
Abstract
Background:
Failed reconstruction in cases of severe acetabular bone loss, with or without pelvic discontinuity, in revision total hip arthroplasty (rTHA) remains a great challenge in orthopaedic surgery. The aim of this study was to describe the outcome of a “second” rTHA with “custom-made acetabular components (CMACs)” after a previously failed reconstruction with CMACs.
Methods:
4 patients with severe acetabular bone loss (Paprosky Type IIIB), who required a second rTHA after a previously failed reconstruction with CMAC, due to prosthetic joint infection (PJI), were included in our retrospective study. All prostheses had been constructed on the basis of thin-layer computed-tomography scans of the pelvis. The second rTHA was considered unsuccessful in the event of PJI or aseptic loosening (AL) with need for renewed CMAC explantation.
Results:
The treatment success rate after second rTHA with a CMAC was 50% (2 of 4). In the successful cases, the visual analogue scale (VAS) score and Harris Hip Score (HHS) after the second rTHA (VAS range 2–4; HHS range 45–58 points) did not differ from those after the first rTHA, before onset of symptoms (VAS: range 2–4; HHS: range 47–55 points). In the failed cases, the second CMACs needed to be explanted due to PJI, with renewed detection of previous pathogens. Patients with treatment failure of the second CMAC had required a higher number of revision surgeries after explantation of the first CMAC than patients with a successful outcome.
Conclusions:
In patients with severe acetabular bone loss and previously failed rTHA with CMACs, repeat rTHA with a CMAC may be a solid treatment option for patients with an “uncomplicated” multi-stage procedure, i.e., without persisting infection after explantation of the original CMAC. While the outcome in terms of clinical function does not appear negatively affected by such a “second attempt,” the complication rate and risk of reinfection, nonetheless, is high.
Keywords
Introduction
Total hip arthroplasty (THA) is currently the most successful and most frequently performed orthopaedic joint replacement surgery in patients with osteoarthritis of the hip and failed conservative treatment. Worldwide, over 1 million total hip arthroplasties are performed per year. 1 As recent studies have shown, a major complication after THA is loosening of the acetabular component with need for revision surgery. The subsequent loss of periacetabular bone stock in such cases is the main problem in acetabular revision surgery.2,3 In severe cases of bone loss, implantation of a “custom-made acetabular component” (CMAC) is, therefore, needed as an individualised treatment strategy. Especially in old and multimorbid patients, treatment failure may necessitate a permanent girdlestone arthroplasty, with severe reduction in mobility.
To date, several studies have described the use of CMACs as a treatment strategy that delivers good clinical results for patients with severe acetabular bone loss.4,5 Nonetheless, postoperative periprosthetic joint infection (PJI) remains 1 of the devastating complications after revision total hip arthroplasty (rTHA). Whereas the incidence of PJI after primary arthroplasty is described as ranging between 0.5% and 2%, the incidence rises to 30% after rTHA with megaprostheses, and to 43% in cases with previous PJI.6,7
To our knowledge, there is, to date, no available data in regard to the outcome and reinfection rate in patients who underwent rTHA with a CMAC a second time after a previously failed rTHA with a CMAC.
Knowledge of the outcome of such repeated attempts could prove helpful, not only in terms of being able to advise patients better, but also in terms of optimising rTHA treatment.
The aim of this case study was thus to describe the outcome and arising complications in patients who had undergone rTHA with CMACs a second time after a first unsuccessful treatment attempt with necessitated explantation of the original CMAC.
Our hypothesis was that the treatment success rate in patients with need for a second CMAC is similar to that of patients with only one CMAC, and, further, that, after treatment failure of the second CMAC, repetitive revision surgery is needed until wound consolidation. Our second hypothesis was that the clinical outcome after a second CMAC does not differ from that after only 1 CMAC.
Materials and methods
We performed a single-centre, retrospective case study including 4 consecutive patients, treated between December 2008 and December 2018, with a Paprosky IIIB or AAOS type III/IV periacetabular defect. All patients had undergone a second CMAC-rTHA after failure of a previous rTHA with a CMAC.
The inclusion criteria were, firstly, the renewed need for revision surgery with a CMAC due to severe periacetabular bone defects and the unfeasibility of a biological defect reconstruction with the aim for downsizing of the existing periacetabular defect and subsequent use of standard implants, such as a cranial socket or a modular revision system, and, secondly, failure of previous rTHA with subsequent need for explantation of the original CMAC.
The study was approved by our local institutional review board (Institutional Ethics Committee, No. 226/13). Written informed consent was obtained from all patients. Patients with a severe periacetabular bone defect after explantation of a CMAC due to a PJI were treated in a multi-stage procedure, according to Wimmer et al. 8 To exclude persisting PJI, implantation of the second CMAC was performed only after the histopathological and microbiological results from samples collected during open revision surgery were negative.
