
Abstract
Introduction:
Heterotopic ossification (HO) occurs in almost ⅓ of total hip arthroplasties (THAs). A direct anterior approach (DAA) with an orthopaedic table is less likely to cause HO than a posterior approach. Without an orthopaedic table, the exposure of the femur requires additional soft tissue release. Soft tissue trauma leads to the production of HO inductors. Our study evaluated the incidence of HO 6 months after THA and compared the results between DAAs without an orthopaedic table and posterior approaches.
Methods:
Retrospectively, 164 consecutive, primary THAs were included: 76 through a posterior approach and 88 through a DAA. The main objective was to measure the presence of HO on pelvis radiography 6 months after surgery.
Results:
The incidence of HO was significantly higher in the DAA group than in the posterior approach group (47.7% vs. 27.6%, respectively; p < 0.01). The overall incidence of HO was 38.4%. No significant difference was found between the 2 approaches regarding the severity of HO. No significant risk factor for HO was identified other than the surgical approach.
Discussion:
In our study, the incidence of HO after THA in patients undergoing DAA without an orthopaedic table was higher than in patients undergoing a posterior approach after 6 months of follow-up. This result is closely related to the surgical trauma. It suggests that the minimally invasive feature of a surgical approach cannot be dissociated from the overall conditions in which it is performed.
Introduction
Heterotopic ossification (HO: ectopic formation of mature trabecular bone in soft tissues) is a postoperative complication of total hip arthroplasty (THA). It occurs in about 30% of THAs. 1 Although it is often asymptomatic, HO can affect functional outcomes,2–4 leading to hip ankylosis or revision surgery. 5 HO appears within 12 weeks after surgery. 6 In an environment favourable to osteogenesis, local and systemic inducing agents, which activate the differentiation of mesenchymal cells into osteoblasts, lead to the production of HO. 7 Several risk factors for HO after THA are known. Among them, the surgical approach has been highlighted in the literature.1,8–10 In recent years, there has been renewed interest in Hueter’s direct anterior approach (DAA). Compared to other approaches, it allows a faster functional recovery and reduces the risk of dislocation.11,12 For these reasons, many surgeons are currently changing their approach. Nevertheless the posterior one remains the most commonly used for THA worldwide. 13 Newman et al. 14 has shown that HO is less likely to occur by DAA on an orthopaedic table compared to a posterior approach (24.3% vs. 27.5%, respectively). Without an orthopaedic table, DAA requires additional soft tissue release at the upper end of the femur and the use of retractors that are traumatic for muscles. 15 Soft tissue trauma leads to the production of HO-inducing agents.16–18 An orthopaedic table requires a well-trained surgical team to be safely used. It is not affordable for most hospitals and thus, many surgeons do not have access to this technical tool. Furthermore, using a standard operating table for DAA provides some benefits. It allows for the assessment of leg length and hip testing during the operation which are not possible with an orthopaedic table. To our knowledge, no study has yet evaluated the incidence of HO when using DAA on a standard operating table compared to a posterior approach. The aim of our study was to radiologically compare the incidence of HO in these 2 THA surgical approaches.
Methods
In our University Hospital, 1207 THAs were performed between January 2015 and September 2018. We retrospectively studied 164 consecutive, primary THAs: 76 posterior approaches and 88 DAAs. The inclusion criteria were THAs performed on patients with degenerative disease, which did not require bone grafting, on a hip free of any previous surgical operation. Only THAs performed by orthopaedic surgeons who changed their approach over time from a posterior approach to DAA were included. Patients who presented 1 of the following complications within 6 months after surgery were excluded: prothesis dislocation, surgical revision (haematoma, infection), or fracture (Figure 1).
