
Abstract
Hip abductor tendon tear is a difficult problem to manage. The hip abductor mechanism is made up of the gluteus medius and minimus muscles, both of which contribute to stabilising the pelvis through the gait cycle. Tears of these tendons are likely due to iatrogenic injury during arthroplasty and chronic degenerative tendinopathy. Ultrasound and magnetic resonance imaging have provided limited clues regarding the pattern of disease and further work is required to clarify both the macro and microscopic pattern of disease. While surgery has been attempted over the last 2 decades, the outcomes are variable and the lack of high-quality studies have limited the uptake of surgical repair. Hip abductor tendon tears share many features with rotator cuff tears, hence, innovations in surgical techniques, materials and biologics may apply to both pathologies.
Introduction
The gluteus medius and minimus muscles are often referred to as the hip abductors. They are crucial in maintaining pelvic stability and are essential for normal gait.1 –3 Tears of these tendons are increasingly recognised as a cause for chronic hip dysfunction and pain, particularly in older adults.4 –7 Intraoperative observations, population studies and imaging studies have demonstrated that both complete and partial abductor tendon tears are found in up to 20% of those over the age of 50.5,8 –11
Hip abductor tendon tears are often divided into 3 groups. The first group consist of patients with chronic tears without previous surgery to the hip, the second group are patients with incidental tears discovered at the time of hip surgery, and the third consist of patients who present with tears following hip arthroplasty.7,12,13 Similar to rotator cuff and Achilles tendon diseases, tears in groups 1 and 2 are likely the result of degenerative tendinopathy, while the aetiology of group 3 likely involves both tendinopathy and injury from the surgical approach.14,15 Regardless of cause, patients with hip abductor tears often experience lateral hip pain and gait instability. Group 3 patients also have a higher risk of hip dislocation.16 –20 These symptoms severely reduce the quality of life for patients and often deprives them of their independence. 21
Hip abductor tear is a difficult problem to manage.7,16,19,22 Non-surgical options are often ineffective for patients with severe tendinopathy and tears.13,22 Furthermore, the torn muscle tendon unit degenerates in the absence of load and retracts from the bone, making surgical repair difficult.7,17,23 While direct repair has been attempted for smaller, minimally retracted tears, large full thickness tears often require allograft reconstruction or tendon transfers from adjacent muscles.7,22,24,25 As such, many surgeons are reluctant to offer surgery. With an ageing population and an almost 200% increase in the number of hip replacements performed in the last decade, there is an urgency to improve both the knowledge and treatment for hip abductor tendon tears. 26
This review aims to summarise the known anatomy, pathology and management of abductor tendon tears. Understanding these key features of disease is required for identifying promising areas of research that can improve patient outcomes.
Anatomy
Hip abductor tears involve the tendons of the gluteus medius and gluteus minimus muscles, both of which originate from the external surface of the ilium. 27 Gluteus medius can be divided functionally and anatomically into 3 parts; the anterior, middle and posterior compartments.27,28 The anterior compartment is the largest. Its tendon starts at the apex of the greater trochanter (GT) and measures approximately 3 cm in length, inserting into the lateral facet of the GT. 29 The muscle fibres from the middle and posterior compartments merge into a thin, cord-like tendon above the apex of the GT, inserting distally into the superoposterior facet of the GT (Figure 1).2,29 Gluteus minimus is approximately ¼ the size of gluteus medius.30,31 Its tendon inserts into the anterior facet of the GT, a portion of its deep fibres also directly insert into the hip capsule.27,30,31 Anteriorly, the tendons of gluteus medius and minimus are closely opposed and are often fused, forming the “conjoint tendon” of the hip.1,8,27
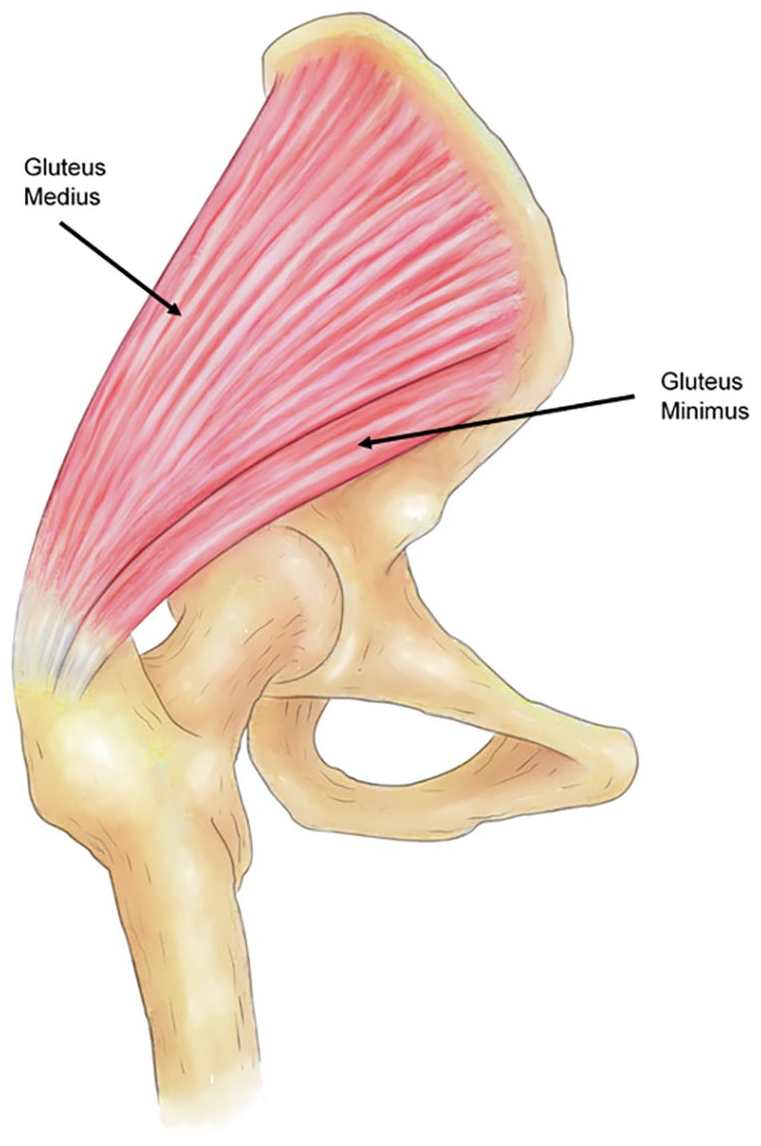
Gluteus medius and minimus (underneath) inserting into the greater trochanter.
