
Abstract
Background:
Vitamin E highly cross-linked polyethylene (HXLPE) was developed to reduce wear in total hip replacement (THR). This formal systematic review and meta-analysis aimed to provide independent synthesis of wear characteristics of Vitamin E treated HXLPE compared to HXPLE/UHMWPE. Secondary outcome measures were differences in revision rates and functional scores.
Methods:
We performed a formal systematic review as per PRISMA guidelines; literature searches were conducted on 14 November 2017 (MEDLINE, Embase on Ovid, and the Cochrane Library). We included randomised controlled trials, analyses of joint registries, and case-controlled studies of primary THR comparing cups with a vitamin E HXLPE bearing with bearing surfaces made from other types of polyethylene. Initial screening was performed by 2 independent assessors; disagreement resolved in discussion with a third reviewer. Studies were evaluated using the Cochrane risk of bias tool. Data extraction permitted meta-analysis.
Results:
372 studies were identified on initial screening, 5 studies met the eligibility criteria. There was no significant heterogeneity between studies. There was variable risk of bias. At a mean of 35 (range 20–60) months, Vitamin E HXLPE had significant advantages over highly cross-linked polyethylene with regards total femoral head penetration (p = 0.004). Given the RSA measurement errors this may not be clinically significant.
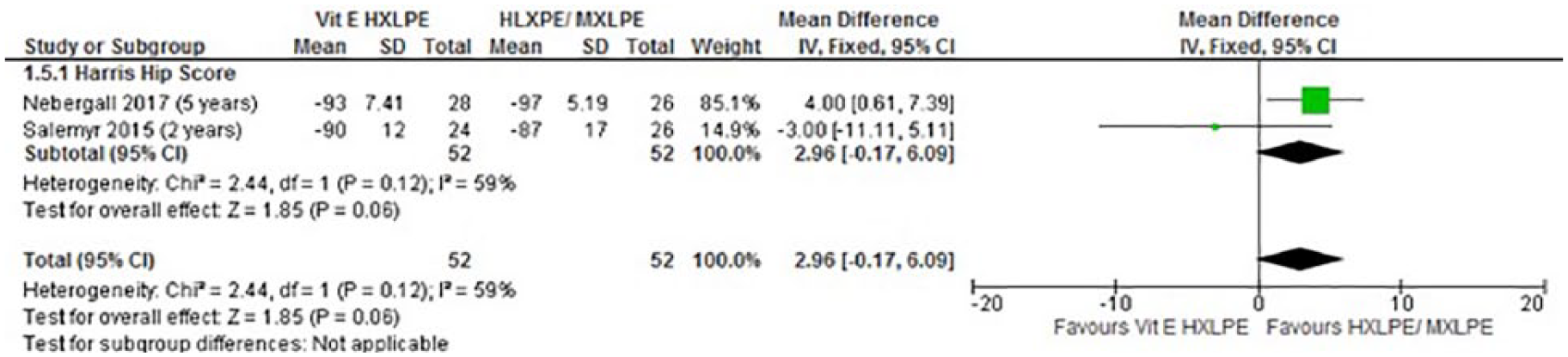
There were neither significant differences in revision rates nor Harris Hip Scores (p = 0.06).
Conclusion:
At a minimum of 3 years follow-up there was reduced total femoral head penetration for vitamin E HXLPE over HXLPE. This bearing surface does not, as yet, have clinically significant advantages in terms of revision rates or patient function over HXLPE.
Introduction
Ultra-high molecular weight polyethylene (UHMWPE) has been in used for nearly 60 years yet historically many other bearing materials have been tried.1,2 According to National Joint Registry of England and Wales (NJR) UHMWPE is used in 88% of total hip replacements (THRs). 3 Wear mediated aseptic loosening is a common cause of revision in THR. 3 UHMWPE wear by oxidative degradation decreases wear resistance and leads to increased osteolysis; a major cause of implant failure.1,3–6
The sterilisation process is a major contributor to UHMWPE degradation.7,8 High-energy radiation, used in sterilisation processes, induces oxidation. Bond scission occurs with the formation of free radicals. 2 This reduces molecular mass and alters the mechanical properties of the UHMWPE. The oxidation continues during storage and in vivo once implanted. 9 In 1998, highly cross-linked and thermally treated polyethylenes (HXLPEs) were introduced to improve wear resistance. It was theorised they would reduce the incidence of revision. Crosslinking results in an increased molecular mass; improving wear resistance and mechanical properties compared to UHMWPE.10,11 Following irradiation, the HXLPEs are thermally treated to remove residual free radicals. Two different processes, remelting and annealing, are used. Only remelting treatment effectively removes residual free radicals.12,13 Other processing methods have been considered but have not been able to eradicate free radicals meaning oxidative degradation can occur. 14
Vitamin E (VE) is an antioxidant that can be added to the HXLPEs to combat oxidative degradation and improve fatigue properties by avoiding post-irradiation melting. 15
In vitro studies have demonstrated a protective effect of VE on oxidative degradation, with improved mechanical and wear properties.16–18 Additionally, in vitro and animal studies have not demonstrated adverse reactions. 19 Despite this, there is currently limited clinical evidence to support the use of vitamin E HXLPE.
There are 2 methods of adding vitamin E: the first is by blending UHMWPE powder with vitamin E prior to consolidation and cross-linking (blended vitamin E HXLPE); the second is by doping the consolidated and cross-linked material in a hot vitamin E solution, allowing vitamin E to diffuse into the material (diffused vitamin E HXLPE). 20 The purpose of this study is to provide an independent synthesis of the wear characteristics of vitamin E treated HXLPE compared to HXPLE or UHMWPE. Secondary outcome measures were differences in revision rates and functional scores.
