
Abstract
In this article the authors describe a modified surgical technique developed to enhance the classical irrigation and debridement procedure to improve the possibilities of retaining a total hip arthroplasty (THA) undergoing acute periprosthetic joint infection (PJI). This technique, debridement antibiotic pearls and retention of the implant (DAPRI), aims to remove the intra-articular biofilm allowing a higher and prolonged local antibiotic concentration by using calcium sulphate antibiotic-added beads. The combination of 3 different surgical techniques (tumour-like synovectomy, Argon Beam application and chlorhexidine gluconate brushing) might enhance the disruption and removal of the bacterial biofilm which is the main responsible of antibiotics and antibodies resistance. The timing of the diagnosis (6 weeks from the original surgery or 1 week from clinical symptoms appearance in the case of an hematogenous infection) and the preoperative isolation of the germ are fundamental in order to obtain a satisfactory outcome. A 12-week course of postoperative antibiotic therapy (6 weeks I.V. and 6 weeks oral) complete the postoperative protocol used by the authors.
The DAPRI technique might represent a safe and more conservative treatment for acute and early hematogenous PJI.
Introduction
Total hip arthroplasty (THA) provides reliable outcomes for patients suffering from end-stage degenerative hip osteoarthritis (OA), especially pain relief, functional restoration, and overall improved quality of life.1–3 Its high rate of cost effectiveness has allowed to be widely distributed in all mid- to advanced healthcare systems to such an extent that more than 1 million THA are performed worldwide yearly.4–6 1 of the causes that most provoke its failure is the insurgence of periprosthetic joint infection (PJI), which has an incidence, following primary THA, of 1–2% approximately and is the leading cause of revision of THA in many published registers and large cohort studies.7,8 PJI is 1 of the most catastrophic and difficult to manage complications following total hip and total knee arthroplasty. 9
In a setting of PJIs, timing of appearance (acute, subacute or chronic) and accurate diagnosis with organism isolation drive the surgical treatment.10–13
Classical PJI treatment options include “debridement, antibiotics, and implant retention” (DAIR), single-stage revision and double-stage revision. 14
THA revisions for PJI are extremely challenging for both patients and the medical team: from the patient perspective, they are often characterised by major blood and bone loss, increased mortality, high rates of intraoperative complications and a difficult postoperative course;15,16 from the medical staff perspective, surgeons are often required to perform multiple procedures, use the most advanced diagnostic techniques, choose very expensive antibiotic therapies and, in general, be prepared to follow the patients for a long period of time.
From a pure economic point of view, whether supported by public or private welfare systems, many authors have defined PJI as a real health emergency: increased length of in-house physical therapy, outside rehabilitation, hospital re-admissions, prolonged antibiotic therapy, elevated implant costs are all influencing the final cost of the treatment. A recent study by Parisi et al. 15 estimated the long-term social cost of an infected THA using a Markov analysis: the results are worrisome. In fact, the overall cost ranges from $389,307 for a 65-year-old patient to US $474,004 for a 55-year-old man.
The current authors recently described a novel surgical technique developed to enhance the classical DAIR procedure in order to improve the possibilities of retaining an infected total knee arthroplasty (TKA). 17 This technique, “debridement, antibiotic pearls, and retention of the implant” (DAPRI), has the goal of improving the outcomes of the classic DAIR procedure in total joint arthroplasty PJI treatment. The current authors believe that, extending the use of this surgical technique to the treatment of THA PJIs, may increase the possibilities of implant salvage respect to the classical DAIR technique.
The objective of this technical note is to describe the original DAPRI procedure adapted to the THA PJI treatment and to present its early results.
Surgical technique
The current authors apply the DAPRI procedure exclusively in the setting of an acute postoperative (within 6 weeks from the original THA surgery) or early haematogenous with a positive blood culture (within 7 days from clinical onset) infections after isolation of the micro-organism following a fluoroscopy guided hip aspiration (culture positive PJI). At the authors main Institution, the current authors do not perform the DAPRI procedure outside from these very narrow indications, which do not include culture positive polymicrobial PJI and generalised sepsis.
The DAPRI procedure, when applied to infected THA, has a stepwise approach. Following regional anaesthesia, preoperative antibiotic therapy is intentionally held to improve the sensitivity of intraoperative cultures, which are routinely performed in the number of 5.