The blood supply of both the gluteus medius and minimus are from the superior gluteal artery and its branches. 32 This artery is in close approximation to the superior gluteal nerve, together, they form a neurovascular bundle between the gluteus medius and minimus. 33 The artery and nerve are at risk of injury during lateral approaches to the hip, and this may contribute to hip abductor tendon failure postoperatively.12,33,34 Interestingly, the superior gluteal artery sends branches into the trochanter through the insertion of gluteus medius and minimus, making it an important supplier to the muscle, tendon and the trochanter.32,35 The branches of the superior gluteal artery supplying the gluteus minimus also contribute to the supply of the hip capsule and the acetabular region.32,35,36
Anatomical and electromyograph studies have clarified the role of both gluteus medius and minimus in gait. Gluteus medius initiates abduction; its 3 compartments fire sequentially during gait and act as the chief stabilisers of the pelvis through the gait cycle.2,3 It is also an external rotator of the femur at the hip joint. 27 Gluteus minimus acts synergistically with gluteus medius to stabilise the hip joint by pulling the femoral head into the acetabulum.3,11,30 The gluteus minimus is also an internal rotator at the hip joint and has a role in pulling the capsule free during abduction, preventing impingement.2,37 These functions are very similar to the rotator cuff muscles of the shoulder. Because of this, abductor tendon tears have been referred to as the “rotator cuff” tears of the hip.8,38
Pathogenesis
The pathogenesis of hip abductor tendon tears is multifactorial. Group 3 tears (following THA) can often be attributed to dissection injury to the tendon, muscle and neurovascular bundle during lateral approaches to the hip and/or failure of the tendon repair to heal.12,33 While a small number of patients in groups 1 and 2 can recall a traumatic injury leading up to pain and dysfunction, most experience insidious and chronic onset of symptoms consistent with the development of tendinopathy.39,40 Tendinopathy is a widely used term to describe chronic pain and degeneration of tendons, it results in the progressive loss of structural organisation and functional strength of the tendon, eventually leading to tendon tears.39,41 The development of tendinopathy and tear in hip abductor tendons can be attributed to both extrinsic and intrinsic factors.
Extrinsically, both the lateral and posterior approaches to the hip are associated with hip abductor tears, likely due to intraoperative injury to the tendon and to its neurovascular supply.11,16,42 Mechanical stress of the hip abductor tendons may also predispose them to degeneration and failure.43 –46 Tendons naturally undergo cycles of loading, however, they respond poorly to compression and tension at supra-physiological levels, leading to catabolism and eventual failure. 47 This combination of tension and compression, often by an adjacent structure, produces friction and shear which may lead to tendinopathy.18,48,49 The compression of the gluteus medius and minimus tendons by the iliotibial band has been identified as a probable cause, especially in females with decreased femoral neck angles. 18 Another potential mechanism involves the unique loads experienced by the deep fibres of the hip abductor tendons. These fibres are shielded from tensile forces by more superficial fibres, yet experience increased compressive loads, especially at low angles of hip abduction.50,51 Such compressive loads are frequently present, as the gluteus medius and minimus are active stabilisers at low angles of hip abduction.18,52 This theory is supported by intraoperative findings, where tears are often found to originate from the deep surface of the tendons. 53 A similar process can be observed in the rotator cuff, where tendon tears predominantly originate from the articular (deep) surface of the tendon.48,54
Several intrinsic risk factors have been associated with tendinopathy and are likely involved in the development of abductor tendinopathy and tear. Recent systematic reviews have confirmed diabetes and hypercholesterolemia as risk factors of tendinopathy, possibly due to their roles in chronic inflammation and microvascular injury.55,56 Advancing age is associated with changes in both cell and matrix metabolism, leading to the development of tendinopathy by decreasing the tendon’s ability to adapt to mechanical loading.57 –60 Rheumatological diseases such as rheumatoid arthritis and gout have also been linked to the development of tendinopathy. 61 This is likely mediated through chronic inflammation involving both the tendon and enthesis. 62
