
Abstract
Purpose:
Aseptic loosening is rare after primary total hip arthroplasty (THA) with mostly uncemented tapered stems; however, different factors can modify the results. We question whether 3 different current femoral components and/or the surgical technique affect the clinical and radiological outcome after a minimum follow-up of 10 years.
Methods:
889 uncemented tapered stems implanted from 1999 to 2007 were evaluated for a minimum follow-up of 10 years. Group 1 (273 hips) shared a conical shape and a porous-coated surface, group 2 (286 hips) a conical splined shape and group 3 (330 hips) a rectangular grit-blasted stem. Groups 1 and 2 were implanted through a posterolateral approach and group 3 using an anterolateral approach. Clinical outcomes and anteroposterior and sagittal radiographic analyses were compared.
Results:
No thigh pain was reported in unrevised patients. Mean Harris Hip score was lower for patients in group 3 for pain and function at all intervals. 14-year implant survival for aseptic loosening was 98.2% (95% confidence interval [CI] 96.2–100) in group 3. No revision for aseptic loosening was found with the other designs. A stem position outside neutral limits in the sagittal alignment (p = 0.001, hazard ratio: 6.17, 95% CI, 2.05–18.61) was associated with aseptic loosening in group 3.
Conclusions:
Most current uncemented straight tapered femoral components can provide adequate bone fixation in primary THA after 10 years. Conical stems inserted through a posterolateral approach are more reliable than rectangular ones inserted through an anterolateral approach.
Introduction
Many contemporary uncemented stem designs have been associated with excellent outcomes and minimal bone remodelling changes in primary total hip arthroplasty (THA).1–4 Given the variation that exists in these designs and surgical techniques, it is important to continue investigating the outcome of these THAs to maximise patient outcomes. 5
Different tapered stems with a fixation located primarily at the metaphyseal-diaphyseal junction can result in bone fixation by different methods. 6 Alignment on both the anteroposterior (AP) and sagittal plane are equally important for this purpose. The femoral neck is anteverted, has an anterior bow, the femoral diaphysis a posterior bow and the femoral neck arises anterior to the axis of the femoral canal anatomy.7,8 The resulting femoral head centre, which may affect impingement and dislocation-related complications, is associated with the functional stem anteversion that depends on anterior or posterior tilting. 9 Modern tapered wedge stems better accommodate the double bow of the proximal femur in the sagittal plane. 10
We ask whether 1 of 3 different tapered uncemented femoral component types perform differently than the others. We have analysed the clinical and radiological outcomes of 3 different designs implanted in our institution over at least 10 years. We assessed complication rate, clinical results and survivorship analysis regarding revision stem surgery for any cause and for aseptic loosening in all groups. We also evaluated bone remodelling changes over time and the possible reasons for aseptic loosening, if any, with particular attention to sagittal alignment.
Patients and methods
In this cohort analysis of our prospective database, 988 uncemented THAs with a straight tapered stem implanted in our institution between January 1999 and December 2007 were identified. A minimum time of 10 years from the operation was required for unrevised stems to be included in the follow-up study. Revisions for cup loosening with radiographically osseointegrated stems were not excluded. Eight-hundred and eighty-nine hips (688 patients) were prospectively followed and formed the basis of the follow-up study. Approval from the regional ethics committee from our Institution was obtained (PI-3101).
3 different femoral components were classified into groups according to Khanuja et al.: 6 Group 1, considered as type 3-A, rounded conical tapered stems, most with porous coating on the proximal part and 3-point fixation, included 273 hips with a Summit stem (De Puy-Johnson & Johnson, Warsaw, IN, USA); Group 2, type 3-B, conical tapered stems with sharp-edge longitudinal splines, that cut into the bone and provide rotational stability, included 286 hips with a Cerafit fully hydroxyapatite (HA) coated stem (Ceraver, Roissy, France); Group 3, type 3-C, rectangular tapered stems that are grit-blasted across the entire length, included 330 hips with a SL-Plus stem (Smith & Nephew, Memphis, TN, USA). All hips had an uncemented press-fit cup: Group 1 had a Duraloc cup (De Puy), conventional polyethylene (CPE) with a 28 mm metallic femoral head diameter; group 2 a Cerafit cup (Ceraver) with an alumina-on-alumina 28 or 32 mm femoral head; and group 3 a EP-Fit cup (Smith & Nephew) with a metal-on-CPE 28 mm femoral head size. During these years, CPEs were used in patients over the age of 65 years and alternative bearing surfaces such as ceramics or highly cross-linked PEs were used in younger patients. Uncemented stems were used in patients under the age of 80 years or those over that age with a Dorr femoral type 1 or 2. Patients with femoral deformities, previous surgeries requiring material removal or additional shortening osteotomies were not included in the study There were more male, younger and more active patients in group 2 (Table 1). Table 2 includes data on hips in each group.
Patient demographic data.
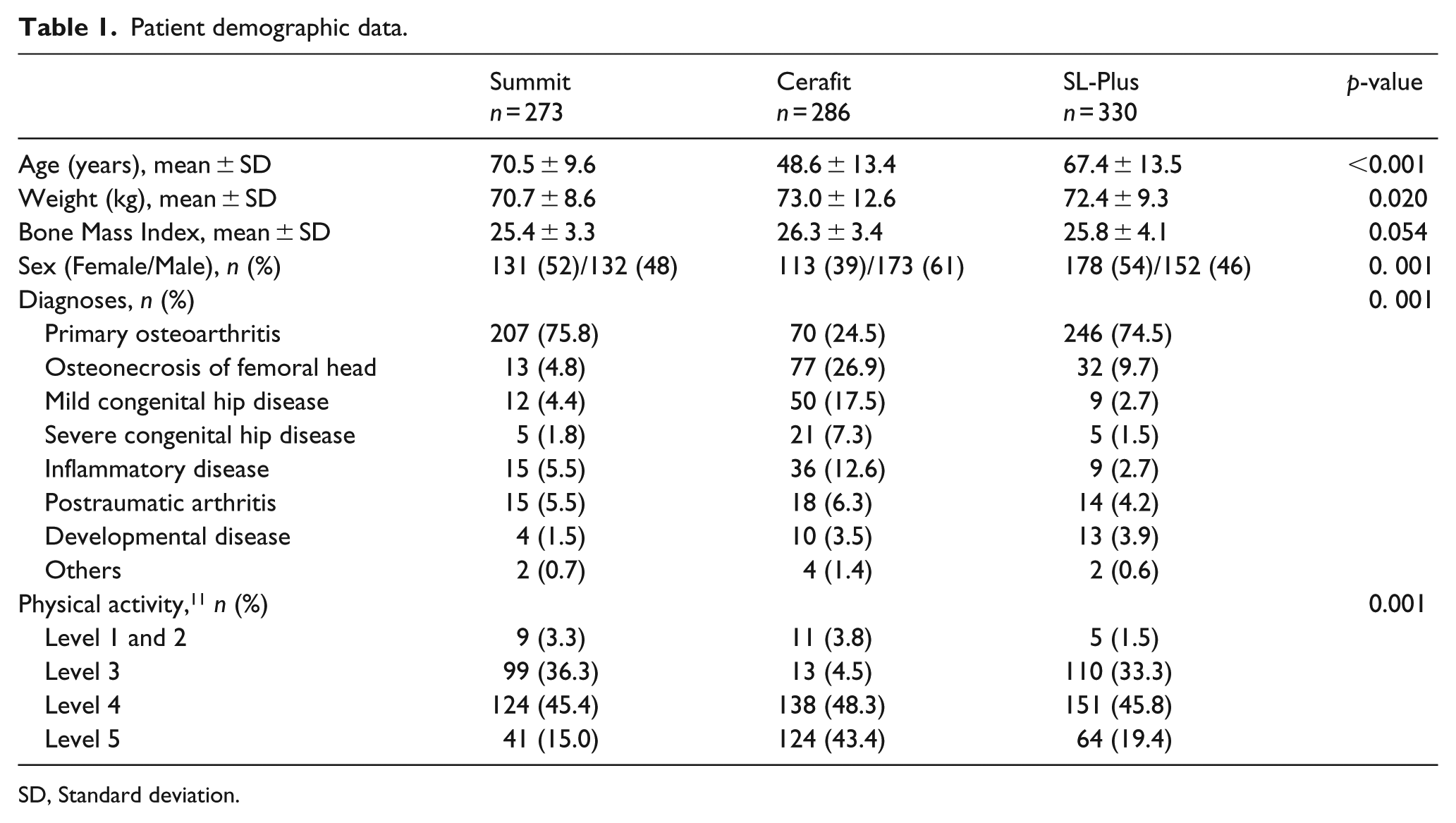
SD, Standard deviation.
