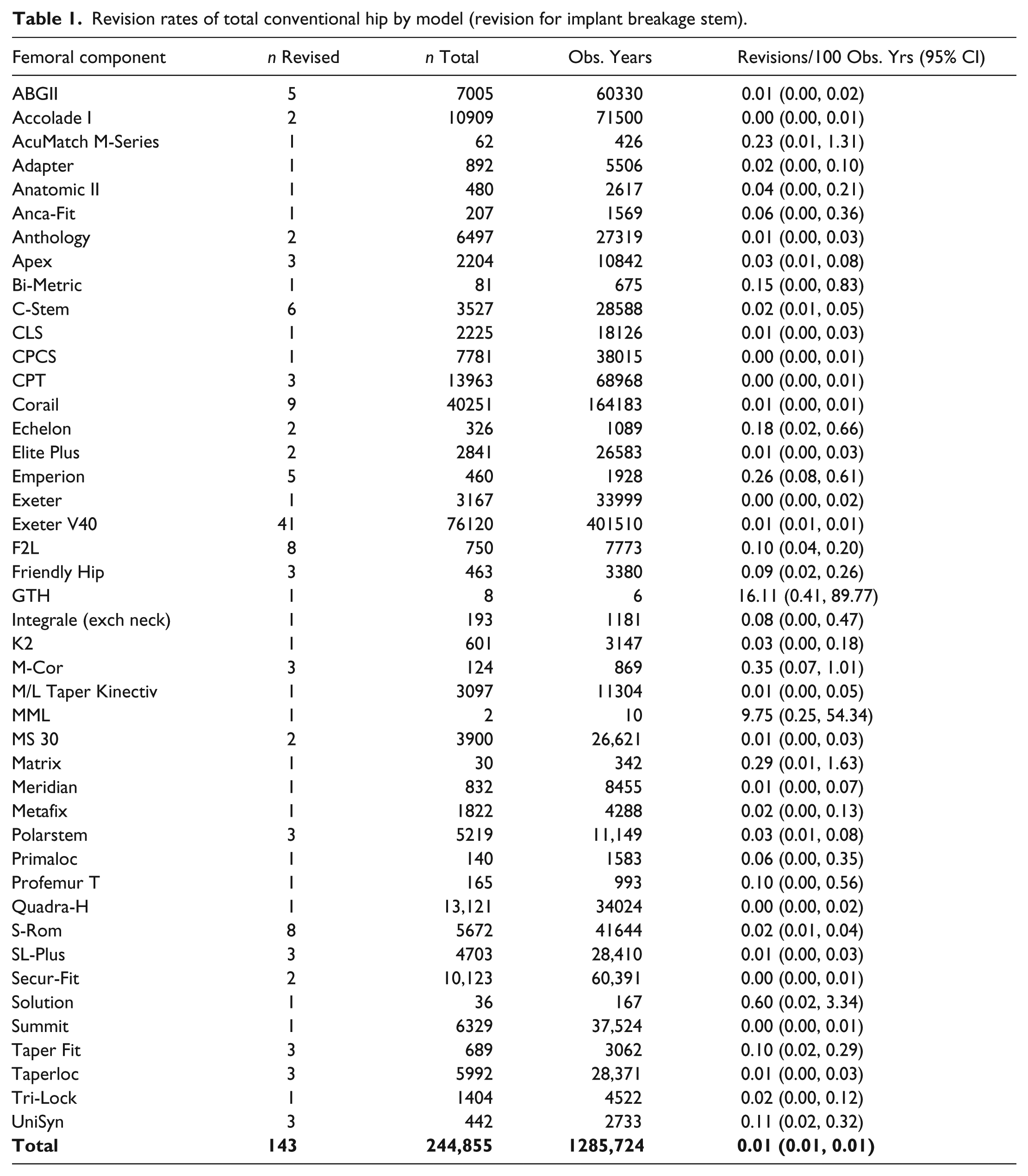
The analysis searched 346,782 primary THRs, from which 143 revisions for femoral stem breakages were recorded. Stem breakage was recorded for 44 of the 236 different femoral stem types recorded by the Registry. The revision rates by stem design per 100 observed years are shown in Table 1. The 10-year cumulative percent revision (CPR) for all femoral stem breakages recorded in the AOANJRR was 0.1%.
