
Abstract
Background:
Acquired hip deformities in patients affected by hereditary multiple exostosis (HME) may incur in early hip osteoarthritis and functional limitation requiring primary total hip arthroplasty (THA). Characteristic coxo-femoral joint dysmorphisms in HME may pose a challenge for the orthopaedic surgeon. Here we report our experience in a series of patients with HME treated in our hospital with THA.
Methods:
With a mean follow-up of 5 years, 10 primary THAs were reviewed; proximal femur deformities, acetabular dysplasia and joint osteoarthritis has been assessed through x-rays and CT-scan evaluation. In all cases hemispheric press-fit cups were used; 4 stem had metaphyseal engagement, 5 had proximal diaphyseal engagement and 1, with anatomical geometry, had metaphyseal fixation. 2 cases required stem cementation, 3 modular neck and 1 lateralised. The clinical data, complications and clinical outcomes, were recorded and analysed.
Results:
The mean Harris Hip Score (HHS) increased from 34 preoperative to 86 postoperative; preoperative mean neck shaft angle (NSA) was 150°, head/neck ratio 0.6, offset 31 mm; Wiberg angle 28°, Sharp angle 38°, 1 patient had subluxation grade 4 according to Crowe, 8 hips showed osteoarthritis (Tönnis grade ⩾2 ); 5 femurs were classified as Dorr type C, 2 as type B and 3 as type A. Perioperative complications were not observed.
Conclusions:
Primary THA in HME significantly improved clinical and functional outcomes. Press-fit cup fixation together with metaphyseal and proximal diaphyseal stem engagement on reliable bone quality femur, represents a valid option in HME patients with normal acetabular morphology, wide broaden neck and valgus NSA.
Keywords
Introduction
Hereditary multiple exostosis (HME) is a rare autosomal dominant disorder, characterised by a development of multiple osteochondromas generally localised around the metaphysis of the long bones, among others, with a prevalence of 1 per 50,000 in the general population. 1 The axial and appendicular skeleton is unequally involved and this condition usually affects knees, shoulders, ankles and wrists; however in literature the incidence of hip exostosis has been reported to be very common, around 30–90%.1–3
The patients afflicted by HME can present variable bone deformities of the femoral neck and of the inter-trochanteric region, resulting in an abnormal metaphyseal enlargement and coxa valga, that represent the 25% of cases.3,4
While acetabular dysplasia is not necessarily common in skeletally mature patients afflicted by HME, 5 the aforementioned deformities may determine the narrowing of the ischio-femoral space, increasing the risk of femoroacetabular impingement and premature coxofemoral osteoarthritis up to 62% of the cases.6,7 However, patients often remain asymptomatic until a mechanical restriction, trigged by the exostosis in association with the degenerative joint processes, causing functional hip limitations and constant pain; this clinical evolution may require in some cases a surgical treatment. In fact, the surgical excision should be preventively considered in young patients with peduncolated exostosis of the hip and with a reduction of ischio-femoral space, and also in absence of significant degenerative changes, while, total hip arthroplasty (THA) remains the principal surgical treatment available in patients with extensive exostosis or hip deformations with severe osteoarthritis. The aim of this retrospective study is to evaluate and describe the follow-up of 7 patients affected by HME, who underwent THA.
Material and methods
This study is a retrospective review of several adult patients affected by HME, treated with a primary THA in a primary referral centre for bone tumours (Istituto Ortopedico Rizzoli, Bologna, Italy) between August 2009 and February 2020.
For the following study, the orthopaedic oncologists selected a total of 7 patients (6 female, 1 male). The mean age at the moment of the surgical treatment was 54 years (range 37–72 years). 3 patients were affected bilaterally by coxofemoral arthritis, and therefore, underwent to a bilateral implantation of THA; indeed the total number of THA were 10. Informed consent was obtained from every patient undergoing the surgical treatment.