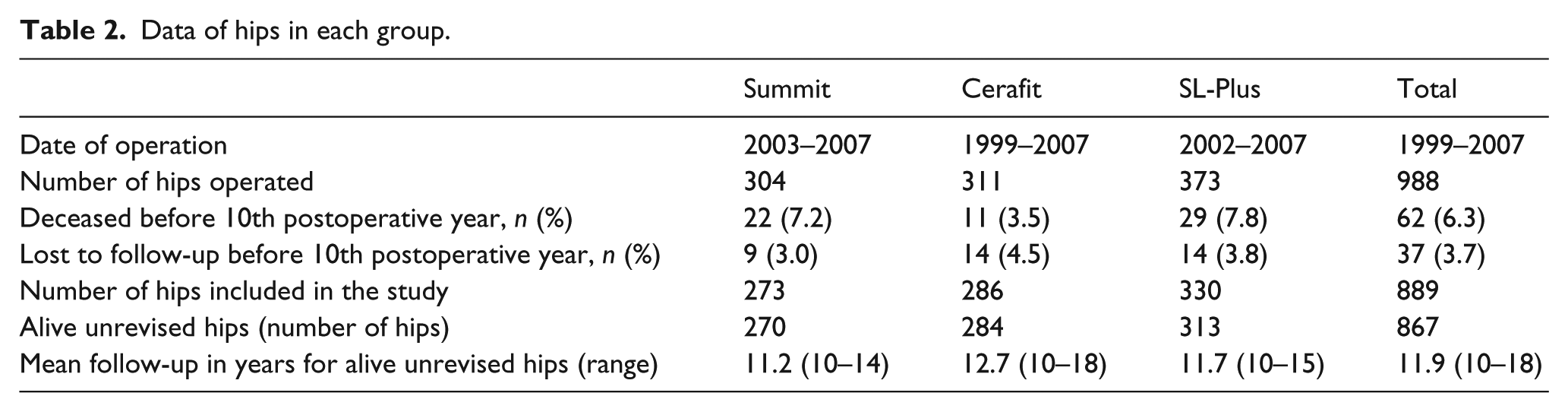
Data of hips in each group.
Operative data
In groups 1 and 2 different surgeons used a posterolateral approach. In group 3 an anterolateral approach was performed by surgeons following recommendations reported by Zweymuller when this femoral component was first introduced. 3 Stems were implanted as recommended by the manufacturers: the Summit stem requires distal reamers and proximal broaches; the Cerafit stem conical broaches; and, the SL-Plus stem rectangular broaches to prepare the canal. The patients were allowed to place their partial weight on the operated limb the second day after surgery, as pain allowed, and under physiotherapeutic guidance in all groups. Patients walked with crutches for 3–6 weeks postoperatively depending on wound conditions, pain and gait stability.
Clinical and radiographic assessment
On each postoperative visit, patients were clinically evaluated using the Harris Hip Score (HHS). 12 Patients were also asked about the degree and location of their pain. 13 The standard imaging protocol of our institution consists of pelvic AP and lateral proximal femur radiographs taken immediately after the operation, at 6 and 12 months, and annually thereafter for all patients following the same protocol. Measurements were performed using analogic radiographs until 2006. After that time, digital radiographs were used (PACS Health, Scottsdale AZ, USA). Preoperative femoral type was classified according to Dorr et al. 14 Stem position in the AP radiographs