Materials and methods
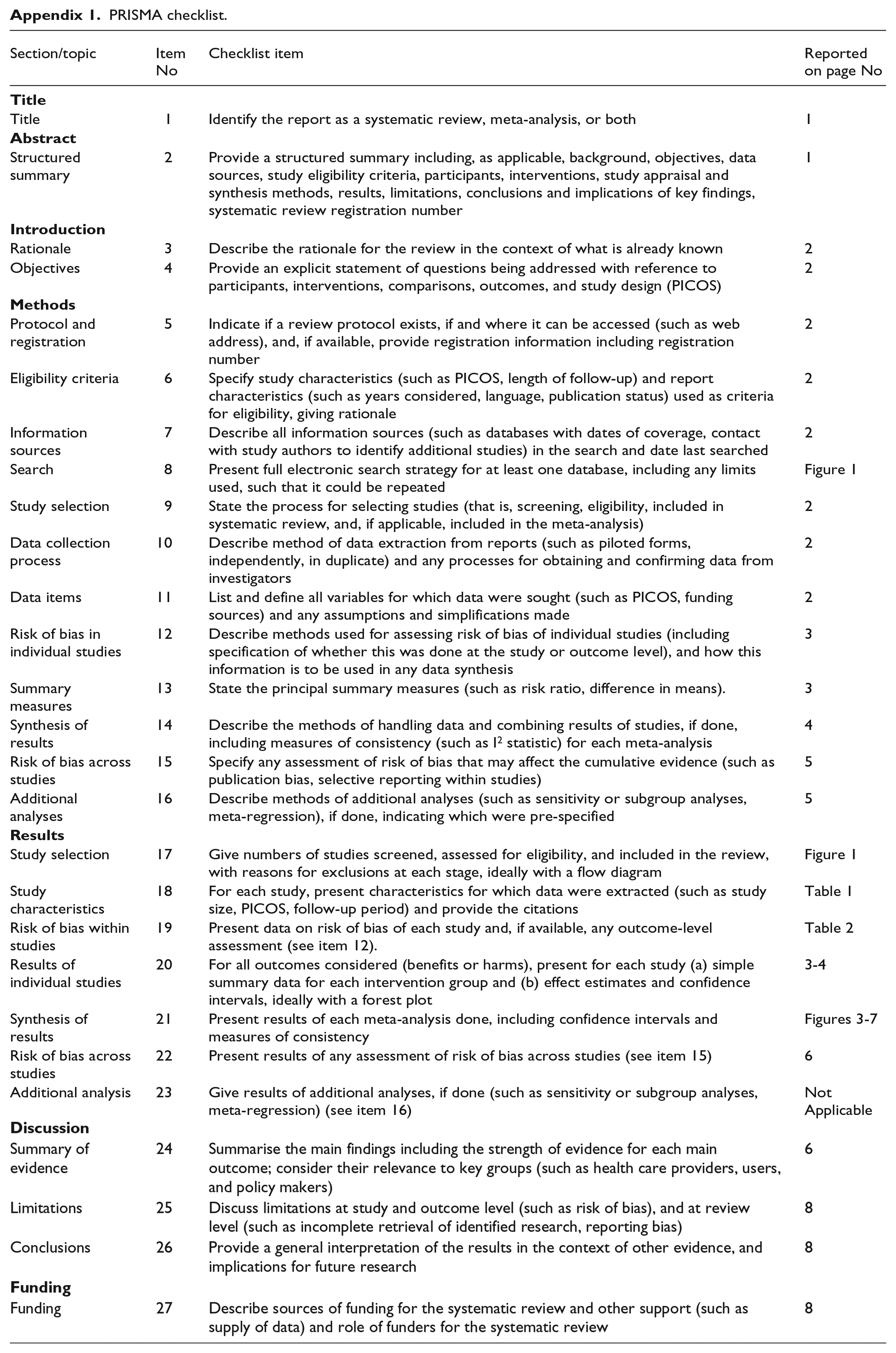
Before commencing the review, the study protocol was registered with PROSPERO (CRD42017074141) as recommended by the Quality of Reporting of Meta-analyses (QUOROM) statement. 21 We used a rigorous and systematic approach conforming to the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) and a PRISMA checklist is included in Appendix 1.
Search strategy
We searched the electronic databases MEDLINE and Embase on the OVID platform, and The Cochrane Library using the search strategy shown in Figure 1. Searches were conducted from database inception to 15 November 2017. We did not limit the search to English language publications. We also evaluated the grey literature with hand searches of conference abstracts published in 6 major orthopaedic journals in the 5 years before the search date. Bibliographies of relevant articles were checked and key citations tracked in Web of Science.
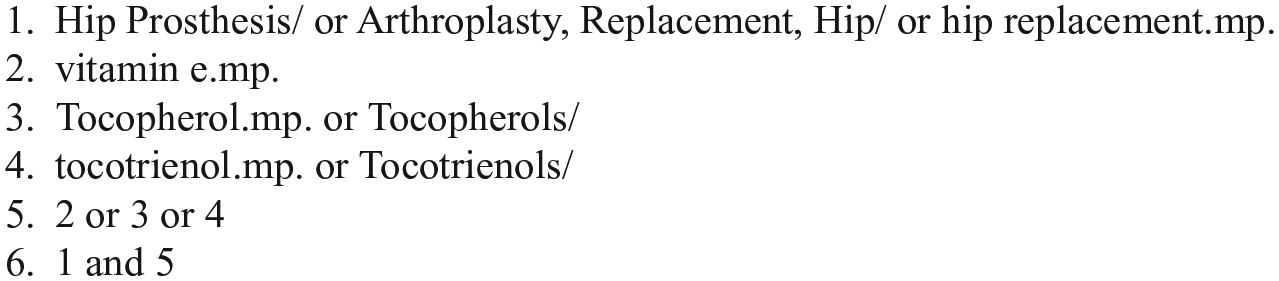
Search strategy.