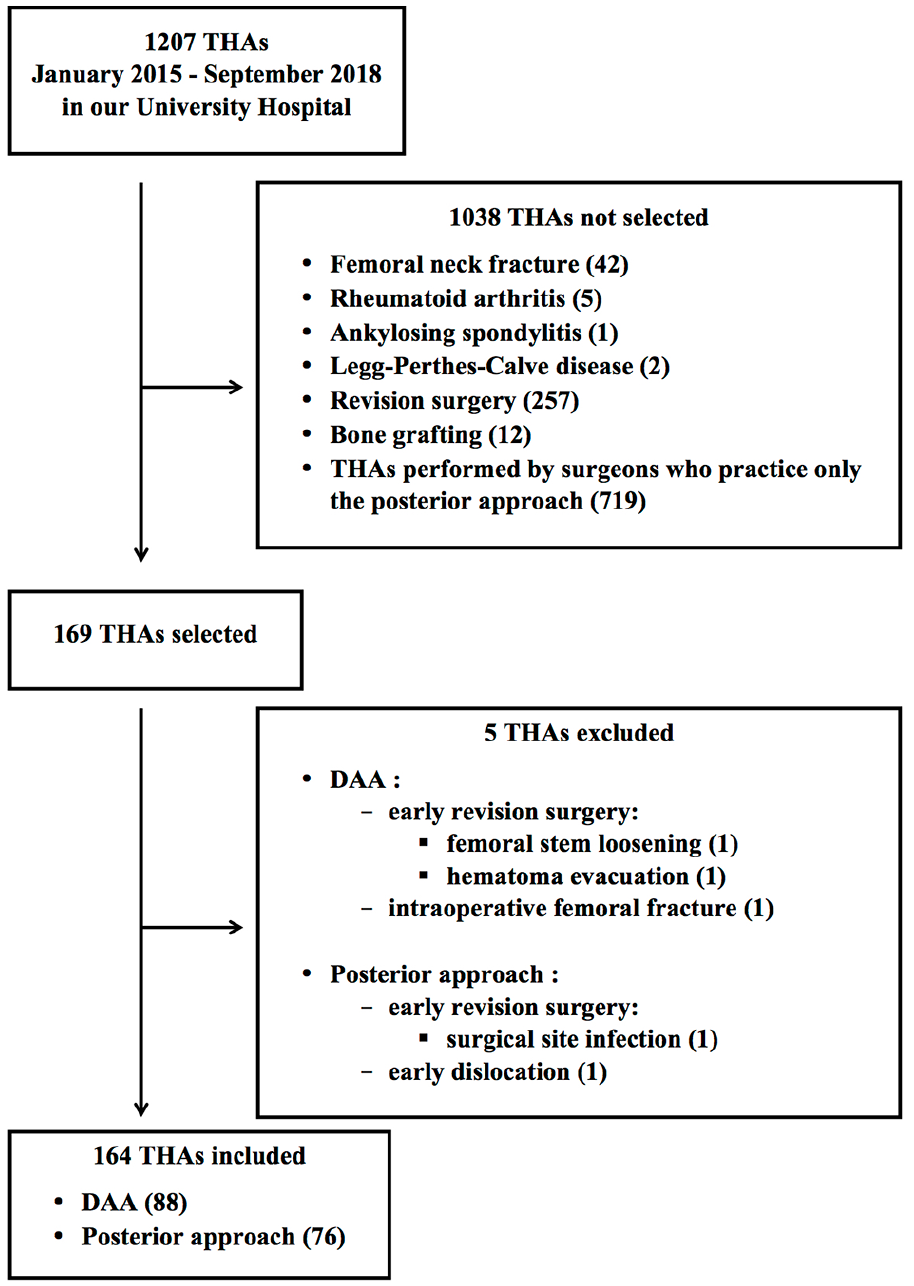
Flowchart.