Radiological analysis
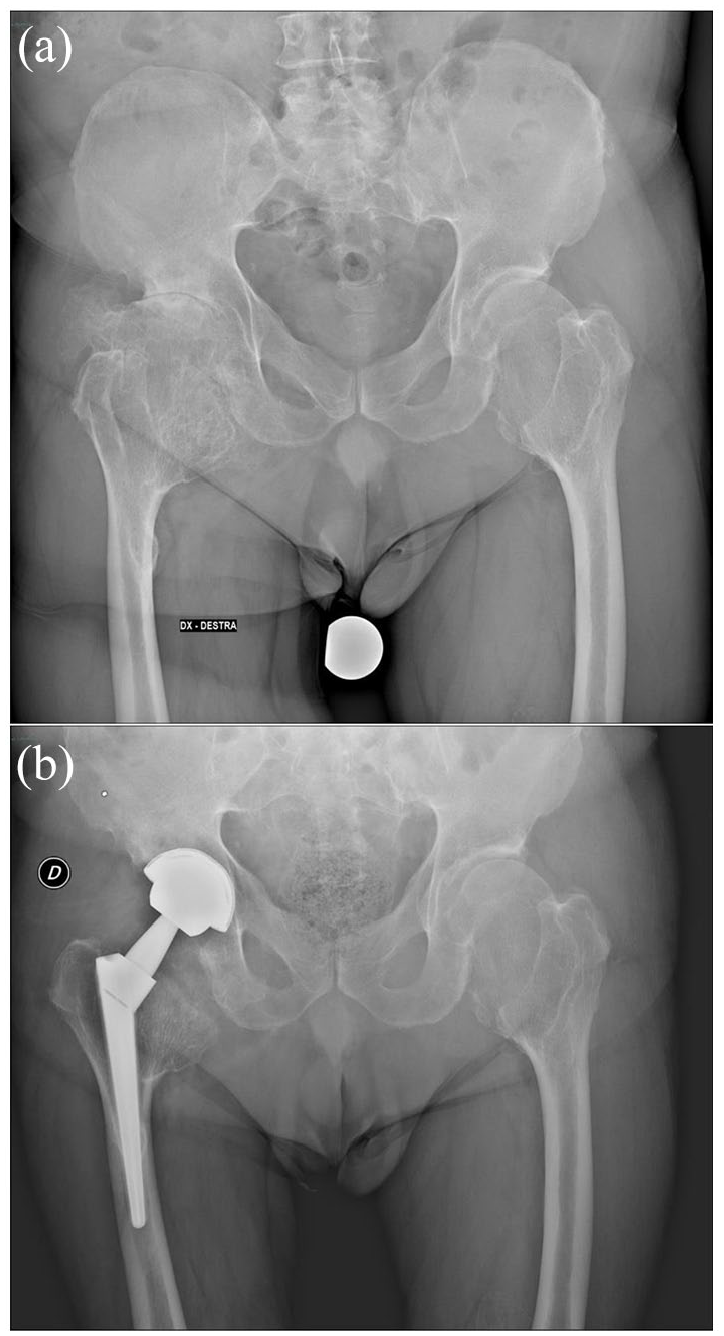
Every patient in this study underwent anteroposterior (AP) radiographs and a preoperative computed tomography (CT) scan (Figure 1) of the pelvis. The obtained radiological data were evaluated, in order to detect hip deformities and degenerative joint conditions.
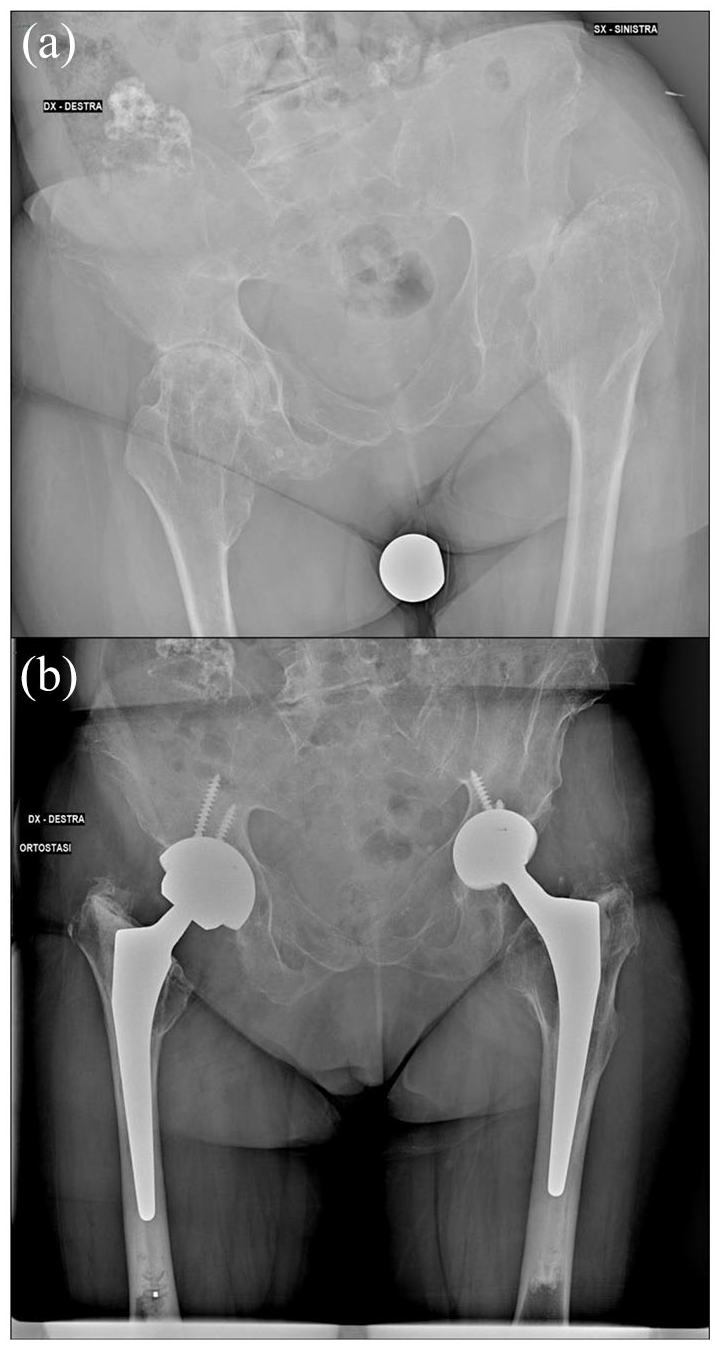
(a) 64 female bilateral case: left hip Crowe grade 4, Dorr type B; right hip Tönnis grade 3, Dorr type B and (b) bilateral hip arthroplasty at 2.9 years follow-up: hemispheric press-fit cup with 2 screws, cemented stem, lateralised neck on the left hip, standard neck on the right.
Proximal femur anatomy and deformity were assessed by different radiological and anatomical parameters: we considered the femoral neck shaft angle (NSA - angle between the line passing through the middle of the femoral neck and the anatomical axis of femur - normal range 120–135°), 8 the femoral head/neck ratio (calculated dividing the widest diameter of the head and neck - average normal value 1.29), 9 the femoral offset (perpendicular distance between the centre of rotation of the femoral head and a line bisecting the femoral canal - normal range, 41–44 mm) and in the end the Dorr index (ratio of cortical width minus endosteal width to cortical width at a level of 100 mm below the tip of the lesser trochanter - types A: Fluted, B: Normal, C: Stove Pipe).10,11
Usually, exostosis are classified based on their morphology in 2 types: all-around type (broad circumferential exostosis around the methaphysis) (Figure 2) and peduncolated-type (connected to the bone by a narrow stem).
