
Abstract
Introduction:
The broad aim of this study was to compare the safety and efficacy of using barbed sutures and running closure versus interrupted placement of standard of care sutures for closure of the arthrotomy during total hip arthroplasty (THA). Specifically, we compared duration of arthrotomy closure, the number of sutures utilised for arthrotomy closure, and 90-day outcomes including wound-related readmission, reoperation, and complications.
Methods:
A total of 60 patients undergoing 60 THAs were enrolled in a prospective, single-blinded trial and randomised to receive either running closure of the arthrotomy with barbed sutures (n = 30) or interrupted closure with standard of care sutures (n = 30). Patients were eligible if they were undergoing primary THA for osteoarthritis and excluded if they had a BMI > 45 kg/m2 or age > 80 years or <18 years.
Results:
Arthrotomy closure duration was significantly shorter in the barbed suture group (3 minutes ± 9 seconds) versus the standard of care group (8 minutes ± 26 seconds, p < 0.001). The suture utilisation for arthrotomy closure was 1 suture in the barbed sutured group 28/30 (93%) patients versus 2–4 sutures in 27/30 (90%) in the standard of care group (p < 0.001). The overall number of wound-related complications in the barbed suture group was 1/30 (3%) versus 1/30 (3%) in the standard of care group (p = 1.00). The rate of suture abscesses was 1/30 (3%) in barbed suture group versus the standard of care (p = 1.00). There was trochanter bursitis 1/30 (3%) in the standard of care group versus zero in the barbed suture group (p = 1.00).
Conclusions:
These results suggest that barbed suture utilisation may be faster and more resource efficient than use of standard of care sutures for arthrotomy closure in THA.
ClinicalTrials.gov Identifier: NCT03285555
Introduction
Barbed suture technology allows for running closure of wounds previously closed with standard of care sutures applied in an interrupted fashion.1,2 Closure with barbed sutures theoretically produces water-tight wounds and also provides other benefits such as reduced closure time, lower rates of infection, and lower total hospital costs. 3 A recent systematic review of closure modalities concluded that barbed sutures may in fact significantly reduce closure time; however, this report noted that the inconsistent designs and methodological features of prior studies limited the strength of conclusions regarding these sutures. 1
The literature evaluating the use of barbed sutures in total hip arthroplasty (THA) remains comparatively sparse to that examining the use of these sutures in total knee arthroplasty (TKA). A number of studies have been performed on mixed cohorts of patients undergoing either TKA or THA4–6; however, inconsistent reporting of outcomes of THA patients in some studies and relatively low number of THA patients limits the applicability of these studies to a THA population. Studies that have focused solely on the use of barbed sutures in THA have generally been retrospective and non-randomised.7,8
Therefore, a randomised controlled study to evaluate arthrotomy closure during primary THA with barbed sutures versus standard of care sutures was performed. The following parameters were compared: (1) arthrotomy closure times; (2) number of sutures required; and (3) complications within 90 days postoperative, including wound related readmission and/or reoperation, stitch abscess, trochanter bursitis, wound hematoma, wound dehiscence, superficial surgical site infection, deep surgical site infection, periprosthetic joint infection (PJI).
Methods
Study population
A single-centre, single-hospital, prospective randomised, controlled trial was performed after institutional review board (IRB) approval and clinical trial registration. From July 2018 to February 2019, research personnel prospectively screened 191 patients who received a primary THA procedure. Exclusion criteria were: (1) age < 18 or > 80 years; (2) body-mass index (BMI) ⩾ 45 kg/m2; or (3) involvement in a concurrent interventional study. Figure 1 provides screening and exclusion details. Of the 144 eligible patients, 84 declined to participate. The most common reason patients declined was apprehension regarding barbs in the active group. Furthermore, many patients with a prior arthroplasty requested that they receive exactly the same type of closure in their previous surgery and were thus unable to be randomised. A total of 60 patients provided written consent for the study and enrolled (Figure 1). Baseline demographic and medical history data were collected using electronic health records. Charlson comorbidity index (CCI) for each patient was calculated as previously described. 9 Demographics and other baseline characteristics are summarised in Table 1. There were no statistically significant differences between the 2 groups. (p > 0.05).