Eligibility criteria
We included all randomised controlled trials (RCTs), analyses of joint registries and case-controlled studies including patients of all age groups receiving primary total hip replacement using vitamin E HXLPE compared to any other type of polyethylene.
Screening
Title and abstracts were screened by 2 independent assessors with any disagreements resolved in discussion with a third reviewer. If any uncertainties relating to inclusion occurred, we planned to contact authors for clarification.
Data extraction
2 of the authors worked independently to extract the data using standardised forms. We extracted data on: study country; recruitment dates; setting; participant characteristics; duration of follow-up; acetabular and femoral head bearing material an size; outcomes relating to primarily the degree and measurement of femoral head penetration; secondarily the revision rates, Harris Hip Score (HHS, patient-reported outcome measures; and risk of bias). An electronic spreadsheet was constructed to summarise the findings of relevant studies.
Study quality
Potential sources of bias in RCTs were assessed using the Cochrane risk of bias tool. 22 This method assesses selection, performance, detection, attrition, and reporting biases. Summary assessments of risk-of-bias (high, low or unclear) for each outcome in each trial are reported. We planned to use alternative risk of bias assessment methods for assessment of non-randomised studies.
Statistical analysis
Data was combined in meta-analysis using Review Manager software (Review Manager (RevMan) 5.3. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration; 2014). Heterogeneity was assessed using the I2 statistic representing the proportion of variability across studies not due to chance or random error. Pre-specified subgroup analysis was performed relating to different polyethylene comparators and femoral head materials.
Results
A total of 372 records were identified by literature searches. The titles and abstracts were screened to identify potentially useful articles for inclusion. After screening, 16 articles were assessed for eligibility. A flow diagram of the progression of studies through the systematic review is provided in Figure 2.
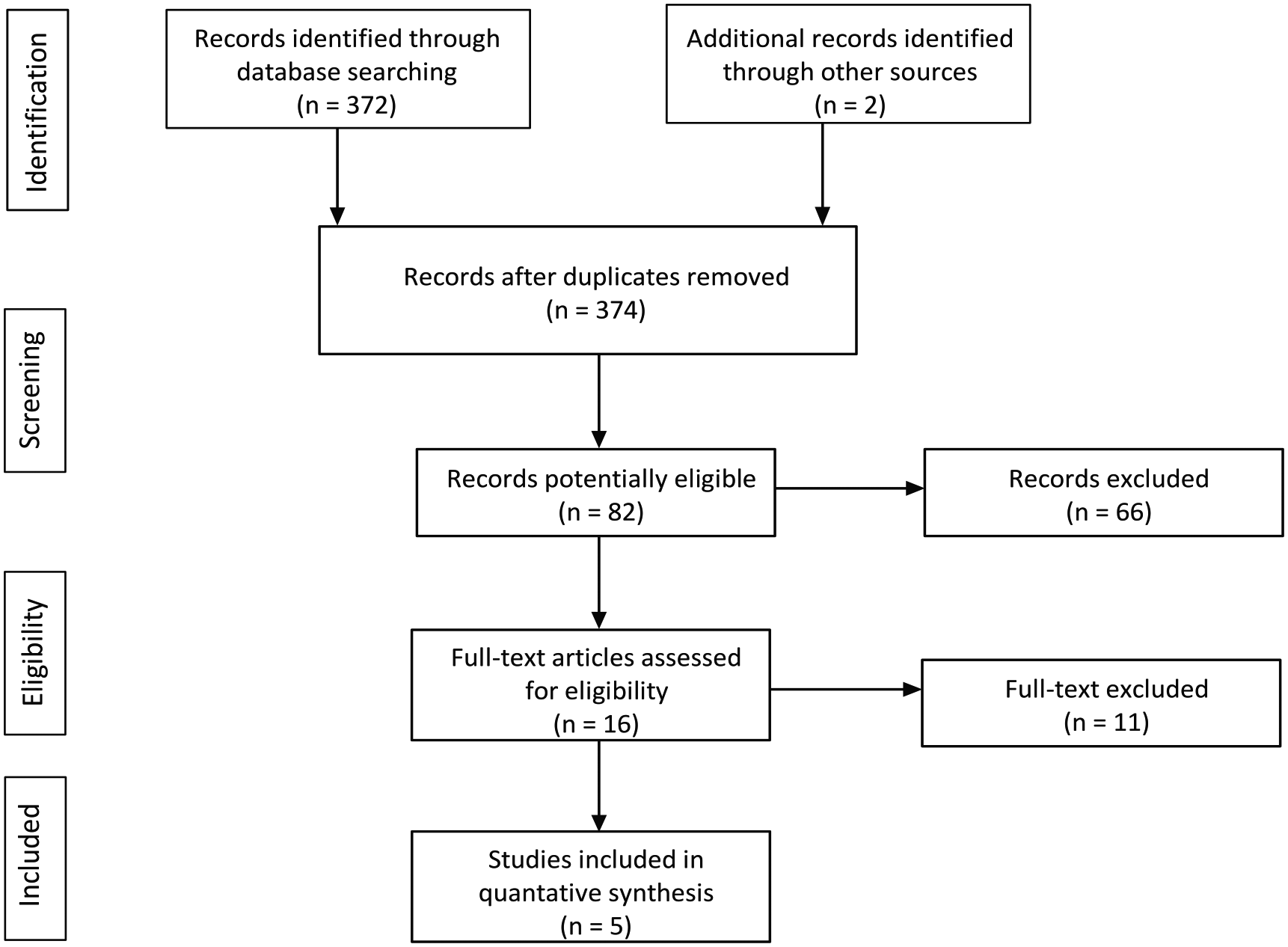
PRISMA flow diagram.