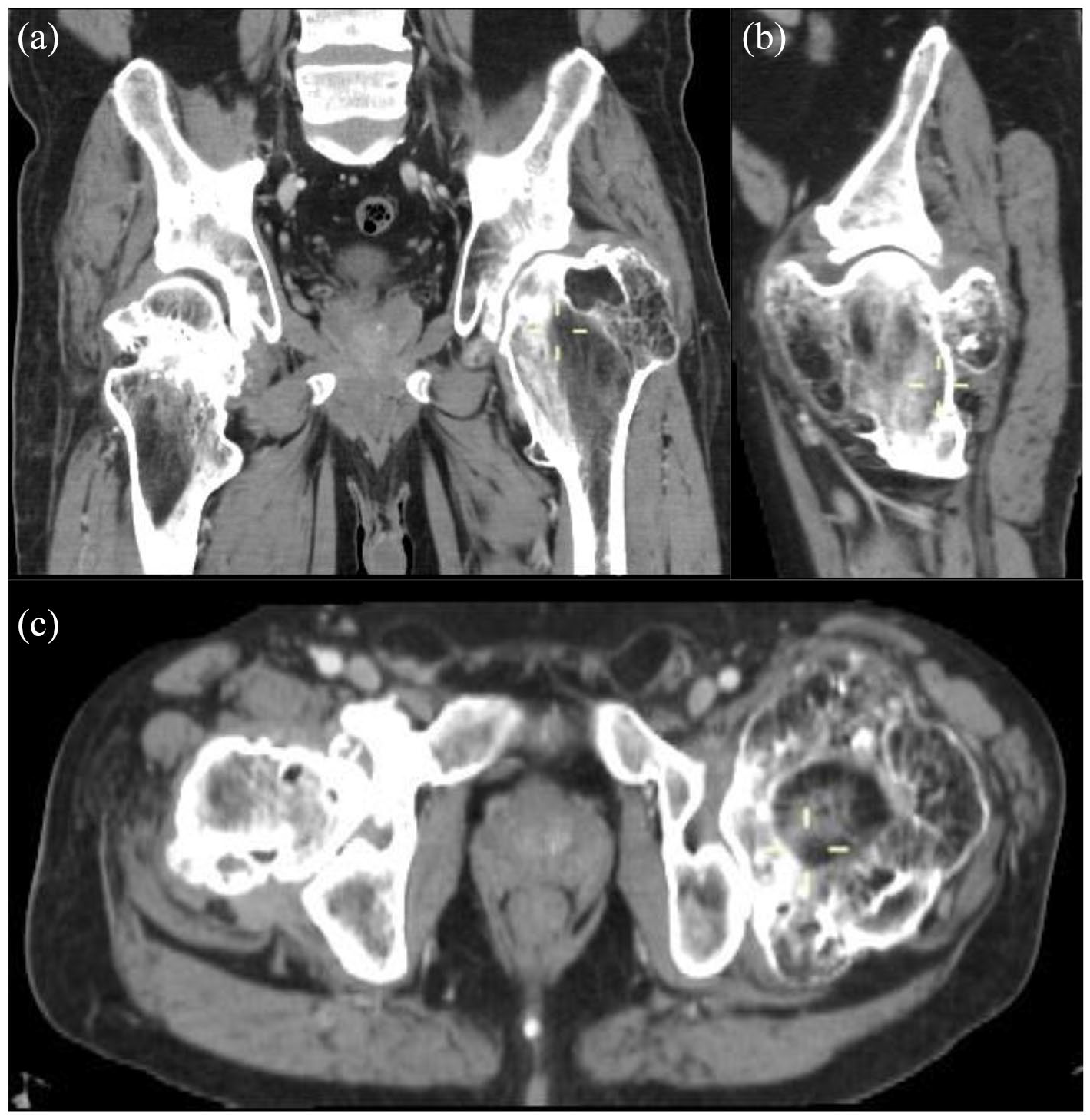
CT scan showing proximal femur all-around type exostosis with metaphyseal enlargement: (a) coronal view, (b) sagittal view, and (c) axial view.
Acetabular morphometry was investigated using the Wiberg centre-edge angle (head coverage, subtended by a vertical line through the centre of the femoral head and a line between the center of the femoral head and lateral acetabular border - normal 20–45°) 12 and Sharp’s acetabular obliquity angle (angle subtended by the line joining the inferior tips of the tear-drops and the line joining the supero-lateral to the infero-medial edge of the acetabulum - normal <45°). 13
In order to estimate the degenerative process in the joint, the orthopaedic oncologists used the Tönnis classification and assessed the grading of hip osteoarthritis, 14 while the Crowe classification was used to determine the grade of femoral head subluxation. 15
Histological analysis
All surgical pieces removed from the patient, were sent to the Anatomy and Pathological Histology Department of Istituto Ortopedico Rizzoli for histological analysis.