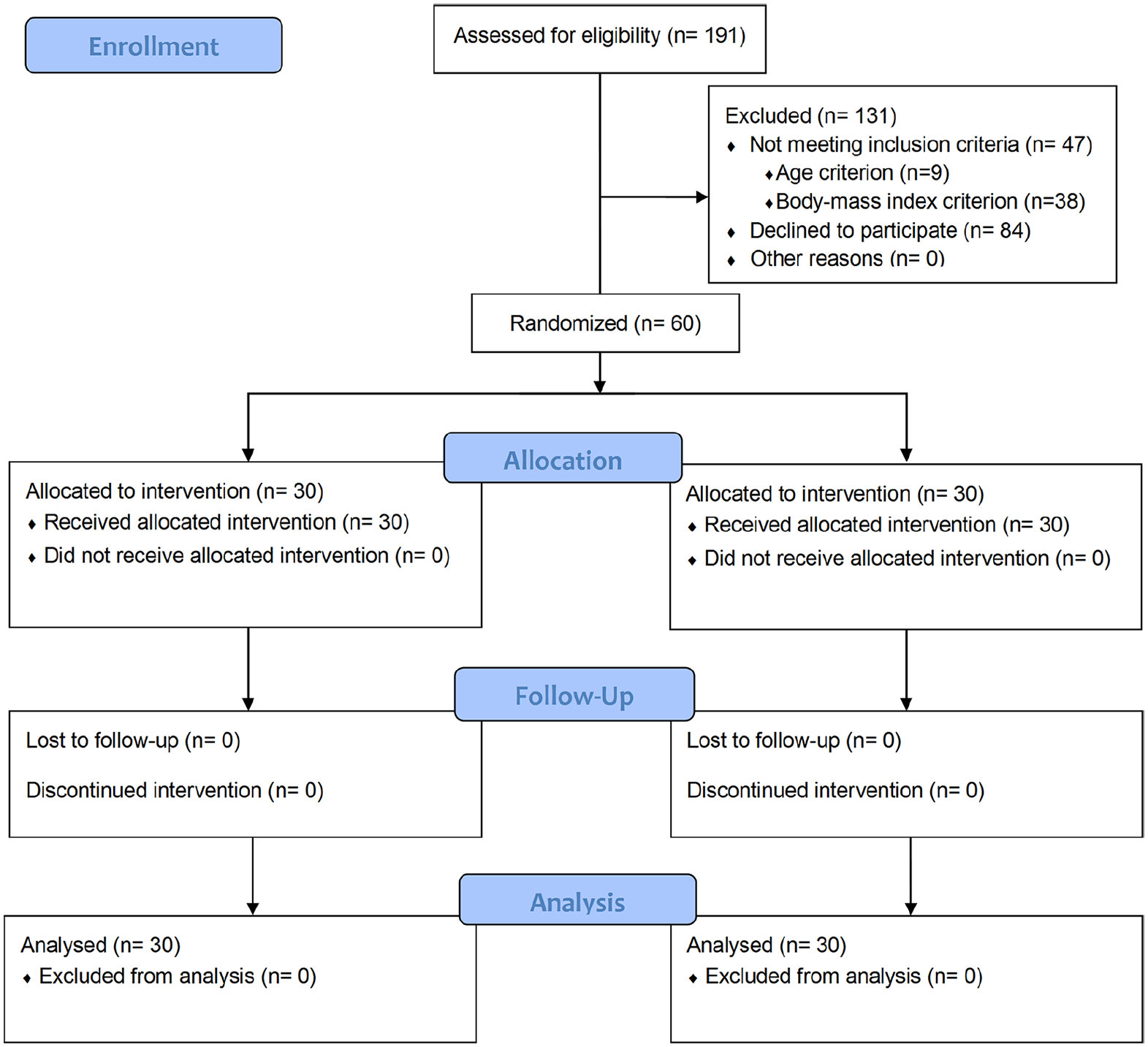
Consolidated Standards of Reporting Trials (CONSORT) flow diagram of enrollment.
Demographics and baseline characteristics.