Although a key feature in advanced tendinopathy is vascular infiltration, vascular insufficiency is an important intrinsic risk factor in the development of abductor tendinopathy. Immunohistochemistry studies utilising vessel markers have identified regions of hypo-vascularity in the central portion of the tendon. 63 This becomes more pronounced with age and may be key driver of tendinopathy. 64 A similar pattern has been observed in the rotator cuff, where a “critical zone” of decreased vascularity in the supraspinatus tendon is predisposed to injury and degeneration.65,66 However, it must be noted that the blood supply of the gluteus medius and minimus tendons differ from tendons of the rotator cuff. The superior gluteal artery sends branches through the tendons to reach the bony insertions of both muscles on the greater trochanter.35,36 This contrasts with the rotator cuff, where the tendon is supplied by anastomoses of muscular and bony vessels.65,67 Furthermore, current studies of the vascularity of the abductor tendons rely on ex-vivo methods, and this may not be reflective of blood flow in life. 68 Recent in vivo studies have better characterised regions of hypovascularity in the rotator cuff, similar studies of the hip abductors will clarify the role of vascularity in the development of tendinopathy and tears.69,70
The failure of the tendon to adapt and heal from both extrinsic and intrinsic factors leads to the development of tendinopathy. 71 Here, the microstructure of the tendon is damaged and maladaptive changes are seen in both cells and extracellular matrix.41,43,47 In tendinopathy, collagen III and proteoglycan content are increased and disorganisation of collagen fibres becomes evident.72,73 Other features include abnormal rounding of nuclei, increased irregularity in cell distribution, decreased collagen stainability and increased vascularity.15,74,75 Macroscopically, a decline in the stiffness and energy storing ability of the tendon is observed.76,77 This further predisposes the tendon to injury, eventually leading to tendon tears. 78 These tendinopathic changes are observed in rotator cuff, patella tendon and Achilles tendon tears, limited reports have also demonstrated similar changes in hip abductor tendon tears.4,14,15,79
An important mediator of these observed degenerative changes is inflammation. Tendinopathy was thought to occur without the influence of inflammatory pathways, largely due to the lack of inflammatory cells seen in the early studies. 80 More recent studies have noted the presence of inflammation in both the tendon and the bone tendon junction (enthesis) in various stages of tendinopathy.81,82 In both human and animal studies, macrophages, T cells, and mast cells are present in greater numbers in tendinopathic tendons.81 –83 Furthermore, the enthesis contains resident T cells that become activated following abnormal mechanical strain, implicating T cells in the development of tendinopathy. 84 Tendon injury and early tendinopathy are also associated with upregulation of many important signalling molecules including IL-1, TNF-α, IL-15, IL-17, IL-18 and IL-21.81,82,85 These pro-inflammatory cytokines induce production of enzymes of the MMP family,86,87 reduce the production of collagen 1 by tenocytes, promote tenocyte apoptosis and upregulate a host of secondary inflammatory mediators such as PGE2, Substance P and COX-2.88 –90 Other cytokines such as IL-6 can deliver both pro and anti-inflammatory effects, and the loss of their regulatory function may be important in the development of tendinopathy.90,91 Current evidence suggests there are complex interactions between immune cells, tenocytes and cytokines. Imbalance in this network provides the cellular and molecular basis for the degenerative changes observed in tendinopathy.41,82,92 Influencing inflammatory pathways is key to both preventing tendon tears and improve the quality of healing following surgery. 43 Improved understanding of the roles of specific cell types and inflammatory molecules, as well as their interactions will provide future prognostic markers and therapeutic targets.43,61,81
Pathological features of abductor tendon tears
A clear understanding of the micro and macroscopic patterns of disease is required for effective treatment planning and identifying promising future areas of research. Microscopically, only 2 studies have reported on the histological features of abductor tendon tears. Fearon et al. 4 examined small biopsies from patients undergoing repair for symptomatic tears. 4 While the pathology was reported to be “degeneration”, no other details were available. Connell et al. 93 obtained 5 biopsies, again from patients undergoing abductor repair surgery. These samples demonstrated collagen degeneration, fibroblastic and vascular proliferation and dystrophic calcification, all features associated with tendinopathy. Due to the limited size of the clinical samples, these studies could not identify whether the changes were seen in the deep or the superficial layers of the tendon. Imaging of the enthesis was also not possible.