Hueter’s DAA was performed in the supine position on a standard operating table. The fascia of the tensor fasciae latae muscle was incised to the intermuscular plane of Smith Peterson. Anterolateral capsulectomy was performed up to the insertion of the gluteus minimus muscle wide proximally and to the lesser trochanter wide distally. To enable exposure of the femur, a femoral retractor was positioned on the lateral edge of the greater trochanter. 19 The posterior approach was performed in lateral decubitus. The gluteus maximus muscle was split, and short external rotators were detached. For both surgical approaches, irrigation to evacuate bone fragments was done with a syringe of 0.9% NaCl (500 ml). No pulsating lavage was used. After surgery, the rehabilitation protocol was the same for all THAs: weight-bearing was allowed immediately after surgery.
Postoperative antithrombotic prophylaxis was provided with low-molecular-weight heparin for 6 weeks. Ketoprofen (100 mg) was given twice a day for 48 hours postoperatively for analgesic purposes, except for 12 patients who had contraindication for non-steroidal anti-inflammatory drugs (NSAIDs). All patients received dexamethasone (8 mg) as part of the anaesthetic protocol before surgery. No patient had prophylactic radiation therapy before or after surgery. No bilateral THA was performed in a single stay. The main evaluation criterion was the presence of HO on anteroposterior pelvis radiography at 6 months after surgery.
The HO grade was defined according to the Brooker classification (Figure 2). 20 An initial double-blind assessment was made by 2 independent senior orthopaedic surgeons. In case of discrepancy, they performed a second evaluation together. They would then agree on the most accurate HO grade. The secondary outcomes were to compare the rate of HO grades ⩽2 and ⩾3 and the rate of HO spurring the greater trochanter. The type of osteoarthritis was defined according to Bombelli: atrophic, normotrophic and hypertrophic. 21 Data were analysed by an independent investigator using Systat software (V11.0). Continuous variables are expressed as the mean and standard deviation. A Student’s t-test was used for continuous variables. A Pearson’s chi-square test was used for categorical data. The duration variables were compared by a nonparametric Kruskall-Wallis test. Statistical significance was set at p = 0.05.
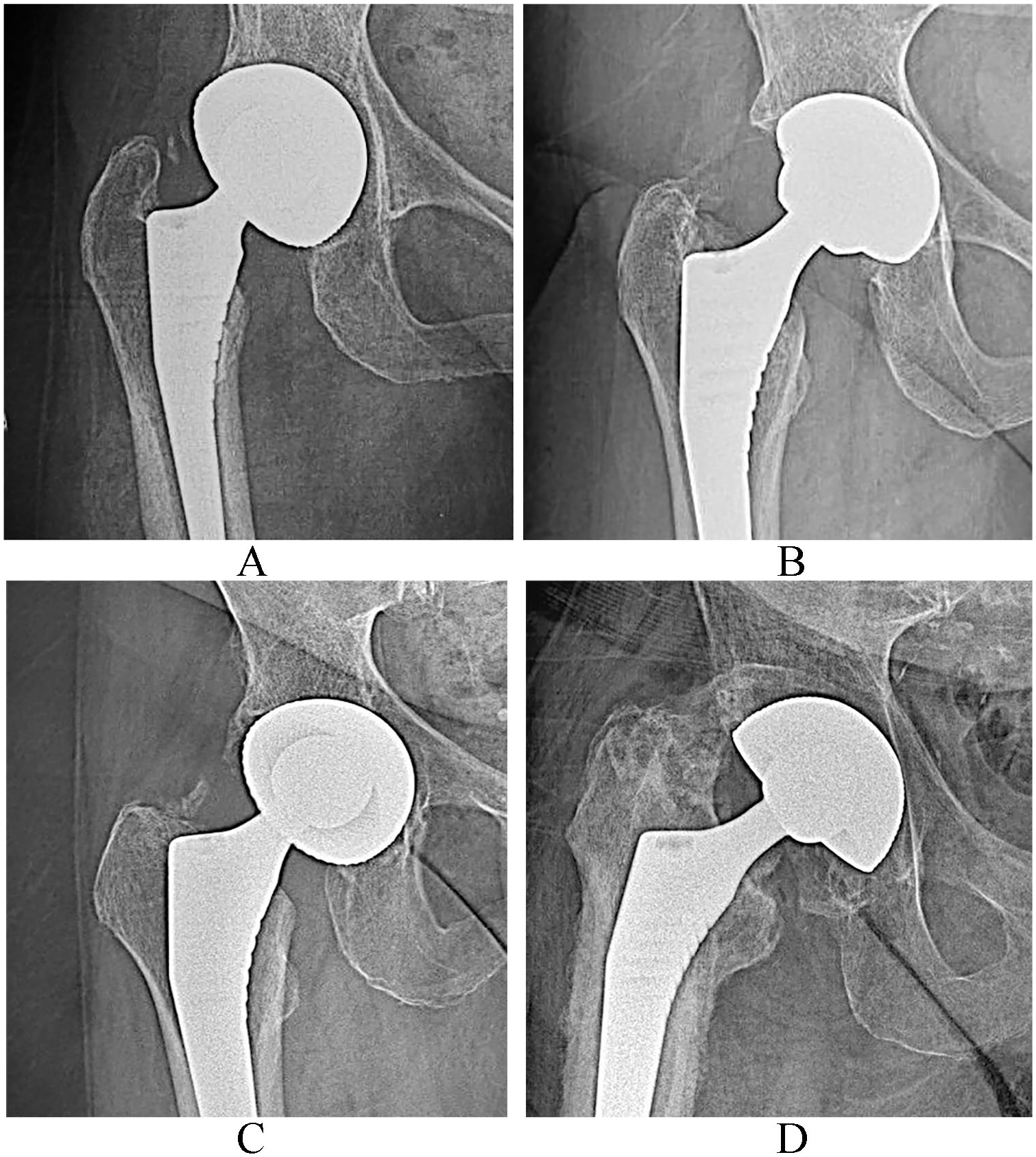