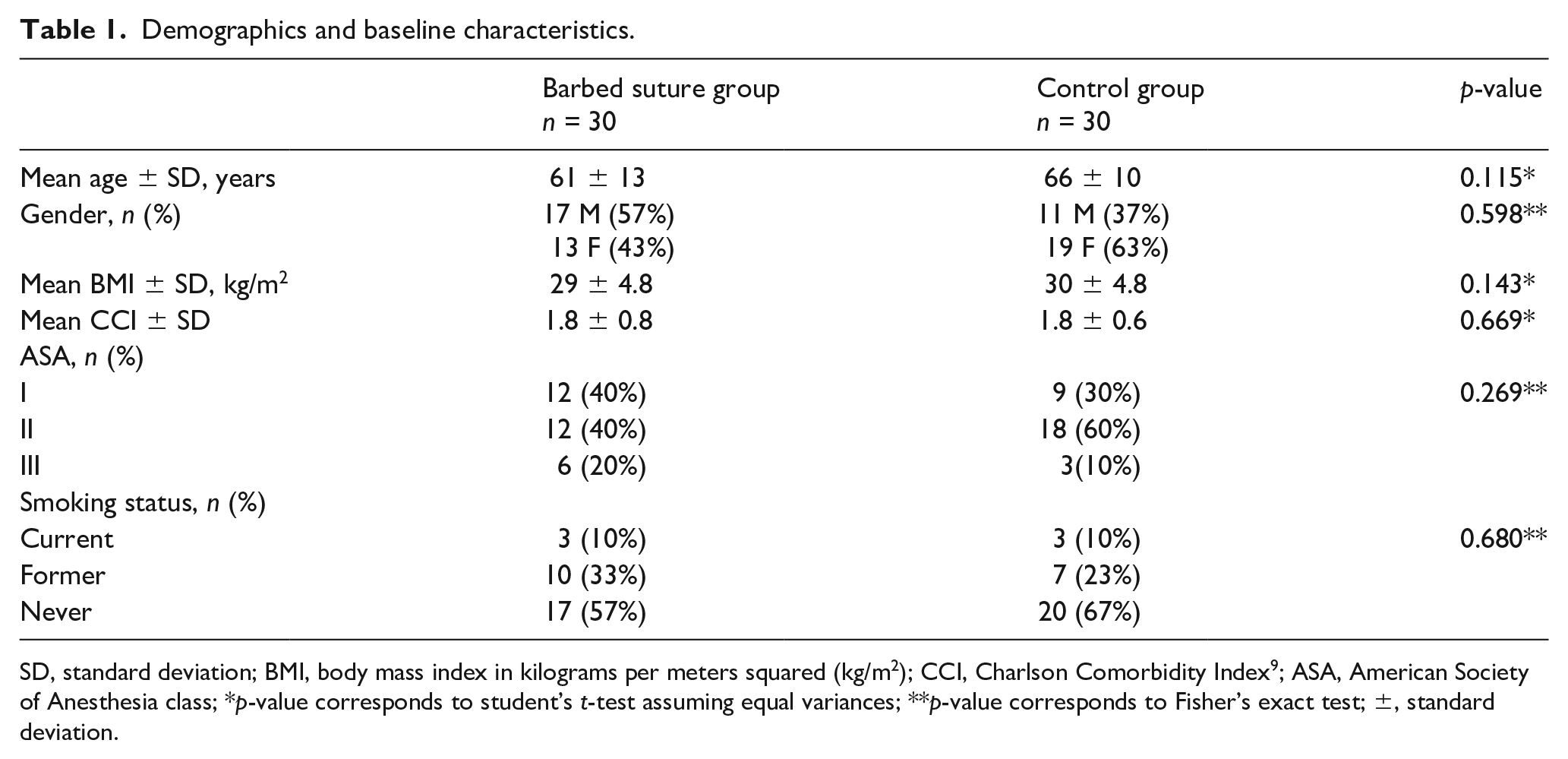
SD, standard deviation; BMI, body mass index in kilograms per meters squared (kg/m2); CCI, Charlson Comorbidity Index 9 ; ASA, American Society of Anesthesia class; *p-value corresponds to student’s t-test assuming equal variances; **p-value corresponds to Fisher’s exact test; ±, standard deviation.
Subject allocation and randomisation
Patients were randomised to receive barbed sutures (barbed suture group) or conventional sutures (control group) in a 1:1 ratio using a computerised randomisation system at the time of consent. Participating surgeons and operating room personnel were notified at the time of surgery. Research personnel, who were blinded to subject allocation, performed outcome assessments at regularly scheduled orthopaedic clinic visits at three weeks and 90 days postoperative.