After generous skin incision according to the classical posterior hip approach and abundant soft tissue exposure, the hip capsule is first identified, a classic “L–shape” capsulotomy is performed and the hip is finally dislocated. 18 At this point, the femoral head is removed and the proximal femur is gently moved antero-superiorly in order to get the best access possible to the intra-articular space. The acetabular polyethylene liner is removed first. At this point, an aggressive and radical “tumour-like” synovectomy and capsulotomy is performed including the posterior capsule layer. The objective of this surgical step is to remove all the soft-tissues contaminated by the infected biofilm.
Argon beam
Next, the biofilm on retained surfaces (proximal femur and acetabular component) is addressed by mechanical disruption with the use of an argon beam coagulator, (ConMED, USA), as electrical stimulation has been shown to enhance detachment of biofilm from orthopaedic implant surfaces. 19 The argon beam coagulator is usually set to 120 watts: its probe is placed in contact with the visible prosthetic surfaces (proximal femur and acetabular component) and the beam is applied in a painting brush-like fashion. The authors suggest caution applying this technique because it is still unclear whether this part of the procedure can alter the implants surfaces. 20
Chlorhexidine gluconate scrub
At this point, a 4% chlorhexidine gluconate-added brush is used to scrub all visible surfaces of the femoral and acetabular components: this is performed to mechanically remove the preformed biofilm as suggested by Tria et al. 21
Last, abundant pulse irrigation with 9 litres of povidone iodine added saline is performed.
At this point the wound is provisionally closed with an antimicrobial incision drape after placing a povidone-iodine soaked gauze in the wound. The surgical team un-scrub and the contaminates instruments are removed from the surgical field. The patient is re-draped again with clean drapes, the surgical team uses new gowns and gloves, and a new back table with new instruments is brought in the surgical theatre. After removing the gauze, further irrigation of the joint is undertaken using 3 L of bacitracin added 0.9% sodium chloride prior to inserting the new acetabular liner.