While the microscopic features of disease are limited, ultrasound (US) and magnetic resonance imaging (MRI) studies have provided insight into the macroscopic features of abductor tendinopathy and tear. Ultrasound allows direct imaging of sites of pain and can be used to guide therapeutic injections.94 –96 The gluteus medius and minimus tendons appear hypoechoic on ultrasound in tendinopathy and are typically enlarged (Figure 2(a) and (b)).97,98 Full thickness tears are typically found near the insertion of the tendon to bone, while partial tears have been described on both the superficial and deep surfaces of the tendon.95,98 Other pathological features identified on ultrasound include bony erosions at the tendon insertions, intra-tendinous calcifications and associated fluid accumulation in the trochanteric bursa.98,99 Tears involving the anterior and posterior gluteus medius tendon, gluteus minimus tendon and both have been described. However, there is no agreement on the predominant pattern of disease.42,94
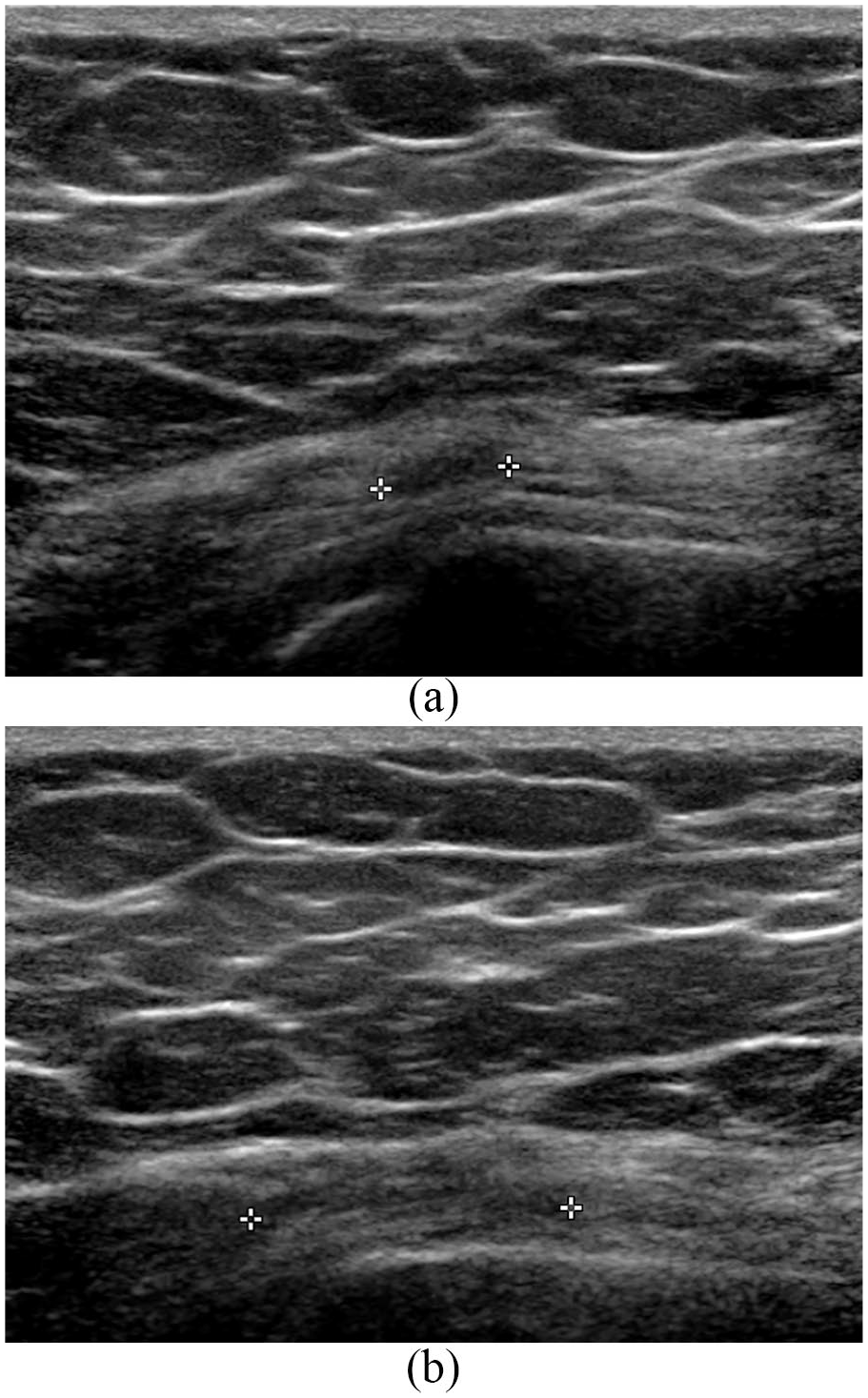
(a) and (b) Longitudinal ultrasound views of the gluteus medius tendon in a 67-year-old female with left gluteus medius tendinopathy, note the hypoechoic regions between the white crosses, a typical feature of tendinopathy on ultrasound.
The accuracy of ultrasound has been compared to intraoperative findings in 2 studies. In 37 patients, Connell found that ultrasound correctly identified all but 2 cases of tendinopathy and 1 case of partial tendon tear. 98 Fearon reported a sensitivity of 0.79 and positive predictive value of 1 for identifying tears in either tendon. 4 However, ultrasound was unable to identify gluteus minimus tears when a concurrent gluteus medius tear was present.
MRI is the most extensively used modality to investigate abductor tendinopathy and tears. 96 Pathological features in tendinopathy include adjacent soft tissue oedema signifying peritendonitis, thickening of the tendon and increased signal intensity from the tendon on T2 weighted images (Figure 3(a) and (b)). Partial thickness tears can appear as longitudinal fissures where complete tears are diagnosed when a “bald” trochanteric facet is visualised (Figure 4(a) and (b)).99,100 The majority of studies found tears in the anterior portion of the gluteus medius tendon. While the bone-tendon junction has not been specifically examined in any MRI studies, Lequesne et al. 101 reported that all identified tears in their series involved the distal tendon at or near its insertion.