was defined as neutral, valgus (5° of lateral deviation), or varus (5° of medial deviation) (Figure 1). Sagittal stem position was recorded using the lateral radiograph of the proximal femur, and defined as neutral if the alignment was within 0 and 5 degrees from the longitudinal axis, or anterior (>5°) (Figure 2). All radiographs were assessed by a single author, who repeated the measurements 3 times for each radiograph before recording the mean. Femoral canal filling was the ratio of the width of the stem to the width of the medullary canal, as measured in AP; 15 and lateral radiographs at 3 levels: Level A (at the metaphyseal part of the stem); Level B (at the middle of the stem); and Level C (1 cm proximal to the tip) (Figure 3). The distribution of any radiolucent lines (RL) seen on AP radiographs was recorded in the zones described by Gruen et al. 16 Only RLs affecting 50% or more of a Gruen zone were considered. 17 Femoral osteolysis, 18 subsidence, 19 femoral osteopenia and fixation were also recorded.20,21
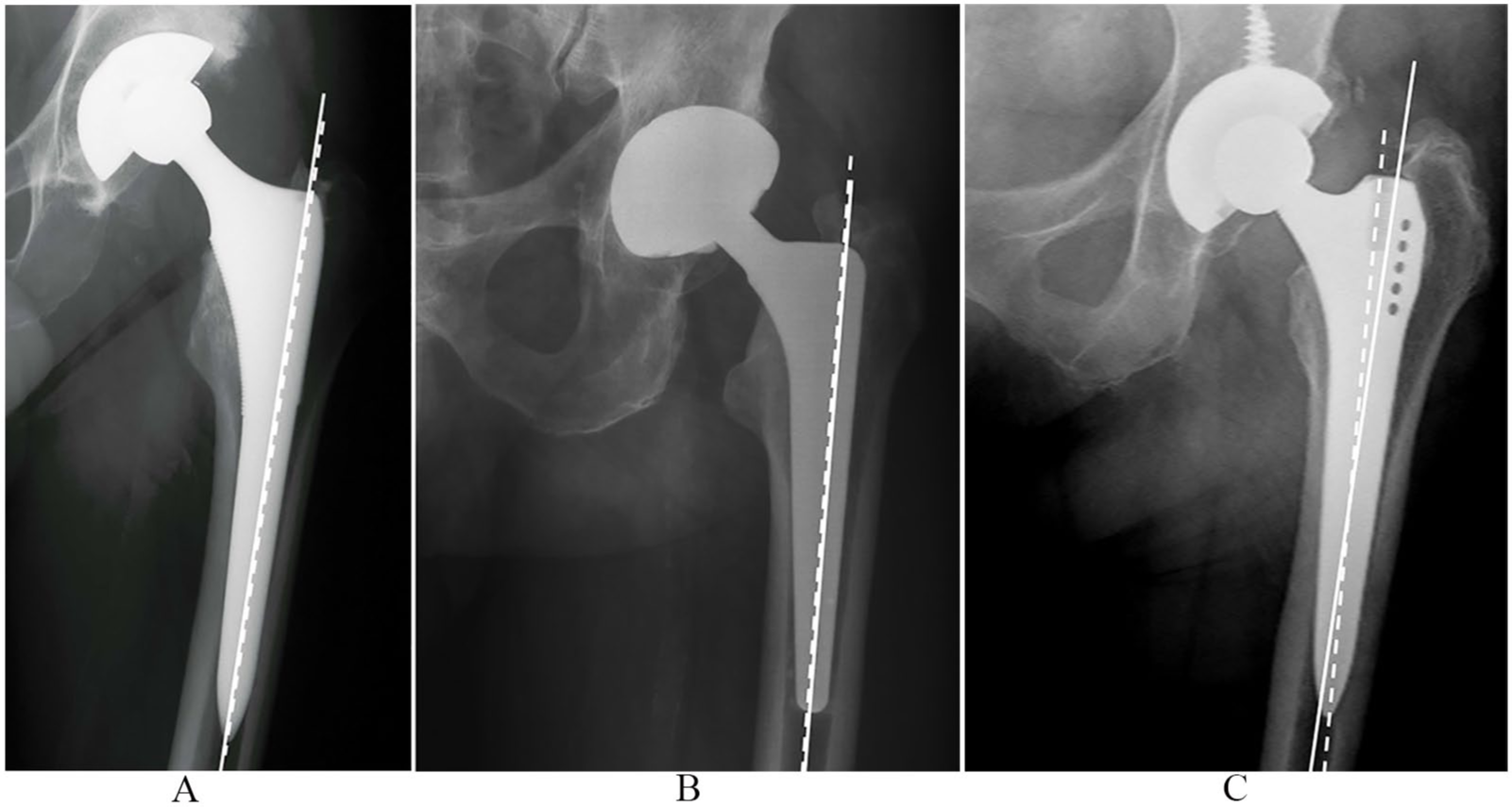
Anteroposterior alignment of 3 different stems evaluated in the study. Solid lines represent proximal femoral axis and dotted lines femoral component axis: (A) Summit stem, (B) Cerafit stem, and (C) SL-Plus stem.
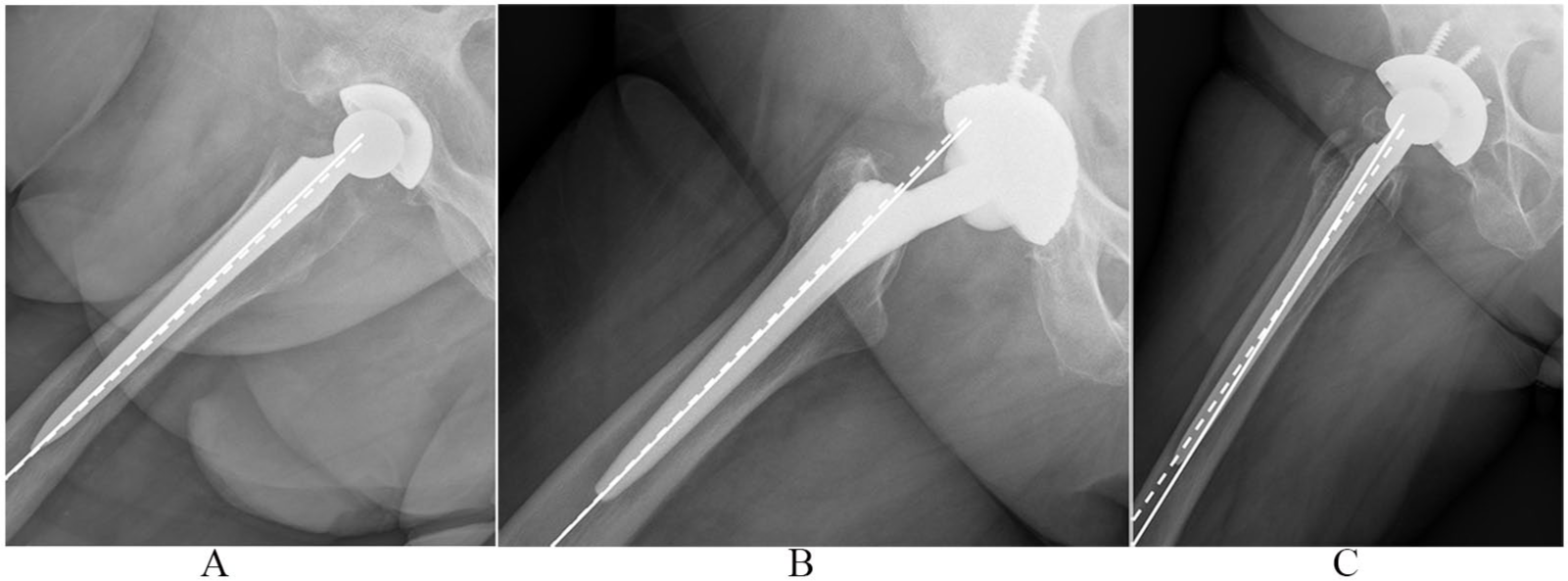
Sagittal alignment of 3 different stems evaluated in the study. Solid lines represent proximal femoral axis and dotted lines femoral component axis: (A) Summit stem, (B) Cerafit stem, and (C) SL-Plus stem.