A thin-layer CT scan was performed preoperatively to acquire detailed planning shots. All eight of the custom-made implants (4 “original” CMACs, 4 “new” CMACs) used in this study were manufactured either by Peter Brehm (n = 6) (Peter Brehm GmbH, Weisendorf, Germany) or by AQ Implants (n = 2) (AQ Implants GmbH, Ahrensburg, Germany).
Clinical and radiographic follow-up assessments were performed postoperatively at 6 weeks, 6 months, and 1 year, and, thereafter, in 1-year intervals. The Harris Hip Score (HHS) and the visual analogue scale (VAS) were assessed preoperatively and again postoperatively during follow-up. 9 The evaluation of the pre- and postoperative radiological imaging was carried out by 3 independent examiners in respect to new osteolysis, significant or progressive radiolucent lines in comparison with previous images, changes of the “centre of rotation” (COR), and migration of the acetabular or femoral prosthesis component.
The definitions of the THA complications workgroup were used to evaluate postoperative complications. 10 Treatment failure was defined as an increasing change of the COR (>4 mm), screw failure, material failure, or (recurrent) PJI with need for explantation of the CMACs, as published by Roessler et al. 11
Outcome analysis
The endpoint of this study was defined as successful implantation of a second CMAC, without signs of implant dislocation or migration, or of infection at last follow-up, as described by Roessler et al. 11
Statistical analysis
Data was collected in Microsoft Excel 2016 (Microsoft Corporation, Richmond, USA) and SPSS statistics 25 for Windows (SPSS, Inc, an IBM company, Chicago, IL, USA).
Results
4 patients (1–4) underwent implantation of a second custom-made acetabular implant after treatment failure that necessitated explantation of the first CMAC. For the patients’ demographic data see Table 1.
Descriptive summary of patient data after retrospective evaluation at first and second rTHA with CMACs.
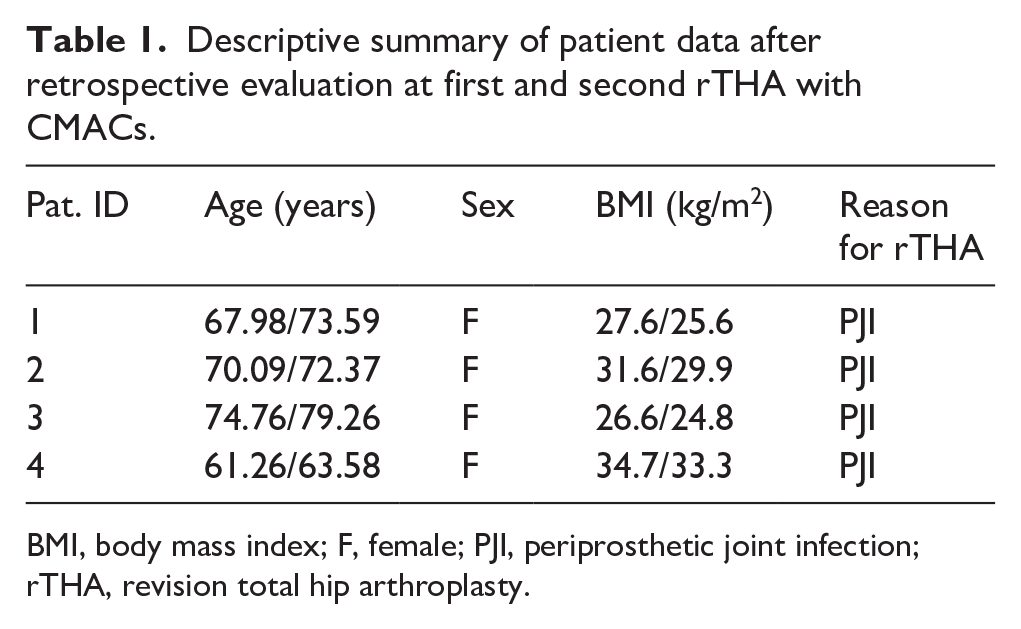
BMI, body mass index; F, female; PJI, periprosthetic joint infection; rTHA, revision total hip arthroplasty.
For all 4 patients, the reason for the first rTHA with CMAC had been PJI, with need for a two-stage procedure. In all of these cases, there had not been any microbiological or histopathological signs for a persisting infection in samples collected during previous revision surgery. At first CMAC-rTHA, all patients, with the exception of patient 3, had needed implantation of a prosthesis that replaced the proximal femur (see Table 2). Following the first CMAC-rTHA, patients 1–3 had needed revision surgery for various reasons prior to explantation, such as a persisting wound secretion (patient 1, 12 days after implantation) or a periprosthetic femoral fracture (patients 1 and 3; 57, respectively, 116 days, after implantation). Patient 4 had not required revision surgery prior to admission with a chronic PJI that necessitated explantation of the CMAC.