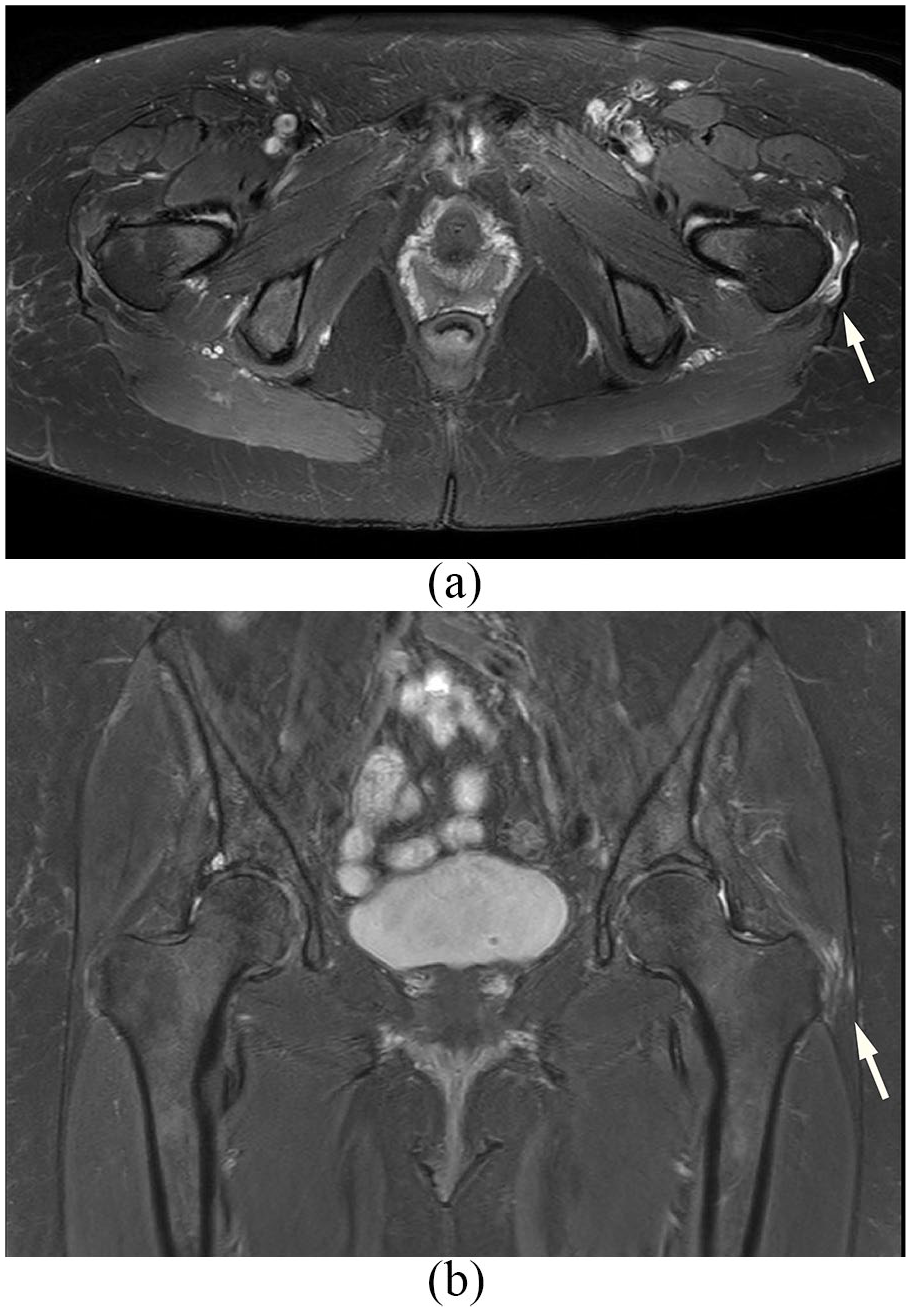
(a) and (b) Axial and coronal T2 MRI images of a 67-year-old female patient with partial tear of her left gluteus medius and minimus. Note the increased peritrochanteric signal and mild oedema in the surrounding tissue (white arrows).
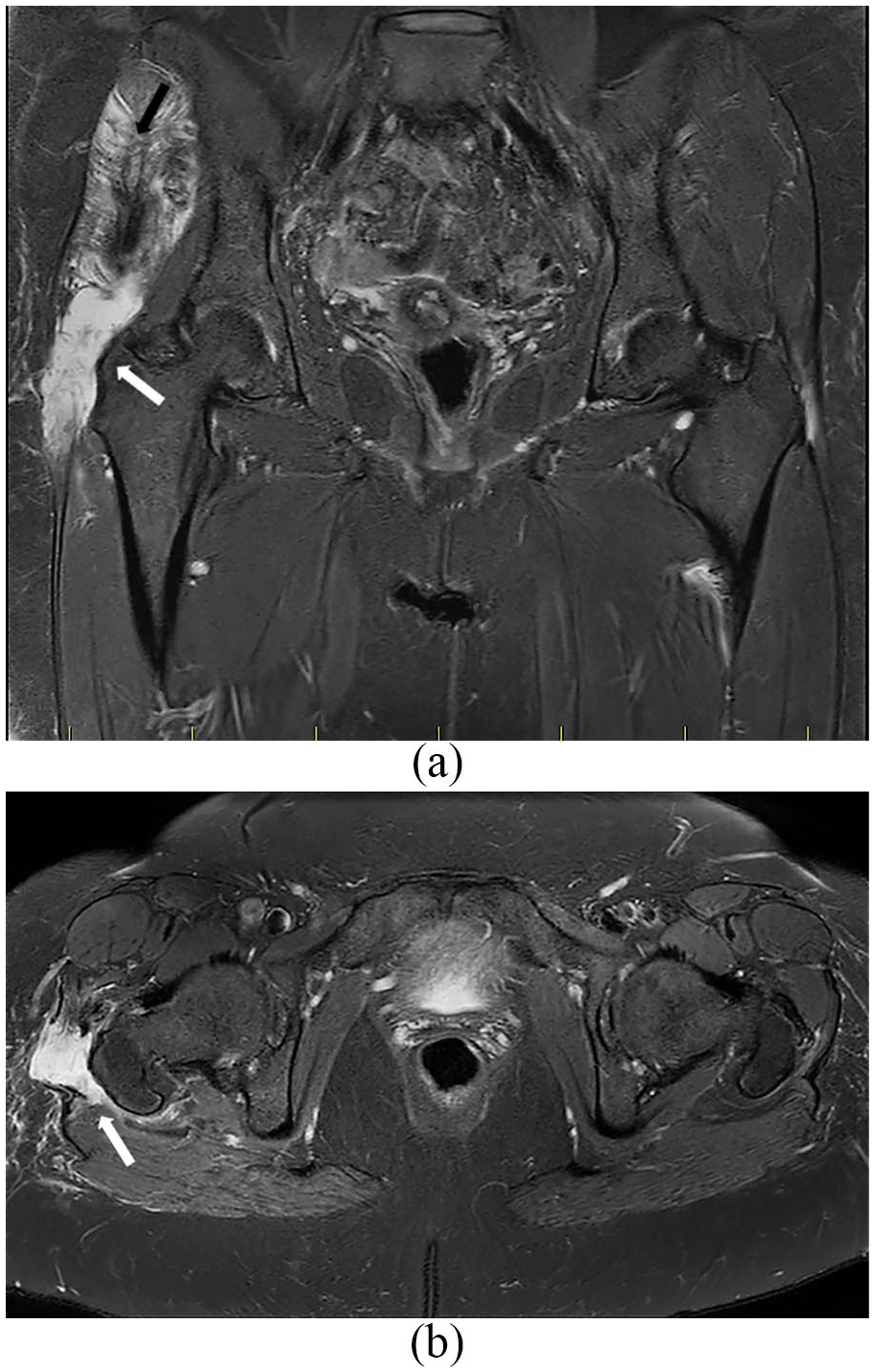
(a) and (b) Coronal and axial T2 MRI images of a 70-year-old female patient with complete tear of her right gluteus medius and minimus. Note the fatty atrophy in both muscles (black arrow) and increased signal intensity in the peritrochanteric region indicative of a complete tear (white arrows).
There are concerns regarding the accuracy of these MRI findings. Blakenbaker et al. 102 examined 131 consecutive hip MRIs and found peritrochanteric abnormalities in 50% of asymptomatic patients. 7 studies have correlated MRI findings with intraoperative findings. A review of 5 in 2015 reported a sensitivity of 33–100% and specificity of 92–100% when MRI was used to diagnose tears. Since then, Lindner et al. 39 found MRI missed 20 of the 47 tears identified intraoperatively. This finding was echoed by Makridis et al. 103 ; in 70 of patients undergoing abductor repair, 94% were found to have a tear in the anterior gluteus medius tendon and 33% had a concomitant gluteus minimus tear intraoperatively. Only 40% of these tears were identified on preoperative MRI. 103
In summary, ultrasound and MRI have provided useful information on the macroscopic features of abductor tendon tears. The concerns regarding their accuracy highlights the need for careful intraoperative examination during surgery. In particular, the incidence of gluteus minimus tears found intraoperatively are often higher than reported by imaging studies.
Surgical treatment
For the majority of patients with complete abductor tendon tears and severe symptoms, conservative management is often unsuccessful.13,22,104 Surgical repair was first described by Bunker et al. 8 and Kagan et al. 38 in the 1990s for patients with incidental tears found during surgery for neck of femur fractures. Since then, repair has been attempted in patients both with and without a history of ipsilateral total hip arthroplasty (THA).