Revision rates of total conventional hip by model (revision for implant breakage stem).
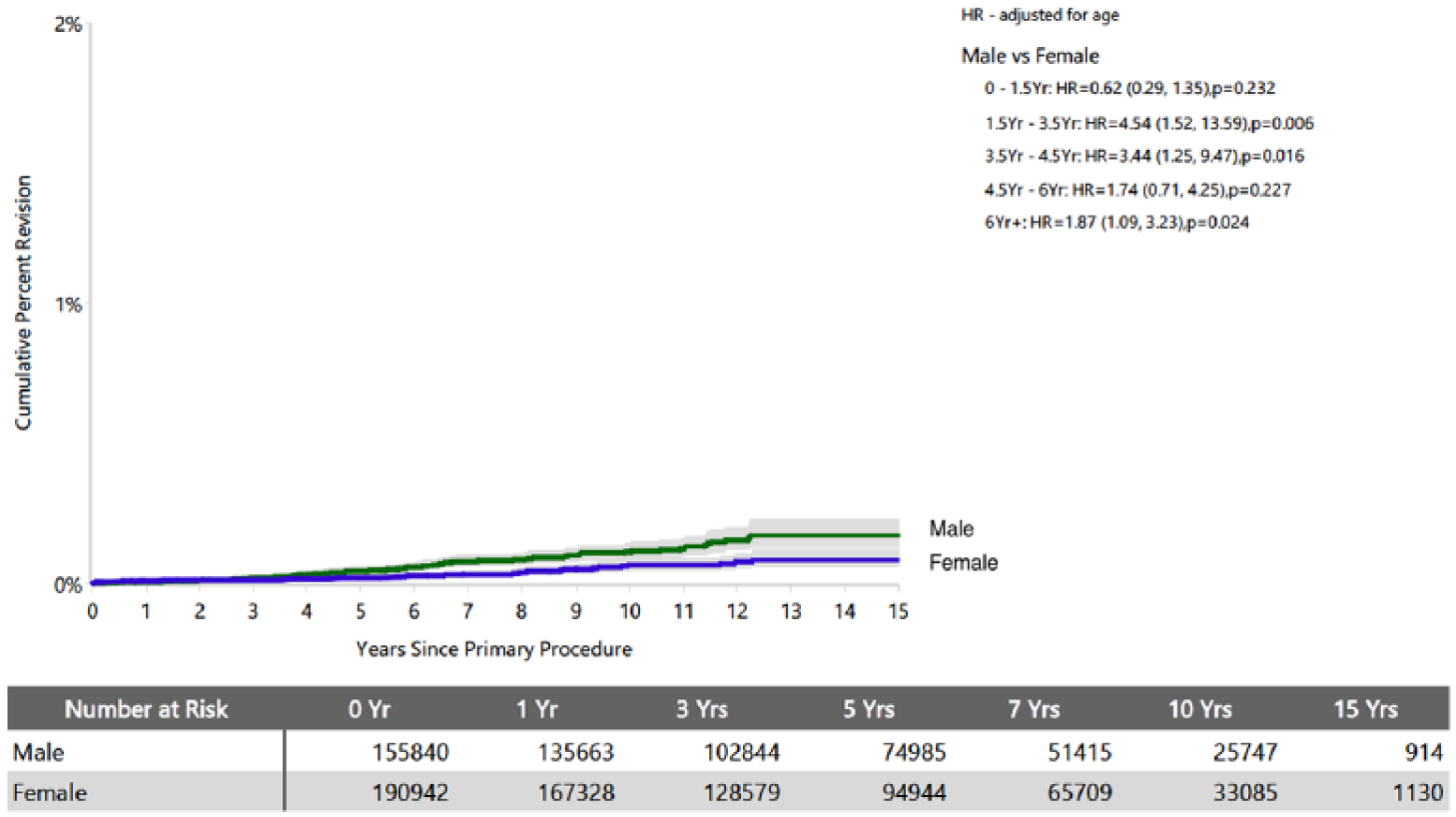
Whilst osteoarthritis was the commonest primary diagnosis associated with femoral stem breakage there were a variety of other primary diagnoses. There were more revisions for femoral stem breakages in males (61% versus 39%), and a significantly increased risk of revision for femoral stem breakage in males after 6 years following implantation (Table 2) (Figure 1).