Descriptive summary of patient data for first rTHA with CMAC.
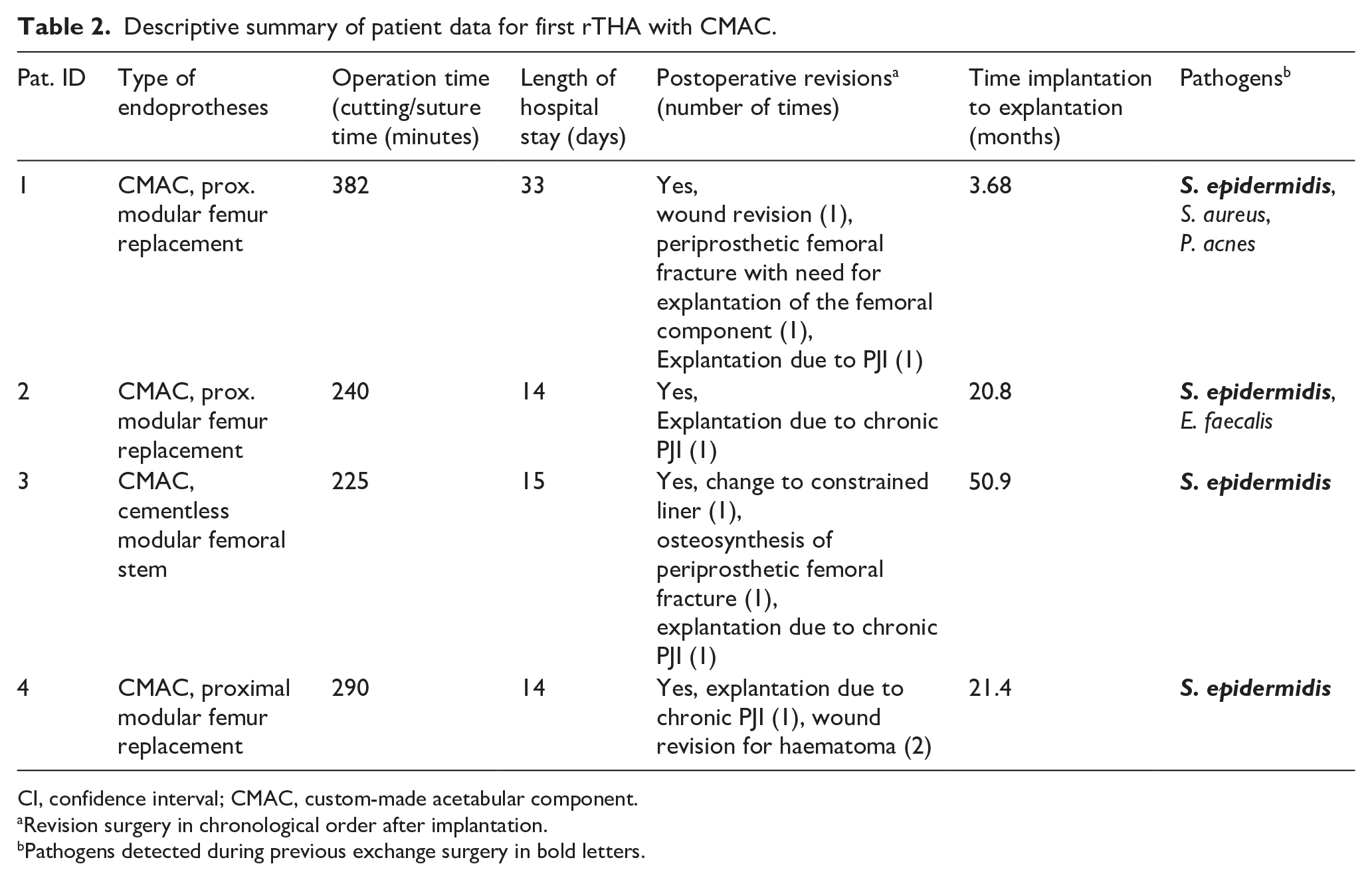
CI, confidence interval; CMAC, custom-made acetabular component.
Revision surgery in chronological order after implantation.
Pathogens detected during previous exchange surgery in bold letters.
In all 4 patients, explantation of the original CMAC had been necessary because of chronic PJI that had been diagnosed at next presentation, with a duration of symptoms >4 weeks.