Repairs in primary tears
Most studies have focused on patients with no prior history of THA, with both open and arthroscopic repairs attempted. In the largest study to date, Ebert et al. 105 reported on 112 patients with primary gluteus medius tears who underwent open repair augmented with a LARS ligament through intraosseous tunnels. Both complete and partial tears were treated, no further pathological details were available. The author reported excellent improvements in self-reported functional scores, range of motion and mobility as measured by a 6-minute walking test. Only 3 re-tears occurred within a 12 months follow-up period. Walsh et al. 106 performed open repair utilising intraosseous tunnels in 72 patients. Most tears were partial thickness and found predominantly on the under surface of the tendon. While most tears involved the gluteus medius, severe tears involved both the gluteus medius and minimus and caused exposure of the underlying trochanter (Figure 5). Overall, patients reported significant improvements in functional scores post-operatively with 4 re-tears at 6 weeks postoperatively. With 22 patients, Davies et al. 107 reported functional improvements in 19 patients at an average follow-up of 70.8 months after open repair of the gluteus medius and minimus tendons. All patients had MRI confirmed pathology without muscle atrophy pre-operatively. 2 re-tears were reported. In all 3 studies, the extent and size of the tears, as well as the presence of muscle atrophy and tendon retraction were incompletely described. Despite this, the excellent functional outcomes following open repair of primary tears are encouraging.

Intraoperative view of a complete tear through both the gluteus medius and minimus. Note the bald trochanteric facet visible (arrow). The tear extends further superiorly on the under surface of the tendon.