Cumulative percent revision of total conventional hip by gender (revision for implant breakage stem).

Cumulative percent revision of total conventional hip by gender (revision for implant breakage stem).
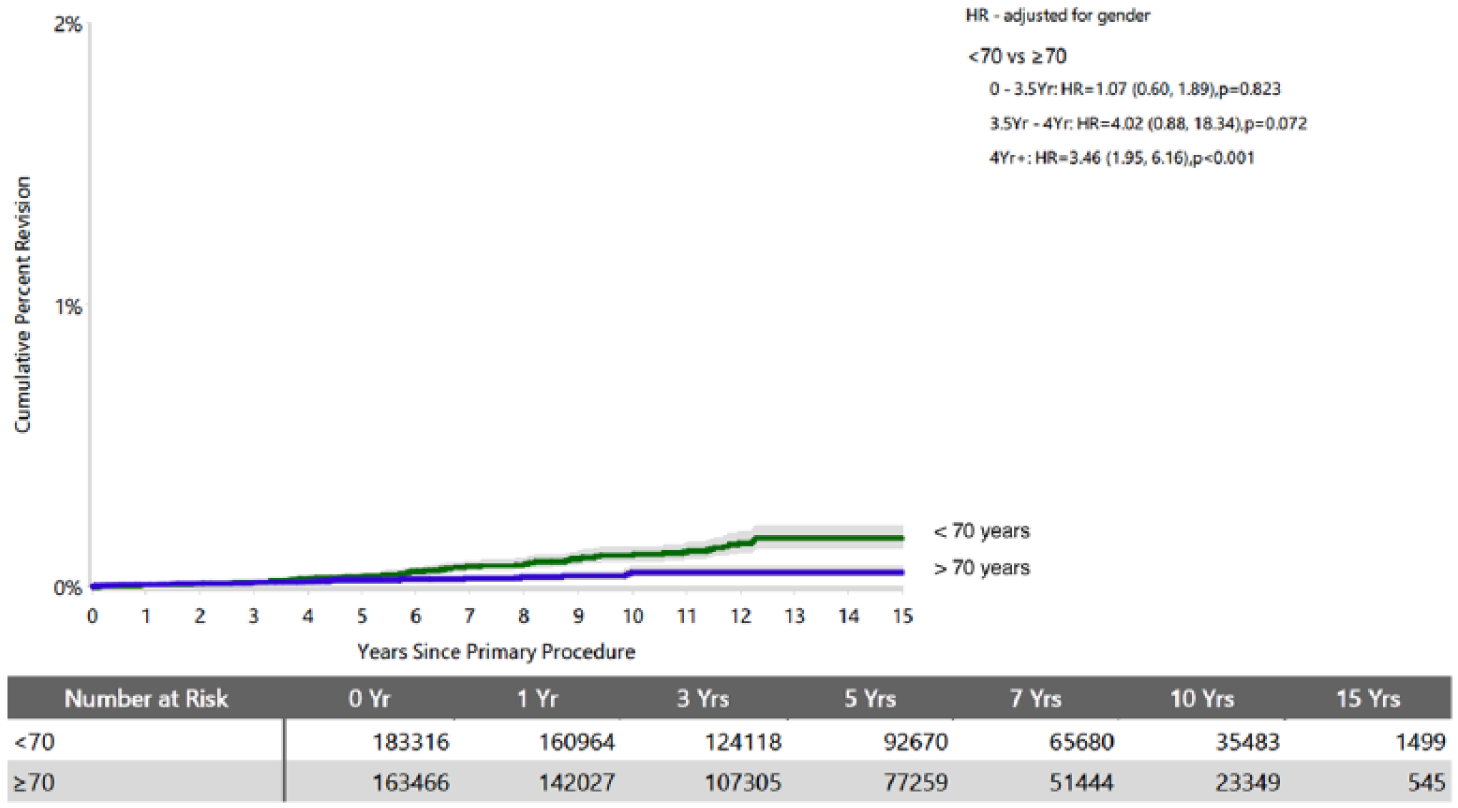
There were more revisions for femoral stem breakages in those aged less than 70 years at implantation compared to those ⩾ 70 years (74.1% versus 25.9%), along with a significantly increased risk of revision for femoral stem breakage in those less than 70 years after 4 years following implantation (Table 3) (Figure 2).