There were 5 articles that contributed to our estimates of femoral head penetration, revision and functional outcome. There were 4 prospective randomised controlled trials (RCTs), all from Europe with recruitment from 2008, of which 3 examined diffused vitamin E HXLPE compared to HXLPE.23–25 The remaining RCT compared
Vitamin E blended HXLPE to conventional UHMWPE. 26 Study characteristics are summarised in Table 1. There was a low risk of bias amongst RCTs when we examined sequence generation, allocation/concealment, blinding, completeness of data and reporting (Table 2). 1 other study from Japan had a case-control design and compared blended Vitamin E HXLPE and HXLPE. Although the authors reported propensity matching, we considered the study to be at high risk of bias because under a quarter of the 348 patients recruited were followed up. 20
Study characteristics: RCT)s.
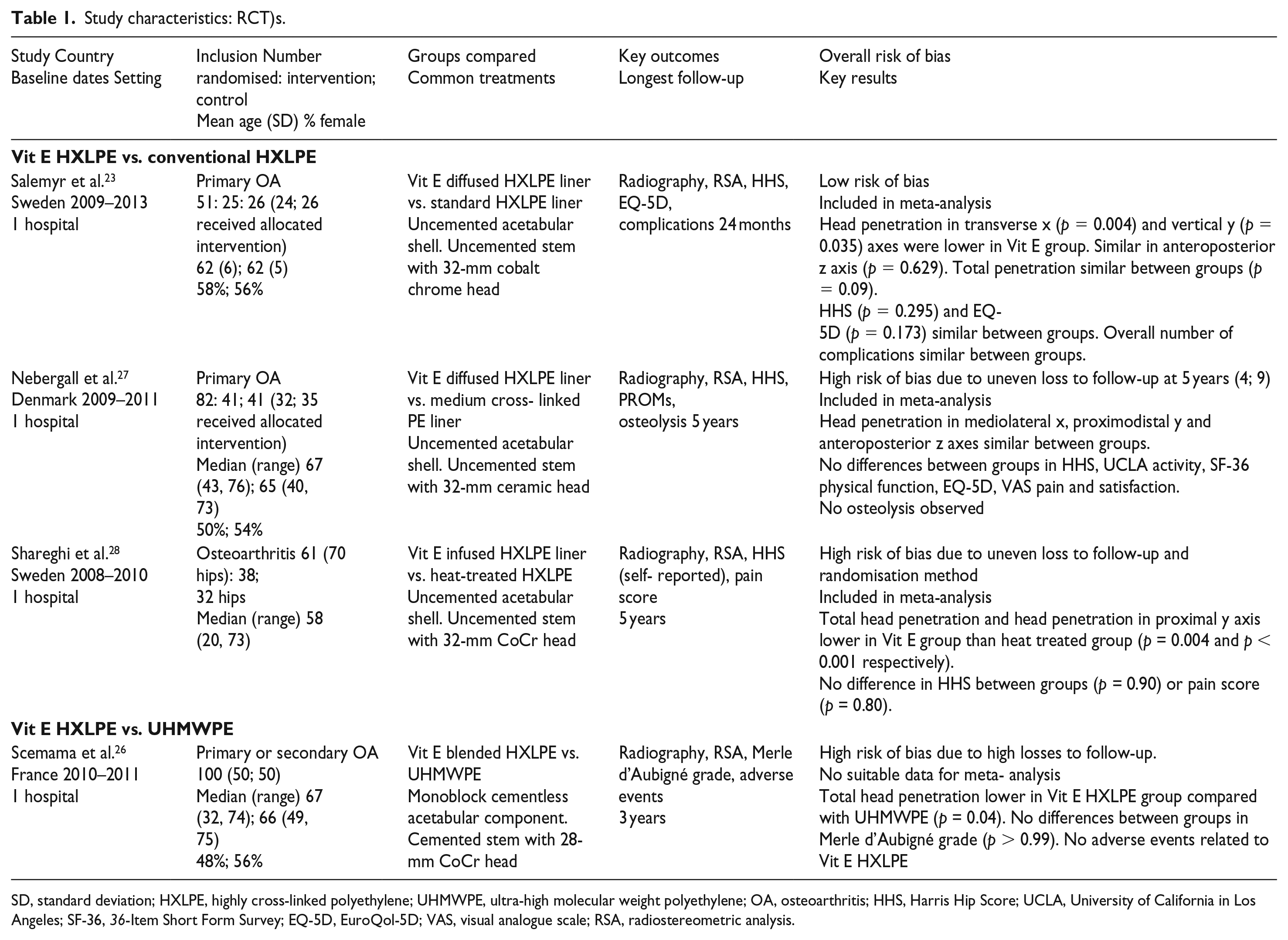
SD, standard deviation; HXLPE, highly cross-linked polyethylene; UHMWPE, ultra-high molecular weight polyethylene; OA, osteoarthritis; HHS, Harris Hip Score; UCLA, University of California in Los Angeles; SF-36, 36-Item Short Form Survey; EQ-5D, EuroQol-5D; VAS, visual analogue scale; RSA, radiostereometric analysis.
RCT risk of bias assessment.