Implant analysis
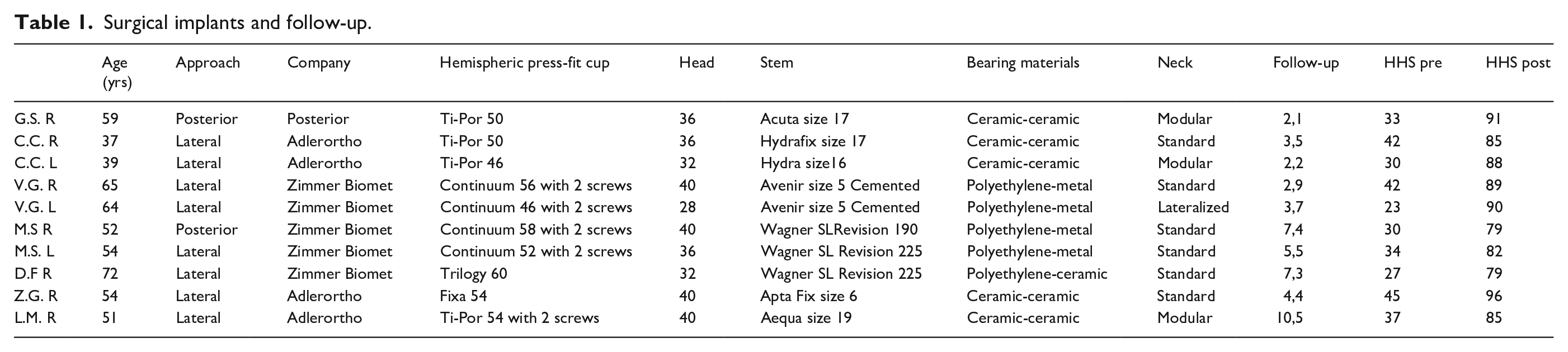
The primary total hip arthroplasty was performed using a direct lateral approach in 8 cases, 16 while a posterior approach was performed in 2 cases. 17 The patients affected by a bilateral presence of hip exostosis associated with an articular degeneration, underwent a 2 times surgery; the second THA has been performed after 12 month from the previous surgical treatment. All acetabular components were press-fitted in the native acetabulum and in 5 cases 2 screws were used for additional fixation. As for the femoral component, according to the Mont group classification, 18 4 stems belonged to type 1 (single wedge geometry, metaphyseal fixation), 5 to Type 3b (conical tapered geometry with splines, metaphyseal-diaphyseal junction and proximal diaphyseal fixation) and 1 to Type 6 (anatomical geometry, metaphyseal fixation). Only 1 case has required a bilateral cemented stem for poor bone quality, 3 cases required modular necks, while in 1 patient a lateralised neck was used (Table 1).
Surgical implants and follow-up.
Rehabilitation
Patients started the physiotherapy protocol on the first postoperative day with static quadriceps exercises, passive flexion and extension of the hip and progressive weight-bearing - standing, mobilisation with a walking frame or crutches as comfort permitted; they were advised not to adduct and internally rotate the limb and to use a walking aid for at least 4 weeks.
Follow-up
Patients were evaluated at a mean follow-up of 5 (range 2–10) years. No patient was lost at follow-up. Clinical and functional outcome was assessed using Harris Hip Score (HHS); particular attention has been paid to the detection of periprosthetic joint infections (PJIs), femur fracture, prosthetic loosening or dislocation.
Ethical approval
This research was conducted according to the World Medical Association Declaration of Helsinki and the local Ethics Committee of University provided approval.