Research procedures
All operations were performed by 2 adult reconstruction fellowship-trained surgeons who either performed or directly supervised closure. All patients received a posterior approach THA with repair of posterior capsule and short external rotator using polyester suture (Ethibond Excel®, Ethicon Corporation, Somerville, NJ, USA).
Closure was performed in 4 layers (Table 2). For the barbed suture group, closure of the arthrotomy was performed using unidirectional #1 polydioaxanone suture with symmetric barbs (Stratafix® PDS® Plus with Symmetric Barbs, Ethicon Corporation, Somerville, NJ). For the control group, closure of the arthrotomy (deep layer) was achieved using number #1 braided polyglactin 910 absorbable sutures (Vicryl® Ethicon, Johnson & Johnson, Somerville, NJ). The remaining layers were closed in identical fashion in both groups. The subcutaneous layer was then closed with simple interrupted knots using number 2-0 braided polyglactin 910 absorbable sutures (Vicryl®). The subcuticular layer was closed with a 3-0 monofilament suture poliglecarpone 25 (Monocryl™ Ethicon, Johnson & Johnson, Somerville, NJ) followed by adhesive strips (Steri-strips® 3M, Maplewood, MN, USA) followed by surgical dressing (AquaCel ConvaTec, Deeside, UK) that was removed on postoperative day 7.
Suture type for closure by layer.
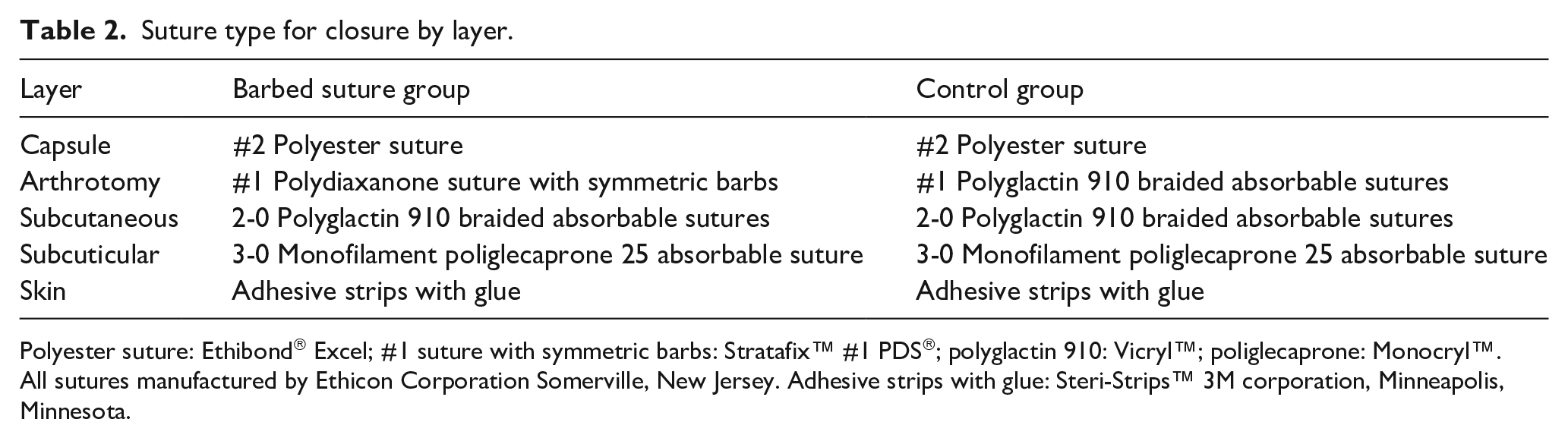
Polyester suture: Ethibond® Excel; #1 suture with symmetric barbs: Stratafix™ #1 PDS®; polyglactin 910: Vicryl™; poliglecaprone: Monocryl™. All sutures manufactured by Ethicon Corporation Somerville, New Jersey. Adhesive strips with glue: Steri-Strips™ 3M corporation, Minneapolis, Minnesota.
Using an electronic timer, research personnel measured closure time in minutes for the arthrotomy layer. Throughout closure, research personnel tracked the number of sutures utilsed. Prior to application of the dressing, surgical staff measured wound length in centimetres.