After explantation of the original CMAC, patient 1 had needed wound revision surgery 13 days later, due to persisting wound secretion. Patient 2 had needed 4 revisions within 9 weeks after explantation of the first CMAC due to a persisting infection, followed by 2 wound revisions due to a superinfected hematoma, 4 months after explantation. In contrast, patient 3 had needed revision surgery due to a persisting infection that required 2 cycles of negative-pressure wound therapy (NPWT) and resection of the distal femur before wound consolidation. Patient 4, on the other hand, had needed revision surgery due to acute bleeding within 24 hours after explantation of the original CMAC. Microbiological evaluation of the intraoperative samples could identify the pathogen responsible for explantation of the original CAMC. In all cases, microbiological examination of samples taken during explantation of the first CAMC demonstrated the presence of the same pathogens that had originally been identified during explantation of the inlying implant prior to the first CMAC (see Table 2). The time between implantation and explantation of the original CMAC varied between 3.7 and 50.9 months.
Following explantation of the original CAMC and wound consolidation, all four patients had undergone open sampling. Implantation of the second CMAC was performed only in the absence of signs for a persisting infection (Table 2) (Figures 1 and 2). Figure 3 exemplifies the preoperative 3D planning proposal.
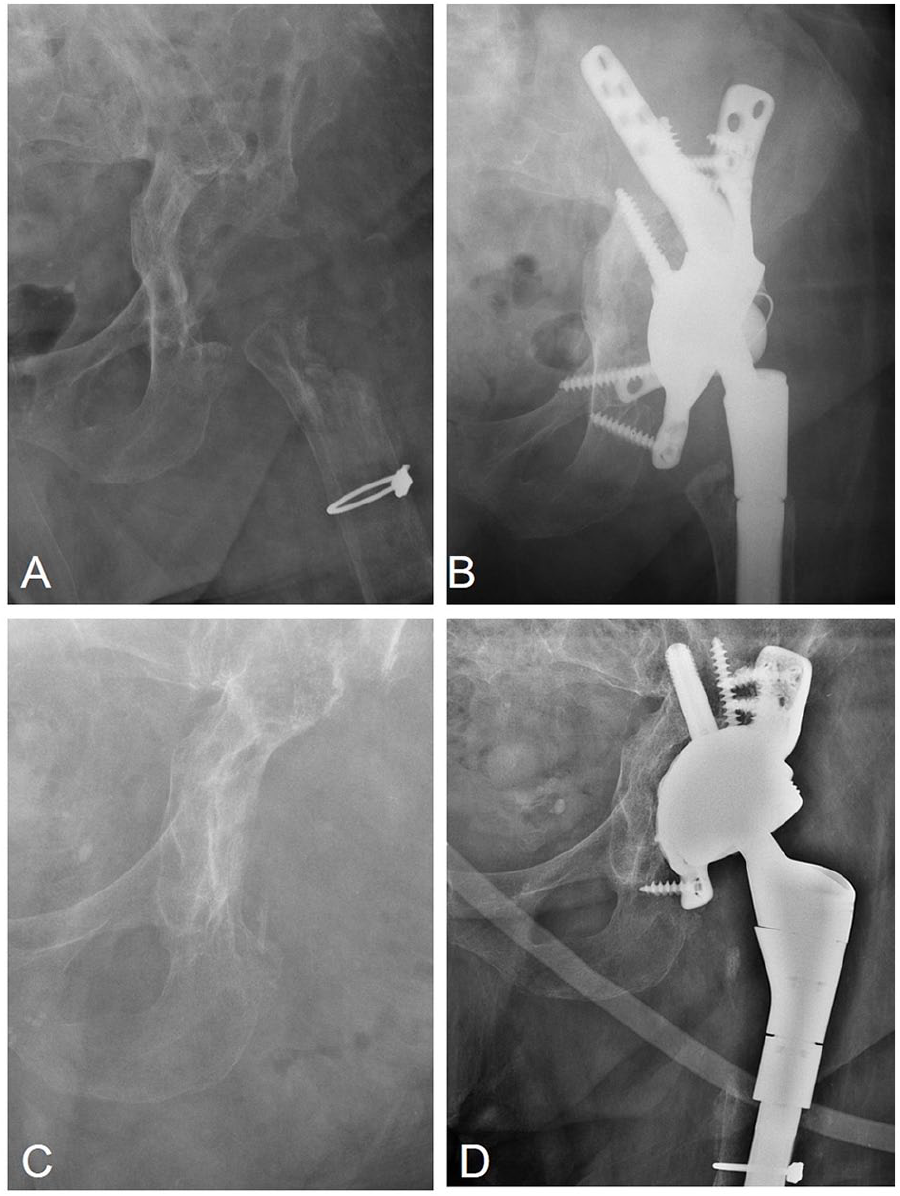
Preoperative anteroposterior radiograph for patient 3 before (A, C) and after (B, D) revision arthroplasty with custom-made acetabular components.