Brooker classification. (A) grade 1: islands of bone in the periarticular soft tissues (B) grade 2: acetabular or femoral bone spurs with at least 1 cm between the bone surfaces (C) grade 3: acetabular or femoral bone spurs with less than 1 cm between the bone surfaces (D) grade 4: apparent ankylosis of the hip joint.
Results
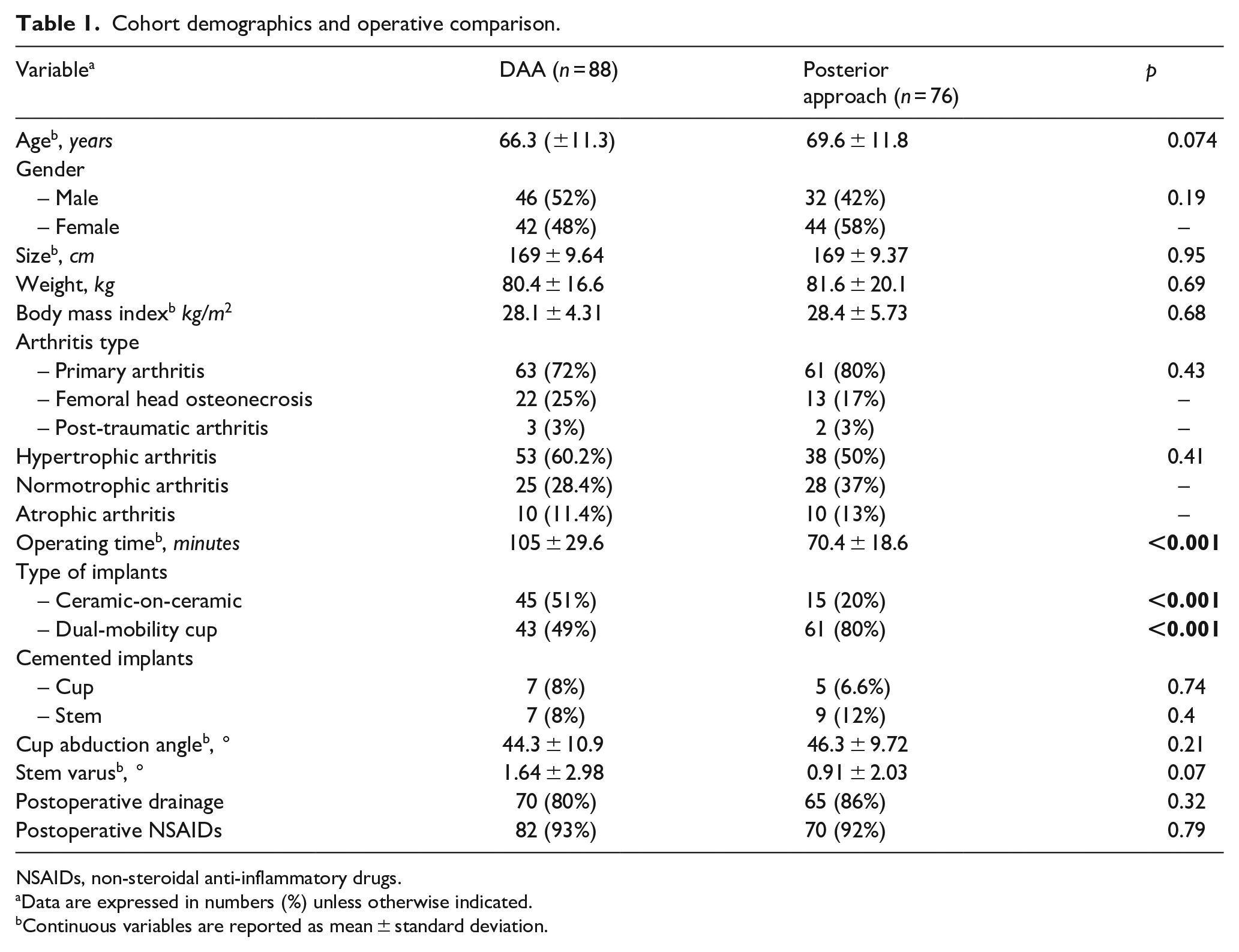
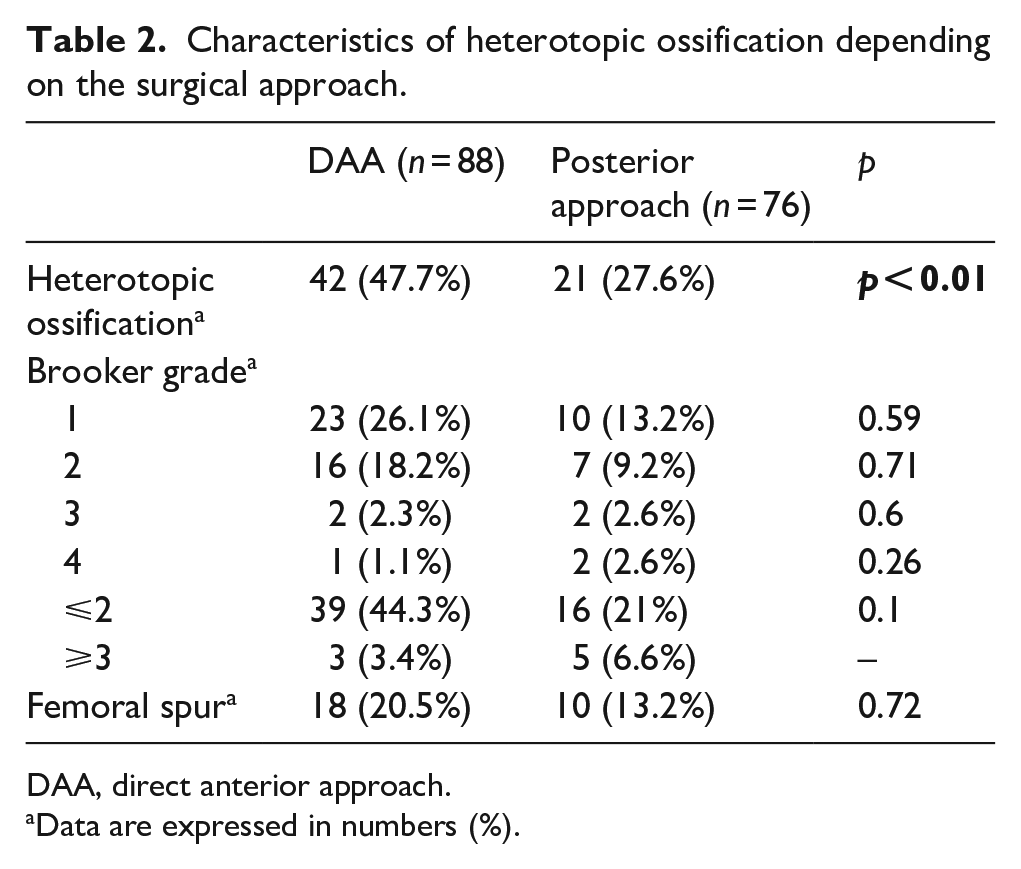
Demographic and surgical characteristics are summarised in Table 1. Some variables were significantly different between the surgical approaches including the type of prosthesis (ceramic-on-ceramic: 51% for DAA and 20% for posterior approach; dual-mobility cup: 49% for DAA and 80% for posterior approach; p < 0.001) and mean operating time (70.4 minutes for posterior approach vs. 105 minutes for DAA; p < 0.001). The incidence of HO in the DAA group was 47.7% while it was 27.6% in the posterior approach group (p < 0.01). The overall incidence of HO was 38.4%. There was no significant difference between the 2 approaches regarding the severity of HO, femoral spur formation on the greater trochanter, or rate of HO grades ⩽2 and ⩾3 (Table 2). Population characteristics failed to demonstrate a significant