Outcome measures
Complications were defined according to consensus criteria from Healy et al. 10 Wound complications were defined as any wound-related event that required a reoperation or change in THA perioperative care. Readmission and reoperation were defined as any event related to THA wound condition that required readmission to the hospital or reoperation. Stitch abscess was defined as a collection of purulent fluid in association with the site of a suture. Wound hematoma was defined as a collection of blood contained within normal tissue boundaries that is composed mostly of blood as evidence through wound discharge composed of blood or blood on aspiration. Wound dehiscence was defined as failure of wound closure leading to compromise of anatomic boundaries. Wound discharge was defined as elaboration of fluid from the site of the wound. Superficial wound infections were defined as infections of the superficial surface of the wound with no physical exam findings or clinical progression associated with deep infection or periprosthetic infection. Deep wound infection included sub-dermal infection such as a myofacscial abscess or periprosthetic infection. Periprosthetic infection was defined according to consensus criteria. 11
A secure, electronic database (REDCap, Vanderbilt University, Nashville, TN, USA) was utilised for data collection and storage. Sample size calculations utilsed a power of 0.80 (1-Type II error rate) and an alpha (type I error rate) of 0.05. The predicted duration of arthrotomy closure in the barbed suture group was 9 minutes (standard deviation 1 minute) and the predicted duration of arthrotomy closure in the control group was 8 minutes (standard deviation 1 minute). The minimum sample size based on these parameters was 16 patients in each group and 32 patients in total.
Data analysis