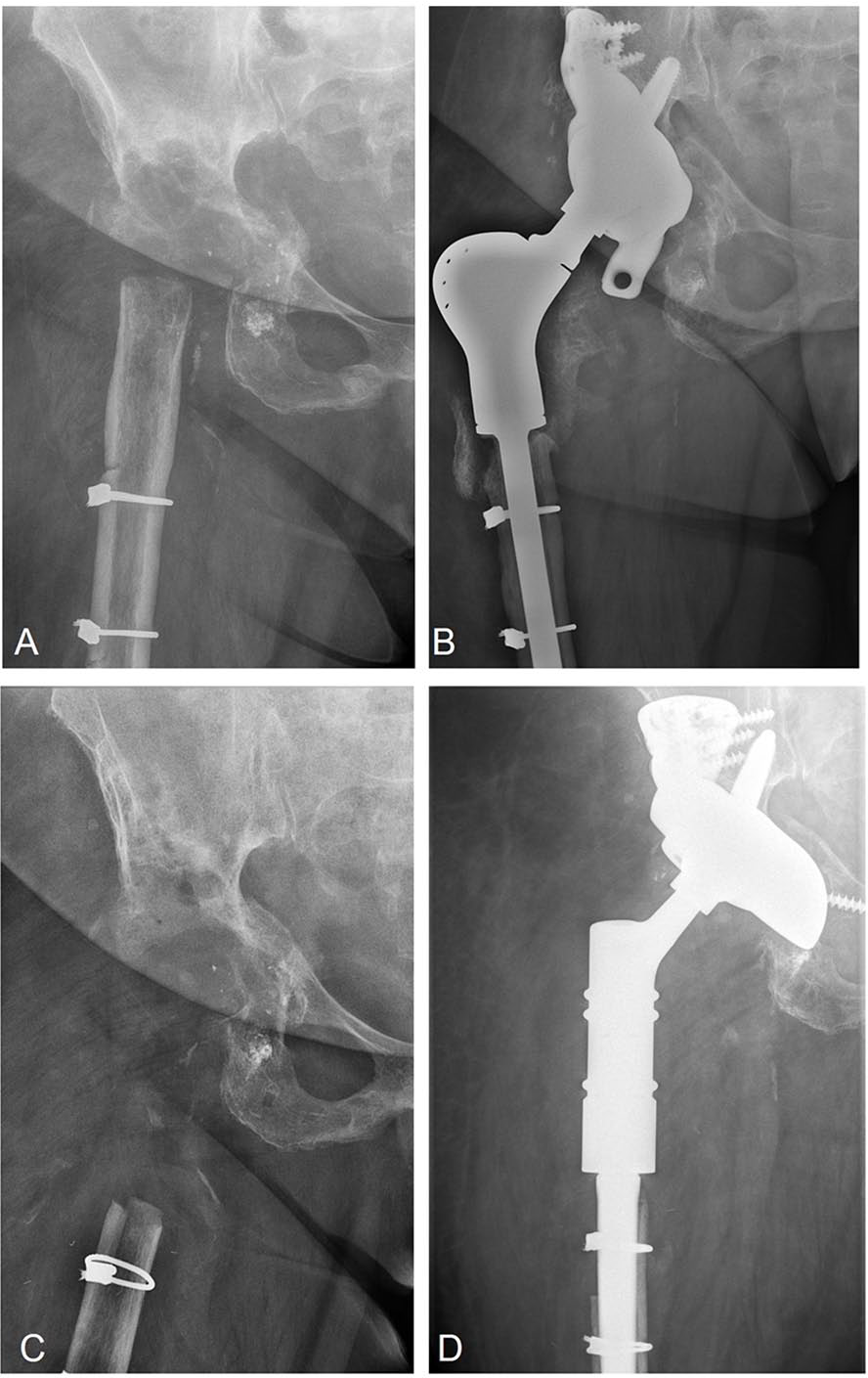
Preoperative anteroposterior radiograph for patient 4 before (A, C) and after (B, D) revision arthroplasty with custom-made acetabular components.