Cumulative percent revision of total conventional hip by age (revision for implant breakage stem).

Cumulative percent revision of total conventional hip by age (revision for implant breakage stem).
Overall, femoral stem breakages occurred in 78 cementless and 65 cemented stems (Table 4). Exchangeable neck and modular femoral stems are used almost exclusively with cementless fixation and this group in our Registry study have a 7-fold increased risk compared to fixed neck cementless stems. With these excluded, cemented femoral stems had a higher rate of revision for breakage compared to fixed neck cementless stems (Figure 3). This trend was most significant at the 4.5 years following implantation stage (p-value 0.001).
Cumulative percent revision of total conventional hip by fixation (revision for implant breakage stem).

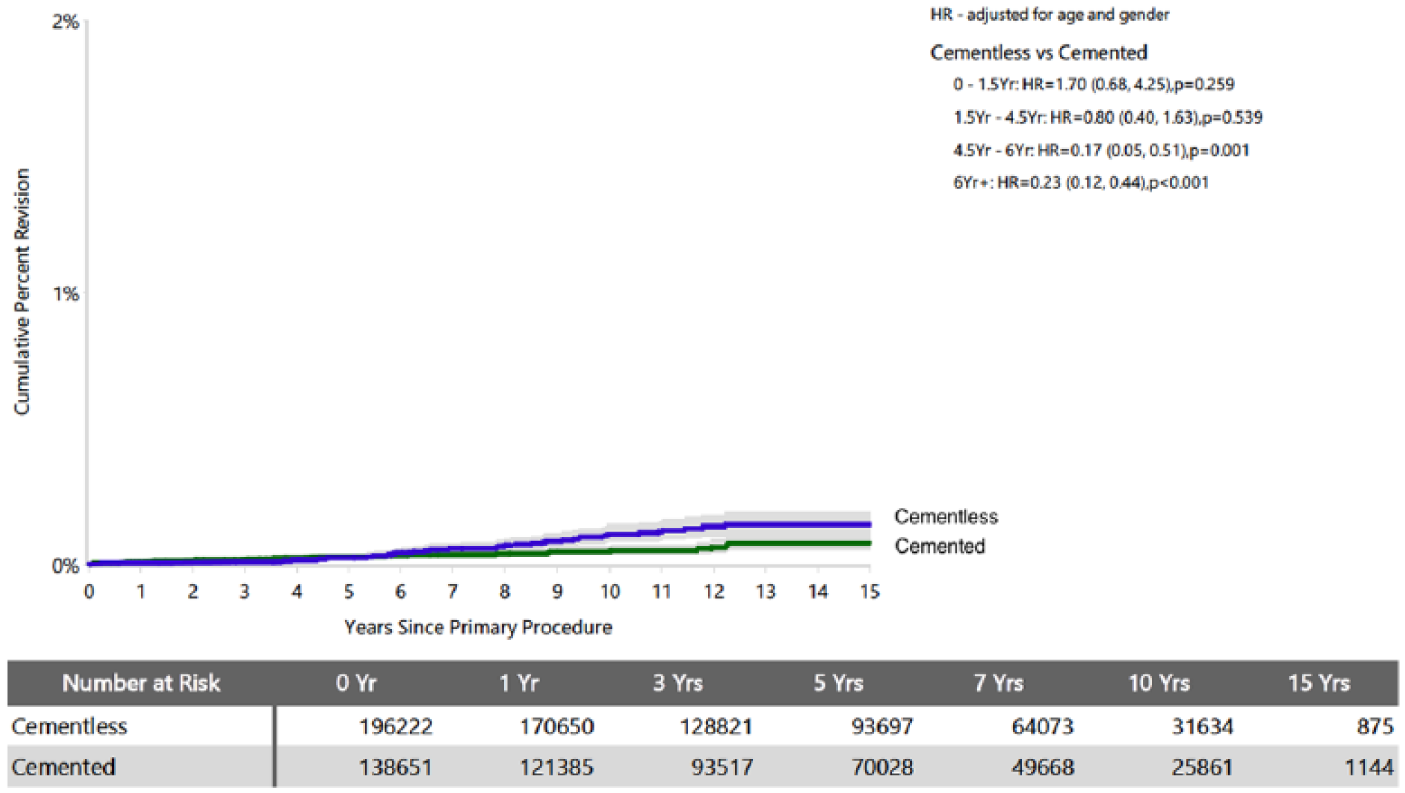
Cumulative percent revision of total conventional hip by fixation (revision for implant breakage stem, excluding exchangeable necks).