Calcium sulphate antibiotic-added beads application
At this point, new calcium sulphate antibiotic-impregnated beads are prepared on the new back table. A 10 ml-kit of PG-CSH (Stimulan; Biocomposites Ltd., UK) is mixed with 1 gr of vancomycin powder, 0.8 gr of tobramycin and a third antibiotic powder if suggested by the preoperative antibiogram. A smooth paste is formed by mixing all components for 60 seconds and is pressed into 3-mm and 4.8-mm diameter hemispherical cavities in a flexible mold (Figure 1). 22 These calcium sulphate beads are a biocompatible and resorbable antibiotic-loaded intra-articular delivery system, which allow for a continuous local elution of the appropriate antibiotic. The hydrophilic crystalline structure is normally reabsorbed over 4–6 weeks, and their presence is visible on radiographs for the same amount of time.
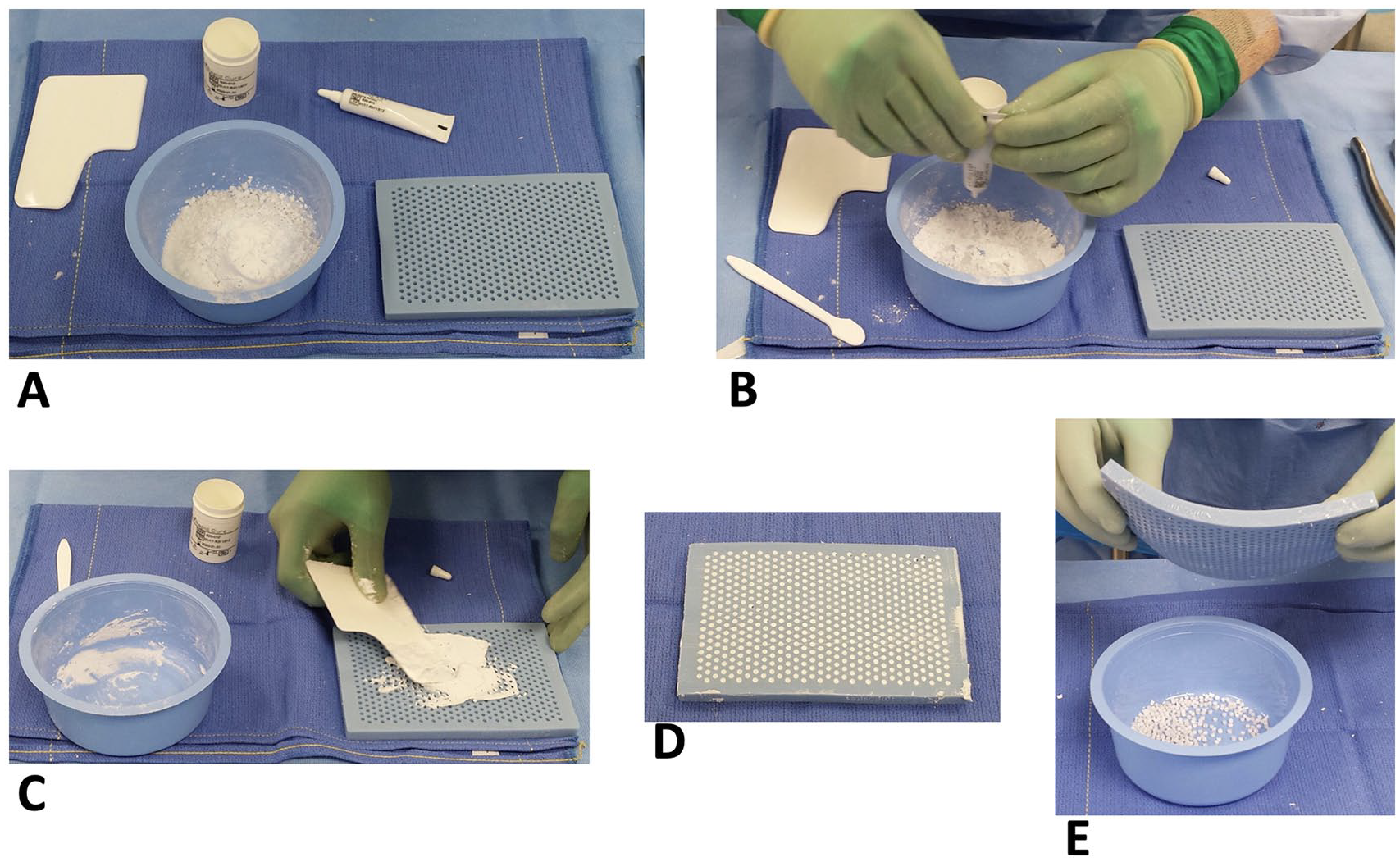
A 10-ml kit of PG-CSH (Stimulan; Biocomposites Ltd., UK) is mixed with the antibiotic powder (A) according to the preoperative antibiogram. A smooth paste is formed (B) by mixing all components for 60 seconds and is pressed into 3-mm (C) diameter hemispherical cavities in a flexible mold (D). The final beads are visible in Figure (E).
Ordinarily, the antibiotic beads are inserted in the hip joint in close contact to the joint and in the peri-articular soft tissues (Figure 2) in order to allow for a high concentration of antibiotics in the intra-articular space. A new ceramic-made femoral head is then placed on the femoral neck after irrigation and drying and the hip undergoes standard reduction. After placing an intraarticular drain, the fascia is closed with Stratafix size-1 (Ethicon, Johnson & Johnson, USA) suture, the subcutaneous tissue with 2-0 PDS suture and the skin with staples.