All demographic data were summarised using the mean and range for continuous variables and the absolute number and frequency for categorical variables. The means of the two groups were compared using hypothesis testing. Continuous variables were evaluated for normal distribution using the Shapiro-Wilk test. All variables were normally distributed thus hypothesis testing was conducted using independent t-tests. Categorical variables were assessed using Fisher’s exact test. Closure durations were coded in the database in hours and minutes and assessed as continuous variables using independent t-tests. Wound complications were coded as dichotomous variables and assessed using the Fisher’s exact test. All tests used a p-value < 0.05 as the criterion for statistical significance. All data were analysed using SPSS® statistical software (version 23 for Macintosh, IBM, Armonk, NY, USA).
Results
Arthrotomy closure time was significantly shorter in the barbed suture group (3 minutes ± 9 seconds) versus the control group (8 minutes ± 26 seconds, p < 0.001) (see table 3). The suture utilisation for arthrotomy closure was 1 suture in 28/30 patients (93%) versus 2–4 sutures in 27/30 (90%) in the control group (p < 0.001).
Comparative surgical details and closure times.
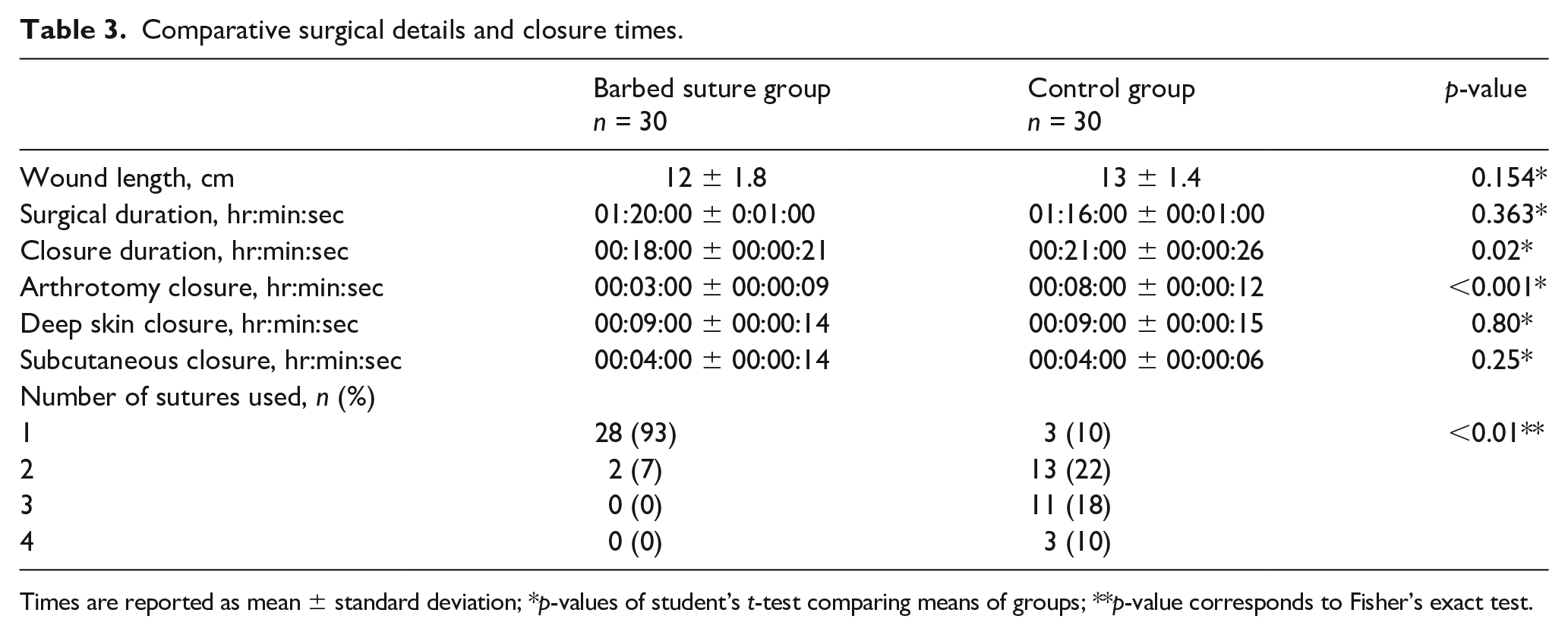
Times are reported as mean ± standard deviation; *p-values of student’s t-test comparing means of groups; **p-value corresponds to Fisher’s exact test.
The overall number of wound-related complications in the barbed suture group was 1/30 (3%) versus 1/30 (3%) in the control group (p = 1.00) (see Table 4). The rate of suture abscesses was 1/30 (3%) in barbed suture group versus zero in the control group (p = 1.00). A 54-year-old man with past medical history significant for diabetes mellitus and atrial fibrillation secondary to haemochromatosis, and active smoking, underwent primary THA for primary osteoarthritis during which he received barbed sutures. During a follow-up visit 3 weeks postoperative, he was noted to have a “dime-sized” area of erythema and induration at the proximal extent of his wound with no discharge, no drainage, and no wound-tract. He was treated empirically with a 1-week course of doxcycyline and his symptoms completely resolved.
Wound-related complications.
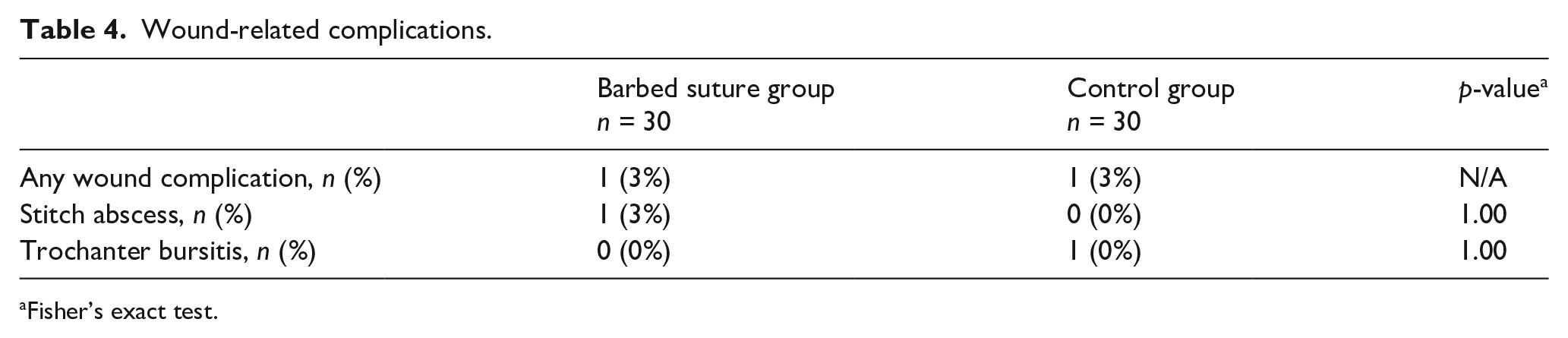
Fisher’s exact test.