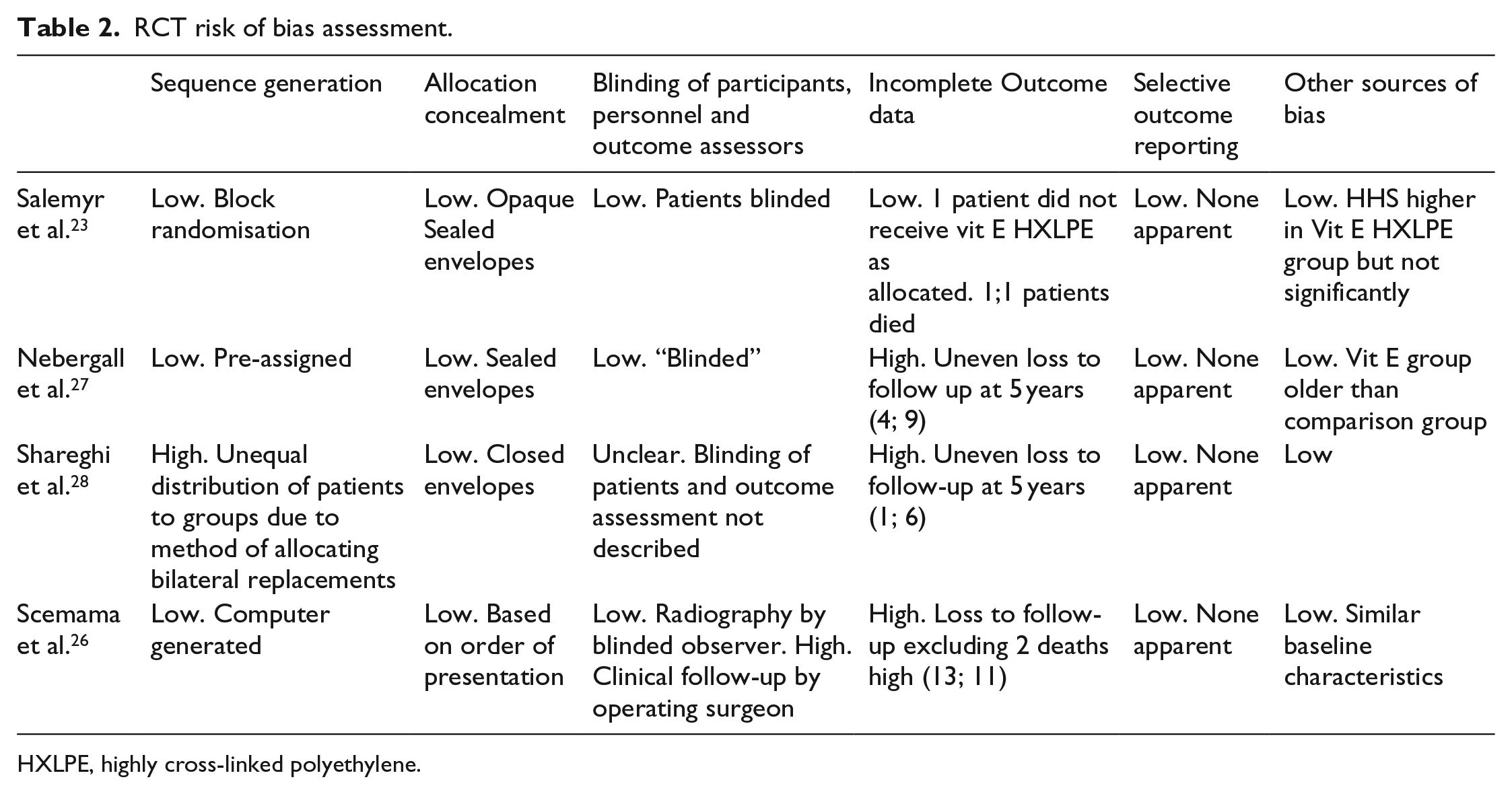
HXLPE, highly cross-linked polyethylene.
Vitamin E HXLPE compared to HXLPE
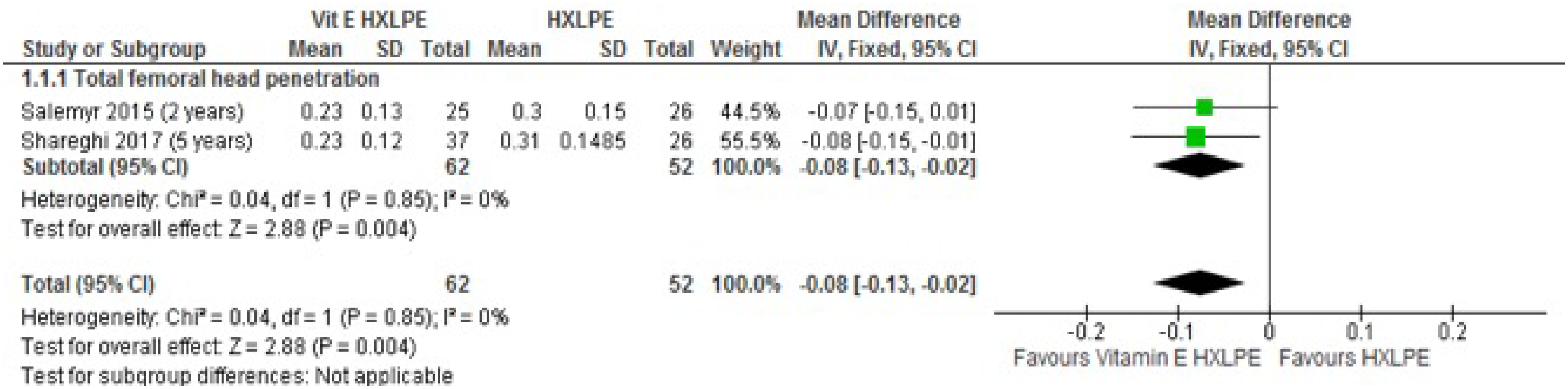
All RCTs used radiostereometry (RSA) to examine femoral head penetration. In 2 studies with 187 patients followed up for 2 and 5 years,23,28 total reported femoral head penetration was presented. In the meta-analysis shown in Figure 3, total reported femoral head penetration was significantly less in the vitamin E diffused HXLPE groups compared with conventional HXLPE, mean difference 0.08 mm (95%CI 0.13, 0.02; p = 0.004) and no heterogeneity was evident (Figure 3). However, the RSA measurement errors in these 2 studies were 0.13 mm and 0.14 mm respectively therefore this numerically significant difference is unlikely to be clinically significant. Furthermore only 1 study was at low risk of bias and in this study with 51 patients followed up, 23 the difference between groups was not statistically significant (p = 0.09). In 1 case-control study there was no difference between patients in femoral head penetration between vitamin E blended HXLPE and HXLPE liners (p = 0.161) but risk of bias was high due to the reporting of interim follow up of 24% of patients. 20
PRISMA flow diagram.