Endoscopic repair of primary tears was first described by Voos et al. 108 using suture anchors. Domb et al. 53 described transtendinous repair for partial thickness gluteus medius tears in 15 patients. In this study, defects on the under-surface of the gluteus medius tendon were found and repaired after incising the tendon longitudinally. No complications were reported in these studies, pain and functional scores were significantly improved at a minimum of 12 months follow-up. McCormick et al. 109 reported on repair of complete tears of the gluteus medius and minimus in 10 patients. All reported fair to excellent functional outcomes at an average of 2 years postoperatively. 109 More recently, Byrd and Jones 110 reported positive functional outcomes at 24 months postoperatively in 12 relatively young patients (average age 54 years) with gluteus medius tears. When comparing endoscopic and open repairs for primary abductor tendon repairs, a recent systematic analysis concluded that both produce good functional results with fewer complications in the endoscopic group. 111 However, endoscopic repair is difficult to perform if significant retraction of the tendon is present. It is also not recommended for tears where muscle atrophy is present on MRI. 112
Repairs in tears following THA
For patients presenting with an abductor tendon tear following THA, treatment is guided by the extent of soft tissue loss. Open repair has been attempted using direct repair of the tendon and trans-osseous fixation. The results are inferior in this group of patients compared to primary repairs, most likely secondary to the larger size of tears present and increased degeneration and retraction of the tendon. Weber and Berry 16 reported functional improvements in only 5 out of 9 patients with 3 “complete failures”, Lübbeke et al. 113 found that only half of the 18 patients with complete follow-up had an improvement in pain and function following direct repair of the abductor complex. Miozarri et al. 114 reported 4 re-tears in 12 cases followed with postoperative MRIs. Furthermore, while the functional and pain scores improved significantly in patient with intact repairs, the fatty atrophy of gluteus medius and minimus was not reversed.
Muscle transfers have been reported in treating large tears following hip arthroplasty, especially if the trochanter bone stock is poor. 7 Kohl et al. 115 advanced vastus lateralis to bridge defects in the abductor tendon mechanism in 11 patients. They found favourable pain and functional outcomes at 2 years. Whiteside 13 described transferring the anterior portion of gluteus maximus in 11 patients; at 16 months post-op, all but 2 patients walked without a limp. 13 The same author has supplemented this technique with an additional transfer of tensor fascia lata, 14 of 16 patients experienced an improvement in their abductor function after 1 year. 25 While effective, muscle transfer is a significant undertaking with a high rate of complications. 115 It has been used only in patients with significant tissue loss and intractable symptoms. 19
An alternative to muscle transfers involve using bone-tendon allografts blocks. While they prevent the de-functioning of another muscle, the long-term integrity of the construct is unclear. 116 Fehm et al. 117 used an Achilles bone-tendon allograft block to treat patients with massive abductor tears. 6 of 7 patients achieved improvements in pain and function outcomes at 2 years. Drexler et al. 118 used patella allografts with its attached quadriceps and patella tendons. At 33 months post-operatively, 7 of 11 patients reported no pain and above “fair” functional outcomes. 2 proximal re-tears were seen on MRI. The authors suggested that this technique can be used with significantly retracted tears and prevents the morbidity associated with the transfer of large muscles.
Both muscles transfers and allograft tendons require extensive exposure and dissection and are associated with high rates of complications.115,119 Both synthetic and extracellular matrix-based patches have been used as overlay reinforcement for rotator cuff repairs, similar products have also found use for hip abductor repairs. Synthetic patches have excellent material properties; however, there are concerns regarding long term tissue integration and chronic immune reactions.120,121 Bajwa et al. 122 retrospectively reviewed 24 cases of LARS ligament augmented repairs. Overall, they reported 2 failures and significant improvements in functional outcomes at a mean follow-up of 108.5 weeks. Caviglia et al. 123 used a Prolene mesh to repair 46 abductor tendon deficits in patients undergoing concurrent revision for implant loosening following THA. Interestingly, the mesh was not secured to the trochanter but to the vastus lateralis muscle. They reported significant improvement in functional scores, but no details of follow-up were given. Extracellular matrixes are derived from animal or human cadaveric sources, a number of these are commercialised for rotator cuff repairs and have seen use also in hip abductor tendon tears. Rao et al. 24 used Graftjacket, a decellularised human dermal extra cellular matrix patch to overlay repairs and reported favourable outcomes in 12 patients. Most recently, Fink and Braun 119 reported augmenting transosseous fixation using a non-reabsorable collagen patch derived from porcine dermal matrix in 30 patients. The majority of patients in this study presented with advanced tears on MRI with more than 50% fatty infiltration of the gluteus medius and minimus. Only 1 re-rupture was reported at an average follow-up of 47 months. Furthermore, the authors observed dramatic improvements seen in both pain and function as measured by the Harris Hip Score in their cohort. 119 To date, this is the most promising study utilising patches.
All studies quoted above are level IV case series. Furthermore, the majority of studies did not perform postoperative imaging to objectively confirm repair integrity at follow-up. Overall, there is good evidence for the efficacy of both open and endoscopic repairs for patients with primary tears (without a prior history of THA). In patients with tears following THA, significant tissue loss is often the limiting factor to repairs. 19 Direct repairs have a high failure rate due to the degenerative nature of torn and retracted tendons; while current tendon patches do not necessarily address the lack of biological healing that may eventually lead to re-tear. Lastly, allograft and muscle transfers remain reserved for selected cases due to the demanding nature of the procedures.