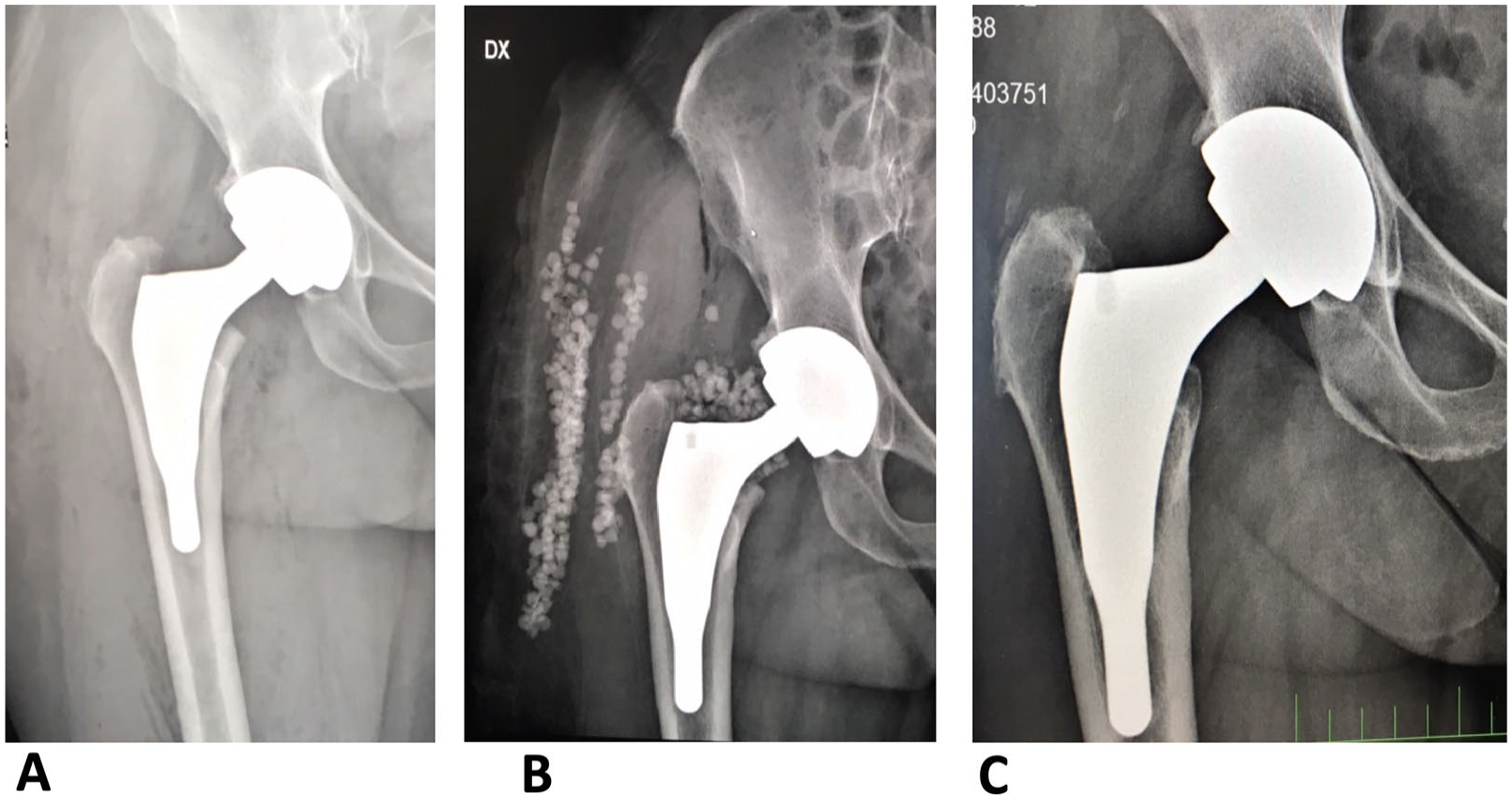
55-year-old female patient (A) right THA: acute PJI 28 days postoperatively; MRSA infection is detected and a DAPRI procedure is performed. The antibiotic-added beads have been placed intra-articularly and in the periarticular soft tissues. (B) at 2 years from the DAPRI procedure: the patient is asymptomatic and the serologic markers for PJI are negative.
All patients follow an identical, standard postoperative rehabilitation protocol, including weight-bearing as tolerated with crutches on the first postoperative day. Discharge from the hospital occurs when the patient achieves independence in activities of daily living, including walking 20 steps, climbing and descending stairs, and independent toileting.
Postoperative antibiotic treatment is routinely established in accordance with our institutional infectious disease service based on preoperative and intraoperative findings. A DAPRI procedure is usually followed by a six-week course of intravenous antibiotic therapy: after this, another 6-week course of oral antibiotic therapy follows. The procedure is usually considered successful when clinical presentation and serologic tests (erythrocyte sedimentation rate, C-reactive protein, and D-Dimer) normalise.