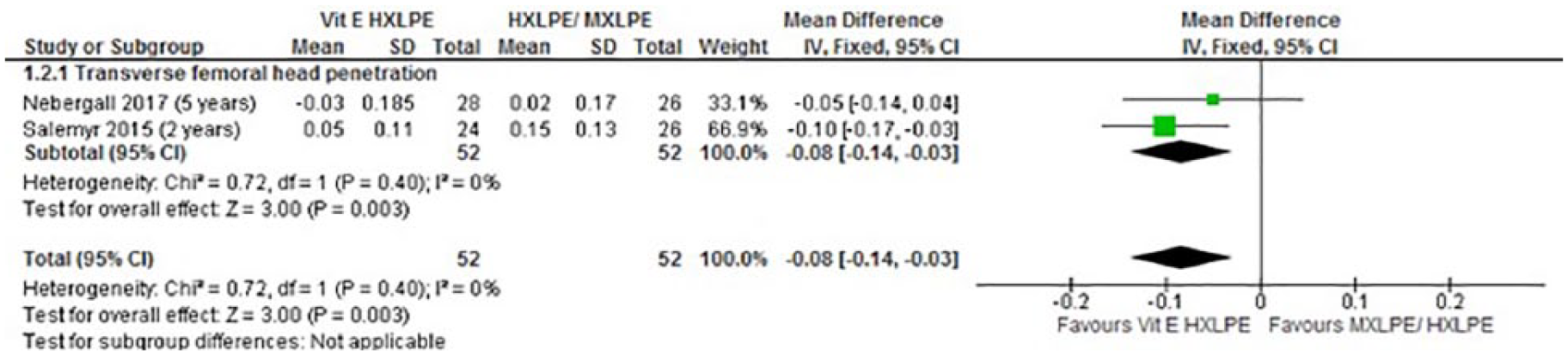
Meta-analyses of femoral head penetration by vector are shown in Figures 4–6. Transverse femoral head penetration was reported in 2 RCTs with data from 104 patients followed up for 2 and 5 years.23,27 In the meta-analysis shown in Figure 4, transverse femoral head penetration was lower in patients receiving a Vitamin E diffused HXLPE liner, mean difference 0.08 mm (95%CI 0.03, 0.14; p = 0.003) with no heterogeneity evident. In the 1 study at low risk of bias, 23 the difference was statistically significant (p = 0.004).
Meta-analysis of total femoral head penetration.
Meta-analysis of transverse femoral head penetration.
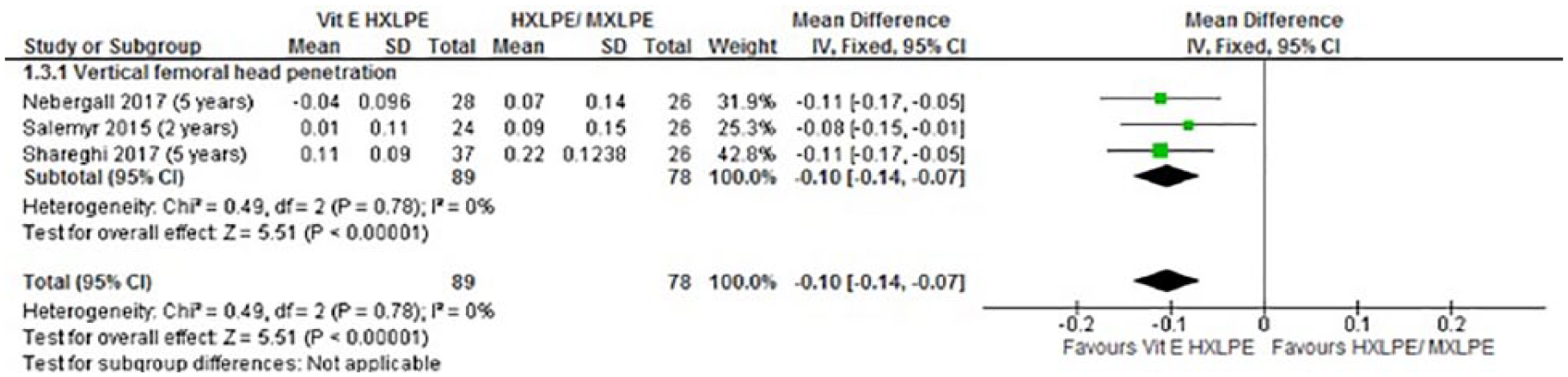
Meta-analysis of vertical femoral head penetration.
3 RCTs with 167 patients followed up for 2 or 5 years reported vertical femoral head penetration.23,27,28 In the meta-analysis shown in Figure 5, vertical head penetration was lower in patients receiving a vitamin E diffused HXLPE liner, mean difference 0.10 mm (95% CI 0.07, 0.14; p < 0.00001) and there was no heterogeneity between studies. In the 1 study with low risk of bias, 23 the difference was statistically significant, p = 0.035.