Results
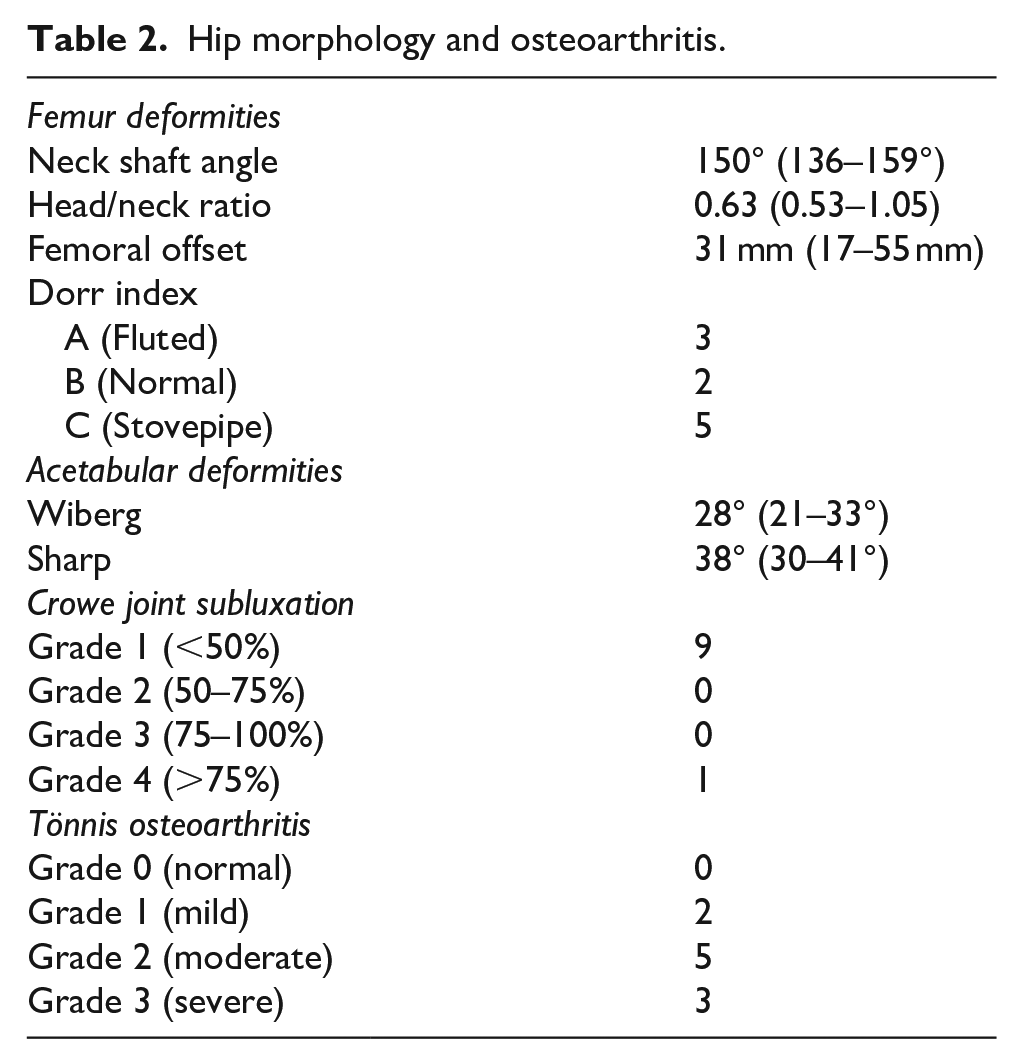
9 cases had all–around neck type exostosis whereas 1 patient had a peduncolated type exostosis arising from the “calcar” associated with avascular necrosis (AVN) of the femoral head. 8 cases (80%) showed degenerative osteoarthritis (Tönnis grade ⩾2). 1 patient had subluxation grade 4 according to Crowe classification; all other patients were classified as grade 1. The average preoperative neck/shaft angle was 150° (136–159°), head/neck ratio 0.63 (0.53–1.05), offset 31 mm (17–55 mm). Wiberg angle 28° (20.8–33.2°), Sharp angle 38° (30–41°). 5 femurs had Dorr morphotype C (stove pipe), 2 B (normal) and 3 A (fluted) (Table 2). In all Dorr type A were used type 3b stems.
Hip morphology and osteoarthritis.
Straight stems (both type 3b and type1) were used in patients with severe femoral deformities: NSA >144° and all-around neck type exostosis with head/neck ratio <0.70. Curved anatomical stem instead (type 6 stem), was used in a patient with NSA 136°, with a sessile infero-medial type exostosis with a head/neck ratio 1.03.
The histological report of all the resected exostoses confirmed the absence of malignant transformation.
No intraoperative complications (femur fractures, sciatic/femoral nerve palsy) or early/late prosthetic dislocation occurred. At 5-year mean follow-up, no incidence of PJIs, implant loosening, exostosis recurrence has been recorded.
Average HHS at follow-up, improved from a preoperative 34 (23–45) to a postoperative 86 (79–96).
Discussion
Patients affected by HME of the hip develop characteristic deformities, resulting from a physeal growth plate disorder; some authors, like Higuchi et al. 5 reported a mean NSA of 147° on 36 hips, while acetabular indices like Wiberg and Sharp’s angle were within normal limits. Our study confirmed an increased valgus deformity (mean value 150°) and acetabular morphometry within the anatomical range.