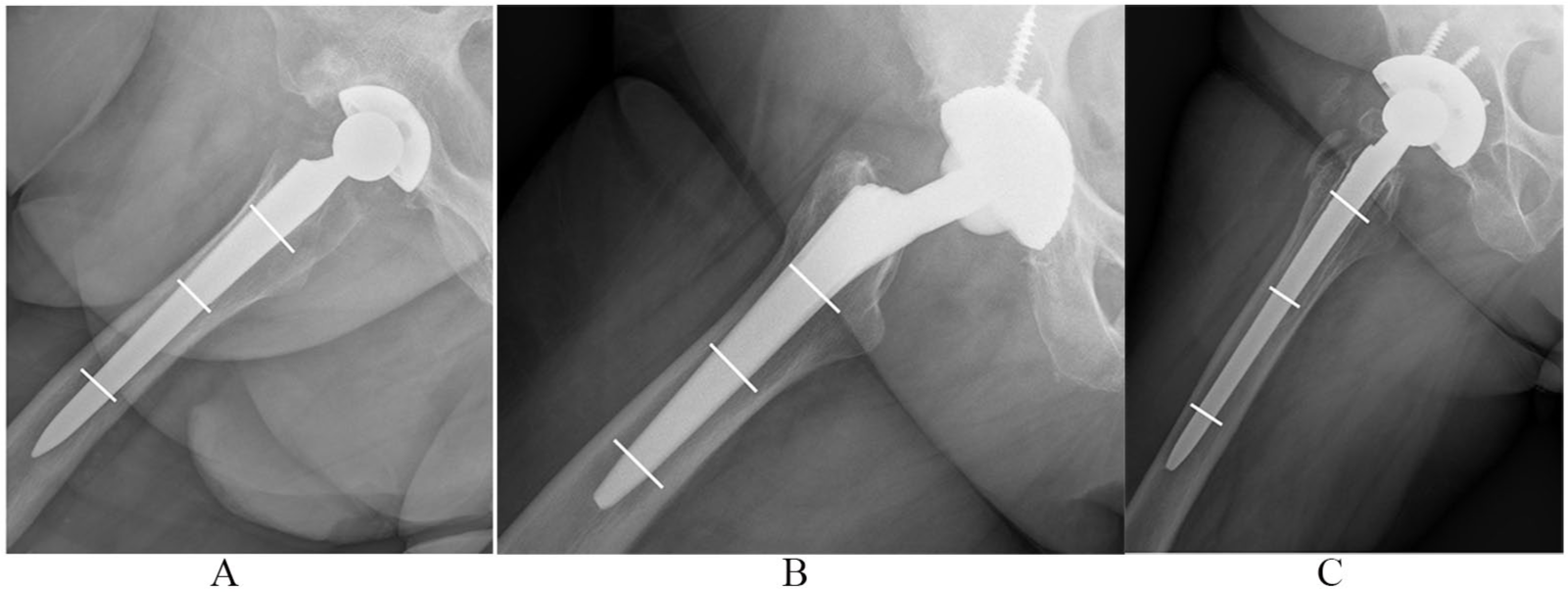
Femoral canal filling at 3 different levels evaluated on the sagittal plane in the 3 groups: (A) Summit stem, (B) Cerafit stem, and (C) SL-Plus stem.
Statistics
Qualitative data were expressed as counts and percentages and quantitative data by means ± standard deviation (SD). Qualitative data were compared using the chi-square test or Fisher’s exact test, and quantitative data for these groups were compared using the ANOVA or Kruskal-Wallis test. The level of significance for preoperative and immediate postoperative patient data are indicative of homogeneity between groups. “Post-hoc” comparisons were studied by Bonferroni’s test. Kaplan-Meier survivorship analysis, with 95% confidence intervals (CIs), was used to estimate the cumulative probabilities of not having revision surgery for any cause and for aseptic stem loosening. Variance analysis was used to assess femoral canal filling at levels A, B and C. Main effects were the groups, femoral type and stem position. Interaction effects were studied at two levels: group and femoral type, group and stem position. A significant interaction effect (p < 0.1) would show that femoral type or stem position would differ by group. Differences in survival were determined using the log-rank test. Cox proportional hazard regression analysis was performed to determine whether age, sex, stem position (neutral or not), femoral type (funnel shaped, intermediate or cylindrical) or femoral canal filling at level A, B and C affected the femoral aseptic loosening rate for revision surgery over time. The level of significance was p < 0.05. Statistical analysis was performed by statistical package SAS 9.3 (SAS Institute Inc, Cary, NC, USA).
Results
There were 4 intraoperative cracks in group 1, 1 in group 2 and 2 in group 3, with 2 intraoperative subtrochanteric fractures in groups 1 and 2, and 3 in group 3; all were solved with cerclage wiring. There were 3 infections: a loosened stem with positive intraoperative cultures in group 2; and 2 early infections in the group 3 which were treated with a 2-stage revision. There were 17 dislocations in group 1, 2 in group 2 and 21 in group 3. 9 cups were revised due to dislocation in group 1, 2 in group 2 and 6 cups in group 3. There were 6 periprosthetic fractures: there was a femoral fracture with stable stem in group 1, 8 years postoperatively solved with an osteosynthesis, and 5 hips revised to an uncemented long femoral component, 3 in group 1 one, at 12 and 54 months postoperatively, 1 in group 2, at 48 months postoperatively and 1 in group 3, at 38 months postoperatively.
13 SL-Plus stems were revised due to aseptic loosening (Table 3). No hips were revised for aseptic loosening in the Summit or Cerafit groups. The survival rate of not having stem revision for any cause was 98.5% (CI, 98.8–100) for the Summit group at 12 years, 99.3% (CI, 97.9–100) for the Cerafit group at 16 years and 97.7% (CI, 94–100) for the SL-Plus group at 14 years (p = 0.11, log-rank test) (Figure 4). The survival rate for stem revision due to aseptic loosening was 98.2% (CI, 96.2–100) for the SL-Plus group at 14 years (Figure 5). No patient complained of thigh pain except of the revised stem. At the latest follow-up, clinical evaluation showed that results were inferior in the SL-Plus stem group for all parameters (Table 4).
Patient data for revision for aseptic loosened SL-Plus stems.