correlation with the development of HO. Regarding the surgical intervention parameters, only the surgical approach was associated with differences in the rate of HO development (Table 3).
Cohort demographics and operative comparison.
NSAIDs, non-steroidal anti-inflammatory drugs.
Data are expressed in numbers (%) unless otherwise indicated.
Continuous variables are reported as mean ± standard deviation.
Characteristics of heterotopic ossification depending on the surgical approach.
DAA, direct anterior approach.
Data are expressed in numbers (%).
Population characteristics depending on the presence of HO.
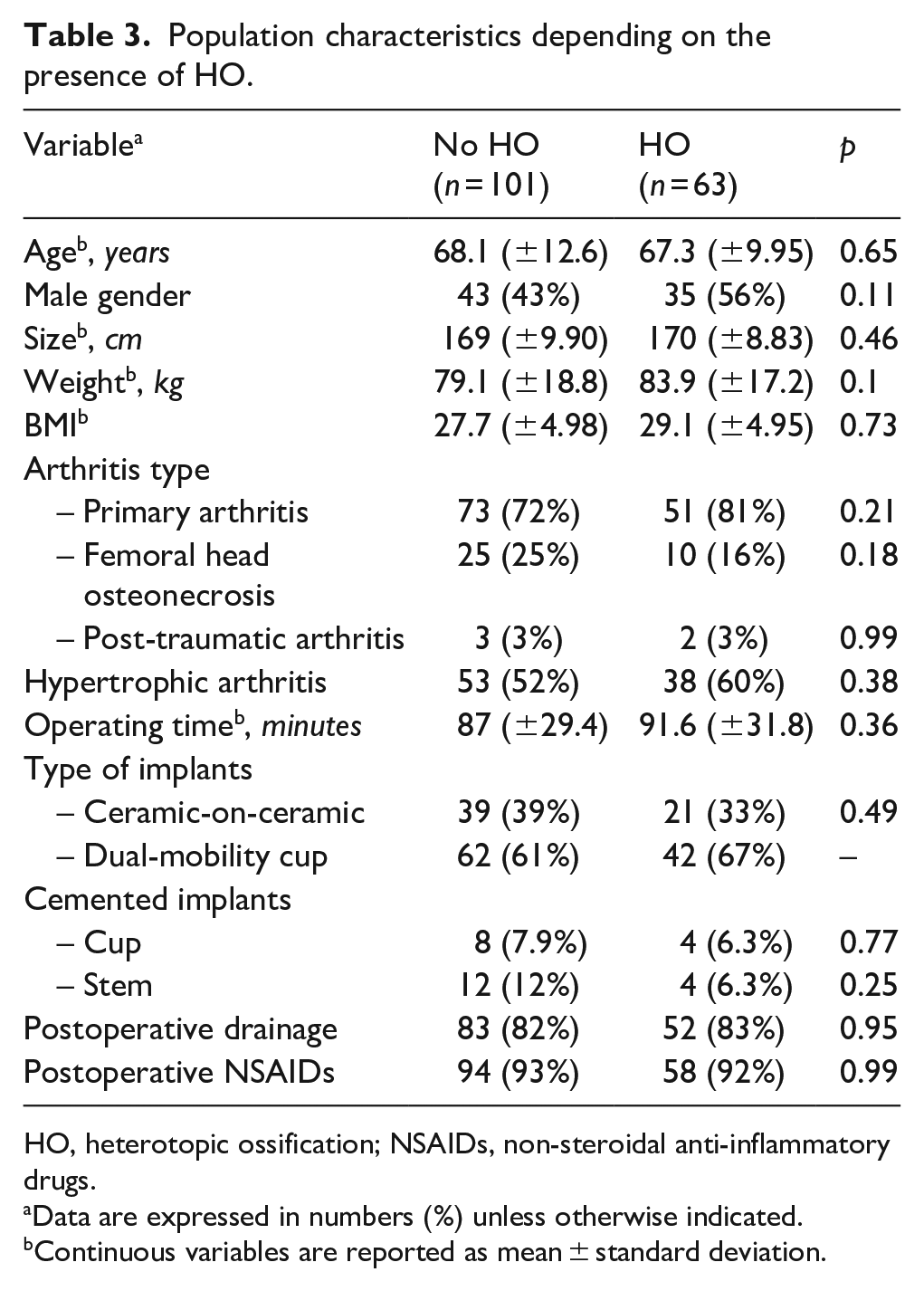
HO, heterotopic ossification; NSAIDs, non-steroidal anti-inflammatory drugs.
Data are expressed in numbers (%) unless otherwise indicated.
Continuous variables are reported as mean ± standard deviation.
Discussion
The reported incidence of HO after THA in the literature varies from 5% to 90%. In a meta-analysis published in 2015 by Zhu et al., 1 the incidence of HO was 30%. In our study, it was 38.4%. Tippets et al. 8 carried out a retrospective study including 236 THAs operated by DAA in 2 different hospitals. In hospital 1, DAA was performed on an orthopaedic table; in hospital 2, on a standard operating table. The incidence of HO was significantly higher in hospital 2 (48.8%) than in hospital 1 (33%) (relative risk [RR] = 1.48; 95% confidence interval [CI], 1.07–2.04). Furthermore, the severity of HO according to the Brooker classification was significantly higher in hospital 2. These results suggest that the use of an orthopaedic table for DAA may influence the incidence of HO. However, the 2 hospitals had heterogeneous treatment strategies concerning anti-thrombotic prophylaxis (NSAIDs, Coumadin, or heparin) and postoperative drainage. Newman et al. 14 carried out a retrospective monocentric study in which they compared the incidence of HO after THA through a DAA using an orthopaedic table or a posterior approach. The incidence of HO was 24.3% for DAA and 27.5% for posterior approach (p = 0.04) on the radiological evaluation 6 months after surgery. They justified this significant difference by the minimally invasive characteristic of DAA since this surgical approach goes through the intermuscular plane. In our study, the incidence of HO by DAA without an orthopaedic table was 47.7%, which is close to the incidence found by Tippets et al. 8 in hospital 2.