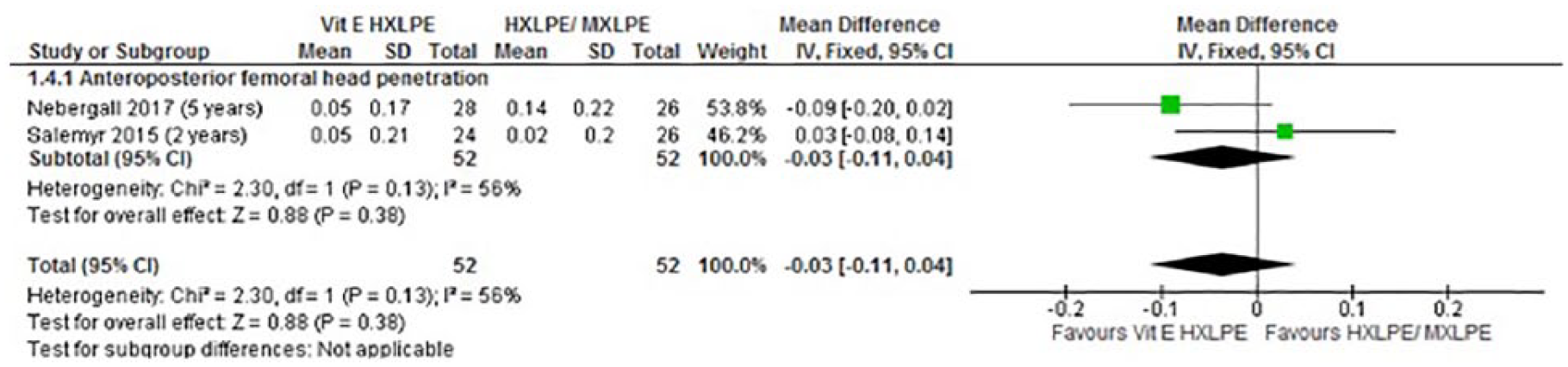
2 RCTs with 104 patients followed up reported anteroposterior femoral head penetration at 2 and 5 years.23,27 The meta-analysis in Figure 6 showed a high level of heterogeneity between the studies, I2 = 56% and we only show the results for completeness. One study showed a trend favouring the group who received a vitamin E diffused HXLPE liner, 27 and the other a trend favouring the control group receiving HXLPE. 23 Neither trend was statistically significant and only the latter study was at low risk of bias.
Revision rates
Study sample sizes were small and revision rates low. Overall there were 3 revisions in the vitamin E diffused group and 5 revisions in the control HXLPE group. Two revisions for dislocations occurred in patients receiving vitamin E diffused HXLPE and 1 in control patients receiving HXLPE but all were in a study with unclear risk of bias due to uneven losses to follow up between groups at 5 years. 27 In the case control study with high risk of bias, there was 1 dislocation in patients receiving blended vitamin E HXLPE liners compared with 2 in those receiving an HXLPE liner.
Patient-reported outcomes
2 RCTs with 104 patients and data suitable for meta-analysis reported the Harris Hip Score at 2 years and 5 years follow-up.23,27 As shown in Figure 7, heterogeneity between studies was high. 1 study with low risk of bias showed no statistically significant difference between groups at 2 years (p = 0.295). One RCT with data suitable for meta-analysis and another only reporting medians and ranges had unclear risk of bias due to uneven loss to follow up. In neither was there a statistically significant difference in HHS between groups.27,28
Meta-analysis of anteroposterior femoral head penetration.
In 2 RCTs, patient-reported health related quality of life was assessed using the Euroquol-5D (EQ-5D).23,27 There were no differences between outcomes in either study, including one at low risk of bias. 23
Vitamin E blended HXLPE compared to UHMWPE
In 1 RCT with 100 patients randomised and followed up for 3 years, vitamin E blended HXLPE liners were compared with UHMWPE liners. 26 Total head penetration was lower in the vitamin E HXLPE group (p = 0.04) but the study was at unclear risk of bias due to high losses to follow up. There was no difference in functional outcome measured using the Merle d’Aubigné score (p > 0.99).
Discussion
Total hip replacement is a clinically effective and cost-effective intervention. 29 Any improvement in the outcome of THR is likely to arise through reducing the incidence of adverse events or reducing the need for subsequent revision surgery. This formal systematic review and meta-analysis has shown that vitamin E HXLPE has reduced femoral head penetration over highly cross-linked and conventional polyethylenes. However, the differences are small in comparison to the measurement error of the techniques used to measure it and there is no evidence from our rigorous systematic review to show a clinically significant benefit of vitamin E HXLPE over HXLPE in terms of revision rate or function at this early stage. The lack of difference in functional scores is perhaps not surprising as HHS is a score to assess the effect of THR as an intervention and not to tell the difference between patients undergoing THR with different types of bearing surface. Ceramic-on-HXLPE in primary THR has been shown to have the lowest all-cause revision rates in a large national joint registry study and the reduced wear evident with the use of vitamin E HXLPE may lead to further reduction in revision rates. 30 A reduction in revision rates has not been shown in this study.
The findings of our study should be interpreted with caution. A recent high quality systematic review and network meta-analysis of 3177 THRs concluded that there was currently insufficient evidence to recommend any bearing combination over a traditional metal on UHMWPE THR. 31 However, a prospective RCT of 122 patients at 10 years follow-up not included in this systematic review and network meta-analysis showed that HXLPE liners have a significantly reduced wear and greater survival rate compared to UHMWPE liners. 32 Furthermore although in vitro evidence has shown increased bacterial resistance with vitamin E HXLPE, 33 there was no evidence in our study to support a decreased rate of revision for periprosthetic infection with this bearing surface.