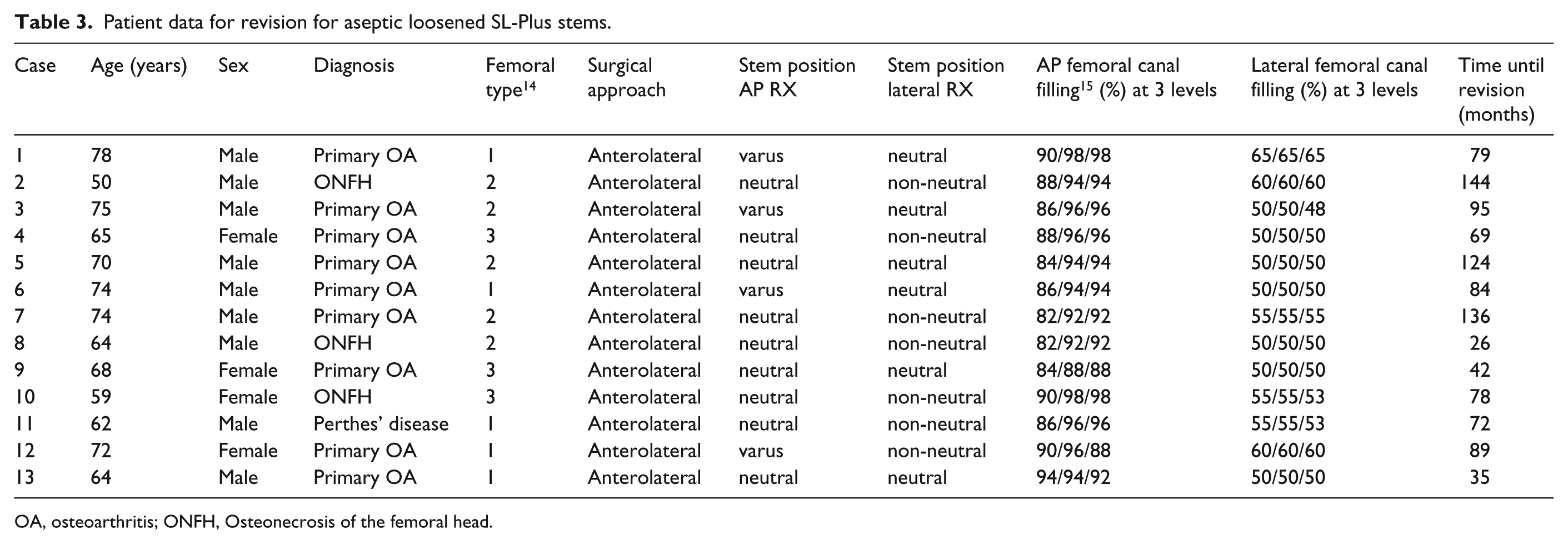
OA, osteoarthritis; ONFH, Osteonecrosis of the femoral head.
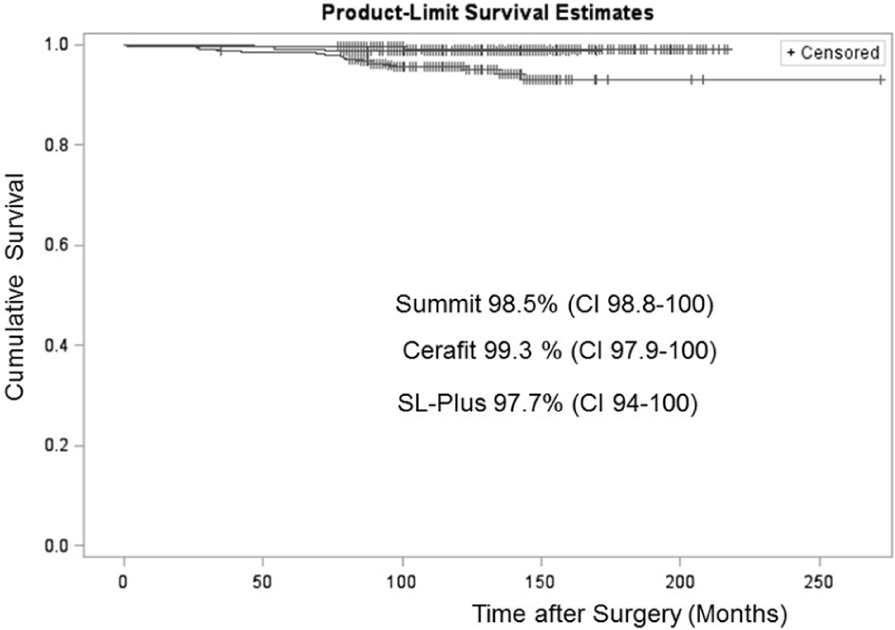
Kaplan-Meier curve comparing survival with femoral component revision for any cause as the endpoint in every group.
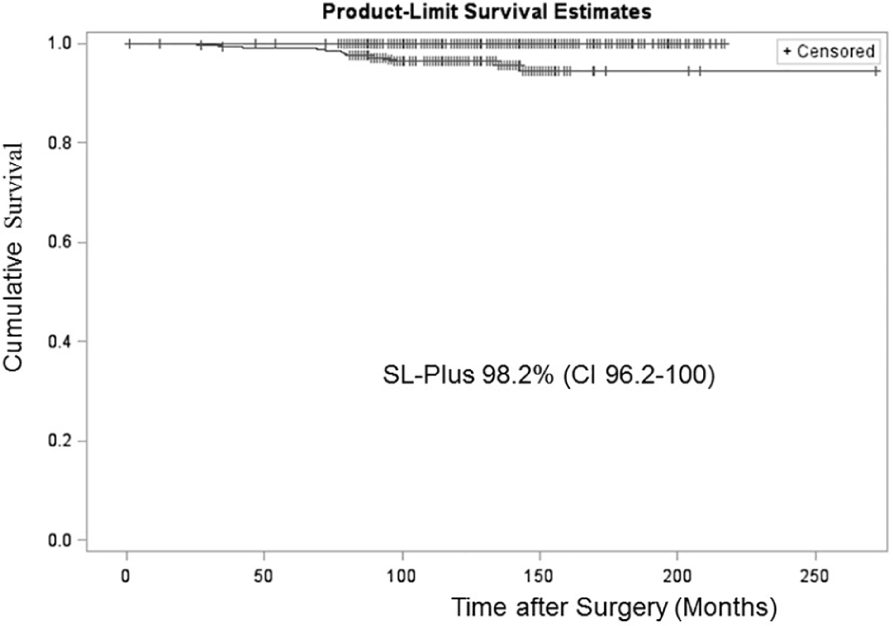
Kaplan-Meier curve comparing survival with femoral component revision for a septic loosening as the endpoint in every group. No hips were revised for aseptic loosening in the Summit or Cerafit groups.
Clinical results according to the Harris Hip score, 12 mean and standard deviation (SD), and change from preoperative to different postoperative intervals.