Future directions
The healing of tendon following surgical repair needs to be improved to achieve better clinical outcomes for patients. While there is a lack of data on the quality of healing following abductor tendon repair, studies on rotator cuff repairs have highlighted that simple suture/anchor repair is often insufficient. 124 To this end, a large number of studies have examined the role of growth factors, patches and stem cells in promoting tendon healing following surgical repair, predominantly in rotator cuff tears. These findings should prove transferrable to the repair of abductor tendon tears.
Growth factors and PrP
Growth factors are highly versatile, they can be delivered locally by direct injection and incorporation into slow release matrices and sutures.125,126 Systemic applications have also been trialled.127,128 Overall, the goal of growth factors is to biologically augment the healing that occurs at both the tendon and bone-tendon junction (enthesis), leading to a stronger repair. 128 A number of growth factors and cell signalling molecules have been studied using in-vivo animal models, these include VEGF (vascular endothelial growth factor), IGF1 (insulin like growth factor 1), FGF (fibroblast growth factor), TGF-B (transforming growth factor Beta) isoforms, BMP (bone morphogenic protein), PDGF (platelet derived growth factor) and parathyroid hormone.129 –135 So far, single growth factor studies have not been able to demonstrate significant improvements in the quality of healing or the strength of repair. 128 Furthermore, no growth factors have reached clinical trials for tendon repair. 136
PrP (platelet rich plasma) has also been studied as it contains a variety of growth factors (such as TGF, VEGF, IGF1, PDGF) that can modify the healing response. 137 A comprehensive review of its use in tendon injuries was recently published. 138 While numerous clinical trials have evaluated the use of PrP as an adjuvant for tendon repair, its effectiveness remains unclear, with 5 metanalysis in disagreement regarding its benefits for quality of healing and patient reported outcomes following arthroscopic rotator cuff repairs.137,139 –143 This is not surprising due to the lack of standardisation in PrP preparation and extraction, leading to different growth factor concentrations and release profiles. 144 Overall however, 3 of these studies agreed that PrP improves the quality of healing small to medium sized rotator cuff tears, especially if the preparation is delivered to the bone tendon junction (enthesis).140,142,143,145
The effectiveness of PrP may stem from the fact that it contains a combination of growth factors, rather than individual factors. 140 Growth factors are expressed in combination in native tissue and often have synergistic effects on their targets. With the goal of improving healing in both the tendon and the tendon bone junction, it is likely that more than 1 growth factor is required.120,124,146,147 What is currently unknown is how growth factors interact and how timing of administration can influence the desired outcome. 148 More carefully designed translational research is needed to clarify this interaction and may provide insight into how growth factors and PrP should be used to augment tendon repairs. These therapies should prove effective for both hip abductor and rotator cuff tendons given similarities in their enthesis structure.
Patches
Patches for tendon repair have also been extensively researched in recent years. The ideal tendon patch needs to have similar biomechanical properties to normal tendon and incorporate into the biological environment and guide the regeneration of the native tendon tissue.120,149 Mechanically, current commercial patches are unable to achieve the combination of strength and elasticity seen in rotator cuff tendons. 150 Furthermore, cycles of loading have been shown to adversely affect the mechanical properties of manufactured patches, leading to elongation of loss of effectiveness.151,152 Biologically, there is limited evidence that tendon in-growth into patches is achievable.153,154 Overall, despite the interest and investment in this area, patches have not been shown to be effective at enhancing outcomes following the surgical repair of tendons in Level I and II studies.155 –157 Future use of patches will be dependent on whether new products can be adapted to the larger loads required for hip abductor repairs, and whether they are able to improve the quality of healing of the native tissue. 158
Lastly, the use of stem cells have been explored in tendon repair, with their effects mediated through the release of cytokines and growth factors.120,124,149 This topic has been well summarised in a recent review article. 159 While pluripotent, embryonic stem cells (ESC) have been studied in animal models, ethical considerations and oncogenic potential have severely limited their utility for tendon repairs.159 –161 By far, the most utilised stem cells in tendon related applications are adult mesenchymal cells.120,124,160 These are commonly derived from fat, bone marrow and amnion-related tissue. Animal studies utilising MSCs, especially in the repair of rotator cuffs have yielded positive results.162–164 This has led to a number of clinical studies utilising MSCs, particularly from the bone marrow to enhance tendon to bone repair in the rotator cuff.20,165 –169 These studies have only demonstrated limited improvements in patient outcomes, with key concerns being the viability and dispersal of MSCs, and the number of cells delivered.120,124,170,171 Given similarities between rotator cuff and hip abductors and the larger repair area required in the hip, these issues also need to be resolved for hip abductor tendon repairs.
Overall, the application of growth factors, patches and stem cells in abductor tendon repairs will likely follow their use in rotator cuff tendon tears given the greater market available for rotator cuff tendon repairs. However, these therapies all must be specifically tailored to fit the surgical workflow and mechanical requirements of abductor tendon repairs. Recently, there has been an emphasis on improving pre-clinical models to ensure greater relevance and translation into clinical use. 172 The relative lack of well designed, randomised controlled trials with standardised outcome measures is also another hurdle to clinical uptake in both the rotator cuff and hip abductor tendon. 173
Conclusion
Abductor tendon tendinopathy is gaining recognition as a significant clinical problem in those over the age of 50 years. The microscopic features of disease and the underlying pathological processes are not well described. Surgical repair is difficult and there is a need to explore novel materials and biologics to improve both the scope and results of repair.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors would like to acknowledge the Health Research Council of New Zealand (Grant number 3714609) for funding the salary of MZ.