There was trochanter bursitis 1/30 (3%) in the control group versus zero in the barbed suture group (p = 1.00). A 61-year-old woman with a past medical history significant for diabetes mellitus underwent primary THA during which she received standard of care sutures for arthrotomy closure. At her 90-day postoperative office, she presented with complaints of pain overlying her trochanter region with no clinical or radiographic signs of infections. Her symptoms and signs were consistent with trochanter bursitis and she was treated with non-steroidal anti-inflammatory medication.
Discussion
Wound infection and other wound related complications may have implications for both the cost and quality of care after elective primary THA.12,13 As the United States healthcare system shifts towards a bundled-payment based reimbursement model, increasing attention and scrutiny have been direct towards potential methods to improve quality of care and reduce costs. 14 Barbed sutures may reduce operative time, costs, and complications associated with THA1,3,15 Prior studies have evaluated the use of barbed sutures for superficial closure after THA.7,8 These studies generally support the use of barbed sutures in superficial closure, but they have been limited by non-random design and their applicability to closure of the arthrotomy is uncertain. The present study is the first randomised, controlled trial to evaluate the use of barbed sutures in the closure of the arthrotomy after THA. The major findings of this study were that patients who received barbed sutures had less than half the arthrotomy closure duration, lower suture utilisation, and an equivalent rate of wound-related complications compared to patients who received standard of care, non-barbed sutures.
Several prior studies comport with the findings of the present report. Thacher et al. 7 concluded that the use of barbed sutures reduced the rate of superficial infection among patients undergoing superficial closure with barbed sutures rather than staples. Knapper et al. 8 found that patients who received barbed sutures for superficial closure had a faster time to developing a dry wound. The THA-specific literature remains relatively sparse. Studies evaluating the use of barbed sutures in closure of either THA or TKA have generally supported the findings in the present study. Borzio et al. 16 conducted a meta-analysis of level-I trials in 2016. Four trials met inclusion criteria for a total of 290 patients randomized to barbed sutures (22 THA patients, 268 TKA) versus 298 patients allocated to standard of care sutures (19 THA patients, 279 TKA patients). The duration of closure with 6 minutes faster in the barbed suture cohort (p < 0.05). The odds of minor complications between the 2 groups was not significantly different (p = 0.95). Similarly, the odds of major complications were not significantly different between the 2 groups (p = 0.27).
Ting et al. 4 conducted a prospective, randomised controlled trial of 65 patients randomised to receive either barbed sutures (14 THA and 17 TKA) for all 3-layers of wound closure versus standard of care sutures (11 THA and 18 TKA) for all three layers of wound closure. The mean duration of closure was significantly (p = 0.0218) faster among THA patients receiving barbed sutures (9.6 minutes, range 5.4–13.6 minutes) compared to standard of care sutures (15 minutes, range 9.5–26.2 minutes. The number of sutures utilised per THA was significantly (p < 0.01) lower among barbed suture group (mean: 2.6 sutures, range 2–4) versus the standard of care group (mean: 6.5 sutures, range 3–10). In this study there was 1 patient in the barbed suture group who developed peri-incisonal erythema treated with oral antibiotics compared to zero in the standard of care group.
Not all studies in the prior literature support these findings. Smith et al. 17 performed a randomised controlled trial of both total hip and knee arthroplasty patients who were randomised to receive either barbed sutures (Quill™ Angiotech Pharmaceuticals Incorporated, Vancouver, Canada) or conventional sutures for all 3 layers of sutures. The report found that closure with barbed sutures was 9.72 minutes (p < 0.05) faster among all 34 patients. The investigators tabulated the rate of complications among patients in this randomised controlled trial. In order to increase the power of their study to detect differences in the rate of complications, they conducted a retrospective chart review of an additional 100 patients. They pooled the results of this review with the results of their randomised controlled trial and conducted a final analysis on 98 patients who received barbed sutures compared to 36 patients who received standard of care sutures. The rate of major complications was not significantly different between the 2 groups (barbed: 2/98, 2% versus standard of care: 0, p = 0.488) nor was the rate of minor complications (barbed: 8/98, 8% versus standard of care: 2/36, 6%, p = 0.45). Although the rate of complications were not significantly different between the 2 groups, the investigators expressed concerns regarding the higher rate of major complications which included a patient with full-thickness skin necrosis of a TKA ultimately requiring an above-the-knee (AK) amputation and another patient who required a 2-stage revision TKA after developing a periprosthetic infection. This study was limited by inadequate power to detect differences in deep infection and unclear reporting of diagnostic parameters fulfilling consensus criteria for periprosthetic infection. 11 Furthermore, the nature of minor complications was not discussed in this study. Other studies have raised concerns regarding the rate of arthrofibrosis and superficial infection following closure with barbed sutures, but these studies have been limited to the TKA literature and their applicability to closure THA is uncertain,18,19 thus, further research is needed.