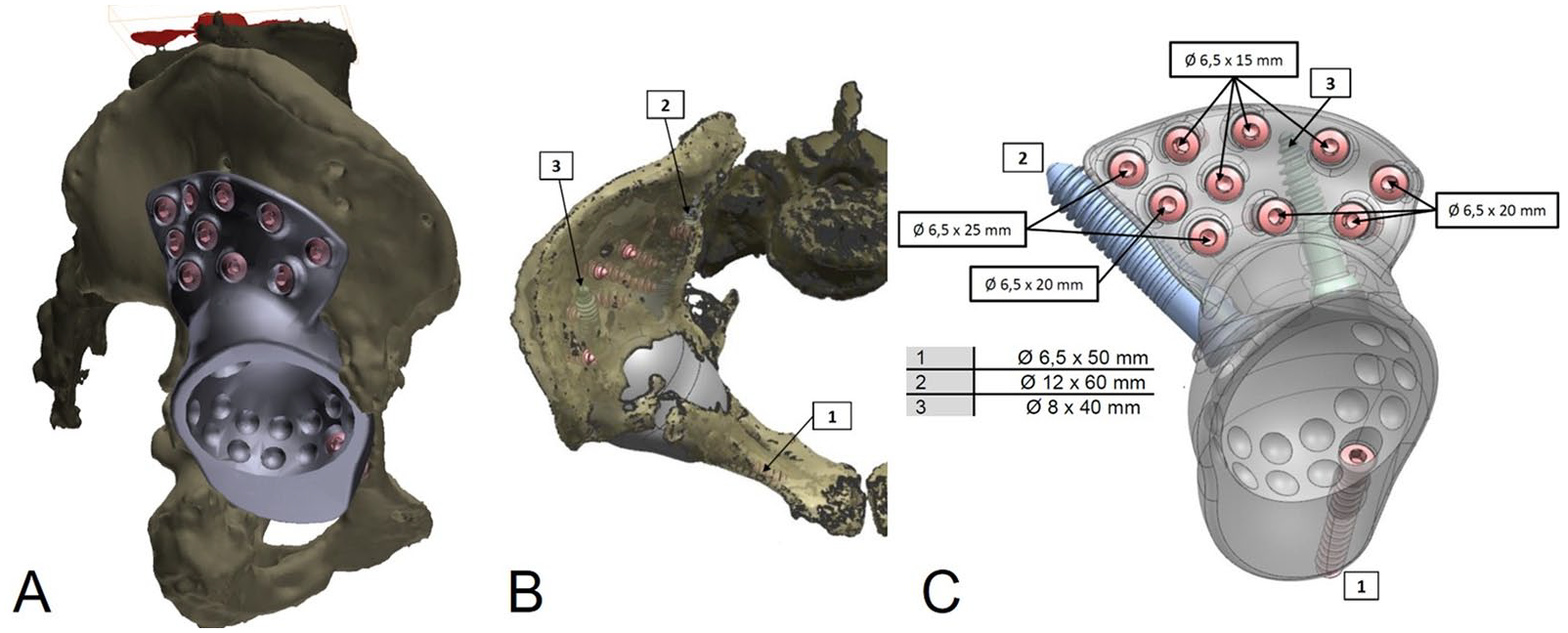
Preoperative interactive 3D planning proposal for second CMAC for patient 4 (A) view from the right side; (B) view in cranio-caudal direction; (C) lateral view of the implant with optimal length and diameter of the pole screws, e.g., to spare the sacroiliac joint.
The outcome of the second rTHA with CMACs, was successful for patients 1 and 4. The patient data for the second rTHA with CMAC is summarised in Table 3. Patients 2 and 3, however, presented with chronic PJI and need for explanation of the second CMAC at 12.9 months (patient 2), respectively, at 26.3 months (patient 3) after the second CMAC. Both of these patients had also needed revision surgery prior to explantation of the second CMAC. In the case of patient 2, revision surgery had been necessary due to a wound healing disorder, 10 days postoperatively, without microbiological detection of pathogens. Patient 3, on the other hand, had needed revision surgery, with exchange of the inlying liner to a tripolar cup and reconstruction of the offset, due to recurrent dislocations (third dislocation without trauma) 23.8 weeks after implantation of the second CMAC. In the end, patient 3 had additionally needed hip disarticulation for infect consolidation because the surrounding soft-tissues had been so heavily affected that local consolidation of the infection was not possible. Following explantation of the second CMAC, patients 2 and 3 had both needed revision surgery: in the case of patient 2, wound revision for hematoma followed by 4 cycles of NPWT was necessary until wound consolidation and wound closure was possible. In contrast, patient 3 needed 5 cycles of NPWT until wound consolidation and wound closure was possible.
Descriptive summary of patient data for second rTHA with CMACs.