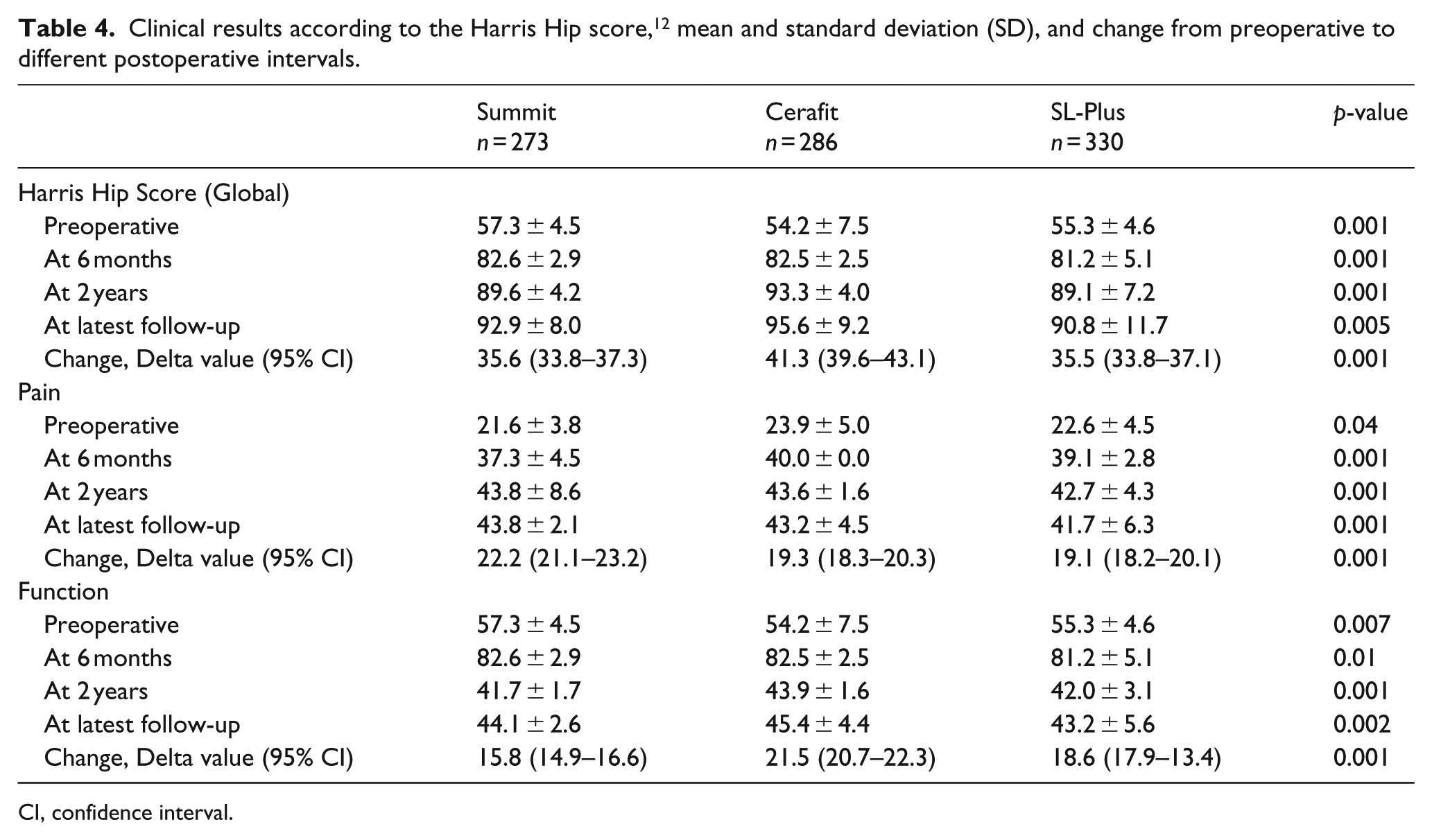
CI, confidence interval.
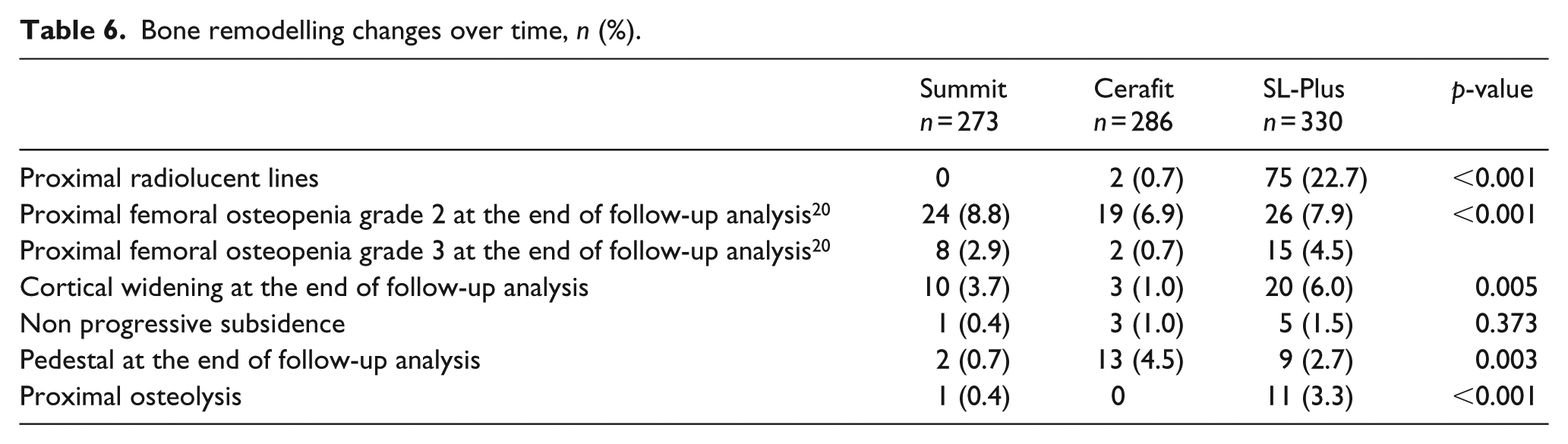
Radiographic analysis showed that in the SL-Plus group there were more hips in varus in the AP view, and an anterior position and less femoral canal filling in the lateral view (Table 5). There were more hips showing proximal RL, femoral osteopenia, cortical widening and proximal osteolysis in the SL-Plus group (Table 6). The average interval from operation to the appearance of RL lines in the 13 loosened stems in the SL-Plus group was 44.5 months (range 20–100), and in the other 62 hips with RL lines found in non-loosened stems without clinical relevance at the end of follow-up analysis, was 45.8 months (range 14–80). Cortical thickening was found in 10 hips (3.7%) in the Summit group; all were in Gruen et al. zone 5 and continued without clinical relevance at the end of follow-up analysis, with an average interval from operation to the appearance of cortical thickening of 33.4 months (range 14–78). Cortical thickening was also found in 20 hips (6.0%) in the SL-Plus group, all in Gruen zones 3 and 5, at a mean time of 30.3 months (range, 12–48) post-surgery. A pedestal was found in 13 hips (4.5%) in the Cerafit group and was without clinical relevance in all cases at the end of follow-up analysis; the pedestal was lateral in 9 hips and central in 4; the average interval from surgery to the appearance of a pedestal was 96.3 months (36–144 months). Proximal osteolysis was found in 11 hips (3.3%) in the SL-Plus group, at an average time of 64.4 months (range 24–120) post-surgery (Table 6). The multivariable Cox regression analysis showed that an SL-Plus stem was more frequently placed outside the neutral sagittal alignment and was thus associated with an increased risk of aseptic loosening (Table 7).