Revision for stem breakage undertaken in the first 3 years accounted for a greater proportion of all revisions for stem breakage for cementless stems (50.9% compared to 12.3% of cemented stem revisions), with the reverse being true beyond 3 years (Table 5).
Timing of revision for implant breakage stem.

Due to the absolute numbers implanted, the Exeter stem experienced the highest number of revisions for stem breakage. There are 45 different Exeter V40 stem types, each with a unique catalogue/reference number. Stem breakage of the Exeter V40 stem occurred in 12 of the 45 different stems (40 revision procedures) from a total of 63,028 primary THR using 1 of those 12 stems. 1 revision occurred in a stem with a 30-mm offset and 1 revision in a stem with a 50-mm offset (Size 5 stem).
Discussion
This study has demonstrated that femoral stem breakage is uncommon with modern femoral stem designs. This differs from earlier studies of femoral stem breakage, which report an incidence ranging from 0.23% to 11%. The incidence of breakage in these studies varied depending on stem material and design as well as patient characteristics.12,13,25 The original series of Exeter stems, implanted between 1970 and 1975, had a breakage rate of 3%. 26 These original Exeter stems were made form EN58J stainless steel, this was followed by the matt finish 316L stainless steel stem. In 1986 this was changed to the Orthinox polished stainless-steel stem with a non-V40 spigot. The current V40 Orthinox highly polished stem was introduced in 2002. For the entire period of data capture for our study the Exeter stems have been made from Orthinox stainless steel. Breakage of the Precoat stem (Zimmer, Warsaw, Indiana, US) was also attributed to the stem design. 14
With the introduction of modular stems, stem breakages have been reported at the various taper junctions.27,28 Similarly, with the introduction of exchangeable neck prostheses, there have been reports of neck breakages.2–6,29 Like a number of previous reports, this study has shown a significant increased risk of stem breakage when exchangeable neck prostheses are used. The mechanisms for this are now widely accepted and include micro-motion/fretting and corrosion-assisted fatigue. This mode of failure has also recently been shown to be more likely in male patients, overweight patients, and with the use of a longer neck component. 4 Stem breakage has also been reported with the use of large head metal-on-metal bearings.30,31
Excluding exchangeable neck designs, our study showed that after 4.5 years a cemented stem had a significantly higher risk of breakage then a cementless stem. In a series of 4 fractured cemented Exeter stems the failures all occurred at between 2 and 10 years, and were thought to be multifactorial. 32 The biomechanical mechanism of failure is thought to be as a result of cantilever loading, typically when the distal part is well-fixed and the proximal part less so. This may occur in the early postoperative period due to poor primary fixation due to poor cementation technique, or poor initial ingrowth/ongrowth of a cementless stem. Alternatively, it can be due to progressive proximal bone loss over time due to osteolysis or stress-shielding. Stress-shielding is traditionally attributed to cementless stems with well-fixed stiff stems while osteolysis is traditionally attributed to cemented stems exposed to high polyethylene wear.33,34 How the above factors contribute to the difference in stem breakage between cemented and cementless stems at 4.5 years is not clear.