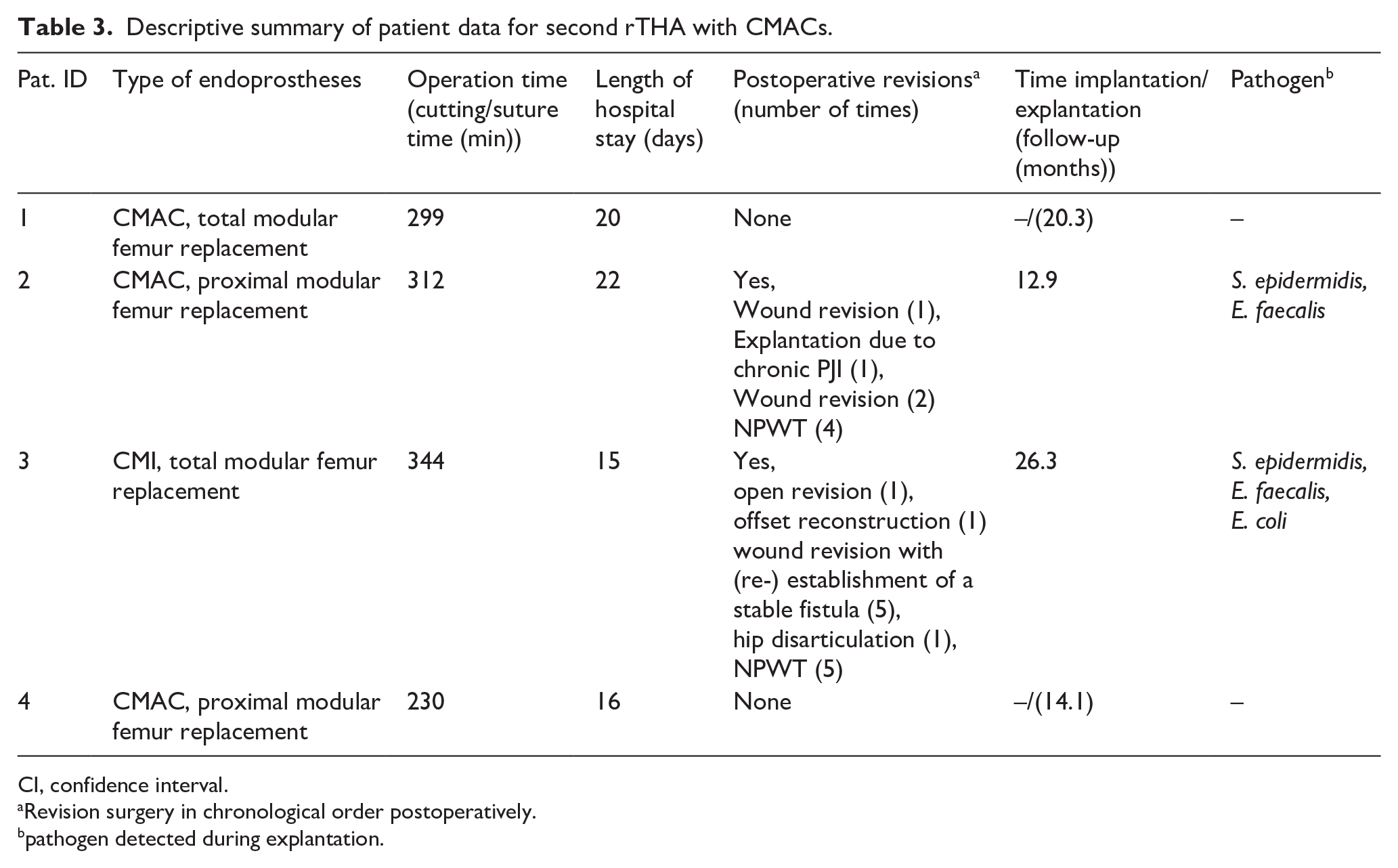
CI, confidence interval.
Revision surgery in chronological order postoperatively.
pathogen detected during explantation.
In summary, 4 patients underwent 2 consecutive rTHAs with CMACs, both times as part of a multi-stage procedure. The HHS and VAS scores, preoperatively, and postoperatively at last follow-up, before the diagnosis of PJI, are given in Table 4.
Descriptive summary of clinical data after retrospective evaluation after first (*), respectively, after second (†) rTHA with custom-made components before (‡) onset of symptoms.

VAS, Visual Analogue Scale; HHS, Harrison Hip Score.
There was no change of the postoperative VAS and postoperative HHS, prior to the onset of symptoms, after the first and second rTHA with CMACs. Furthermore, there was no difference in these scores after implantation of the second CMAC between patients with treatment failure and those with treatment success, at least, prior to the onset of symptoms.
All 4 patients had needed revision surgery after implantation of the first CMAC (see Table 2). In addition, all 4 patients had needed revision surgery after explanation of the first CMAC. The 2 patients with subsequent treatment failure of the second CMAC had undergone a higher number of revision operations after explantation of the first CMAC than those with successful treatment (patients 2 and 3: 6, respectively, 4 revisions vs. 1 revision each for patients 1 and 4). The number of revision surgeries operations after the second CMAC-rTHA varied between 0 (patients 1 and 4) and 13 (patient 3) (Table 3).
The treatment success rate after the second CMAC was 50% (2 of 4 patients). Patients 1 and 4 presented without signs for implant failure, 2 years after surgery (see Table 3).