Results
The authors were able to report the early outcome of this procedure in 10 patients treated with DAPRI following a PJI in the hip joint. The original procedure was primary THA in all patients. Most patients undergoing DAPRI were male in our series (80%). The mean age of the patients was 74.8 years (range 57–84 years) and the mean body mass index (BMI) was 31 kg/m2 (28–35 kg/m2).
No patient was lost to follow-up at a minimum of 12 months (range 12–26 months): all the infections were classified as acute (within 6 weeks from the original surgery) or early haematogenous (within 7 days from clinical onset) infections with a known microorganism isolated after standard synovial fluid culture (Table 1). All DAPRI procedures were performed on average 3 days after onset of symptoms (range 1–6 days). The average length of stay at the treating Institution was 5 days (range 3–7 days). All patients underwent an Infectious Disease (ID) consult before leaving the hospital: the DAPRI procedure was followed by a 6-week course of intravenous antibiotic therapy (according to the antibiogram) and another 6-week course of oral antibiotic therapy afterwards (total of 12 weeks). At the final follow-up, the procedure was considered a success in 8 out of 10 patients: 2 patients underwent resection arthroplasty at 3 and 4 months respectively from the DAPRI procedure; a 2-stage THA revision has been planned afterwards.
Patients demographic and treatment data.
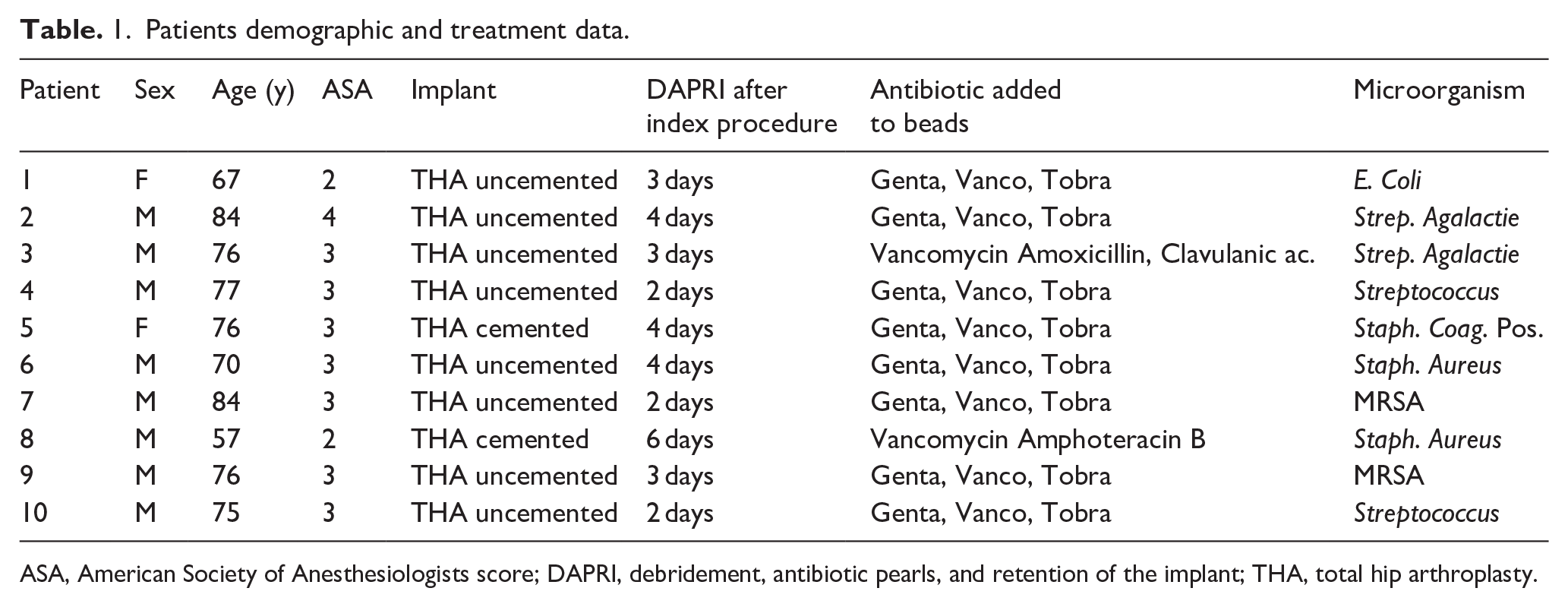
ASA, American Society of Anesthesiologists score; DAPRI, debridement, antibiotic pearls, and retention of the implant; THA, total hip arthroplasty.