Cemented stems necessitate a smaller stem diameter then cementless stems. It is understood that stem diameter influences the section modulus, and ultimately the fracture toughness, to the 3rd power. Therefore from the biomechanical perspective, undersizing refers to the relation of the stem diameter to the patient’s body weight. 18
In an environment conducive to cantilever bending a stem with a smaller diameter is more likely to succumb to fatigue failure over time due to repetitive bending forces then a thicker stem. In a biomechanical study, undersized cemented stems showed large and increasing micromotions, and failed after few loading cycles, because of macroscopic cracks in the proximal part of the cement mantle. 35 Harrington et al. 36 investigated the effects of multiple factors in loosening of cemented femoral stems. They found that body weight had the largest effect on the peak strain of the proximal cement mantle and suggested that cemented femoral stems should not be used in heavy patients with small medullary canals as this leads to high cement stresses. 36
This study demonstrated that those patients aged < 70 years appeared to be at a higher risk of stem breakage. In general, increasing age at surgery often correlates with decreased overall activity. 37 This may in turn produce lower polyethylene wear, less osteolysis and therefore may be the reason why there is a lower rate of stem breakage in older patients. The increased risk of stem breakage in male patients is likely to be multifactorial. Male patients tend to be heavier, and also taller, placing greater load on their implants. In general, male patients will receive implants which are larger in size, and so these loads should be within implant tolerance. However, young male patients who tend to have good bone stock are more likely to have Dorr type A proximal femurs which may limit the size of the implanted stem. 38 Whether male patients after THR are more active than female patients is uncertain.
Increased patient weight or BMI has been postulated as a risk factor for stem breakage.1,15,27,29,32 In 1975, Charnley reported an incidence of 6% for overweight male patients. 15 Collis reported a 33% incidence of femoral stem breakage in patients who were overweight and over 1.8 metres tall. 39 An analysis of 120 Charnley femoral stem breakages found an association with both patient weight and surgical technique. 40 Whilst this seems logical, breakages still occur in smaller patients and so this cannot be the only factor. Craik et al. 41 pointed out the flaws inherent in using BMI from an engineering point of view when interpreting explanations for material failure: they felt patient weight was more appropriate. Several other risk factors for stem breakage have previously been identified including laser etching of the stem and other potential mechanical stress risers.14,42–45 A further commonly cited risk factor is component varus positioning.15,39,46 While the majority of cemented stem breakages reported in the literature are in the mid-third region, there are some reports of cemented stems breaking through the neck.22,23 Registry data does not provide this level of detail to allow this study to comment on the exact location of stem breakage nor the other risk factors. This study has a number of limitations. Large datasets are important to identify patterns and provide information about rare complications which may be too infrequent to be identified in smaller datasets. However, such registry studies are prone to systemic bias which is most sensitive when the field entry incidence is very low - such as stem breakage. There may be a considerable under-reporting of this failure mechanism due to ignorance of the field’s presence, compounded by the habitual nature of completing forms. Registry data is dependent on the quality of the original information entered on the form. A clear and universally consistent definition of stem breakage is assumed and the choice of failure attribution when > 1 cause of failure is considered is not well represented in registry studies. Also, registry data has no information about the exact site of breakage, or technical difficulties in the operative procedure (i.e. stem positioning, adequacy of fixation, stem under-sizing). Familiarity with cemented and cementless implants can vary between surgeons and therefore may affect surgical technique. Patient weight and height was not reported to the Registry during this study period and nor was there any indication of patient activity levels pre- and post-surgery. Registry studies are therefore unable to provide accurate information about causality. Furthermore, registry studies are prone to surgical selection bias. It is likely that surgeons made a conscious decision to implant a cemented or cementless stem based on the morphology of the proximal femoral bone and the patients’ weight and activity profile. These selections should be taken into consideration when interpreting the findings presented in this study. This study based on registry data is unable to provide information about the reason for the higher risk of cemented stem breakage demonstrated at 4.5 years. Further studies particularly clinical and biomechnical studies may be able to shed light on our findings
Conclusion
This is a unique study reporting incidence and risk factors of femoral stem breakage from a large national registry over 16 years. The overall incidence of femoral stem breakage is very low and a number of risk factors have been identified. Patients aged < 70 years and males have an increased risk of stem breakage. Cemented stems and cementless stems with exchangeable necks have a higher rate of breakage. Whilst some of the stems analysed in this registry database have been superseded by newer stems with improved materials and manufacturing processes, it remains a useful analysis to allow surgeons to make informed choices about stem selection for certain groups of patients.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.