Systematic review and meta-analysis with assessment of risk of bias can help clinicians to interpret results of studies in diverse settings with different outcome measures. There are limtations to this study, however. There are a limited number of randomised controlled trials all of limited follow-up from which to extract data and there were only 187 patients contributing to the meta-analysis of total femoral head penetration. Further RCTs examining vitamin E HXLPE are underway however.34,35 We did not perform a network meta-analysis to compare blended and diffused vitamin E HXLPE especially given the high risk of bias determined in the only study that examined the latter. There were a variety of femoral head sizes used in the studies and both metal and ceramic femoral heads were included. However, we extracted data using rigorous selection criteria and there was low heterogeneity for total femoral head penetration. Furthermore, this study could not account for precise cup positioning, patient activity, body mass index and whether the requisite hip biomechanics were restored in the cases used; such factors we acknowledge can affect wear rates.
Long-term follow-up, high-quality independent RCTs involving large numbers of patients and using consistent outcome reporting or large generalisable observational cohorts with comprehensive coverage are required to determine if lower wear results in lower revision rates. Such studies should be undertaken however before guidance can be provided on clinical effectiveness of new technologies in THR.
Conclusion
This systematic review and meta-analysis showed that there were numerically but not clinically significant wear advantages in terms of femoral head penetration for vitamin E HXLPE over HXLPE. There was no improvement in revision rates or functional outcome at this stage. However, there were few high-quality studies and longer-term follow-up is required. This bearing surface has encouraging early results in terms of wear.
Footnotes
Appendix
PRISMA checklist.
| Section/topic | Item No | Checklist item | Reported on page No |
|---|---|---|---|
|
|
|||
| Title | 1 | Identify the report as a systematic review, meta-analysis, or both | 1 |
|
|
|||
| Structured summary | 2 | Provide a structured summary including, as applicable, background, objectives, data sources, study eligibility criteria, participants, interventions, study appraisal and synthesis methods, results, limitations, conclusions and implications of key findings, systematic review registration number | 1 |
|
|
|||
| Rationale | 3 | Describe the rationale for the review in the context of what is already known | 2 |
| Objectives | 4 | Provide an explicit statement of questions being addressed with reference to participants, interventions, comparisons, outcomes, and study design (PICOS) | 2 |
|
|
|||
| Protocol and registration | 5 | Indicate if a review protocol exists, if and where it can be accessed (such as web address), and, if available, provide registration information including registration number | 2 |
| Eligibility criteria | 6 | Specify study characteristics (such as PICOS, length of follow-up) and report characteristics (such as years considered, language, publication status) used as criteria for eligibility, giving rationale | 2 |
| Information sources | 7 | Describe all information sources (such as databases with dates of coverage, contact with study authors to identify additional studies) in the search and date last searched | 2 |
| Search | 8 | Present full electronic search strategy for at least one database, including any limits used, such that it could be repeated | Figure 1 |
| Study selection | 9 | State the process for selecting studies (that is, screening, eligibility, included in systematic review, and, if applicable, included in the meta-analysis) | 2 |
| Data collection process | 10 | Describe method of data extraction from reports (such as piloted forms, independently, in duplicate) and any processes for obtaining and confirming data from investigators | 2 |
| Data items | 11 | List and define all variables for which data were sought (such as PICOS, funding sources) and any assumptions and simplifications made | 2 |
| Risk of bias in individual studies | 12 | Describe methods used for assessing risk of bias of individual studies (including specification of whether this was done at the study or outcome level), and how this information is to be used in any data synthesis | 3 |
| Summary measures | 13 | State the principal summary measures (such as risk ratio, difference in means). | 3 |
| Synthesis of results | 14 | Describe the methods of handling data and combining results of studies, if done, including measures of consistency (such as I2 statistic) for each meta-analysis | 4 |
| Risk of bias across studies | 15 | Specify any assessment of risk of bias that may affect the cumulative evidence (such as publication bias, selective reporting within studies) | 5 |
| Additional analyses | 16 | Describe methods of additional analyses (such as sensitivity or subgroup analyses, meta-regression), if done, indicating which were pre-specified | 5 |
|
|
|||
| Study selection | 17 | Give numbers of studies screened, assessed for eligibility, and included in the review, with reasons for exclusions at each stage, ideally with a flow diagram | Figure 1 |
| Study characteristics | 18 | For each study, present characteristics for which data were extracted (such as study size, PICOS, follow-up period) and provide the citations | Table 1 |
| Risk of bias within studies | 19 | Present data on risk of bias of each study and, if available, any outcome-level assessment (see item 12). | Table 2 |
| Results of individual studies | 20 | For all outcomes considered (benefits or harms), present for each study (a) simple summary data for each intervention group and (b) effect estimates and confidence intervals, ideally with a forest plot | 3-4 |
| Synthesis of results | 21 | Present results of each meta-analysis done, including confidence intervals and measures of consistency | Figures 3-7 |
| Risk of bias across studies | 22 | Present results of any assessment of risk of bias across studies (see item 15) | 6 |
| Additional analysis | 23 | Give results of additional analyses, if done (such as sensitivity or subgroup analyses, meta-regression) (see item 16) | Not Applicable |
|
|
|||
| Summary of evidence | 24 | Summarise the main findings including the strength of evidence for each main outcome; consider their relevance to key groups (such as health care providers, users, and policy makers) | 6 |
| Limitations | 25 | Discuss limitations at study and outcome level (such as risk of bias), and at review level (such as incomplete retrieval of identified research, reporting bias) | 8 |
| Conclusions | 26 | Provide a general interpretation of the results in the context of other evidence, and implications for future research | 8 |
|
|
|||
| Funding | 27 | Describe sources of funding for the systematic review and other support (such as supply of data) and role of funders for the systematic review | 8 |
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the NIHR Biomedical Research Centre at the University Hospitals Bristol NHS Foundation Trust and the University of Bristol. The views expressed in this publication are those of the author(s) and not necessarily those of the NHS, the National Institute for Health Research or the Department of Health.