Most infections were caused by Staphylococcus aureus species (60%) and 20% of them were methicillin resistant (MRSA). The rest of the patients developed Streptococcus agalactiae infection (20%), Staphylococcus coagulase negative (10%) and Escherichia coli (10%). The DAPRI procedure was considered a failure in 2 patients with MRSA Staphylococcus aureus and MSSA Staphylococcus aureus. The infection was controlled in 80% of the patients, thus the success rate of infection eradication was 80%. The current data had not sufficient power for statistical analysis, but prompt intervention and lower bacterial virulence appeared to facilitate the success of the surgical intervention.
Discussion
This article intends to propose a more effective method, when compared with previous surgical technique like DAIR, for the treatment of acute PJIs. The main innovations are represented by the use of an argon beam coagulator to undermine the integrity of the biofilm and bacterial cells, the use of chlorhexidine gluconate to remove any residue of bacteria and biofilm and the use of calcium sulfate antibiotic-impregnated beads to obtain an efficient intra-articular antibiotic MIC up to 40 days.22,23 The main objective of DAPRI is to eradicate an infection not yet strictly adhered to the bone-implant interface.24,25
Historically, the DAIR procedure showed a reasonable infection eradication rate between 50% and 80% when used in appropriately selected patients. 26 Several factors have been associated with its failures: patient’s own immune deficiency and a high ASA score, the presence of methicillin-resistant Staphylococcus aureus (MRSA), Streptococcus agalactiae or Pseudomonas aeruginosa species, a poor local tissues viability, the presence of rheumatologic disease, delayed presentation from the original surgery and erythrocyte sedimentation rate above 60mm/h at presentation.27–29
Historically, in front of a PJI, timing of the treatment is crucial in terms of obtaining a satisfactory outcome: a prompt treatment in acute PJIs may reach 100% of eradication while the success rate in chronic PJI has been reported between 28% and 62%. 30
The current authors established the described stringent timing criteria for DAPRI according to the current literature on biofilm biology and the results of other implant preservation techniques.26,28,29,31–34
The Center for Disease Control (CDC) recently identified a small group of bacteria that are posing a huge threat to global health: these are grouped under the acronym ESKAPE (Enterococcus faecium, Staphylococcus aureus, Klebsiella pneumoniae, Acinetobacter baumannii, Pseudomonas aeruginosa, Enterobacter sp.) 35 Unfortunately, >80% of human bacterial infections involve biofilm-producer microorganism and the current literature has shown that biofilm is the main actor in PJI’s development.36,37
Biofilm multilayer is 1 of the most widely distributed and successful mode of life on earth as well as on other planets. It has been described as either a mono or mainly polymicrobial community with a high cell density: bacteria in biofilm act first as habitat formers, supporting to their generation a matrix that provides structural and functional benefits. Biofilm formation is a complex process regulated by the availability of nutrients, external stresses (mechanical, chemical and physical), cellular competition, extracellular enzymatic activity and ultimately integration of internal and external stimuli to the layer. The extracellular matrix is composed by exopolysaccarides that physically provide architecture and stability to the biofilm itself.32,33,38
DAPRI’s multimodal approach focuses on biofilm destruction and prevention of recolonization of the joint environment. In fact, biofilm removal is mandatory for success with any implant retention procedure.36,39
After performing an aggressive, tumour-like intra-articular synovectomy and capsulectomy to radically remove the tissue in contact with the joint environment, the plasma argon beam coagulator is used on the visible retained components after removing the femoral head and the polyethylene insert from the acetabular component. Plasma is 1 of the 4 state of matter with gaseous, solid and liquid states: it has been described as an ionised gas consisting of ions, a broad spectrum of radicals, ultraviolet irradiation, electric fields, and ozone, which are all responsible for its antimicrobial efficacy. 40 Plasma argon beam has showed to disrupt the biofilm and bacteria through various plasma-produced reactive species which penetrate the extra cellular matrix and disrupt it. The disruption happens as the reactive species, passing through the outer membranes, interact with the inner cell membrane via lipid peroxidation: 41 its combination with a subsequent scrub of chlorhexidine at 4% concentration increases its microbicide potential.