Discussion
THA has become a well-established, highly standardised treatment option in patients with osteoarthritis of the hip and symptoms that are refractory to conservative therapy. 12 Consequently, rising numbers of rTHAs must be expected. Although, with a rate of 0.9%, large-sized acetabular defects with severe bone loss (Paprosky IIIB; AAOS III or IV) are rare, appropriate management remains a challenge in rTHA. 13 Because treatment success is also determined by the amount and quality of remaining bone stock, a well-fitting implant and an appropriate surgical technique are decisive in achieving a stable fixation of the implant and good clinical function. Previous studies that have used CMACs have reported promising results.3,14,15 Nevertheless, this customised treatment option is still rarely used, as it has several disadvantages, such as increased costs in comparison to standard implants, delay in surgery due to production time, need for an extensive surgical approach for implantation, and a long surgery time.
The aim of our study was to describe the outcome and complications in patients after a second rTHA with CMACs. The first part of our first hypothesis, which was that the overall implant survival after second CMAC-rTHA is similar to that reported in the literature for first-time rTHA with CMACs, could not be confirmed by our results, as our treatment success rate of 50% is significantly lower than that reported in previous studies, which describe failure rates of 0% (Christie et al. 16 ), 11% (Wind et al. 17 ), and 12% (Taunton et al. 14 ) for CMACs.14,16–18 However, in contrast to our study, which describes the outcome of a second rTHA with a CMAC, these studies evaluated the outcome after a “first” rTHA with a CMAC. It is difficult to identify precisely why the implant survival in our study was so low: a possible explanation could be that a selection bias occurred due to the small number of patients included in our case series. Another possible explanation may lie in the reason for explantation of the first CMAC, as all patients had needed revision surgery due to recurrent PJI. In this context, it is important to mention that the patients included in our study had all undergone CMAC implantation only after microbiological and histopathological exclusion of a persisting infection through a previous open sampling procedure.
The second part of our first hypothesis, which postulated that repetitive revision surgery would be required until wound consolidation in case of treatment failure is supported by our findings. All of the patients had needed revision surgery, either after the first CMAC only, or also after the second CMAC. Although revision surgery was needed for various reasons, the circumstance reflects the high complication rate in these complex cases. Interestingly, the patients with treatment failure after the second CMAC had needed a higher number of surgeries until wound consolidation after explantation of the first CMAC. For patients in this category, permanent girdlestone arthroplasty might, therefore, be a treatment option. Due to our low number of patients, further studies must confirm if the number of previous revision surgeries might be a prognostic factor for treatment failure. The 2 reported periprosthetic femoral fractures in our case series might, conceivably, be a “symptom” of poor osteointegration, for example, early-stage loosening of the implant due to low-grade infection that may have been present despite negative microbiological evaluation of the intraoperative samples.
Hip dislocation is another frequent problem encountered after rTHA. Although previous studies have reported dislocation rates of up to 30%,15,16 only 1 patient (patient 3) in our study needed open revision and exchange of the inlying liner, respectively offset-reconstruction. This had been necessary due to 2 dislocations after the first rTHA and 3 dislocations after the second rTHA, without appropriate trauma. Patient 3 had been the only patients for whom we had not used a tripolar cup during the initial/first rTHA with CMAC because an intraoperatively stable situation without a tendency towards (partial) dislocation had been achieved without it.
Our second hypothesis, which postulated a similar clinical outcome after a second CMAC-rTHA as after a first CMAC-rTHA, can be regarded as fulfilled: at last follow up after the second surgery, our results did not show a difference in HHS scores after second surgery in comparison to those after first surgery, before diagnosis of PJI. There was also no difference in HHS scores between patients with treatment failure and those without. We must, however, admit that we compared scores before the onset of symptoms. In comparison to the results published in the literature, in which HHS scores of 69 (Weber et al. 19 ), and, respectively, 81 (Mao et al. 20 ) are reported, the clinical function observed in our study after second CMAC-rTHA, must be regarded as inferior.14–16,19,20 In this context, we would like to note that we could not evaluate an insufficiency of the musculus gluteus medius or minimus as a clinical correlate for an intraoperative lesion of the superior gluteal nerve, as all of our patients had needed implantation of either a proximal femoral replacement or a total femoral replacement.
Lastly, our study does have several potential limitations. A first limitation is its retrospective design without a control group. A second limitation is that the sample size in our study is small for a retrospective study. A third limitation is the circumstance that the studied cohort was heterogeneous in terms of the extent of periacetabular bone loss or pelvic discontinuity. Nonetheless, our study is, to our best knowledge, the only one in this thematic field to date to evaluate the outcome of a second rTHA with CMAC after previously failed rTHA with a first CMAC.
Conclusion
In patients with severe acetabular bone loss and previously failed revision THA with custom-made acetabular components, repeat rTHA with a CMAC may be a solid treatment option for patients with an “uncomplicated” multi-stage procedure, i.e., without persisting infection after explantation of the original CMAC. While the outcome in terms of clinical function does not appear negatively affected by such a “second attempt,” the complication rate and risk of reinfection, nonetheless, high.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.