We did not find any significant difference concerning the severity of HO according to the Brooker classification between the 2 groups. Several studies have shown that HO was associated with a reduced range of motion and pain after THA, proportional to the grade of HO. 22 The pathophysiology of HO is not fully established. Trauma, such as a surgical operation, leads to the release of local- and systemic-inducing agents (bone morphogenetic protein-4, prostaglandin E2, and interleukin-1β in particular). There are modifications of environmental tissue factors (hypoxia and alkalosis) that induce the differentiation of quiescent pluripotent mesenchymal stem cells into osteoblasts in periarticular soft tissues.7,16–18 Using a minimally invasive approach for THA limits the surgical trauma. Therefore, it seems relevant to think that the cascade leading to the formation of HO is then reduced. Although this hypothesis has not been demonstrated yet, Bergin et al. 23 showed that biochemical markers of muscle damage and inflammation were lower when DAA was performed for THA compared to a posterior approach. They do not specify the type of operating table that was used for DAA or the type of retractor. The minimally invasive characteristic of DAA may be less pronounced on a standard operating table. Greater release of soft tissue is needed to expose the femur.15,24 Placement of aggressive retractors on top of the greater trochanter can damage the abductor muscles, especially the gluteus minimus muscle. To support this hypothesis, we studied the proportion of HO originating from the proximal femur, but no significant association was observed on this criterion.
There are some limitations to our study. Indication and confusion biases are possible in retrospective studies. A significant difference existed between the 2 groups concerning the type of prosthesis. Dual-mobility cups are known to improve prosthetic stability, and they were preferentially used in the posterior approach group for fear of dislocation with this approach.
A significant difference was also found for the mean operating time, shorter in the posterior approach group than in the DAA group. In the literature, operating time has not been identified as an HO risk factor. 6 No HO risk factor other than the surgical approach was highlighted in our study. The Brooker classification is the most used classification in the literature (43% of studies). It is a simple and reproducible measurement method to perform in common practice.22,25 Wright et al. 26 found that the inter-observer correlation of the Brooker classification was fair, although the intra-observer correlation was good.
Lastly, the study is limited by the lack of clinical data. It would have been relevant to study the hip range of motion according to the surgical approach and HO grade. Unfortunately, a large number of these data were missing at the 6-month follow-up.
In our cohort, 2 patients required revision >6 months after surgery for disabling hip stiffness due to HO (1 patient from the DAA group with HO grade 3 and 1 patient from the posterior approach group with HO grade 4).
Measurement bias was limited due to our use of double-blinded analysis and observation bias was limited as the position of implants was the same for both groups. It has been shown that HO appears between 4 and 12 weeks postoperatively, 6 so is constituted and easily radiologically assessable at 6 months. Therefore, the occurrence of HO >6 months post-surgery was not evaluated.
The surgeon’s experience and mastery of a surgical approach may influence the importance of surgical trauma. Hartford and Bellino 27 found a decrease in HO incidence following the learning curve of DAA. This difference was mainly attributed to changes in the surgical technique over time and the importance of the intraoperative irrigation performed. Historically, the posterior approach was the only surgical approach used in our hospital for THAs. Some surgeons learned DAA during their internships at other hospitals that specialised in prosthetic surgery, where they performed >50 THAs each by DAA. This minimised the effect of the learning curve on our study cohort.
Our study is a reflection on the use of DAA in our hospital. Surgeons were encouraged by the good results of DAA in the literature, particularly in terms of the rapid rehabilitation after THA. In our study, the incidence of HO at 6 months was higher after DAA on a standard operating table than that after a posterior approach. This result suggests that the minimally invasive feature of a surgical approach is not dissociable from the overall conditions in which it is practiced. Using an orthopaedic table or specific retractors for DAA as exposure tools significantly affects the outcomes of THA.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.