Chlorhexidine gluconate (CHX) is 1 of the most widely used antiseptics for decontaminating skin, mucous membranes and medical devices: it has a bactericidal effect due to precipitation and/or coagulation of bacterial cytoplasmic contents caused by protein cross-linking. 42 In vitro studies have shown its effectiveness in eradicating various bacterial species from a biofilm culture:43–46 2% CHX has been verified being toxicologically safe and in fact it is used as an oral mouthwash without reports of adverse events.43,45 Although 2% and 4% chlorhexidine is not toxic to the skin and 2% chlorhexidine is the less cytotoxic antiseptic used in endodontics,43,45 their safety profile is not known in an intra-articular environment.
The innovation of the DAPRI technique stays only on the combination of previously well described techniques which combine the known microbicidal power of the aforementioned procedures having a well-documented high synergistic power.47,48
The addition of calcium sulphate beads constitutes a remarkable innovation as it allows to create an environment unfavorable to bacterial proliferation and biofilm synthesis for a period of time up to 40 days;49–51 moreover, these beads are completely re-absorbable, leaving no substrate for the proliferation of pathogens. 1 great advantage of calcium sulphate beads is their flexibility in terms of being mixed with antibiogram driven antibiotics: heat labile antibiotics can be added because there are no exothermic reactions during calcium sulphate beads preparation on the back table.
Historically, polymethylmethacrylate (PMMA) beads have been used in revision surgery for PJI since the 1970s. However, PMMA is not resorbable, its use requires a second intervention to remove it and has the intrinsic risk that to turn into a substrate for bacterial colonization and development of antibiotic resistances.52–54 PMMA elution profile is characterised by a massive release of antibiotic in the first 48 hours with risks of systemic toxicity and lack of drug elution afterwards.55–57
In vitro tests have shown a long-term rate of antibiotic-load release while maintaining antimicrobial efficacy and constant antibiotic elution profile by calcium sulphate beads compared to PMMA.23,58,59
The described DAPRI technique has multiple aspects still to be investigated. First, during the argon beam irradiation, temperatures of 40°C are reached and applied for a few seconds on the retained implants; it is not clear whether this can eventually be detrimental on the mechanical properties of the stem neck and on the acetabular component:41,60 hypotheses of relation between contact with electrocautery devices and failure of prosthetic implants have been raised.61,62
The use of calcium sulphate beads is prone to complications: a large series has described the safety profile and complication rate of a specific brand of calcium sulphate beads, which is the same used by the current authors, during lower limb PJI surgical treatment; 63 the main complications described in this series are prolonged wound drainage and transient hypercalcemia. If wound drainage occurred in 4.2% of patients and was mainly treated conservatively, transient hypercalcemia averaged 11.7 mg/dL and was detected in 5.4% of patients: in all cases the value returned to normal within 5 days. To avoid an increase in serologic calcium, Kallala et al. 63 suggested to limit the volume of calcium sulphate to a maximum of 40 cc per procedure. Another complication linked to the use of calcium sulphate beads is the development of heterotopic ossification, noted in 1.7% of cases. 63
The DAPRI technique proposed in this article has several potential and major limitations. First, inclusion criteria are very rigorous and the authors do not suggest applying this surgical approach outside of those criteria, as preoperative microorganism identification and accurate timing are fundamental. Second, this technique represents a multimodal approach using several surgical techniques previously reported by different authors. Third, long-term clinical outcomes have not been reported and further investigation is mandatory.
Conclusion
The debridement antibiotic pearls and retention of the implant (DAPRI) is a standard DAIR technique augmented by the intraarticular use of the argon beam coagulator to burn and disrupt the biofilm, the chlorhexidine gluconate brush to further kill and remove biofilm, and calcium sulphate antibiotic-impregnated beads to prolong and elevate the intra-articular antibiotic concentration in the setting of THA PJI.
PJI prevention is still key but the current literature still lacks well documented and effective PJI prevention protocols.
We believe that the DAPRI technique might represent a reasonable treatment for acute and early hematogenous PJI. We expect that this approach will improve upon the DAIR success rate, although more studies are necessary to evaluate the clinical efficacy of this surgical procedure.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.