Radiographic data in the 3 groups.
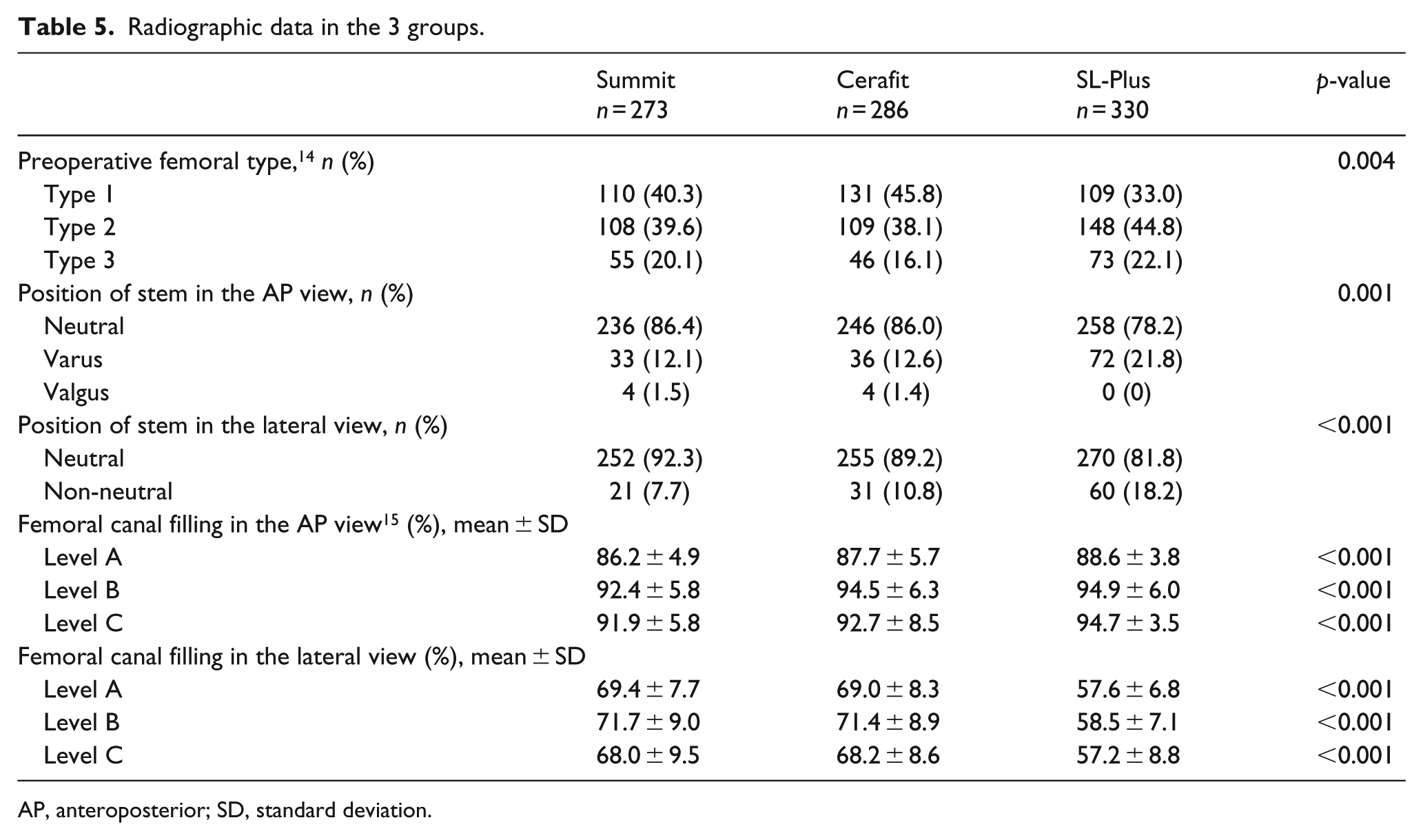
AP, anteroposterior; SD, standard deviation.
Bone remodelling changes over time, n (%).
Risk factors for aseptic loosening in the SL-Plus group (all inserted through an anterolateral approach).
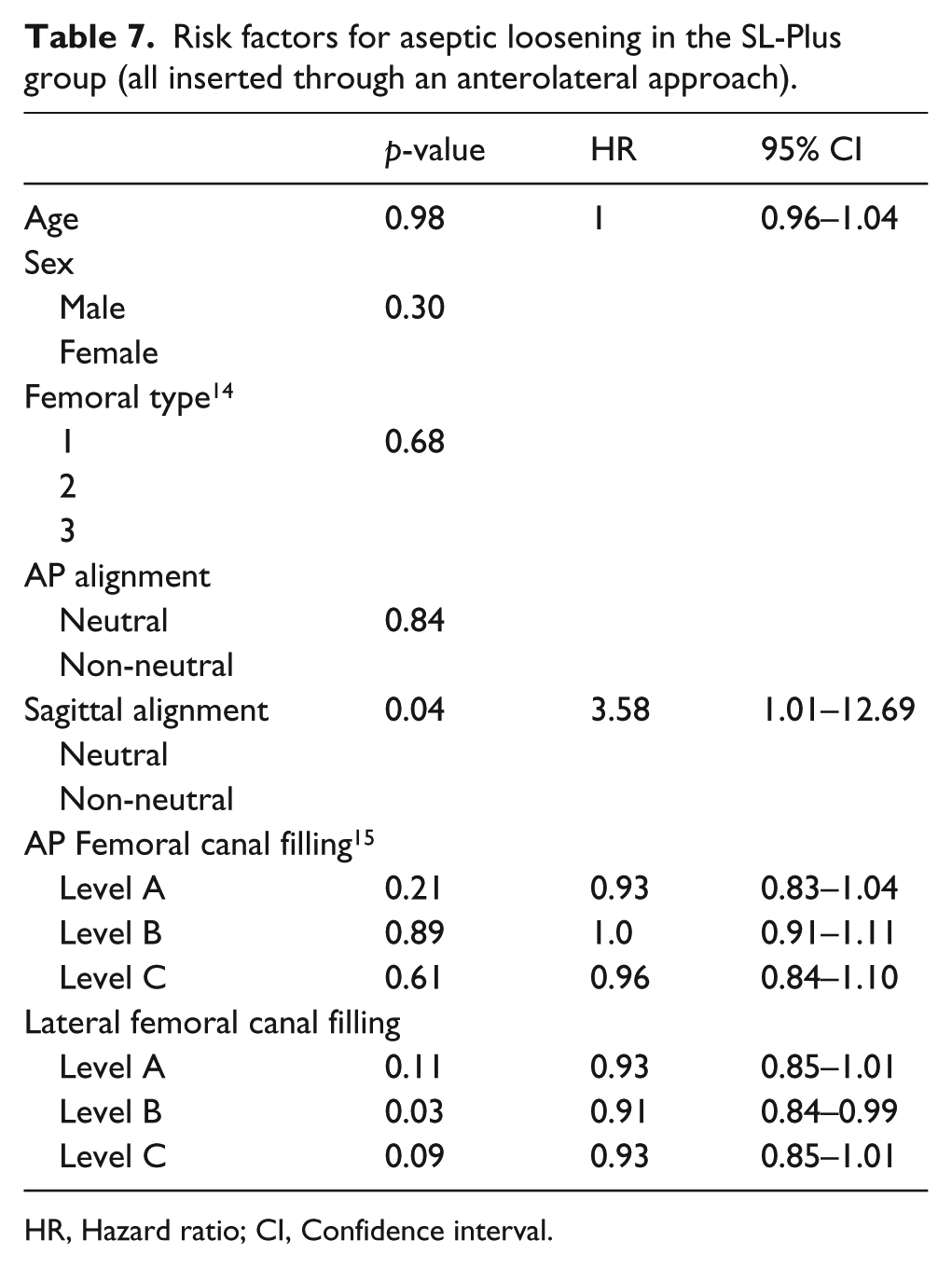
HR, Hazard ratio; CI, Confidence interval.