The decreased femoral head/neck ratio and a reduction of femoral offset, typically representing an abnormal broadened femoral neck, directly affect hip joint kinematics with progressive limitation, generating a reduction of abductor leverage 19 ; as a consequence, moderate to severe early hip arthritis (Tönnis grade ⩾2) was found in 80% of the examined cases as a result of extended proximal femoral deformities; 1 case with infero-medial exostosis, arising from the lesser trochanter, had mild arthritis associated with AVN, suggesting perhaps the involvement of peduncolated exostosis in the impairment of the proximal femur vascularisation.
Since proximal femoral osteochondromas relate to coxa valga and overgrowth of femoral neck, lateral subluxation of the femoral head may occur as a result of medial impingement. 4
Total hip replacement should be considered in patients affected by HME when a severe OA occurs, and when the excision alone does not allow symptom resolution, as well as in wide circumferential deformities.
The incidence of hip replacement in HME, as reported by Scarborough and Moreau, 7 is about 1%; when arthroplasty is required, surgeons must deal with severe hip dysmorphisms that can make surgery challenging.
After neck osteotomy, surgery should be addressed to remodel proximal femur, without the intent of a complete exostosis resection. Particular attention should be taken in shaping the infero-medial part of the osteotomy area in order to reduce the risk of ischio-femoral impingement in case of prominent osteochondromas.
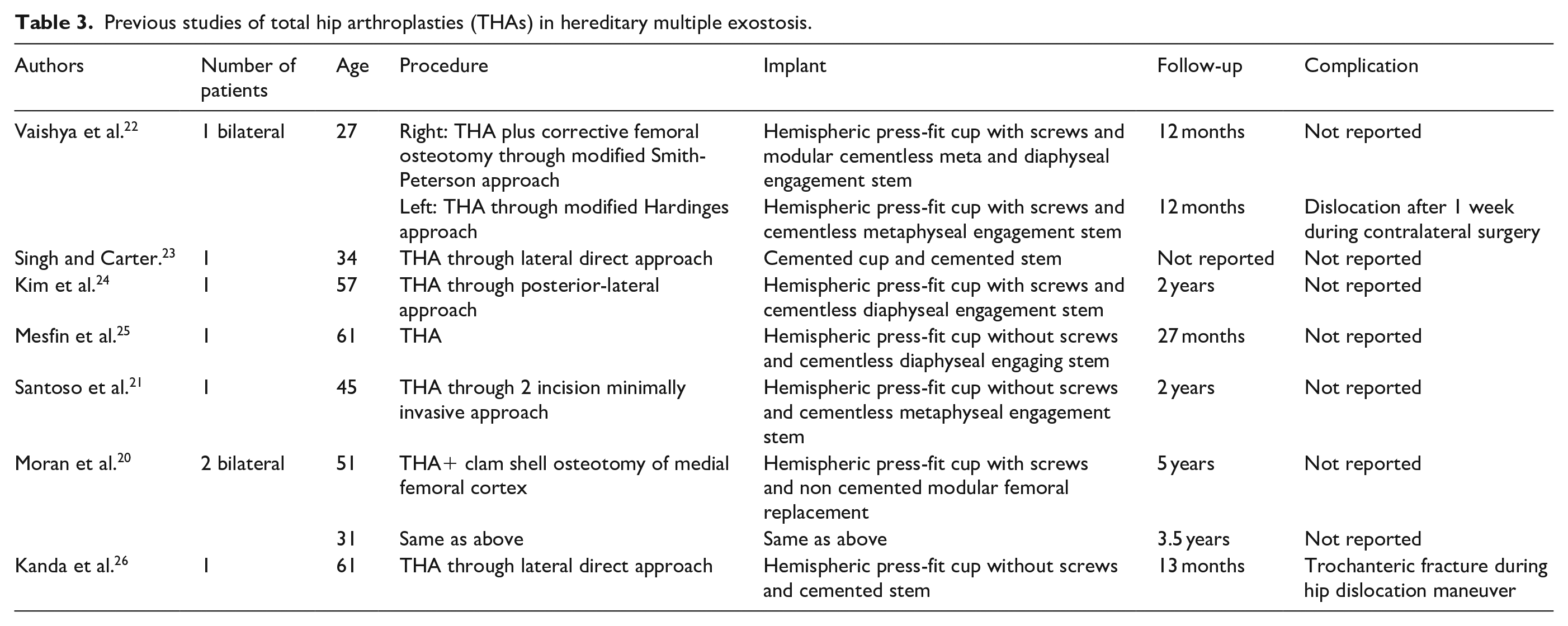
In the current literature, different techniques have been proposed to face femur deformities (Table 3): Moran et al. 20 suggests that patients with severe deformity require proximal femur replacing prostheses and “clam shell technique” to provide an optimal diaphyseal access and acetabular exposure. On the other hand, Santoso et al. 21 proposed a mini-invasive 2 incisions approach with excellent clinical result at 2 years follow-up; other authors managed to reduce the excessive valgism performing a THA associated with upper third femoral osteotomy to accommodate the femoral stem, 22 as it appears clear that the bony deformity dictates the surgical technique and the implant’s choice.