There are several limitations to this study. All surgeons in this study utilised a posterior approach and the applicability of these findings to wounds created through other approaches is uncertain. Furthermore, the relatively low number of patients in each study group and antibiotic impregnation of the barbed suture pose challenges to making comparison regarding the rate of periprosthetic infection and other rare but clinically significant complications. Although continuous locked suturing techniques with standard sutures are possible, this was not utilised in the comparison group as it was not the standard of care, and there were concerns regarding the potential failure of closure. Finally, a formal cost analysis remained outside the scope of this study for several reasons. Nevertheless, it is important to note that there is a greater cost per unit of barbed suture. Future formal cost analysis studies will be required to assess the overall cost effectiveness of this approach. Despite these limitations, this is one of the few studies to evaluate the utilisation of barbed sutures in arthrotomy closure during total hip arthroplasty and to our knowledge the only prospective, randomised controlled trial.
Overall, this study suggests that utilisation of barbed sutures for arthrotomy closure after THA reduces the duration of arthrotomy closure and suture utilsation without increasing the rate of complications. These early promising results in the clinical setting build upon prior basic science studies which suggest that the use of a single barbed suture may be effective and safe for closure during THA.20–23 Future randomised trials and/or prospective cohorts with larger patient populations may further establish the safety of this method, particularly with regards to infection as an endpoint.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: this study was sponsored by Ethicon Corporation. Outside the submitted work, the authors report:
MAM: reports grants from Ethicon during the conduct of the study. Outside the submitted work, MAM reports personal fees from Cymedica Orthopedics®. MAM reports grants from National Institutes of Health National Institute of Arthritis and Musculoskeletal and Skin Diseases and Eunice Kennedy Shriver National Institute of Child Health and Human Development (NIAMS & NICHD), and Tissuegene, incorporated. MAM reports grants and personal fees from DJ Orthopaedics LLC., Flexion Therapeutics, Ongoing Care Solutions, incorporated, Orthosensor, incorporated, Pacira biosciences, incorporated, Performance Dynamics, LLC., Pfizer, incorporated, Johnson & Johnson, and Stryker corporation. MAM reports other support from Medicus Works, LLC., Peerwell, incorporated, UpToDate®, and Wolters Kluwer Health - Lippincott Williams & Wilkins. MAM has a licensed patent with Microport® and a licensed patent with Stryker Corporation. MAM reports board or committee membership with the American Association of Orthopaedic Surgeons and the American Association of Hip and Knee Surgeons. MAM serves on the editorial or governing board of the Journal of Arthroplasty, Journal of Knee Surgery, Knee Society, Orthopedics, and Surgical Technology International.
VEK: reports grants from Ethicon, incorporated during the conduct of the study. Outside the submitted work, VEK reports personal fees from Stryker Corporation. Also, VEK has a patent with Stryker Corporation with royalties paid and serves as a member of the editorial board or governing board of the Journal of Arthroplasty.
CAH: Outside the submitted work, CAH reports grants from CD Diagnostics, CyMedica Orthopedics, incorporated, Ferring Pharmaceuticals, Orthopedic research and education foundation (OREF), Orthofix, incorporated and Stryker Corporation. CAH reports grants and personal fees from KCI and Zimmer Biomet. CAH reports serving as a committee member of the American Association of Hip and Knee surgeons. CAH reports serving as a board or committee of the American Journal of Orthopedics, Journal of Hip Surgery, Journal of Knee Surgery, American Orthopaedic Association, and Musculoskeletal Infection Society.
RMM: Outside the submitted work, RMM reports grants from Zimmer Biomet and grants and personal fees from Stryker Corporation. RMM reports board or committee member of the American Association of Hip and Knee Surgeons.
NSP: Outside the submitted work, the author discloses board membership in the Orthopaedic Research Society (ORS).
The remaining authors (KS and AKK) report no disclosures.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Ethicon Corporation with an investigator-initiated grant.