Discussion
Although most current uncemented femoral components are widely used given their very low percentage of complications and high functional score and survival rates, continued monitoring is critical in order to confirm these data. Straight tapered stems differ in terms of their surface characteristics, shape and surgical technique, so comparative studies may help to investigate whether these differences could affect outcome. The clinical results and probability of not having revision surgery of the stem were generally satisfactory 10 years after surgery; nevertheless we did identify some differences.
Intra- and postoperative complications, including infection and periprosthetic fractures, were uncommon in all groups. Hailer et al proposed that the incidence of early revision due to fracture indicates that patients receiving an uncemented stem are more vulnerable to trauma during the first postoperative year, and that some of these fractures probably occur during the index operation but remain undetected at the time of surgery. 1 Thigh pain, more frequently reported with the stiffer early anatomic uncemented stems,17,20,22 was only found in the loosened stems. This thigh pain in stable recent stems has not appeared in other studies of tapered femoral components.2,5,23 The survival rate between 12 and 16 years of follow-up for any cause in our series was above 95%, and even higher when aseptic loosening was the end-point, independently of different tapered stem designs, patient characteristics or surgical technique.
Although long-term results for all designs were good, femoral component alignment can affect clinical outcome. AP alignment can influence uncemented stem fixation as well as complications such as insufficiency fractures; 24 similarly, sagittal femoral component alignment affects the position of femoral head anteversion and consequently the risk of impingement. 9 Patients’ femoral characteristics, which can affect the torsion of a straight femoral component,25,26 and technical issues like bone-saving femoral-neck osteotomies can shift the femur entrance plane anteriorly and medially and result in an anterior tilt of the stem axis. 9 In this study, lateral canal filling and sagittal stem position were associated with aseptic loosening when using the SL-Plus femoral component.
Surgical approach may also influence sagittal alignment and clinical outcome. Mac Pherson et al. 27 recommended a posterior approach to expose the fossa piriformis; canal entry may be easier and this should improve sagittal alignment. Recently, Janssen et al. 28 found a higher risk of early aseptic loosening after using similar stems to the SL-Plus stems placed using an anterolateral approach. These authors suggested that the obstruction of the gluteus medius muscle could affect femoral preparation during surgery and result in under-sizing or malalignment. To date, more limping has been related to an anterolateral approach. 29
Each stem design is associated with a particular load pattern leading to specific adaptive periprosthetic bone remodelling. RL lines, more frequent in the SL-Plus group, can be partially explained due to differences in femoral canal filling and stem position in both AP and sagittal alignment. Interestingly, the SL-Plus stem proximal shoulder is wider than the previous Alloclassic design, 18 which might have influenced the high varus alignment rate. Zweymuller et al also reported that more cancellous bone is removed by rasping the bone of the neck resection line during any intraoperative change in the primary rasping-direction. 30 Possibly, proximal micro-motion against the distally well-fixed stem and the rectangular cross-sectional shape of the SL-Plus stems would create less rotational stability than was obtained with the more trapezoidal cross-section of the other designs. Despite HA use being recommended to enhance mineralized bone growth onto the implant,31,32 different series have demonstrated no differences in clinical and radiographic outcomes between stems with HA and the same stems without HA.33,34 Thus, metaphyseal debonding has also recently been reported as a possible failure mechanism after using an extensive HA coated tapered stem. 35 Stress shielding and cortical widening were frequent with older, stiffer designs;36–38 however, bone remodelling changes over time were uncommon in the Summit and Cerafit groups. Carlson et al. 5 also reported excellent bone fixation with minimal radiographic changes with the proximal porous-coated design used here. 5 In a computed tomography assisted osteodensitometry study, Mueller et al. 23 found that despite cancellous and cortical bone loss there was no thigh pain or loosening in patients with the Cerafit stem. It has been reported that the decreased rigidity of the tapered stems may transfer most of the femoral load onto the proximal portion of the stem, but, Karachalios et al. 39 showed that proximal bone atrophy is highest in the second postoperative year, recovering to baseline values at 10 years. Other radiographic findings like stem subsidence were infrequent in stable stems; in fact, subsidence was non-progressive, and hips became secondarily stable in all cases with loading.35,40
The main limitation to our study was that the Summit and Cerafit stems were inserted through a posterolateral approach and the SL-Plus stem through an anterolateral one. Secondly, the different follow-up times for different groups, the small number of events, and preoperative differences may have influenced some of the results. We recognise that our radiographic measurements of loosening, bone remodelling changes and subsidence may not be entirely precise. No computed tomography or dual-energy x-ray absorptiometry studies were used here to evaluate stress-shielding. Also, this is not a single-surgeon series and consequently an individual surgeon’s technique may have influenced the results.
Most current uncemented straight tapered stem designs can provide adequate bone fixation. Different ingrowth and ongrowth surfaces with or without HA coating are equally effective for this purpose; however, double rectangular femoral components are less forgiving than conical tapers with a porous-coated surface or with splines in the proximal area, particularly when inserted through an anterolateral approach. Continued follow-up is required to determine if these results are maintained over time. More studies are needed to determine whether surgical approach affects femoral component alignment.
Footnotes
Acknowledgements
Thank you to Rosario Madero, MS for her statistical support and Eduardo García-Cimbrelo, MD, PhD for reviewing the manuscript.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship and/or publication of this article.