Previous studies of total hip arthroplasties (THAs) in hereditary multiple exostosis.
In our experience, a significant emphasis must be placed on the femoral deformity assessment through preoperative x-rays and CT scan, in order to choose the most suitable implant.
Cup choice does not represent a critical issue, since acetabular morphology is usually preserved; in this regard, the use of hemispheric press-fit cups with the possibility to insert screws, always provide a correct placement and stable primary fixation. Femoral deformity can be managed by taking advantage of the variety of stems geometry, modularity and site of fixation offered on the market. In our case, both type 1 and type 3b stems were preferred in femurs with all-around neck type exostosis, valgus NSA and wide neck, as the straight geometry provides good meta-diaphyseal fixation; instead curved anatomical stem could be a valid option in femurs having peduncolated type of exostotsis, where deformities are less pronounced and head/ neck ratio is preserved.
In fluted femur morphotypes (Dorr type A) Park et al. 27 reported a higher complications rate (periprosthetic fracture, aseptic loosening and deep infection) compared to Dorr type B; in our experience a conical tapered stem with splines (type 3b) should be preferred to ensure proximal diaphyseal fixation considering that, from a geometric point of view, a sharp narrowing of proximal canal do not represent a favorable shape for broaching procedure with anatomical broaches (Figure 3); normal and stovepipe morphology, instead, can be managed with metaphyseal fitting stem, capable of providing stable fixation. Singh and Carter 23 used a cemented stem in 38-year-old patient to prevent instability because of a wide methaphysis.
(a) 59-year-old male, femur Dorr type A, Tönnis grade 3 and (b) total hip arthroplasty: hemispheric press-fit cup, uncemented conical stem with splines (Mont type 3b), modular neck at 2.1 years follow-up.
In this study there was no evidence of press-fit stem failure at mid term follow-up, and considering the general age of the sample group (mean value 55), our experience suggests that cementation is a second level option that should be considered only in old patients in view of inferior bone quality (Figure 3).
Finally, an increased joint laxity, as a consequence of a larger proximal femoral geometry, together with offset reduction and valgus neck, may lead to a higher postoperative hip dislocation rate. Vaishya et al. 22 reported the occurrence of hip dislocation in a bilateral case at about 1 week after surgery, following contralateral arthroplasty. No other dislocations were reported in literature; in case of significant offset reduction, in combination with the ante-retroversion of the femoral neck, the joint centre of rotation restoration can be eventually managed with a modular neck in order to improve implants stability. 28 We encourage the use of a large diameter head and a well performed preoperative planning to prevent hip dislocation.
Limits of this study are related to the small cohort of patients, the relatively short-term follow up and the retrospective design that did not allow the assessment of a reliable evaluation of leg-length discrepancy.
Conclusion
Patients with hereditary multiple exostosis may incur in early osteoarthritis or functional limitations due to the wide architectural deformations of the afflicted articulations. In this selected group of patients, the total hip replacement represents the only solution to restore joint motion and ensure pain relief. Because of the difficulty of an anatomical correct restoration, a careful preoperative assessment is mandatory in order to understand the hip deformity; THA providing press-fit cup fixation and uncemented straight stem with metaphyseal and proximal diaphyseal, represents a valid option in HME patients with normal acetabular morphology, wide broaden neck and valgus NSA; indeed our study has demonstrated a good midterm clinical results in absence of perioperative complications in patients with these morphological characteristics. Larger case series studies with longer follow-ups and, possibly, with standard implants and surgical approach analysis are required to outline a proper implant selection and validate the safety of this procedure in HME patients.
Footnotes
Acknowledgements
We thank Giulia Zoggia for her contribution to the English correction of the article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.